
Abstract
The current study examined the mediating role of affect dysregulation, maladaptive personality traits, and negative urgency in the association between childhood cumulative trauma (CCT) and psychological intimate partner violence (IPV). A total of 241 men and women from the general population answered self-report questionnaires assessing these variables. Results indicated that 70% of participants reported at least two different types of childhood trauma, while, over the past year, 80% indicated having perpetrated or experienced psychological IPV. Path analyses of a sequential mediation model confirmed that the CCT–IPV association is explained by affect dysregulation, maladaptive personality traits, and negative urgency. These findings support the need to assess affect regulation and personality traits in CCT survivors. Psychosocial interventions should aim to increase self-soothing skills and decrease negative urgency to prevent psychological IPV.
The majority of current policies and practices developed to address intimate partner violence (IPV) in Canada, the United States, and the United Kingdom often have their foundations in feminist theories, and the specific interventions tend to be based on the Duluth model (Pence & Paymar, 1993). Research has demonstrated that the theoretical underpinnings of these approaches are partially flawed (e.g., Bates, Graham-Kevan, & Archer, 2014) and that they are not always effective (e.g., Babcock, Green, & Robie, 2004). In the face of these challenges, when assessing and treating violent men, a growing number of researchers emphasize the need to take into account other variables such as the history of childhood interpersonal trauma (CT) and associated psycho-emotional sequelae (Fisher, Goodwin, & Patton, 2009; Godbout, Dutton, Lussier, & Sabourin, 2009; Sonkin & Dutton, 2003).
CT includes the experience of physical, psychological, and sexual abuse; physical and psychological neglect; witnessing physical or psychological interparental violence; and peers’ bullying during childhood and adolescence (Godbout, Briere, Sabourin, & Lussier, 2014). Recent studies have shown that CT is associated with a higher risk of sustaining (Lilly, London, & Bridgett, 2014) and perpetrating (Brassard, Darveau, Péloquin, Lussier, & Shaver, 2014) psychological IPV in adulthood. However, it has been suggested that examining single CT experiences separately may not be the optimal way to understand the long-term consequences of CT. In addition, considering that most children who experience CT tend to sustain additional victimization in relationships (Finkelhor, Ormrod, & Turner, 2007), the experience of multiple types of early CT, known as cumulative CT or childhood cumulative trauma (CCT), and its effect on IPV warrant further examination.
Psychological IPV refers to the use of verbal and nonverbal communication to emotionally harm and/or exert control over one’s partner (Breiding, Basile, Smith, Black, & Mahendra, 2015). Psychological violence is the most prevalent form of IPV in the general population, with prevalence rates reaching 57% in couple partners, and is equally high in men and women (Breiding et al., 2015; Hellemans, Loeys, Dewitte, Smet, & Buysse, 2015). In addition to its deleterious impact on couples’ well-being, psychological IPV is also recognized as a precursor to other forms of violence within relationships (Frieze, 2005). Still, this form of violence is rarely analyzed separately from other forms of IPV, and very few studies have examined the presence and underlying mechanisms of its associations with CCT (Dugal, Godbout, Bélanger, Hébert, & Goulet, 2018).
The current study was inspired by the empirically based theoretical framework proposed by Holtzworth-Munroe and Stuart (1994). In identifying subtypes of male batterers, the authors isolated two types of perpetrators of IPV that were more likely to report a history of CT: the dysphoric/borderline perpetrator and the violent/antisocial perpetrator. Despite distinguishing features, these two classes of individuals shared a tendency to react without thinking to negative affects despite the likelihood that these actions may result in adverse consequences. This phenomenon has been described as negative urgency (Whiteside & Lynam, 2001) and is associated with affect dysregulation and maladaptive personality traits. Thus, these three variables were retained as hypothetical mediators and are introduced below.
Affect Dysregulation
Affect dysregulation is a multidimensional construct that encompasses both a cognitive and a behavioral dimension (Berzenski & Yates, 2010). Cognitively, it refers to the inability to control and tolerate strong and negative emotions, as well as to inhibit mood swings without resorting to avoidance strategies (Briere, 2002). Behaviorally, it reflects the inability to refrain from externalizing those emotions through dysfunctional behaviors such as self-harm, substance abuse, impulsivity, or violent behaviors (Briere & Runtz, 2002).
