
Abstract
Exposure to child maltreatment in the family-of-origin has consistently been linked to intimate partner violence (IPV) perpetration in adulthood. Although the concept of a cycle of violence presumes that the transmission of violence is expressed directly across generations, some protective factors such as social support, self-esteem, and relationship quality with parents may ultimately be influential in nonviolent behavior in adult relationships. Using the National Longitudinal Study of Adolescent Health data set, we tested protective factors to see if and to what extent they disrupted the association from early childhood maltreatment to experiencing violence later on in adult relationships. We found that there was a positive association between adolescence exposure to maltreatment and adult perpetration and victimization of IPV. Also, social support in adolescence was identified as a predictor of lower levels of violence in adult relationship. Clinical implications were discussed to help therapists intervene with adolescents in the hopes of reducing their propensity toward violent relationships in adulthood.
Keywords
Domestic violence remains an important and wide-spread problem all over the world; nearly one in every three adult women experiences at least one physical assault by a partner during adulthood (World Health Organization [WHO], 2016a), and 275 million children around the world are exposed to violence in their family (UNICEF, 2006). As a form of violence, child maltreatment includes all types of physical and emotional ill-treatment, sexual abuse, neglect, or any act on the part of a parent or caregiver which results in harm to the child (WHO, 2016a). According to the latest child maltreatment report, 3.5 million child maltreatment cases were recorded to the National Child Abuse and Neglect System, and 74.8% of those victims were neglected, 18.2% were physically abused, and 8.4% were sexually abused (U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, 2016).
The effects of child maltreatment include many domains of functioning, such as mental health, behavioral, academic performance, and relationship with others (e.g., Crockett, Keneski, Yeager, & Loving, 2015), and these negative consequences have been found to continue into adulthood with an increased risk of violence (e.g., Iratzoqui & Watts, 2019). Although some factors attenuate the effects of child maltreatment, such as family relationships, social support, and personal resources (WHO, 2016b), much less is known about the process by which these factors mitigate the risk of experiencing violent behaviors in future romantic relationships among adolescences.
Theoretical Framework
In the vulnerability–stress–adaptation (VSA) model, Karney and Bradbury (1995) proposed that relationship outcomes are determined by the stressful life events that couples encounter, the enduring vulnerabilities that each partner brings to the relationship, and the quality of the couple’s adaptive process. In other words, individual differences in enduring vulnerabilities, such as being exposed to maltreatment in childhood, affect how individuals and couples adapt to stress in later life, such as if they continue to experience violence in their future romantic relationships. Specifically, Karney and Bradbury (1995) highlighted three factors that influence the adaptation process and create changes in relationships over time: (a) enduring vulnerabilities stemming from child maltreatment in the family-of-origin, such as abuse or neglect in the home; (b) stressful life events, such as having conflictual relationships, experiencing loss, or other contextual life challenges; and (c) adaptive processes such as how spouses interact and behave toward one another when they are faced with difficulties (e.g., problem-solving skills, partner support). By considering these vulnerabilities, stressful life events, and adaptations, it is theoretically possible to understand who will and will not be involved in intimate partner violence (IPV) in adulthood. Theoretically, people can change their reactions to maltreatment in childhood to act in new nonviolent ways when there is a sufficient adaptation made.
The VSA model can also help us understand the intergenerational transmission of violence. It is well understood that those who were maltreated in their childhood are more likely to perpetuate violence in their future romantic relationships and toward their children. This can be thought of as an enduring vulnerability to grow up in a violent home, yet this enduring vulnerability can also be modified by adaptations of the individual that serve to stem the perpetuation of violence.
For this study, we propose that exposure to maltreatment during childhood as an enduring vulnerability leads to resolving conflict in a romantic relationship in more hostile and violent ways, thus leading to IPV. Furthermore, we propose that the higher level of self-esteem, social support, and relationship quality with parents during adolescence moderate the association between child maltreatment experience and the odds of experiencing or perpetrating IPV in adulthood. Moderation effects, if existent, would suggest that adolescents who have a supportive relationship with the family and friends, and higher self-esteem, may develop adaptive coping skills and would therefore show a reduced risk of violence in their relationships, even when dealing with stress or conflictual intimate relationship, such that it minimizes the negative consequences of exposure to child maltreatment.
