
Abstract
Institutional betrayal occurs when, following sexual victimization, institutions create hostile environments which normalize sexual violence, make it difficult to report the experience, mishandle the complaint, attempt to cover up the experience, or retaliate against survivors. These responses are not uncommon and have been linked to adverse survivor outcomes such as dissociation, anxiety, sexual dysfunction, poorer physical health, and depression, yet little is known about which survivors are most at risk for experiencing institutional betrayal. Using a sample of 404 sexual assault survivors recruited from Amazon Mechanical Turk, the current study employed logistic regression to identify risk factors for institutional betrayal. The findings indicate that institutional betrayal is more likely to be reported by survivors who identify as heterosexual, were older at the time of the assault, and endorse more severe PTSD symptoms yet, unexpectedly, less severe distress severity. Gender, race, assault characteristics, and disclosure tendencies did not significantly predict institutional betrayal risk. Although some relationships may be bidirectional, the results suggest that survivors already at risk for some negative post-assault outcomes may be particularly at risk for institutional betrayal.
Introduction
Sexual assault is widely known to predict a variety of negative outcomes, including increased risk for depression, anxiety, substance abuse, suicidality, obsessive-compulsive disorder, bipolar disorder, and posttraumatic stress disorder (PTSD; Dworkin, Menon, Bystrynski, & Allen, 2017), and affects one in five women and one in 71 men over the lifetime (Black et al., 2011). The broader literature on trauma exposure and PTSD suggests that social support (or a lack thereof) may be one of the strongest predictors of whether an individual is resilient against PTSD (Andrews, Brewin, & Rose, 2003; Pietrzak, Johnson, Goldstein, Malley, & Southwick, 2009; Ullman, Townsend, Filipas, & Starzynski, 2007 for a review, see Guay, Billette, & Marchand, 2006). The link between poor social support and increased posttraumatic symptomology appears to be strongest in cases of violent crime and abuse and is more salient for women than men (Andrews et al., 2003).
Betrayal trauma theory may help to explain the salience of social support, which posits that negative outcomes of trauma arise from life threat and social betrayal (Freyd, 1999, 2001). The focus in betrayal trauma theory is on the relationship between victim and perpetrator, such that an important bond—as well as related assumptions about interpersonal and social relationships—is betrayed within the context of the trauma (Freyd, 1996). The trauma lies not only in the event itself but in the shattered assumptions and sense of betrayal from an important other, after which survivors find themselves trying to grapple with both the trauma as well as the betrayal of being wronged by those with whom trust was placed (Freyd & Birrell, 2013). Similar to support-seeking from friends and families that is common following sexual assault (e.g., Golding, Siegel, Sorenson, Burnam, & Stein, 1989), survivors who experience trauma within the context of a larger institution (e.g., university, military, religious organization), may turn to the institution expecting support and necessary accommodations—such expectations are often violated. Institutional betrayal refers to survivors’ experiences of an institution as mishandling their traumatic experience and can range from passive actions, such as failing to take proactive steps to prevent the experience, to actively working to cover-up the experience or retaliate against the survivor (Smith & Freyd, 2014). This type of betrayal has been publicized in cases such as the cover-up of sexual abuse within the Catholic church, military, and sexual assault-related Title IX violations within universities. Institutional betrayal has been found to exacerbate dissociation, anxiety, sexual dysfunction, and depression following sexual assault (Smith & Freyd, 2013); among veterans, institutional betrayal in the military predicted suicide attempts and symptoms of PTSD and depression above and beyond the impact of military sexual trauma alone (Monteith, Bahraini, Matarazzo, Soberay, & Smith, 2016).