CT could hamper the development of affect regulation skills by exposing children to extreme emotional demands while simultaneously preventing them from learning how to tolerate distress and control its expression (Gratz, Paulson, Jakupcak, & Tull, 2009). It has already been shown that adult survivors of CCT are more likely to resort to dysfunctional or impulsive strategies to numb negative affects or to reduce their impact and duration (Briere, Hodges, & Godbout, 2010). As violence is often an impulsive strategy used to deal with negative affect triggered by relational conflicts (Ruddle, Pina, & Vasquez, 2017), affect dysregulation is likely to be a mechanism partly explaining why CCT survivors are at higher risk of perpetrating IPV in adulthood. Affect dysregulation could also heighten the risk of sustaining IPV due to difficulties in detecting risky situations (e.g., inability to identify and respond to dangerous situations in an assertive or escape-focused manner; Walsh, Gonsalves, Scalora, King, & Hardyman, 2012). Yet, these hypotheses remain to be tested.
Maladaptive Personality Traits
When Paulhus and Williams (2002) introduced the notion of a Dark Triad, they discussed a set of three socially aversive or maladaptive personality traits widely distributed across the general population at a subclinical level: Machiavellianism, psychopathy, and narcissism (Savard, Lussier, Sabourin, & Brassard, 2014). Machiavellianism describes individuals who are cunning, selfish, and who do not hesitate to use others to further their own ends (Paulhus & Williams, 2002). Psychopathic individuals are generally dishonest, insensitive, and impulsive; they present antisocial behaviors, a lack of remorse, anxiety, and empathy, and they hardly tolerate frustration (Savard et al., 2014). Narcissism characterizes those who believe they are superior and who seek attention, prestige, or admiration from others (Savard et al., 2014).
The antisocial and impulsive behaviors that characterize these maladaptive personality traits have been argued to result from the influence of environmental risk factors such as the experience of abuse and neglect during childhood (Schimmenti, Passanisi, Di Carlo, & Caretti, 2015). Poythress, Skeem, and Lilienfeld (2006) also showed that CCT was associated with psychopathic and antisocial personality traits, but that this relationship was specific to the impulsive lifestyle features of these personality traits. Maladaptive personality traits have also been associated with both perpetration and victimization of psychological IPV (Carton & Egan, 2017) through insensitivity to others’ experience during conflict and a tendency to react impulsively and aggressively to negative emotions (Long, Felton, Lilienfeld, & Lejuez, 2014).
Negative Urgency
Negative urgency, a dimension of impulsivity, has been associated with numerous maladaptive behaviors performed in response to negative emotions, such as psychological IPV in adulthood (Shorey, Brasfield, Febres, & Stuart, 2011). In addition, for CCT survivors, the experience of maltreatment is positively associated with negative urgency (Gagnon, Daelman, McDuff, & Kocka, 2013). Yet, although CCT would appear to act as a risk factor for negative urgency, the specific mechanisms behind this association are not fully understood. According to Gaher, Arens, and Shishido (2015), deficits in affect regulation could partly explain the development of negative urgency in CT survivors. Thus, negative urgency can be considered as a central feature of the behavioral impact of affect dysregulation (Weiss, Tull, Viana, Anestis, & Gratz, 2012). Individuals with a history of CCT and who present maladaptive personality traits are also considered to have a dispositional tendency to show impulsive behaviors (Malesza & Ostaszewski, 2016; Paulhus & Williams, 2002). Therefore, affect dysregulation and maladaptive personality traits, which heighten the propensity to exert impulsive behaviors when failing to cope with negative emotions, could act as mechanisms through which CCT survivors experience psychological IPV.
Aims of the Current Study
Research has shown that not all survivors of CCT become IPV perpetrators or are revictimized in their romantic relationships (Dugal et al., 2018). Thus, there is a need to explore the mechanisms that might mediate the relationship between CCT and psychological IPV in adulthood. Despite previous literature demonstrating significant associations between CT, affect dysregulation, maladaptive personality traits, negative urgency, and psychological IPV, none have yet examined their relations simultaneously in an integrative model. In addition, studies that have examined these links have rarely considered cumulative CT (Gratz et al., 2009), included both perpetrated and sustained psychological IPV (Lilly et al., 2014), distinguished psychological IPV from physical IPV (Berzenski & Yates, 2010), or approached the study of these variables in a gender-inclusive way (Gratz et al., 2009); the current study will address these issues and allow a complex and dynamic understanding of these phenomena.
The current study aims to examine the mediating role of affect dysregulation, maladaptive personality traits, and negative urgency in the association between CCT and psychological IPV perpetration and victimization. We tested a multivariate integrative model providing preliminary, cross-sectional support for such a model. As suggested in previous researches (Berzenski & Yates, 2010; Dugal et al., 2018), this study will also examine whether the relationship between CCT and perpetrated or sustained psychological IPV is mostly driven by the behavioral impacts of CCT or by its more affective or personality repercussions. It is expected that CCT will be associated with higher affect dysregulation and maladaptive personality traits, which will heighten negative urgency in CCT survivors and, in turn, lead to higher levels of psychological IPV perpetration and victimization. Acknowledging the dynamic and often bidirectional nature of IPV in the general population (Langhinrichsen-Rohling, Misra, Selwyn, & Rohling, 2012), it is hypothesized that perpetrated and sustained psychological IPV will be positively correlated in the model.