Review of the Literature
Outcomes of Child Maltreatment and Transmission of Violence
Studies have documented that child maltreatment is a serious threat to children’s emotional and psychological health, including challenges with anxiety, depression, trauma, antisocial behaviors, and physical well-being (e.g., Iratzoqui & Watts, 2019). These symptoms may continue with devastating effects into adulthood (Caykoylu, Ibiloglu, Taner, Potas, & Taner, 2011; Crockett et al., 2015; Sousa et al., 2011 Maxwell, Callahan, Ruggero, & Janis, 2016). Furthermore, experiencing and witnessing domestic violence in childhood can develop into perpetration or victimization of IPV in adulthood (Banyard, Arnold, & Smith, 2000; Black, Sussman, & Unger, 2010; Eriksson & Mazerolle, 2015; Fergusson, Boden, & Horwood, 2006; Iratzoqui & Watts, 2019).
Available research on the transmission of violence has generally been rooted in social learning theory (Bandura, 1977), which posits that parents model violent behavior and children learn and adapt similar behaviors into their own relationships. In addition to modeling violence from family members, an attitude of violence acceptance can be observed from the community and broader context through social norms regarding gender roles, and physical violence against a romantic partner (Debowska, Boduszek, Jones, Willmott, & Sherretts, 2021). Frequent exposure of violence to children and adolescents creates fertile soil for the development of beliefs and behaviors that perpetuate violent behaviors (Lee, Begun, DePrince, & Chu, 2016), and feeling comfortable in romantic relationships where violent attitudes and behaviors exist (Papp, Liss, Erchull, Godfrey, & Waaland-kreutzer, 2017). Furthermore, losing hope from the future; having negative emotions, such as feeling depressed, fearful, and loneliness; and maladaptive coping strategies of those individuals who are exposed to violence are linked with risky lifestyles throughout the life course (Iratzoqui & Watts, 2019).
Even though researchers commonly accept that being exposed to maltreatment during childhood is linked with perpetuating violence in one’s own relationship later in life (e.g., Eriksson & Mazerolle, 2015), a number of studies have shown the relationship between early experience and later perpetration of violence to be far more complex than originally assumed (e.g., Black et al., 2010), and it is clear that not all individuals who were maltreated during childhood continued to live in this vicious cycle (K. M. Anderson & Danis, 2006; Bancroft, Silverman, & Ritchie, 2012). Children’s responses to parental maltreatment vary depending on their risk and vulnerability, as well as the structure of their environments.
Protective Factors as the Moderator of Transmission of IPV
Several factors have been identified in the domestic violence literature as having the potential to buffer the negative outcomes linked with child maltreatment and later risk of IPV. For the present study, we will specifically examine the adolescents’ self-esteem, relationship quality with parents, and social support as the moderators of the future risk of IPV in adult relationships.
Relationship quality with parents
Numerous studies have found an association between parent–child relationship quality and physical aggression in intimate relationships, suggesting that the quality of the parent–child relationship is a key protective factor for young children (Brook, Lee, Finch, & Brown, 2012; Priddis & Howieson, 2010; Tharp & Noonan, 2012). Results of these studies suggested that poor quality of an adolescent’s relationship with parents (e.g., poor parenting, lower level of parental warmth, harsh punishment) has been associated with aggressive behaviors, victimization and perpetration of adolescent dating abuse, and increased risk of future partner violence (Brook et al., 2012; Chen & Foshee, 2015; Makin-Byrd, Bierman, & Conduct Problems Prevention Research Group, 2013). On the contrary, higher quality of parent–child relationships (e.g., high levels of bonding, trust, healthy communication, warmth, empathy, emotional support, and mutual role understanding) has been linked with rejecting abusive relationships, as well as healthier dating attitudes in youth (Raudino, Fergusson, & Horwood, 2013; Tharp & Noonan, 2012), which may also serve as a moderator of the association between childhood exposure to violence and future partner violence among adults. Research on the transmission of IPV also found that strong parent–child bonding was a protective factor against victimization of IPV for youth (Brook et al., 2012; Maas, Fleming, Herrenkohl, & Catalano, 2010; Yan, Howard, Beck, Shattuck, & Hallmark-Kerr, 2010).