As an emerging empirical construct, it is unclear what risk factors predict the likelihood that survivors will report experiencing institutional betrayal. Unpublished studies and findings based on bivariate analyses have provided some preliminary impressions regarding institutional betrayal risk, although this area clearly represents a gap worthy of exploring further. For example, one study using a sample of undergraduate college students found that students who identified as lesbian, gay, or bisexual (LGB) reported significantly more instances of institutional betrayal compared to students who did not identify as LGB (d = .58, p = .01), and LGB students who experienced institutional betrayal were at a heightened risk for psychological distress compared to non-LGB students reporting betrayal; however, the findings did not consider the influence of many important confounds (Smith, Cunningham, & Freyd, 2016). Similarly, Gomez (2015) posited that race may moderate the relationship between institutional betrayal and adverse outcomes, such that Black Americans who experience betrayal within mental health care settings may be more severely impacted than others. Specifically, Gomez suggests that Black Americans’ frequent experiences with microaggressions within mental health care may be a form of institutional betrayal, citing examples of limited cultural competence and normalized microaggressive behavior. Although not empirically tested, Gomez argues that microaggressions experienced by Black Americans within mental health care settings may have a stronger impact than microaggressions perpetrated by individuals outside of the setting because Black Americans may come to expect microaggressions in society generally but may feel betrayed by mental health care systems into whom trust was given. Although bivariate analyses from an unpublished dissertation found that the likelihood of experiencing institutional betrayal was not influenced by race, socioeconomic status, or gender (Smith, 2016), the theoretically based assertion by Gomez (2015) is not incongruent with findings by Smith (2016) that the likelihood of experiencing institutional betrayal does not vary by race but rather suggests that institutional betrayal, when experienced, may be more salient for some individuals, including LGB individuals and Black Americans.
Beyond studies examining institutional betrayal specifically, research on individual and institutional responses to survivors of sexual violence may offer insight about potential assault and disclosure characteristics that predict institutional betrayal. For example, it is not known how age influences risk for institutional betrayal, although studies examining disclosure to law enforcement found that older survivors were more likely to immediately report the assault compared to younger survivors (Chen & Ullman, 2010), suggesting perhaps that older survivors may be more likely to be in contact with institutions broadly following victimization. Law enforcement officials tend to respond more favorably to survivors of more stereotypical assaults, such as those that are more severe, involve physical force, injury, or stranger perpetrators (e.g., Estrich, 1987; Frazier & Haney, 1996; Patterson, 2011; Shaw, Campbell, Cain, & Feeney, 2017; Venema, 2016). Conversely, survivors who used alcohol prior to the assault report being treated more negatively by others (Ullman & Filipas, 2001). Following the assault, survivors who delay disclosing (i.e., “slow starters,” or those who wait at least 2 weeks before telling anyone) report experiencing fewer negative reactions from others, and are also less likely to disclose to law enforcement and medical professionals (Ahrens, Stansell, & Jennings, 2010), perhaps out of fear that their delay will lead to formal support providers not believing them, or will be less able to effectively investigate and respond to the event. Unsurprisingly, disclosure timing also influences the total number of individuals to whom survivors disclose, with ongoing disclosers disclosing to an average of 5.84 individuals (SD = 3.47) compared to slow starters, who disclosed to only 3.58 individuals (SD = 5.03), and crisis disclosers (i.e., those whose first disclosure occurred within 2 days and last disclosure within 1 week of the assault) who disclosed to an average of 2.96 individuals (SD = 1.90). Crisis disclosers report experiencing more negative reactions from others compared to slow starters (Ahrens et al., 2010), perhaps because crisis disclosers are less selective about disclosure recipients and instead disclose to who is most proximal or available rather than most supportive or knowledgeable, which increases the likelihood of receiving a negative response (Petronio, Flores, & Hecht, 1997). Crisis disclosers may also stop disclosing specifically because of the negative responses they received (Ahrens et al., 2010). Given this, survivors who disclose more often may be more susceptible to experiencing negative reactions, including from institutions.
The Current Study
Despite emerging research on institutional betrayal, we were only able to identify two studies to date that have examined risk factors for institutional betrayal, and those findings resulted from bivariate analyses or multivariate analysis with limited covariates (Smith, 2016; Smith et al., 2016) and unpublished dissertations (Smith, 2016). The purpose of this article is to examine risk factors for experiencing institutional betrayal in a sample of sexual assault survivors.
