
Abstract
Intimate partner violence (IPV) has myriad negative health and economic consequences for women and families. We hypothesized that empowering women through a combination of formal business training, microfinance, and IPV support groups would decrease IPV and improve women’s economic status. The study included adult female survivors of severe IPV. Women living in Korogocho received the intervention and women in Dandora served as a standard of care (SOC) group, but received the intervention at the end of the follow-up period. Women in the intervention groups (n = 82, SOC group, n = 81) received 8 weeks of business training, assistance creating a business plan, a small initial loan (about US$60), and weekly business and social support meetings. The two primary outcome measures included change in: (a) average daily profit margin, and (b) incidence of severe IPV. Exploratory analysis also looked at incidence of violence against children and women’s self-efficacy. Average daily profit margin in the intervention group increased by 351 Kenyan Shillings (about US$3.5) daily (95% CI = [172, 485]). IPV directed against participating women decreased from a baseline of 2.1 to 0.26 incidents, a difference of 1.84 incidents (95% CI = [1.32, 2.36]). Violence against children in the household in the prior 3 months decreased from 1.1 to 0.55 incidents, a difference of 0.55 incidents (95% CI = [0.16, 1.03]). Finally, the intervention appears to have increased self-efficacy scores by 0.42 points (95% CIs 0.13, 0.71). In a low-resource urban environment, employing three complementary interventions resulted in higher daily profit margins and lower IPV in the intervention compared with the SOC group. These data support the notion that employing multiple interventions concomitantly might possess synergistic, beneficial effects, and hold promise to address profound poverty and interrupt the devastating cycle of IPV.
Introduction
Intimate partner violence (IPV) is the most common form of violence against women worldwide. The lifetime prevalence of IPV among ever-partnered women is 36.6% in the World Health Organization’s (WHO; 2013) Africa region. In Kenya, IPV is a widely accepted as normative behavior, as 36.2% of men and 41.8% of women agree that physical violence is acceptable under some circumstances (Kenya National Bureau of Statistics & ICF Macro, 2016). Furthermore, the prevalence of violent experiences is high in Kenya, with 44.8% of women reporting physical violence and 14.1% experiencing sexual violence, most often perpetrated by current or former husbands/partners (Kenya National Bureau of Statistics & ICF Macro, 2016). Although IPV affects women worldwide, women in low and middle income countries (LMIC) are 2.5 times more likely to be murdered during an episode of IPV than women in high-income countries (Matzopoulos, Bowman, Butchart, & Mercy, 2008). Although thousands of women are killed and injured by IPV, the toll on reproductive, sexual, and mental health is incalculable (Campbell, 2002; Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; García-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006).
In addition to the profound human cost, IPV also compromises a country’s economic health and development. The annual direct cost of IPV in the United States in 2004 was estimated at US$ 8.5 billion (Max, Rice, Finkelstein, Bardwell, & Leadbetter, 2004). In Australia, in 2007, the direct cost was estimated to be 13.8 billion Australian dollars. Although direct costs can be measured, indirect costs such as lost days of paid work in adults, estimated to be 8 million days a year in the United States, or the developmental compromise that children experience, are arguably far more profound (Centers for Disease Control and Prevention [CDC], 2003; UN Women, 2014).
In many countries and communities, women economically dependent upon a husband or male partner are significantly more likely to experience IPV than economically independent women (Bornstein, 2006; Dhungel, Dhungel, Dhital, & Stock, 2017). Compared with wealthier women, the vulnerability of women living in poverty is accentuated by minimal decision-making power and, often, limited education (Bourey, Williams, Bernstein, & Stephenson, 2015; Heise, 1998). These factors likely combine to fuel the cycle of IPV, as financially insecure women have difficulty leaving abusive relationships and often have low self-efficacy that further reduces their ability to find work or start a business (Hunter, 2010). Nonetheless, decreasing economic dependence does not always decrease IPV, as in areas where few women are in the workforce, IPV may increase as women gain economic independence (Heise & Kotsadam, 2015). Therefore, economic interventions designed to decrease the incidence of IPV must carefully consider local norms and cultural practices prior to broad implementation.