Social support
Social support is defined as support received from friends, family, parents, and teachers. Social support is a relevant protective factor against IPV in adult romantic relationships. Social support buffers against stress in a variety of ways, such as higher social support being linked with enhanced self-esteem, more positive perception of stressful events, and increased knowledge of coping skills (Kocot & Goodman, 2003). Researchers have also found that social support is associated with a decrease in depression and an increase in quality of life over time (Beeble, Bybee, Sullivan, & Adams, 2009). In addition to having positive mental health outcomes, social support has also been associated with IPV victims’ behaviors. The domestic violence literature indicates that possessing greater informal social networks (e.g., friends and family) can help victims end abusive relationship (Bosch & Schumm, 2004; Jose & Novaco, 2016; Richards & Branch, 2012, 2013). Furthermore, literature on the cycle of violence has suggested that parents who did break the cycle of abuse from their own family of origins tended to have extensive social supports group or supportive relationship with one of their parents that evoked feeling loved and cared for (Palfai, 2000). Although research regarding the relationship between early social support and later risk of IPV is limited, social support can be considered a factor in providing resources for survivors of IPV, which also may enhance their well-being and coping strategies for preventing IPV.
Self-esteem
Self-esteem refers to recognizing one’s strengths and qualities and having a positive view of oneself (Walker & Knauer, 2011). Empirical research has demonstrated a strong association between self-esteem and IPV in adult relationships (Gonzalez-Guarda, Vermeesch, Florom-Smith, McCabe, & Peragallo, 2013; Matheson et al., 2015; Papadakaki, Tzamalouka, Chatzifotiou, & Chliaoutakis, 2009). Research suggests that children who grow up witnessing family violence are at risk for low self-esteem (Papadakaki et al., 2009; Tajima, Herrenkohl, Moylan, & Derr, 2011) and are linked with anger problems and aggressive behaviors that contribute to IPV (Copeland-Linder, Lambert, & Ialongo, 2010; Papadakaki et al., 2009; Skeen, Macedo, Tomlinson, Hensels, & Sherr, 2016). On the contrary, self-esteem can be a coping ability and protective factor against IPV (Carlson, McNutt, Choi, & Rose, 2002; Edwards, Gidycz, & Murphy, 2011). Individuals with higher self-esteem tended to have more secure relationships, longer involvement with partners, and experience less psychological or emotional abuse (Edwards et al., 2011; Skeen et al., 2016). Although previous studies revealed adults raised in a healthy family environment during their childhood had higher self-esteem (e.g., Gonzalez-Guarda et al., 2013), children who were exposed to family violence tended to improve their self-esteem over time through having social support from parents and close friends (Riesen & Porath, 2004).
Present Study
Although numerous studies have examined the function of these variables in adolescents exposed to maltreatment during childhood, little research has directly investigated the long-term effects of these variables as a buffer against violence on adult intimate relationship. As a result, it is important to investigate factors that can be identified by clinicians and survivors to help reduce their risk for future experiences of IPV (Cattaneo & Goodman, 2005). Therefore, the purpose of this study is to examine (a) the relationship between individuals’ exposure to violence in childhood and future risk of IPV, and (b) the moderating roles of relationship quality with parents, self-esteem, and social support that may disrupt the association between exposure to child maltreatment and experiencing or perpetrating IPV in adulthood. We hypothesize that these protective factors will be associated with lower odds of both experiencing and perpetrating IPV in later adult intimate relationships, among those who were exposed to violence in childhood and adolescence. The VSA model (Karney & Bradbury, 1995) will be used to provide a framework for hypothesizing how these factors will influence the interruption of transmission of IPV.