Based on limited existing research, we hypothesized that the likelihood of reporting experiencing institutional betrayal would not differ based on gender or race; however, we hypothesized that survivors who were older at the time of the assault would be more likely to experience institutional betrayal due to increased contact with institutions (Chen & Ullman, 2010). Moreover, survivors who identified as LGB were predicted to have an increased risk for institutional betrayal (Smith et al., 2016). Extrapolating from findings that assault characteristics predict negative disclosure experiences (Ullman & Siegel, 1995; Ullman, Starzynski, Long, Mason, & Long, 2008), we also hypothesized that completed rape, perpetrator use of physical force, victim injury, and assaults involving a stranger perpetrator would predict a decreased risk for institutional betrayal, whereas victim substance use would predict an increased risk for institutional betrayal. Similarly, extrapolating from findings about disclosure tendencies (Ahrens et al., 2010; Petronio et al., 1997), we hypothesized that survivors who disclose more often would be at greater risk for experiencing institutional betrayal, and those who delay disclosing would be at a decreased risk for experiencing institutional betrayal due to the reduced likelihood of disclosing to formal support providers. Finally, due to longitudinal findings that social reactions predicted PTSD symptoms, which in turn predicted social reactions (Ullman & Peter-Hagene, 2016), and research that has linked institutional betrayal to anxiety and depression (Smith & Freyd, 2013), we included as covariates PTSD and distress severity to control for these bidirectional effects.
Method
Participants
Data were obtained from 1,173 participants recruited for a study of sexual assault disclosure (see Pinciotti et al., in press) from the crowdsourcing website, Amazon Mechanical Turk (MTurk). MTurk allows workers to search for and complete online studies for pay. Inclusion criteria included age 18 or older, residence in the United States, and an approval rating of 90% or higher on the site to increase the likelihood of quality responses. A total of 601 completed the entire survey, 52.6% (n = 495) of whom reported an unwanted sexual experience after the age of 14. Totally, 69 participants were removed from analyses because they responded incorrectly to more than one of three forced response items (e.g., “If you are still reading, please select moderately agree”), and 22 were removed because they reported that their worst assault occurred prior to age 14, leaving a final sample of 404. The final sample of survivors of sexual trauma ranged in age from 18 to 74 (M = 35.6, SD = 12.1) and identified as 74.0% women, 25.7% men, and 0.2% other. The sample identified as 81.9% heterosexual (n = 330), 12.2% bisexual (n = 49), 4.7% gay/lesbian (n = 19), 0.2% asexual (n = 1), and 1.0% other sexual orientation (n = 4). The reported racial breakdown of the final sample was as follows: White (79.8%, n = 320), Black (8.2%, n = 33), Asian (5.5%, n = 22), American Indian or Alaskan Native (1.7%, n = 7), Native Hawaiian or Pacific Islander (0.7%, n = 3), mixed race (3.0%, n = 12), and other racial background (1.0%; n = 4). An additional 7.8% identified as Hispanic or Latino/a (n = 31).
Measures
Assault disclosure characteristics
The Sexual Assault Inventory of Disclosure (SAID; Pinciotti et al., in press) was used to assess participants’ experiences with sexual assault disclosure. The SAID provides detailed information about sexual assault disclosures, including the types and amount of content shared and the context in which disclosures occur. In the current study, the following SAID items were used: age at the time of worst sexual assault, timing of first disclosure, and total number of individuals to whom survivors disclosed. Survivors’ worst unwanted sexual experience occurred between 14 years and 52 years of age (M = 20.28, SD = 6.27), and first disclosures occurred between the same day as the assault (24.2%) to over 10 years later (2.4%), with the modal disclosure occurring 1 to 6 days postassault (27.3%). This variable was dichotomized for analyses (1 = disclosed within one week of the assault, 0 = disclosed longer than 1 week after the assault). In the current sample, survivors disclosed to between 0 and 100 formal and informal recipients (M = 4.8, SD = 9.3). Given that the SAID is an inventory which represents a tally or sum of endorsement items rather than responses psychometrically related to one another (Clark & Watson, 1995), calculating internal consistency is not appropriate. However, the SAID has demonstrated strong test–retest reliability over a 1-month follow-up, including status of disclosure (r = 1.00, p < .001) and small to large test–retest correlations for disclosure content (r = .25 to .70; Pinciotti et al., in press).