Method
Participants and Procedure
A total of 241 participants (62 men and 179 women) were recruited to answer an anonymous online survey. Participants had to be over 18 years old, speak French, and involved in an intimate relationship for at least 6 months. The mean age was 28.8 years (SD = 10.1, range = 19-65). The sample comprised full-time workers (36.1%), part-time workers (8.8%), students (54.2%), or retirees (0.8%). Participants were married (14.5%), cohabiting (49.4%), or dating a regular partner (36.1%). For their education, 2.1% of participants held a high school diploma, 26.6% attained a college or professional studies degree, 47.3% completed undergraduate studies, and 24.1% completed graduate studies, demonstrating a high proportion of high-educated participants in this sample. A total of 47.5% reported an annual income of CAD$19,999 or less, 21.3% reported an income between CAD$20,000 and CAD$39,999, and 31.2% reported an income of CAD$40,000 or more, which indicated a high proportion of low-income participants.
Invitations for participating in the study described as an exploration of early experiences and romantic relationships were shared through social networks (e.g., Facebook, Twitter). The research questionnaires were managed by the authors’ research team and sent to electronic mailing lists of universities’ faculty, staff, and students, as well as to electronic mailing lists of various research associations in the Canadian province of Quebec. As approved by the Institutional Review Board of the University du Québec à Montréal, participants were asked to complete a consent form and the research questionnaires without consulting their partner. No compensation was offered to participants. Results of an a priori G*Power 3 analysis (Faul, Erdfelder, Buchner, & Lang, 2009) indicated that a sample size of 241 participants was sufficient to detect a weak-to-moderate association between CT and IPV, based on results from Smith-Marek et al. (2015), with a standard Type I error rate (α = .05) and a power of .80.
Measures
Demographics
A demographic questionnaire gathered information on participants’ age, sex, occupation, relational status, sexual orientation, level of education, and annual income.
CCT
Participants were administered a French version of the Childhood Cumulative Trauma Questionnaire (CCTQ; Godbout, Bigras, & Sabourin, 2017), a self-report questionnaire assessing eight types of CT (physical, psychological, and sexual abuse; physical and psychological neglect; witnessing physical and psychological violence; and bullying). This measure was adapted from existing questionnaires (e.g., Early Trauma Inventory–Self-Report, Bremner, Bolus, & Mayer, 2007; Childhood Maltreatment Questionnaire, Godbout et al., 2009) and showed satisfactory psychometric qualities (e.g., Bigras, Godbout, Hébert, & Sabourin, 2017). Items for physical and psychological abuse were rated on a 7-point Likert-type scale ranging from 0 (never) to 7 (almost every day), indicating the annual frequency of each type of maltreatment experienced. In the current sample, Cronbach’s alpha for physical abuse was .74 and for psychological abuse was .91. Childhood sexual abuse was measured through two checklist questions assessing whether participants experienced, before the age of 18, any unwanted sexual contact (e.g., touching, penetration) with any person or experienced any sexual contact with a person who is 5 years older or in a position of authority (e.g., parents, teachers). Witnessing interparental physical and psychological violence was measured by two items; one item was used to assess physical neglect, whereas three items were used to measure psychological neglect (α = .82). Bullying was examined using one item based on the Centers for Disease Control and Prevention definition (Gladden, Vivolo-Kantor, Hamburger, & Lumpkin, 2014). To assess CCT, each scale previously mentioned was dichotomously coded (0 = absence, 1 = presence) and summed up to obtain a continuous score, ranging from 0 to 8, indicating the number of different types of CT experienced. This is in line with the literature where CCT is operationalized as the total number of different types of trauma experienced (Briere et al., 2010).
Affect dysregulation
Affect instability and affect skills deficits were assessed using nine items from a French adaptation (Bigras, Godbout, & Briere, 2015) of the affect dysregulation scale of the Inventory of Altered Self-Capacities (IASC; Briere, 2000). Participants indicated how frequently they experienced different affect regulation difficulties over the past 6 months on a 5-point Likert-type scale ranging from 1 (never) to 5 (very often). Total scores ranged from 9 to 45, with higher scores reflecting affect regulation difficulties. Transformation of the scores into t scores allowed to determine whether participants were above or below the clinical cutoff of 70 (Briere, 2000). In the present study, Cronbach’s alpha was .92, a value consistent with that of the original standardized and validated scale (Briere & Runtz, 2002).