Method
Participants and Procedures
The National Longitudinal Study of Adolescent Health Survey (Add Health) is a nationally representative longitudinal study of over 20,000 adolescents in Grades 7 to 12 in the United States during the 1994-1995 school year who have been followed through adolescence and their transition to adulthood with four in-home interviews in 1994-1995 (Wave I), 1996 (Wave II), 2001-2002 (Wave III), and 2008-2009 (Wave IV) when they were aged 24 to 32. Add Health includes questions about social, economic, psychological, and physical well-being and places each participant into a social context by asking about their family, community, and school.
The data were collected using an in-school survey from 80 high schools and 52 middle schools. It was followed by an extensive in-home interview with a randomly selected group of students and their parents (as part of Wave I). Ultimately, this entire sample of adolescents was followed into young adulthood with in-home interviews, with the final wave (Wave IV) taking place in 2008 when the sample was between the ages of 26 and 32.
For this study, data were taken from the first, third, and fourth waves of the Add Health public-use data set using a sample of 3,193 participants across 14 years. To assess the variables of interest over the entire length of data collection, only participants who had data at Waves I, III, and IV were included in analyses. The final operational sample included 1,447 male and 1,746 female participants. Descriptive statistics from Wave I included race and religious groups. From among the participants, 45% were White, 32% were Black, 8% were American Indian, and 5% were Asian. In regard to religious affiliation, 96% of the participants were Christian, 0.8% were Jewish, 0.4% were Buddhists, and 0.3% were Muslim. At Wave IV, participants reported their relationship status, educational levels, and household income. In this sample, 64% of the participants were married, 19% were cohabiting, and 10% were currently dating. The majority of participants attended college with 48.6% of participants holding a bachelor’s degree and 12.4% holding an associate’s degree. In this sample, 26% of the participants reported an annual household income of less than US$5,000; 36% of the participants earned between US$5,000 and US$19,999; 26% of the participants earned between US$20,000 and US$39,999; 10% of the participants earned between US$40,000 and US$74,999; and only 1% earned between US$75,000 and US$99,999.
Measures
Childhood exposure to maltreatment
Information on child maltreatment was not collected at Wave I; however, early exposure to maltreatment was measured at Wave III by the question “How often their parents or other adult caregivers slapped, hit, kicked, or neglected them by the time they started the sixth grade,” and the response categories were coded as follows: 0 = this has never happened, 1 = 1 time, 2 = 2 times, 3 = 3 to 4 times, 4 = 6 to 10 times, 5 = more than 10 times.
Perpetration of IPV in adulthood
At Wave IV, the participants’ perpetration of violence was assessed with four items. During the Wave IV interview, the following questions were asked: Participants were asked the frequency of psychical and/or sexual violence (e.g., hitting, kicking, pushing, shoving, throwing, slapping, threatening, having injury, and unwanted sex) that was committed from the participant toward the partner. The items were originally coded between 0 = never and 7 = more than 20 times in last year of the relationship. However, due to exceptionally few incidences of reported violence, and extremely skewed data, this measure was recoded such that 0 (no perpetrating behaviors) and 1 (perpetrating behaviors reported). The alpha coefficient of this variable before recoding was α = .83.
Victimization of IPV
During the Wave IV interviews, respondents were asked four questions about the frequency of psychical and/or sexual violence (e.g., hitting, kicking, pushing, shoving, throwing, slapping, threatening, having injury, and unwanted sex) that was committed by the current partner against them. Similar to the coding of perpetration of violence, victimization of violence also had limited people who reported victimization. Thus, although the scale was originally coded between 0 = never and 7 = more than 20 times in last year of the relationship, this was recoded such that 0 (no victimization experience) and 1 (experiencing victimization). The alpha coefficient of this variable before recoding was α = .67.
Relationship quality with parents
Relationship quality of the child with both parents was assessed at Wave I by four statements: “Your mother is warm and loving toward you,” “Your mother encourages you to be independent,” “You are satisfied with your relationship with your mother,” and “You communicate with each other.” The same questions were also asked about the relationship with fathers. The response categories were coded between 1 = strongly agree and 5 = strongly disagree. These items were all reverse coded for subsequent analyses. A total of eight items (four for mother and four for father) were used. The mean of all eight items was taken, and higher scores indicated greater perceived relationship quality with parents. The alpha coefficient was α = .83.