Assault history and characteristics
To assess participants’ history of sexual assault and specific assault characteristics, the Sexual Experiences Survey–Short Form Victimization (SES-SFV; Koss et al., 2007) and additional assault characteristics items adapted from previous research (Swinson, 2013) were used. The SES-SFV is a 17-item self-report instrument of behaviorally specific sexual assault experiences since the age of 14. Sexual assault experiences range from any attempted or actual nonconsensual touching or clothing removal to completed rape (i.e., penetration). Participants endorse on a 4-point Likert-type scale how many times each of the experiences happened to them since age 14 from 0 to 3+ times. All participants included in analyses endorsed some sort of sexual victimization experience, and 63.1% reported contact meeting the legal definition of rape on the SES-SFV. Similar to the SAID, internal consistency for SES-SFV items is not computed; however, previous research has found adequate consistency with verbal reports of victimization (r = .73; Koss & Gidycz, 1985) and convergent validity with measures of dissociation, anxiety, depression, sleep disturbance, and sexual problems (Johnson, Murphy, & Gidycz, 2017).
For assault characteristics, participants were asked to select their most distressing unwanted sexual experience and report on their relationship to the perpetrator at the time of the assault (coded as 1 = friend/acquaintance, significant other, or family member and 0 = stranger perpetrator), perpetrators’ threatened or actual use of physical force (1 = threatened/used force, 0 = did not threaten/use force), whether survivors incurred physical injury (1 = yes, 0 = no) or received medical attention (1 = received medical attention, 0 = did not receive medical attention), and survivors’ self-reported level of intoxication at the time of the assault on a 9-point Likert-type scale (0 = not at all drunk/high to 8 = black out drunk or extremely high). Of assaults, 44.7% were committed by friends/acquaintances, 26.1% committed by strangers or someone the survivor had just met, 18.7% committed by significant others/spouses, 5.3% committed by family members, and 5.3% committed by “other.” In addition, 24.7% involved threatened or actual use of physical force; 37.7% resulted in victim injury ranging from soreness to loss of consciousness; 37.7% resulted in medical treatment sought; and survivors rated their average intoxication level as 2.0 (SD = 2.8).
Demographic characteristics
Participants were asked a series of demographic questions that were dichotomized when entered into the logistic regression, including gender (1 = female, 0 = male), race (1 = White, 0 = non-White), and sexual orientation (1 = heterosexual, 0 = LGB).
Distress severity
The Depression Anxiety and Stress Scale (DASS-21; Lovibond & Lovibond, 1995) was used to measure symptoms of overall distress severity. The DASS-21 comprised three related subscales of depression, anxiety, and stress, and a total score reflects the combination of these symptoms to reflect overall symptom distress in these areas (e.g., “I felt down-hearted and blue”). Items are measured on a 4-point Likert-type scale (0 = did not apply to me at all to 3 = applied to me very much, or most of the time) and reflect distress associated with depressive, anxious, and stress symptoms. The DASS-21 has evidenced strong internal validity in previous research, with Cronbach’s alpha of .93 for the total scale, and demonstrated strong convergent and discriminant validity with other measures of depression and anxiety (Henry & Crawford, 2005). In the current study, internal validity was very strong (α = .96) and participants rated their distress severity as 19.1 on average (SD = 15.2).
Institutional betrayal
The Institutional Betrayal Questionnaire, Version 2 (IBQ.2; Smith, 2014) was used to assess participants’ experiences with institutional betrayal. The IBQ.2 is a checklist that includes 12 types of institutional betrayal, ranging from a failure to take proactive steps to prevent the trauma (e.g., “Creating an environment in which this experience seemed more likely to occur”), to inadequately responding to the trauma (e.g., “Mishandling your case, if disciplinary action was requested”), to covering up the trauma (e.g., “Covering up the experience”) or retaliating against the survivor (e.g., “Punishing you in some way for reporting the experience [e.g., loss of privileges or status]”). Participants indicate whether they have experienced any of the 12 types of betrayal by responding yes (1) or no (0); scores are summed for a total betrayal score ranging from 0 to 12. A total of 11.8% (n = 50) of participants reported experiencing at least one instance of institutional betrayal (M = 2.2, SD = 1.6). In the current study, participants were coded as either having reported experiencing institutional betrayal (1) or not (0). See Table 1 for institutions identified as responsible for betrayal. As with the SAID and SES-SFV, internal consistency is not appropriate for the IBQ.2; however, data on the factor structure and convergent and discriminant validity of the IBQ.2 is forthcoming (Reffi, Pinciotti, & Orcutt, in press).