Maladaptive personality traits
The French and validated version (Savard, Simard, & Jonason, 2017) of the 12-item Dark Triad Dirty Dozen (Jonason & Webster, 2010) was used to measure Machiavellianism, psychopathy, and narcissism. Participants indicated how much they agreed with each item, on a Likert-type scale ranging from 1 (disagree strongly) to 9 (agree strongly), with statements such as the following: “I have used deceit or lied to get my way” (Machiavellianism), “I tend to lack remorse” (psychopathy), and “I tend to expect special favors from others” (narcissism). Scores on each subscale were standardised (z scores) and averaged to create a composite Dark Triad score indicating the presence of maladaptive personality traits, as proposed by Jonason, Li, Webster, and Schmitt (2009) and Jonason, Li, and Teicher (2010), and depicting generally callous, manipulative, and antisocial traits. The internal consistency coefficients from the original standardized (Jonason & Webster, 2010) and the French validated scale (Savard et al., 2017) were replicated in the current sample with a Cronbach’s alpha of .90.
Negative urgency
The negative urgency scale (the tendency to react without thinking to negative affect) of the abridged and French validation (Billieux et al., 2012) of the UPPS Impulsive Behavior Scale (Whiteside & Lynam, 2001) was used. This scale includes four items rated on a Likert-type scale ranging from 1 (disagree strongly) to 4 (agree strongly): “When I am upset I often act without thinking,” “In the heat of an argument, I will often say things that I later regret,” “I often make matters worse because I act without thinking when I am upset,” and “When I feel rejected, I will often say things that I later regret.” In its French version, the negative urgency scale showed good internal consistency (Billieux et al., 2012), and in the current sample, the reliability estimate was high (Cronbach’s α = .88).
IPV
Inflicted and sustained psychological IPV were assessed using items from the French adaptation (Hébert & Parent, 2000; Lussier, 1997) of the Revised Conflict Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) and a back-translation of the Coercive Control Scale (Johnson, Leone, & Xu, 2014). As no French version of the Coercive Control Scale was developed at the time of the study, a French translation of the questionnaire was created, back-translated to English, and approved as equivalent by a group of three bilingual people. Using items from the psychological IPV subscale of the CTS2, participants were asked the frequency, during the last year, at which they inflicted and sustained psychological violence (insulting, yelling, or threatening) to their partner on a 6-point Likert-type scale ranging from 0 (this never happened) to 6 (more than 20 times during the past 12 months). Coercive control was assessed using nine “yes–no” items indicating the use of nonviolent control tactics used by the participant and his or her partner, including “Tries to limit your contact with family and friends” and “Prevents you from knowing about or having access to the family income even when you ask.” For the purpose of this study, items from the CTS2 were dichotomized, as per the authors’ recommendations (Straus et al., 1996), and added to the total score of the Coercive Control Scale to create composite variables of frequency of exposure to perpetrated and sustained psychological IPV. The internal consistencies of the original measures were replicated in the current sample with adequate reliability for both perpetrated (α = .70) and sustained (α = .76) psychological IPV.
Statistical Analyses
Descriptive analyses and correlations were conducted using SPSS 22. To test the hypothesized model (Figure 1), path analyses were conducted using Mplus, version 7 (Muthén & Muthén, 1998-2012) which is robust to non-normality and accounts for missing data through the use of maximum likelihood estimation with robust standard errors (MLR). Model fit was assessed using the comparative fit index (CFI; Bentler, 1990), the root mean square error of approximation (RMSEA; Steiger, 1990), the standardized root mean square residual (SRMR), the chi-square statistic, and the ratio of chi-square to degrees of freedom (χ2/df). A combination of a nonstatistically significant chi-square value, a CFI value of .90 or higher, an RMSEA value below .06, an SRMR value below .08, and a χ2/df less than 3 indicate good fit (Hu & Bentler, 1999; Kline, 2011; Ullman, 2001). To examine the mediational roles of affect dysregulation, maladaptive personality traits, and negative urgency, the magnitude and significance of direct effects (i.e., path coefficients from CCT to perpetrated and sustained psychological IPV), as well as indirect effects (i.e., the product of the path coefficients from CCT to maladaptive personality traits, from maladaptive personality traits to negative urgency, and from negative urgency to perpetrated psychological IPV), were computed using 95% bootstrap confidence intervals (MacKinnon & Fairchild, 2009). Bootstrap confidence intervals were used to examine the indirect effects of affect dysregulation and maladaptive personality traits on negative urgency in a mediators’ series to predict psychological IPV perpetration and victimization. This bias-corrected method is based on a distribution of the product of coefficients and generates confidence limits of the value of the coefficient for indirect effects. Finally, the proportions of the total effect that were mediated through affect dysregulation, maladaptive personality traits, and negative urgency (indirect effect/total effect) were measured.