Social support
Four questions were used from Wave I to assess the social support of participants. The question items included, “How much do you feel that adults care about you?” “How much do you feel that your teachers care about you?” “How much do you feel that your friends care about you?” and “How much do you feel that your family care about you?” The response categories were coded between 1 (not at all) and 5 (very much). The mean of these items was computed. Higher scores indicated higher levels of social support. The alpha coefficient for this measure was α = .65.
Self-esteem
Self-esteem was measured by three items, “you have a lot of good qualities,” “a lot to be proud of,” and “just as good as other people,” at Wave I. Response categories were coded between 1 (strongly agree) and 5 (strongly disagree). Then these items were reverse coded for subsequent analyses. The mean of these items was computed. Higher scores of this scale represented a higher level of self-esteem. The alpha coefficient for this measure was α = .76.
Analytic Strategy
To examine the link between child maltreatment with later perpetration and victimization of violence moderated by social support, relationship quality with parents, and self-esteem, a path analysis was tested that included main effects and interaction effects. The outcome variables—IPV perpetration and victimization in adulthood—were predicted by the main effects of child maltreatment, relationship quality with parents, social support, and self-esteem, as well as the interaction effects of Child Maltreatment × Relationship Quality, Child Maltreatment × Social Support, and Child Maltreatment × Self-Esteem. Variables predicting these two dichotomous outcome variables were estimated as odds ratios (OR), the odds of experiencing or not experiencing violence in adulthood. Predictor and moderator variables were standardized, and interaction terms were computed from taking the product of these standardized variables. Significant interaction terms from the output would indicate that these moderators significantly altered the expected association between child maltreatment in adolescence and later violence victimization and perpetration toward a partner. Any significant interaction terms will be plotted at one standard deviation high and low for the predictor and moderator. Path analysis was chosen as the preferred analysis to test this model because we had two outcome variables and because all variables were modeled as observed variables. The outcome variables were specified as dichotomous, which provided ORs for the prediction model. There are no model fit indices to report because Mplus does not provide model fit indices if there are any dichotomous or categorical outcome variables. Data were analyzed using IBM SPSS Version 22 and Mplus (Muthén & Muthén, 1998). Full information maximum likelihood (FIML) was used to test the model, estimate parameters, and handle missing data (Acock, 2005).
Results
Correlation
Table 1 provides the means, standard deviations, range, and reliability information about the variables for the whole sample. The mean level of child maltreatment was 0.72 (SD = 1.43), indicating that, on average, a maltreatment behavior had occurred at least one time by the age of 11 to 12. The mean level of relationship quality with parents was 4.64 (SD = 0.54), indicating a relatively low parent–child relationship quality; social support was 4.00 (SD = 0.61), suggesting a high level of social support; and self-esteem 4.30 (SD = 0.59), indicating a relatively low level of self-esteem among participants at Wave I. At Wave IV, 83% of the sample reported perpetrating IPV and 76% reported experiencing IPV. Correlations were initially assessed to identify associations between all variables, and are reported in Table 2. Based on correlation results, perpetration of IPV in adulthood was negatively related to adolescents’ social support (r = −.10, p < .01), relationship quality with parents (r = −.05, p < .01), and self-esteem (r = −.05, p < .01) in adolescence. In addition, later risk of victimization of IPV was significantly associated with the adolescents’ social support (r = −.10, p < .01) and relationship quality with parents (r = −.05, p < .01).
Descriptive Statistic for Study Variables (N = 3,193).