The problem of IPV, both in sub-Saharan Africa and worldwide, has proven difficult to effectively address. Strategies that employ multiple, complementary interventions concomitantly, such as microfinance and formal training on gender or health issues, have demonstrated greater efficacy than solo strategies (Gibbs, Willan, Misselhorn, & Mangoma, 2012). A large study that took this approach, the Creating Futures program, focused on livelihood improvement and IPV prevention in South Africa (Jewkes et al., 2008). That study resulted in a significant decrease in IPV, from 30.3% to 18.9% in the previous 3 months (Jewkes et al., 2014). Also in South Africa, the Intervention with Microloan for AIDS and Gender Equity (IMAGE) study decreased past 24-month physical or sexual IPV by about half (Kim et al., 2009; Kim et al., 2007; Pronyk et al., 2006). IMAGE combined microloans with training sessions on IPV, gender norms, and sexuality. Combination intervention approaches have also been effective beyond sub-Saharan Africa and/or in multinational studies. Specifically, structural interventions that included both livelihood and gender components consistently demonstrated positive results, especially for women beyond the age of 18 (Gibbs et al., 2012). Given the tight connections between IPV and economic dependence, and the emerging literature surrounding the power of combined interventions, we tested the hypothesis that in an unplanned settlement in Nairobi, combining formal business training, microfinance, and an IPV support group intervention would improve women’s economic status and decrease IPV. This study took advantage of a natural experiment, where a nongovernmental organization (NGO) was expanding a promising intervention. This provided the opportunity to design a quasi-experimental study to understand the effects of this expansion, and therefore to add to the knowledge base of applied research on combination interventions and IPV prevention.
Method
Intervention
This intervention, titled “Mashinani” (together we can succeed economically), was implemented in one unplanned settlement (Korogocho) in Nairobi, Kenya from October 2014 to May 2015. Mashinani was created and run by the NGO Ujamaa-Africa (http://ujamaa-africa.org/), and provided microloans, business management training, and psycho–social support to groups of five to eight female survivors of severe IPV (defined as rape, serious physical violence, or both) to start their own businesses. Community victims of IPV were recruited and vetted with the assistance of the local administration (Chiefs and Village Elders) and an established community leadership center. Participating women had to be 18 years or older. Dandora, an adjacent and demographically similar unplanned settlement, was selected as the standard of care (SOC) community. This SOC group received the intervention at the end of the follow-up period, but were not followed beyond that.
The Mashinani model began with 8 weeks of training in business skills, including decisions about business type, location, supply procurement, marketing, bookkeeping, and customer service. Following the initial training period, each woman wrote a business plan which was reviewed and revised in collaboration with Ujamaa staff. Upon business plan approval, an initial loan of Ksh.5,000 (~US$59 at that time) was issued with an expectation of attendance at weekly business development and support group meetings. A business development officer was assigned to each participant and provided guidance and advice either in person or via telephone if participants did not attend weekly meetings or request additional support.
The overall design of the study was based loosely on the successful “IMAGE” study in South Africa, with variations, described below, in both the microfinance model and the participatory training sessions, which here were focused on social support more than gender norms and sexuality (Kim et al., 2009; Kim et al., 2007; Pronyk et al., 2006). The microloan model was based upon the Grameen Bank, wherein groups of five women serve as guarantors for each other’s loans (Nanda, 1999). All group members were expected to repay the loans prior to any member of group receiving additional credit. The groups met weekly for 30 to 60 min for ongoing business training and support. Loan installments of Ksh.225 (~US$2.6) were paid weekly. The community-run bank in the Mashinani model was self-governing with each group electing a representative to the parliament of the bank. The parliament created and ratified the Mashinani Constitution which detailed the policies for access to capital, loan payment or nonpayment procedures, loan re-issuance and loan amount following successful group repayment.
The IPV support intervention, titled Tupone Pamoja Initiative (TPI), is a 12-step program focused on coping with prior or even ongoing IPV. The groups met once a week, generally immediately following the business meeting with the same group of women, for sessions lasting between 20 and 60 min. All facilitators were survivors of severe IPV and graduates of the TPI program. Session topics ranged from strategies to mitigate self-blame to insight-driven conversation encouraging women to support other IPV survivors.
In October 2014, 82 women from the intervention community (Korogocho) and 81 women from the SOC community (Dandora) were enrolled. The intervention group began business training. Loans were disbursed to women in December 2014 and January 2015, and final follow-up surveys were collected in April and May 2015, allowing 4 to 5 months of follow-up time (Figure 1).