Institutions Responsible for Betrayal.

Note. Participants may endorse more than one betraying institution.
PTSD severity
The PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) (PCL-5; Weathers et al., 2013) is a 20-item self-report measure of PTSD severity administered after the Life Events Checklist (LEC; Weathers et al., 2013). Following the LEC, participants are instructed to answer PCL items based on the event that they consider their worst event (i.e., is most bothersome currently) out of those listed on the LEC. The PCL items, anchored to this index trauma, reflect the diagnostic symptom clusters of PTSD, including reexperiencing (e.g., “Repeated, disturbing, and unwanted memories of the stressful experience”), avoidance (e.g., “Avoiding memories, thoughts, or feelings related to the stressful experience”), hyperreactivity (e.g., “Feeling jumpy or easily startled”), and negative alterations in cognition and mood (e.g., “Blaming yourself or someone else for the stressful experience or what happened after it”). PCL-5 responses are summed to create a total symptom severity score from 0 to 80. Participants are asked to indicate on a 5-point Likert-type scale how much they were bothered in the past month by each symptom, from 0 = not at all to 4 = extremely. The PCL-5 has demonstrated very strong internal consistency (α = .94) and good test–retest reliability (r = .82; Bovin et al., 2016; Weathers et al., 2013); in the current study, internal consistency was very strong (α = .96). Participants reported a mean PCL-5 score of 19.9 (SD = 19.4).
Procedure
Participants were recruited to complete the Human Intelligence Task (HIT) on MTurk. Participants were informed that they would be asked sociodemographic questions as well as questions regarding their sexual experiences (5-10 min), and that their responses may make them eligible to complete additional items (30-45 min) regarding stressful life experiences and mental health. The study was approved by the Institutional Review Board at the university at which the study was conducted.
After providing informed consent, participants reported on their sociodemographic characteristics and history of adult sexual assault (i.e., after age 14). Participants who endorsed no history of adult sexual assault were debriefed and US$0.15 was credited to their MTurk account. Participants who endorsed a history of adult sexual assault were asked additional items about institutional betrayal, assault characteristics, disclosure characteristics, social support, and symptomatology. Participants were then debriefed and credited a bonus of US$0.60 (total payment = US$0.75) for completing the additional items. All participants were provided a list of national sexual assault resources.
Data Analysis Plan
Prior to computing the logistic regression, bivariate analyses in the form of t tests and chi-square tests were computed to compare group means and percentages for each predictor. Independent samples t tests were used to compare groups across ordinal- and interval-level response variables, and chi-square tests were used to compare groups across categorical variables. Logistic regression was then computed to compare predictors of experiencing institutional betrayal (1 = experienced institutional betrayal, 0 = did not experience institutional betrayal). Logistic regression is robust enough to manage skewed, dichotomous dependent variables (Cleary & Angel, 1984), as in the current study. Independent variables were entered simultaneously in one step to estimate each predictor’s unique contribution to group membership while concurrently controlling for the effects of other predictors.
Results
A series of independent samples t tests and chi-square tests were conducted to examine bivariate relations among the variables (see Table 2). Of the variables, physical force, medical treatment, and PTSD severity were significantly associated with reported institutional betrayal experiences at the bivariate level.
Bivariate Comparisons of Sexual Assault Survivors With and Without Institutional Betrayal.