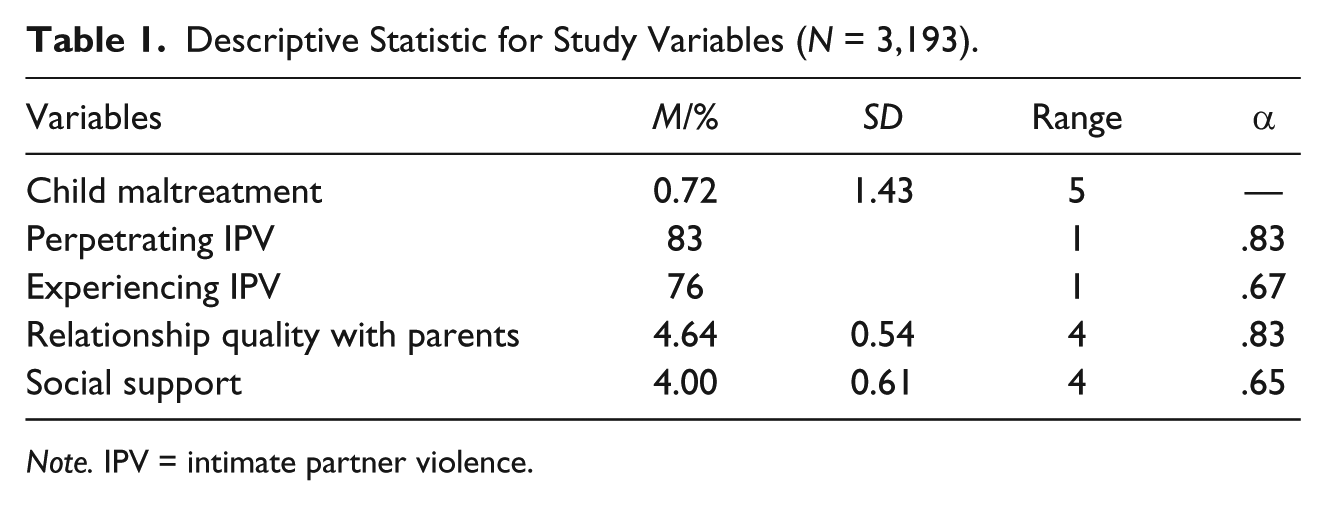
Note. IPV = intimate partner violence.
Correlations Among Variables (N = 3,193).
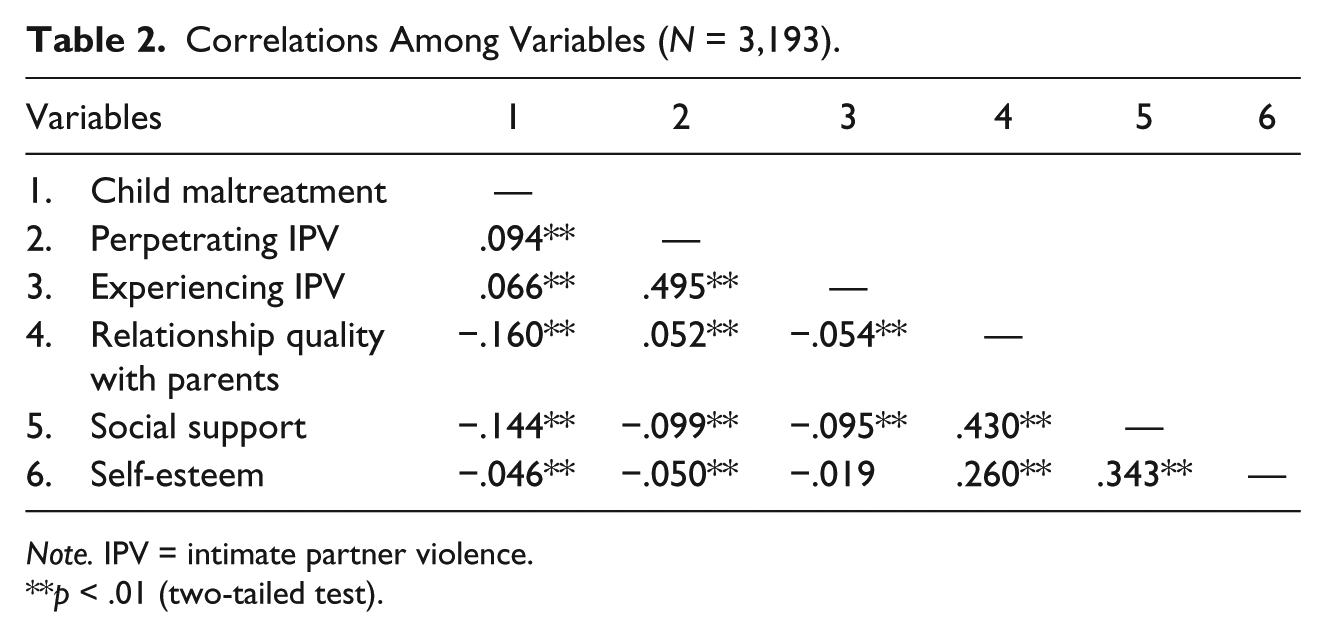
Note. IPV = intimate partner violence.
p < .01 (two-tailed test).