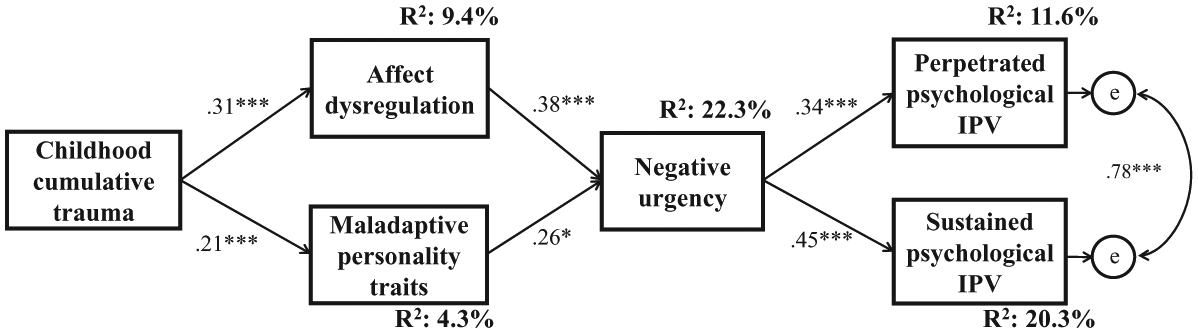
Path analysis of the role of affect dysregulation, maladaptive personality traits, and negative urgency in the relationship between childhood cumulative trauma and psychological IPV perpetration and victimization.
Results
Descriptive Statistics
Descriptive statistics are presented in Table 1. In the sample, 70.1% (n = 169) of participants reported having experienced at least two different types of CT. The number of different types of maltreatment experienced and the prevalence of all types of CT were similar across gender, except for physical abuse and bullying which were more highly endorsed by men. The mean scores for affect dysregulation did not significantly differ across gender. A total of 22.0% of participants (n = 53) scored above the clinical cutoff for affect dysregulation. Mean scores for Machiavellianism and psychopathy were significantly higher in men than in women, but did not significantly differ for narcissism. Scores on the negative urgency scale also did not differ across gender. Among participants, 79.7% (n = 192) reported at