Average self-reported daily profit at baseline (“pre”) and at follow up (“post”).
Study Design
The research team utilized planned expansion of this intervention to design a quasi-experimental study wherein two adjacent unplanned settlements, Korogocho and Dandora, were designated as the intervention and SOC communities, respectively. These communities are demographically similar relative to crime and unemployment rates in the formal sector, as well as poor health metrics, such as very high under-five mortality rates, 99.8 per 1,000 compared with 64.5 per 1,000 in all of Nairobi, and deep poverty (Emina et al., 2011; Ziraba, Madise, Mills, Kyobutungi, & Ezeh, 2009). According to the 2009 Kenya census, Dandora has a population of approximately 90,000 people, and Korogocho has a population of approximately 175,000 people, each comprising an area of approximately 1.5 square kilometers (Kenya National Bureau of Statistics, 2017). Adult women IPV survivors from these communities were eligible for enrollment. The study underwent Institutional Review Board review and approval at Stanford University (protocol #31222) and received research permission from The National Commission for Science, Technology, and Innovation in Kenya.
Outcomes
The two primary outcomes were (a) changes in average daily profit margin, as reported by the women and defined as the money left over at the end of the day once business-related expenses had been paid, and (b) changes in the probability of severe IPV incidents (physical abuse or rape) in the preceding 3 months (self-reported). Severe IPV was measured using a minimal set of questions that were derived from Kenya Demographic and Health Survey (DHS) questions on domestic violence. These questions included information about specific acts of violence and frequency (e.g., “In the last three months, has your husband/partner beat or physically assaulted you? If yes, how many times in the last three months?”). Though use of validated questions such as those from the DHS or World Health Organization would have been preferable, simplifications in the queries were made to owing to the amount of time available for data collection and the highly sensitive nature of the information sought.
Sociodemographic information such as average daily household costs and partnership status, as well as secondary variables of interest, including the incidence of violence against children in the household and changes in self-efficacy (using the previously validated Generalized Self-Efficacy Scale, GSES) were also collected. All data were self-reported and collected on confidential paper surveys distributed by research personnel at regularly scheduled Mashinani meetings.
Data Analysis
Though the two unplanned settlements are similar, there was no randomization or random sampling into the intervention or SOC groups. To account for baseline differences between members of the intervention and SOC groups an inverse probability weighting study design was used (Hernán & Robins, 2006). The propensity scores were modeled using the following measurements collected prior to the start of the study: year of birth, GSES score, partner (y/n), number of children, average profit per day, and recent IPV experiences (severe physical violence and/or sexual violence). In this design strategy, the weights are used to make the two groups similar in terms of their baseline covariates. The weights are fit on pretreatment (aka “baseline”) covariates and then applied to the outcome variables. Under several important assumptions (Hernán & Robins, 2006), the reported estimates can be interpreted as the effect of the intervention on the treatment group. Confidence intervals were calculated using the bootstrap method. Data were analyzed using the R software package ipw (R Core Team, 2015).
Results
Baseline
At baseline (Table 1), the SOC group was similar to the intervention group relative to age, proportion of women that had experienced sexual violence, and rates of child physical and sexual assault. The differences in proportion of partnered women and number of children were small. However, between the SOC and intervention groups, there were important differences relative to daily profit margin, proportion of woman reporting physical violence, and current business ownership. The numbers of missing variables was similar between the two groups. Propensity score methods were employed to address these observed imbalances.
Baseline Values of Key Variables.