Path Analysis
Moderation effects in this model were tested by using two logistic regression analyses simultaneously in a path analysis with main effects and interaction effects (see Figure 1). Table 3 provides the results from our model. The model included all path coefficients between predictors and outcomes. We found that exposure to maltreatment in childhood was significantly associated with an increased likelihood of later adult perpetration of IPV by 16% (b = .15, p < .001, OR = 1.16) and victimization by 10% (b = .10, p < .05, OR = 1.10). More specifically, a one-unit increase in child maltreatment predicted a 10% increase in the odds of becoming a victim of IPV, and a 16% increase in the odds of acting violently to an intimate partner in adulthood. Furthermore, a higher level of social support in adolescence was associated with a 26% reduction in the odds of being a victim of IPV in adulthood (b = −.30, p < .001, OR = .74) and a 24% reduction in the odds of being a perpetrator of IPV (b = −.28, p < .001, OR = .76). Although there was a main effect between social support in adolescence and later perpetrator and victimization of IPV, social support, like the other two moderators (i.e., relationship quality with parents and self-esteem), did not moderate the association between early exposure to violence and later violence.

Path analysis model.
Summary of Path Analysis Predicting Perpetration and Victimization of IPV in Adulthood (N = 3,193).

Note. IPV = intimate partner violence; OR = odds ratio.
p < .001.
Discussion
The present study sought to examine the possible moderating effects of relationship quality with parents, social support, and self-esteem between the association of being maltreated during childhood and the later risk of behaving violently in romantic relationships or being a victim of violence in romantic relationships. We found that there was a positive association between child maltreatment and IPV perpetration and victimization in adulthood, although the proposed moderators did not significantly mitigate these risks. However, social support in adolescence was identified as a significant predictor of lower odds of violence in adult relationships. We found that less violent behaviors within their young adult intimate relationships were associated with more support from adults, teachers, friends, and family in adolescence. Furthermore, we found that receiving support from adults, teachers, friends, and family was related to engaging in less violent relationships in adulthood.
The present study revealed that the association between reported child maltreatment and both experiencing and perpetrating violent behaviors later in life was positively correlated. In other words, maltreatment in the family of origin in childhood increased the risk of both violence perpetration and victimization in adult relationships. Our findings were consistent with the previous literature that claims early exposure to violence in the family of origin may lead to the transmission of violence later (e.g., Eriksson & Mazerolle, 2015). This result can be explained by the VSA model (Karney & Bradbury, 1995). Child maltreatment may contribute to developing two “enduring vulnerabilities” later in adult life: acting violently and being a victim of violence. The adaptive responses we tested as moderators were not strong enough to meaningfully alter the expected risk of the transmission of child maltreatment into later IPV in adulthood.
The lack of significant findings in our model examining the moderators (e.g., having high self-esteem, supportive social support, and close relationship with parents) of the association between child maltreatment and later violence was unexpected. This may be due in part because each of these moderators were assessed during adolescence, and the protective effect from these factors may not continue into early adulthood. It may be that protective factors for young adults in the present serve as better moderators than protective factors from adolescence.
In addition, the present study highlights a noticeable direct association that reinforces previous literature. According to our results, there is a negative association between social support in adolescence and the risk of future IPV victimization and perpetration. In other words, support from peers, teachers, and family during adolescence is associated with a lower risk of both acting violently and experiencing violence in adult romantic relationships. As suggested in previous studies, having social support is an important coping strategy to leave from a violent relationship (e.g., D’Andrea & Graham-Berman, 2017), but it may also prevent, to some extent, developing new romantic relationships in adulthood with partners at higher risk of experiencing IPV. Although limited studies have reported the association between early social support and later perpetration of IPV, our study results suggest the possibility that having strong social ties in adolescence may prevent adults from being a perpetrator of IPV. We speculate that supportive peers and adults, such as teachers and family members, who provide safety, acceptance, help, and advice may aid adolescents in dealing with personal problems. Furthermore, when adolescents perceive support and care from their loved ones, they can use that mental representation of how relationships should be to help them judge the viability of potential later romantic relationships based on this perceived image of how a partner should treat them.