least one instance of psychological IPV perpetration toward their partner over the past 12 months, while 80.5% (n = 194) reported IPV victimization. Mean scores for the frequency of IPV perpetration and victimization did not differ across gender and indicated a mean frequency of 11 to 20 experiences of psychological violence in the past year.
Means, Prevalences, and Gender Differences for Study Variables.
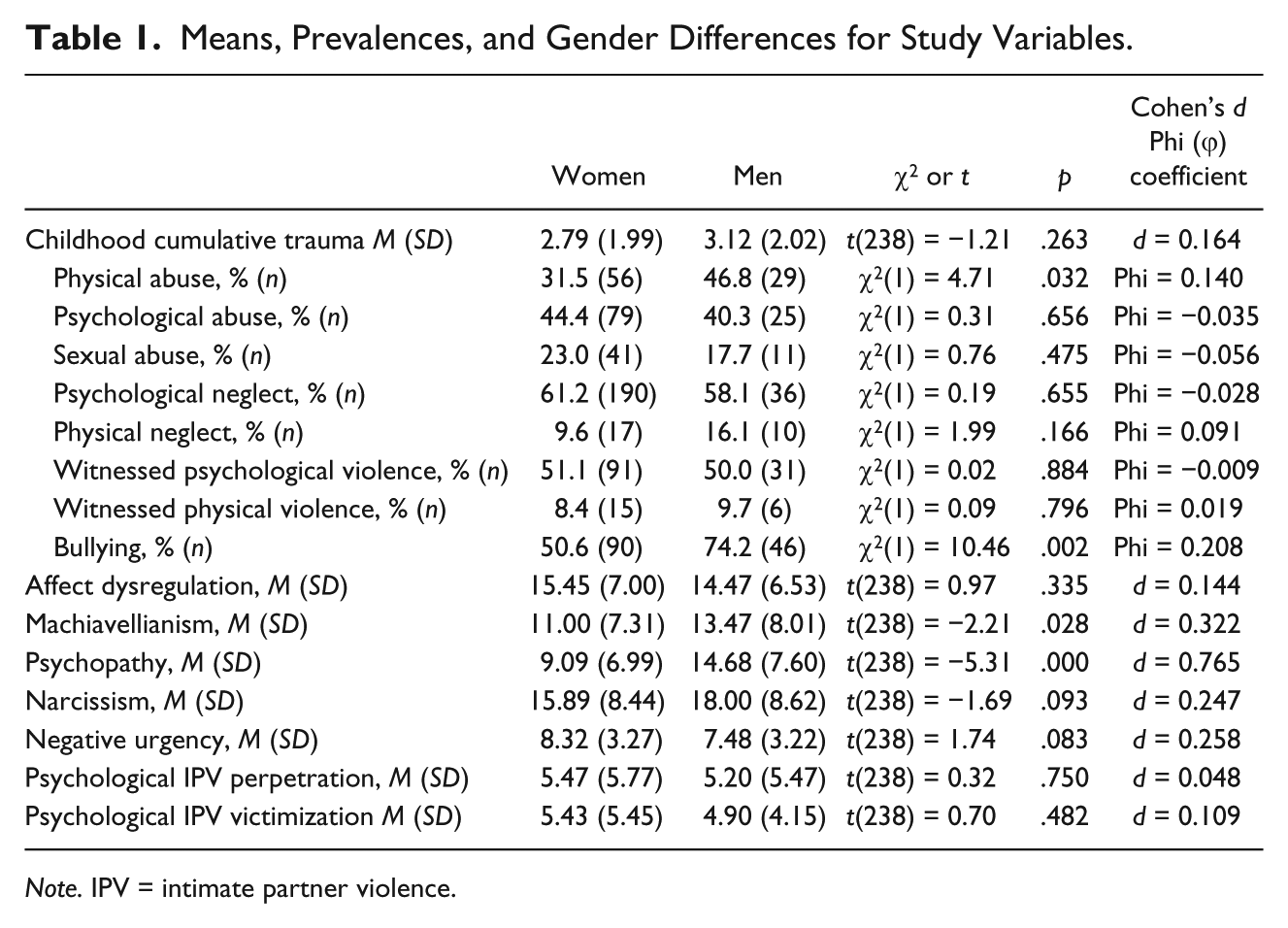
Note. IPV = intimate partner violence.
Correlations
Bivariate correlations among CCT, affect dysregulation, maladaptive personality traits, negative urgency, and perpetrated and sustained psychological IPV are presented in Table 2. Statistically significant correlations were found between all variables, except between affect dysregulation and maladaptive personality traits.
Correlations Between Childhood Cumulative Trauma, Affect Dysregulation, Maladaptive Personality Traits, Negative Urgency, and Perpetrated and Sustained Psychological Intimate Partner Violence.
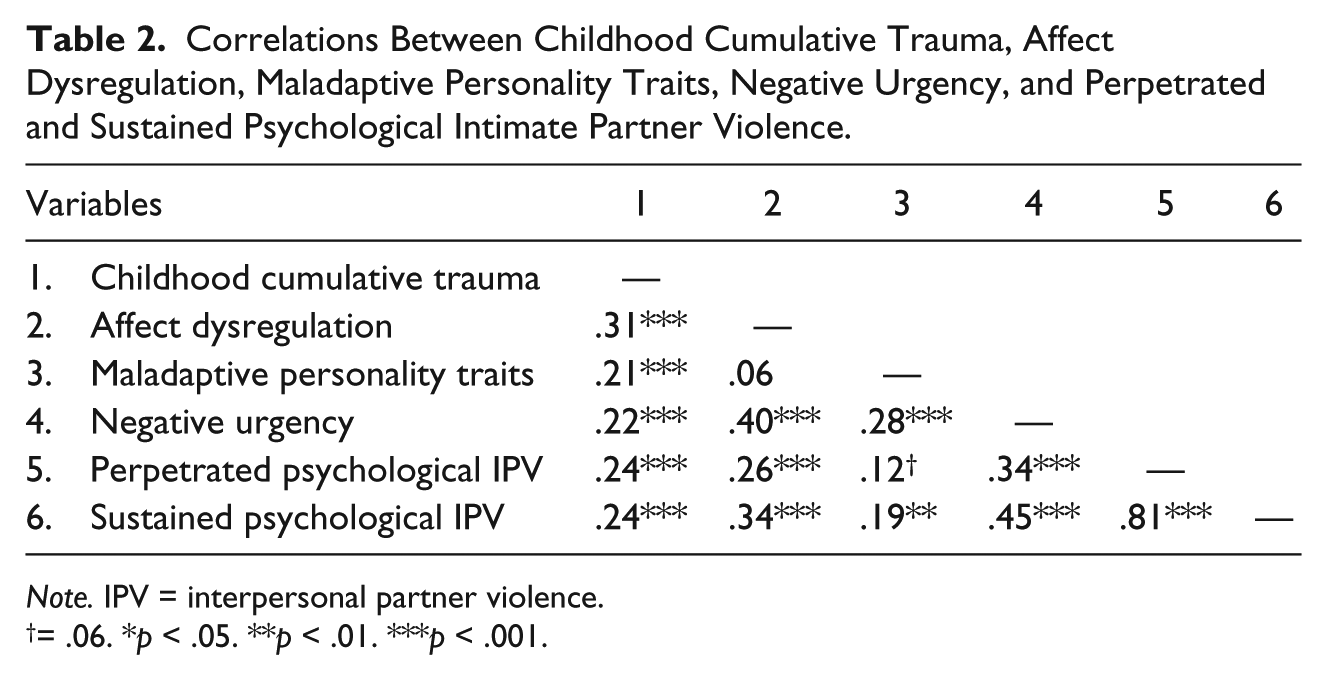
Note. IPV = interpersonal partner violence.