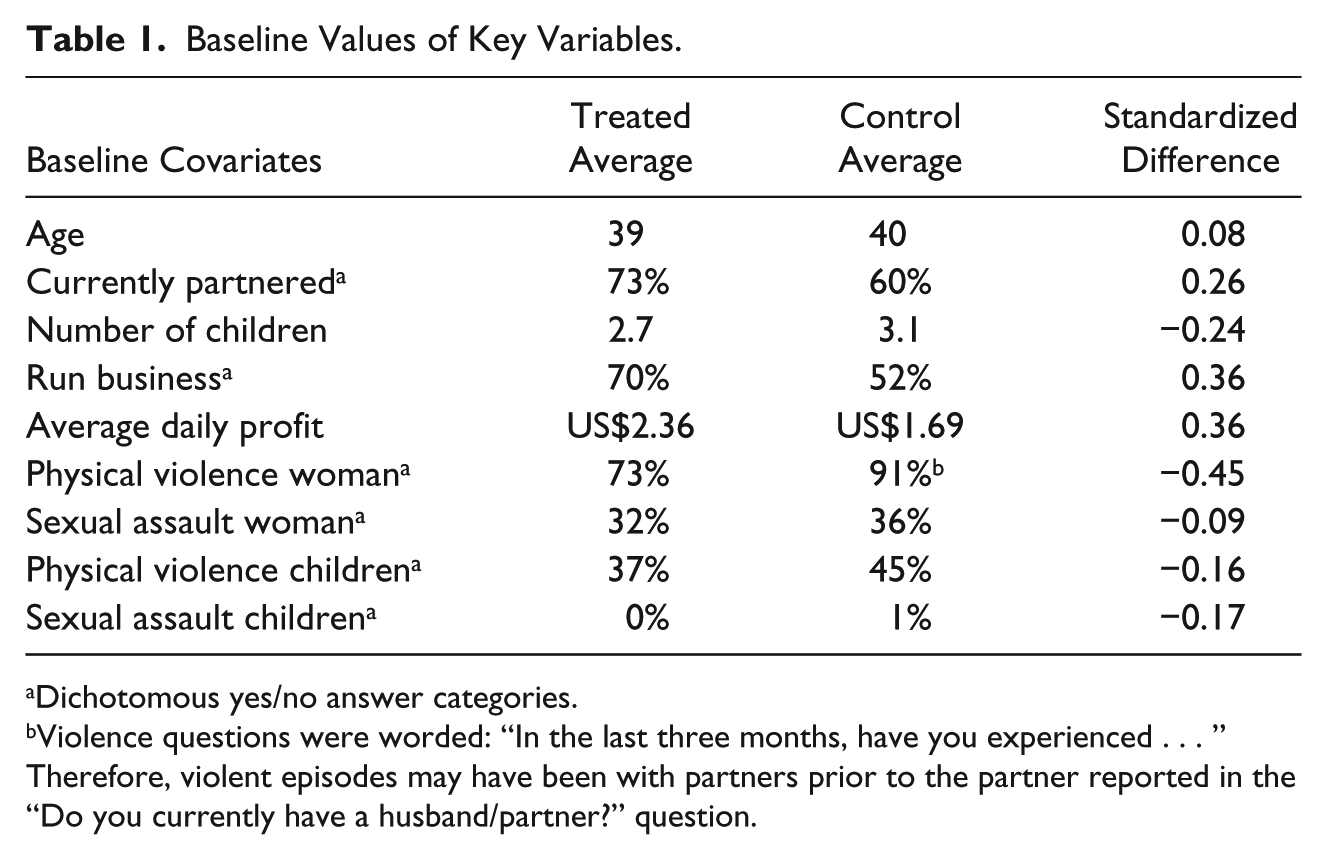
Dichotomous yes/no answer categories.
Violence questions were worded: “In the last three months, have you experienced . . . ” Therefore, violent episodes may have been with partners prior to the partner reported in the “Do you currently have a husband/partner?” question.
Women reported spending a median of US$2.50 per day total, with basic food (US$2.00 per day) and household expenses such as cooking fuel and water (US$0.50 per day) comprising the expenditures. The median, modal, and mean number of children in the household was approximately three, though a handful of families reported having eight or more children in the household.
The majority of women in the intervention group reported physical violence if they asked their partners for money (47/82, 57.3%). Other percieved reasons for abuse included alcohol consumption by their partners (13, 15.8%), stress (4, 4.9%), and infidelity (3, 3.7%).
Post-Intervention
If the individuals had been randomized to treatment and control then we would estimate the intervention increased average daily profit margins by 351 (95% CI = [172, 485]) Kenyan Shillings (about US$3.5) daily. Figure 1 shows average self-reported daily profit at baseline (“pre”) and at follow up (“post”). There was a noticeable increase in the intervention group, indicating a general increase in the average daily profit for most participants. In contrast, in the SOC group, daily profit decreased in the post period, with many women reporting no daily profit.