Limitations and Further Research
There are several limitations that should be noted. One important limitation of this study is the age of data; the final wave of data collection was in 2008 and 2009. Thus, current populations may differ somewhat from the effects found in this sample 10 years ago. Second, this study is subject to retrospective reporting bias, as the measure used in this study assessing violence in adolescence at home was asked not during adolescence but in young adulthood. It has been established when researching socially undesirable behavior, there could be underreporting (Cui, Lorenz, Conger, Melby, & Bryant, 2005). Thus, this may have resulted in lower estimates of the association between early exposure to IPV and later IPV perpetration.
Third, the Add Health study did not use a formal measure of IPV. The questions about parental maltreatment at home generally related to neglect and physical violence. At Wave III, when participants were between the ages of 18 and 24 years, they were asked to report on occurrences after a significant time lapse (e.g., “by the time you started sixth grade. . .”). It is possible that this measure might have been influenced by current events, which could increase recall bias (Cui, Ueno, Gordon, & Fincham, 2013). Similarly, it would have been preferable to have a more standardized and comprehensive measure of violence than the items available in this data set. Another limitation of this study was the measure for relationship quality with parents. For the current study, we measured both mother and father relationship with the child to assess overall relationship quality with parents; however, future studies could separately measure the relationship quality with mother and father. It is possible one parent may be closer to the child than the other parent and this may differentially buffer the effects of maltreatment differentially by parent.
Finally, the current study did not use any control variables as they were not the focus of the current study. Future studies could examine the possible protective factors by controlling some variables such as gender, race, residing state, and education level that might serve to moderate risk for future IPV in adulthood.
Clinical Implications
These results have some implications for prevention of IPV victimization and perpetration. Social support was associated with the lower risk of both victimization and perpetration of IPV. Thus, clinically improving the interpersonal relationship of adolescents may reduce violence in later life to some extent. Clinicians should be aware that weak ties or poor relationships with the social environment in adolescence might be connected to both violent behavior and staying in a violent relationship into adulthood. Therefore, interventions could seek to enhance social bonds between adolescents with adults, teachers, and friends. Group therapy can be considered particularly beneficial for adolescents who have been maltreated in childhood. Through group therapy, adolescents can receive emotional support from their peers; feel accepted, wanted, and valued; and learn effective coping skills, conflict resolution skills, and social skills (Levitan, 2013).
Furthermore, to reduce current violence and future violence, improving parent–child relations and increasing self-esteem in adolescence may play a part in the solution. However, our results showed that even if children have high self-esteem or strong bonds with parents, as long as they live within a violent family environment, there is a risk of acting violently or becoming involved in a violent relationship in the future. Thus, our results suggest that clinicians who work with adolescents to improve their generalized sense of support from others may also be playing a role in reducing adult IPV. Finally, interventions should seek to provide psychoeducation for parents about the effects of domestic violence on their children, child development, and parenting skills (Levitan, 2013).
Conclusion
Intergenerational perpetuation of violence is a serious concern. Using a sample of 3,193 participants across 14 years, we tested several protective factors that may disrupt the association from maltreatment in childhood to experiencing and perpetrating violence later on in adult relationships. Our study found that there was a significant positive association between child maltreatment and adult perpetration and victimization of IPV. At the same time, having a good relationship with friends in adolescence was linked with both a lower risk of being a victim and a perpetrator of IPV in adulthood. Although the proposed moderators did not interact with exposure to violence in adolescence to reduce later risk of behaving violently and being a victim of violence, social support was identified as a predictor of lower levels of violence in adult relationships.
Footnotes
Authors’ Note
Yile Su is now affiliated with Florida State University, Tallahassee, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.