= .06. *p < .05. **p < .01. ***p < .001.
Integrative Mediational Model
Results of path analyses showed significant direct paths from CCT to psychological IPV perpetration (β = 0.24, p < .001, R2 = 5.8%) and victimization (β = 0.24, p < .001, R2 = 5.7%). When the mediators were added to the model, these direct paths were no longer significant. The mediation model (see Figure 1) adequately fitted the data, CFI = .97, RMSEA = .06, 95% confidence interval [CI] = [.00, .11], χ2(8) = 14.51, p = .07, χ2/df = 1.81, SRMR = .06. The standardized coefficients are presented in Figure 1. CCT positively predicted negative urgency through affect dysregulation (b = .19, 95% CI = [.09, .30]) and maladaptive personality traits (b = .09, 95% CI = [.01, .16]), respectively explaining 69% and 31% of the total effect of CCT on negative urgency. Then, as hypothesized, two sequential mediations were found. First, the indirect effect of CCT through affect dysregulation and negative urgency was significant for perpetrated psychological IPV (b = .11, 95% CI = [.03, .20]), as well as sustained psychological IPV (b = .14, 95% CI = [.04, .23]). This sequential mediation through affect dysregulation and negative urgency explained 68% of the total effect of CCT on perpetrated psychological IPV and 69% of the total effect of CCT on sustained psychological IPV. Second, the indirect effects of CCT, through maladaptive personality traits and negative urgency were significant for perpetrated psychological IPV (b = .05, 95% CI = [.01, .10]), as well as for sustained psychological IPV (b = .06, 95% CI = [.01, .12]). This sequential mediation explained 32% of the total effect of CCT on perpetrated psychological IPV and 31% of the total effect of CCT on sustained psychological IPV. To assess the generalizability of the mediational model across gender, sex was added as a covariate in the final model. Results from this additional analysis revealed that controlling for the effect of gender did not change the significance and strength of the associations between the study variables. To examine alternative hypotheses that could also be compatible with the correlational nature of the present study, the integrative model was also tested by changing the order of the study variables (e.g., maladaptive personality traits and affect dysregulation leading to CCT, IPV leading to CCT). None of the five tested models adequately fitted the data.
Discussion
The current study is the first to support the hypothesis that the relationship between CCT and psychological IPV is mediated by negative urgency processes that are, in turn, explained by affect dysregulation and maladaptive personality traits. Our sequential mediational model also goes a step further than past studies (Briere et al., 2010; Poythress et al., 2006) and provides a plausible, more precise, description of affective, cognitive, and personality factors explaining how CCT may lead to inflicted and perpetrated IPV during adulthood.
The current results thus suggest that negative urgency holds a crucial role in the trajectories of CCT survivors who report experiencing psychological IPV. This is consistent with previous studies that have concluded that maladaptive behaviors performed in response to negative emotions and a lack of self-control are associated with the perpetration of aggressive behaviors, especially IPV (Shorey et al., 2011; Stuart & Holtzworth-Munroe, 2005). Of particular interest, CCT was indirectly associated with sustained psychological IPV through higher affect dysregulation, maladaptive personality traits, and negative urgency. Indeed, although research has suggested that partners’ negative urgency is associated with IPV, no study has yet demonstrated the specific impact of negative urgency on psychological IPV victimization. Such associations suggest that negative urgency in CCT survivors not only affects the management of negative verbal behaviors such as insulting, yelling, or uttering threats but can also increase interpersonal vulnerability. For instance, people who are high in negative urgency frequently engage in impulsive or dysfunctional behaviors when they are upset (Blake, Hopkins, Sprunger, Eckhardt, & Denson, 2018) without being necessarily violent. This tendency, when partners discuss distressing events, potentially heightens one’s risk of sustaining psychological IPV, for instance following impulsive reactions to feeling upset or rejected by the partner. It is also possible that individuals who show negative urgency tend to associate with partners who present similar tendencies, thus enhancing their risk of sustaining IPV (Iverson, McLaughlin, Adair, & Monson, 2014). However, future longitudinal studies are warranted to examine this potential cycle of violence between partners.