Regarding the reporting of severe IPV incidents directed at the women (Figure 2), in the intervention group, in the 3 months prior to the survey, the incidence of severe IPV decreased to 0.26 from 2.1 during the baseline, a difference of 1.84 incidents (95% CI = [1.32, 2.36]). As depicted in Figure 2, there were fewer episodes of IPV in the intervention group, whereas there was no detectable change in the SOC group.
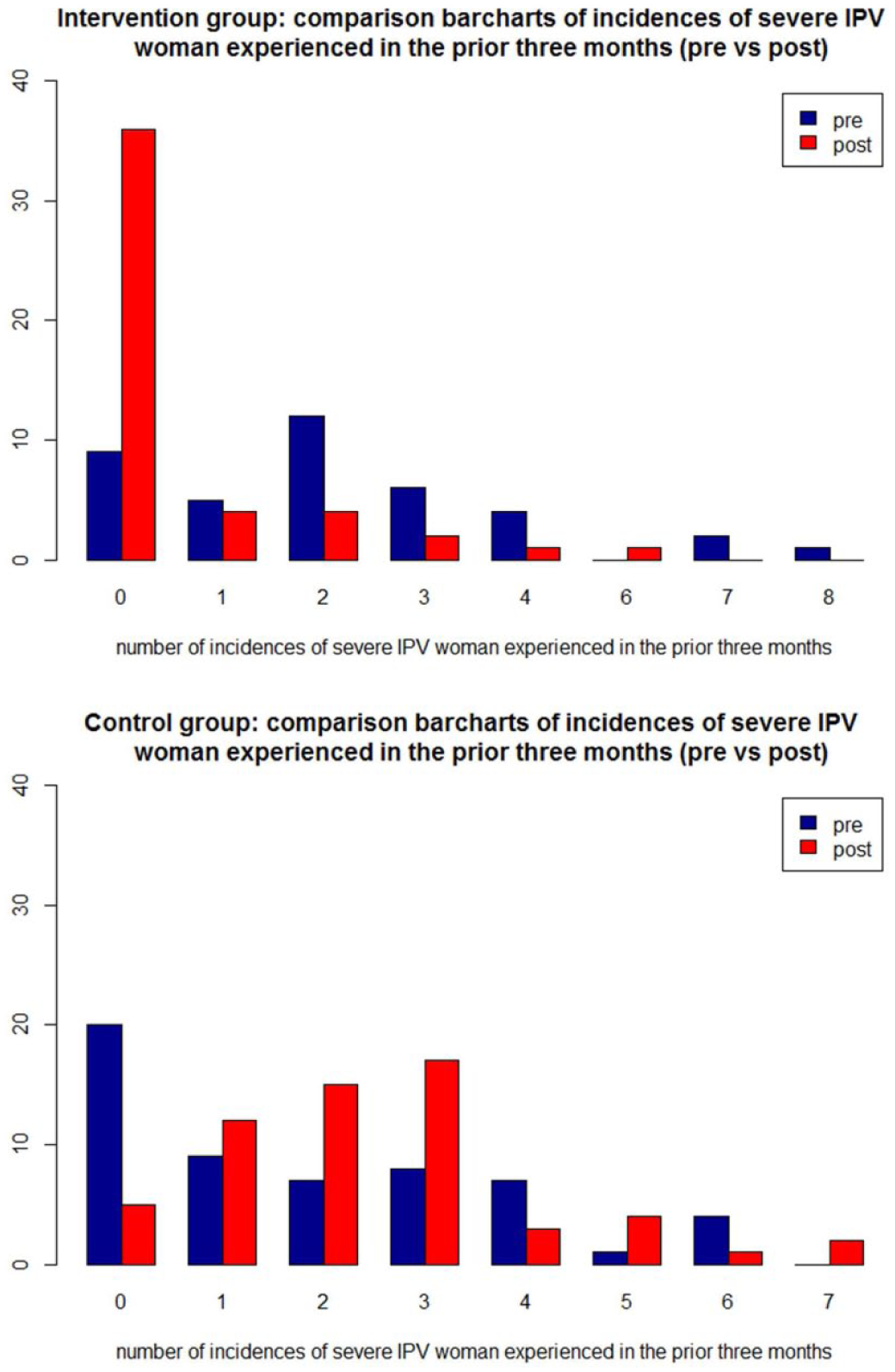
Bar charts comparing the number of assaults on women in the households, pre and post, for intervention (top) and control (bottom).
We also performed exploratory analyses on secondary outcomes of interest, including number of physical assaults on children in the household and self-efficacy of the women (GSES). Severe violence against children in the household in the prior 3 months decreased by 0.55 incidents from a reported baseline of 1.1 incidents, a change of 0.55 incidents (95% CI = [0.16, 1.03]; Figure 3).

Bar charts comparing assaults on children in the household, pre and post, for intervention (top) and control (bottom).
Finally, the intervention appears to have increased self-efficacy scores by 0.42 points (95% CI = [0.13, 0.71]).
Retention rates were high. In the SOC, 16.0% (13/81) were lost to follow-up: 12 of those dropped-out by choice, and one left the community. In the intervention group, 13.4% (11/82) of women originally enrolled were lost to follow-up: two left the community, six were dropped from the program for ongoing loan default, two dropped-out by choice, and one continued to attend business training and support group session but did not want to take a loan. The responses for the “violence against children” variable were however missing ~32% of the time (95/138 reported). Nonresponse was nearly identical between the treated and control (23/70 = 33% vs. 20/68 = 29%). To assess the possible effects of this nonresponse, logistic regression was performed to see if any of the baseline covariates were predictive of not reporting. The two variables that predicted nonresponse were women who did not have a partner and reporting higher average profits.
Discussion
Combining formal business training with microfinance and ongoing support group involvement correlated with an increase in daily profit margin and a decrease in the incidence of IPV. Moreover, in the intervention group, the incidence of violence against children decreased and self-efficacy among women increased; previous evidence shows that women with higher self-efficacy are more able to participate in economic activity (Zhao, Seibert, & Hills, 2005). The observation that over half of the women in the intervention group reported being beaten in response to asking their husbands for money suggests that if women have independent funds for household needs, potentially dangerous confrontations can be avoided. Furthermore, decreasing IPV likely increases profits. Thus, in this setting, as women are economically more empowered, protection from IPV increases as well. It is worth noting that the literature shows mixed results of the effect of economic empowerment on IPV, and in regions with very low penetration of women into the workforce, IPV may actually increase (Heise & Kotsadam, 2015). This reality underscores the importance of empirically evaluating the effect of an intervention to detect any unintended consequences prior to large scale interventions.
It is noteworthy that the increase in daily profit margins between the SOC and intervention groups (~US$3) more than covers average daily expenses (reported to be about US$2.50). Thus, the increase in revenue may possess meaningful financial implications for each family. The recently revised absolute poverty line, as defined by the World Bank, is US$1.90 or less daily, so the increase in profit margin, if sustained over time, may be sufficient to lift these women and their families out of abject poverty (World Bank Group, 2015).
Prior intervention based studies in sub-Saharan Africa addressing both structural economic inequities and gender norms have also shown promising results. A recent multinational study (including two sites in Africa, Ethiopia, and Ghana) demonstrated that combining microfinance, business mentoring, and health/life skills training interventions significantly increased both economic and women’s empowerment variables (Banerjee et al., 2015). That study also provided some evidence that these sorts of multifaceted interventions may be sustainable and scalable in the long run, due to increases in profit and savings. In rural South Africa, the IMAGE study combined a microloan program with ten 1-hr participatory training sessions on gender norms, domestic violence, and sexuality. After 2 years, the risk of past-year physical or sexual violence by an intimate partner was reduced by more than half (Kim et al., 2009; Kim et al., 2007; Pronyk et al., 2006). The intervention was also highly cost-effective, with an estimated cost per disability-adjusted life year (DALY) gained as US$7,688 for the trial phase and US$2307 for the initial scale-up (Jan et al., 2011; Jewkes, 2015). More recently in South Africa, the Creating Futures program, a livelihood strengthening intervention combined with a IPV prevention intervention showed a significant reduction in women’s experience of IPV in the prior 3 months from 30.3% to 18.9% (Jewkes et al., 2014). Creating Futures differed from previously evaluated interventions because it did not provide loans or other access to capital. It was nonetheless able to show significant changes in a short period of time, and those results are consistent with the present findings. A review of structural interventions that included both livelihood and gender components demonstrated positive results, particularly when targeted to older (not adolescent) women (Gibbs et al., 2012).