The findings from the current study hold empirically based theoretical implications. Indeed, the choice of mediators for this study was inspired by Holtzworth-Munroe and Stuart’s (1994) conceptualization of male batterers, which was here applied to men and women from the general population, who report experiencing psychological IPV. Interestingly, these results suggest that the affective and behavioral mechanisms that are at play in severe IPV perpetrated by male batterers are somewhat similar to those observed in adult couples from the general population, even though the type of violence they report is generally less severe and not nested in a general pattern of coercive control (Johnson, 2008).
Also, in contrast to previous studies, the current study incorporates psychological IPV, reported as sustained and inflicted by participants. Yet, to date, only few studies suggest that CT increases the risk to simultaneously experience both psychological IPV victimization and perpetration in adult couple relationships (Dugal et al., 2018; Godbout et al., 2009). Consistent with these studies, the present results show that in individuals from the general population, perpetrated and sustained psychological IPV are highly correlated. This finding supports dyadic models of IPV in couples’ interactions (Cantos & O’Leary, 2014; Capaldi & Kim, 2007) and research indicating that bidirectional IPV is the most common pattern found in this population (e.g., Langhinrichsen-Rohling et al., 2012; Straus, 2008). This may be particularly true at low and moderate levels of psychological violence. Importantly, the findings of the current study support research that indicates IPV should be studied within a general aggression framework (e.g., Bates, Archer, & Graham-Kevan, 2017), such as the General Aggression model (Anderson & Bushman, 2002), rather than a separate type of violence with a “special” etiology (e.g., Browne, 1987). It allows a new understanding of the mechanisms through which survivors of CCT experience psychological IPV in adulthood; future research should consider other variables that could be examined to better understand the link between CCT and IPV (e.g., communication abilities, alcohol or drug use).
Limitations
The use of self-report measures might heighten the risk of distortions in the recall of victimization or aggression experiences, as well as enhance social desirability biases. Yet, the administration of online anonymous questionnaires has been known to provide more reliable results when it comes to experiences of violence (Brock et al., 2015; Whisman & Snyder, 2007). In future research, recruiting both partners and conducting actor–partner interdependence models (Kenny, Kashy, & Cook, 2006) could help rescind this limitation by taking into account IPV as reported by both partners. In addition, as the design of this study is correlational, the direction or temporal order of the associations between the variables included in the mediation model cannot be unequivocally ascertained. Rather, the integrative model was hypothesized using a theoretical framework in which cognitive or emotional processes predict impulsive or violent behaviors. While this theoretically grounded analytic strategy has been recommended for analyses examining repercussions of violent experiences (Byrne, 2010), the order of causation between the studied variables should be confirmed using longitudinal data. Finally, the preponderance of students in the current sample limits the generalizability of the study to participants with distinct demographic profiles.
Implications
Findings of the current study provide an empirical basis for future intervention programs aimed at CCT survivors or adults who report psychological IPV. For instance, results support the need to assess affect regulation and personality in CCT survivors as well as in perpetrators and victims of psychological IPV. Results also emphasize the need to develop prevention and intervention programs aiming to increase resilience and decrease negative urgency to prevent or reduce psychological IPV or to limit its consequences. Such programs could include attachment, mindfulness, or mentalization-based techniques (Diamond et al., 2014; Huprich, Nelson, Paggeot, Lengu, & Albright, 2017; Rathus, Cavuoto, & Passarelli, 2006) that would focus on the treatment of affect dysregulation, maladaptive personality traits, or negative urgency by working on internal representations of self and other. Cognitive-behavioral interventions aimed at the development of communication and conflict resolution skills in CCT survivors or couples dealing with mild to moderate psychological IPV could also hamper partners’ tendency to react in a dysfunctional manner to negative emotions arising during couple interactions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Caroline Dugal was supported by a Doctoral Research Scholarship from the Fonds de recherche du Québec—Société et culture (FRQSC). Natacha Godbout was supported by grants from the Fonds de recherche du Québec Santé (FRQS) and from the Interdisciplinary Research Centre on Intimate Relationship Problems and Sexual Abuse (CRIPCAS).