Other studies that included only one or two components of the present intervention demonstrate less positive results. A 2015 study in northern Uganda, Women’s Income Generating Support (WINGS) program, tested whether an entrepreneurship program that reduces poverty also empowers the women in other aspects of life. That cluster-RCT showed benefits in improving household consumption, income, and savings, but not in overall empowerment (Green, Blattman, Jamison, & Annan, 2015). Similarly, a randomized controlled trial (RCT) that tested the incremental impact of adding “gender dialogue groups” to an economic empowerment group savings program among women in Cote d’Ivoire (Gupta et al., 2013) did not find changes in physical and/or sexual IPV incidence. In that study, however, economic abuse did decrease significantly.
The preponderance of evidence, including this study, supports the proposition that combining structural interventions, such as economic support and gender-related training and education, can improve economic well-being and decrease violence against women and children, even in a short time-period. Furthermore, studies with only one (or possibly even two) components may be less likely to yield results. The present study, when considered in concert with prior data, offers support for expanding and critically evaluating the efficacy of combining structural interventions. In particular, research to identify the core components that lead to sustained economic empowerment and diminished IPV to support the adoption and implementation of these programs on a much broader scale, as well as on how the different components act synergistically upon each other, is needed.
Diversity
The target population of this study, women living in informal settlements, are diverse in many ways, most relevantly in terms of very low socioeconomic status. Thus, every step of the research process was focused on how to ethically and rigorously work with this population. Several of the Kenyan coauthors were instrumental to ensuring that methods and survey questions were culturally and linguistically appropriate, and were involved in reviewing data analysis and interpreting results. The results of this study are not meant to be widely generalizable, especially given the study size, but explicitly focus on promising approach in a highly marginalized group of women and children.
Limitations
This study was limited by a small sample size (163 women), a fairly short follow-up period (4 to 5 months), and the differences between the SOC and intervention groups at baseline. Overall (Table 1), the intervention group was better off than the SOC group prior to the study. The statistics reported above were estimated using a bias-reducing design, propensity scores to form inverse probability weights, but it is unlikely this approach could account for all of the baseline differences between the groups at the start of the study. There was poor overlap between the intervention and SOC groups, leading to propensity score models that predicted complete separation. This indicates confounding of baseline covariates with the level of intervention. Caution should be taken in attributing all of the estimated difference in outcomes to the intervention. There were also unexpected outside events which disrupted women’s abilities to operate and maintain their businesses. In particular, there was considerable gang activity that involved extortion of money from the women during this time period, which was expected, but it was not expected to be at as high a level as anecdotally reported by the women. Furthermore, there were large youth riots against redevelopment activities that were taking place in Korogocho, which resulted in unsafe business conditions for almost 2 weeks during the study period. All of these limitations, except the baseline differences, which we controlled for statistically as well as possible, likely decreased our ability to detect a difference. Finally, this study underscores the importance of rigorously evaluating an intervention to both test a hypothesis and to ensure that no untoward consequences accrue. Furthermore, as this study represented a natural experiment where an partner NGO was expanding an existing program with potential risk to participants, it serves as an example of the importance of evaluating such efforts to ensure that new and existing interventions first, do no harm, and second, have an effect on the outcomes the program is designed to change.
Conclusion
The interventions group in this study increased profits and decreased IPV in a vulnerable group of women, relative to the SOC group. As randomization was not done, the differences in outcomes may not be purely attributable to the intervention. Nonetheless, the coherence of the effects and positive changes in the anticipated intermediate effects, such as self-efficacy, provides evidence of an effect of the intervention. Replicated on a larger scale, a combined business training, microfinance, and support group intervention may be an important tool to address both profound poverty and IPV. Given the community-run nature of the bank and the significant increases in daily profit margins that might allow for savings, the present intervention has potential to become self-sustaining. Integrating health and economic development initiatives holds the promise of addressing the complex problems of multigenerational poverty and violence.
Footnotes
Acknowledgments
The authors would like to thank the Ujamaa-Africa Mashinani team who provided sensitive and thoughtful business development, support group, and financial management skills to the women in the program; Zhi Ping Teo for assistant with the literature review; Jennifer Lee Kang, MPH, for critical review and insights, and the women and their families.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Global Development and Poverty Initiative within the Stanford Initiative for Innovation in Developing Economies, and Manasseh’s Children Foundation in San Francisco, CA.