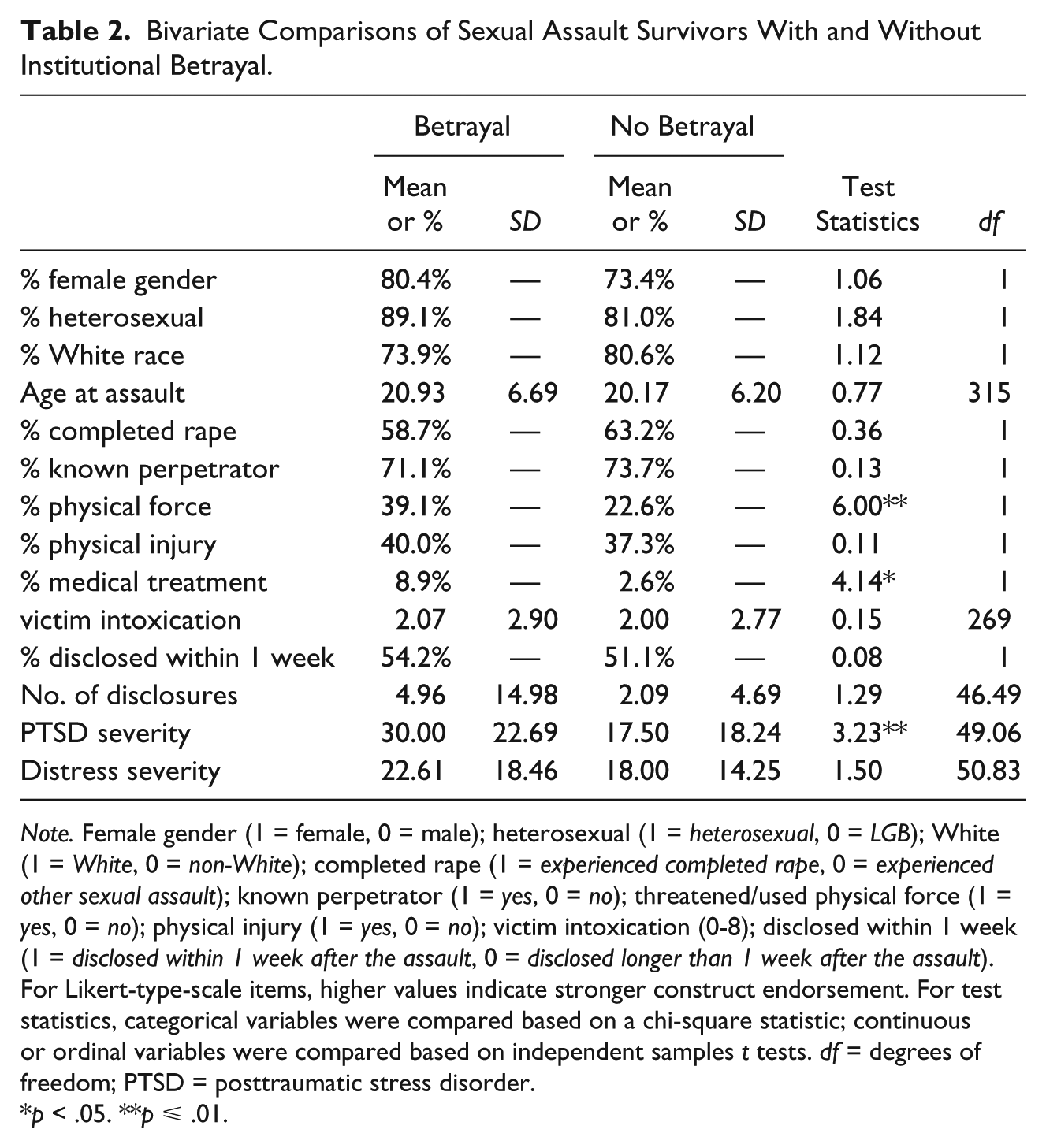
Note. Female gender (1 = female, 0 = male); heterosexual (1 = heterosexual, 0 = LGB); White (1 = White, 0 = non-White); completed rape (1 = experienced completed rape, 0 = experienced other sexual assault); known perpetrator (1 = yes, 0 = no); threatened/used physical force (1 = yes, 0 = no); physical injury (1 = yes, 0 = no); victim intoxication (0-8); disclosed within 1 week (1 = disclosed within 1 week after the assault, 0 = disclosed longer than 1 week after the assault). For Likert-type-scale items, higher values indicate stronger construct endorsement. For test statistics, categorical variables were compared based on a chi-square statistic; continuous or ordinal variables were compared based on independent samples t tests. df = degrees of freedom; PTSD = posttraumatic stress disorder.
p < .05. **p ⩽ .01.
A logistic regression was computed to predict the likelihood of experiencing institutional betrayal (1 = experienced, 0 = did not experience). The overall model accounted for approximately 32% (p < .001) of the variance in predicting whether an individual reported experiencing institutional betrayal, Nagelkerke R2 = .32; 84.4% correctly classified overall; χ2(8) = 6.37, p = .61. Of significant predictors, identifying as heterosexual was associated with 6.71 times increased odds of reporting experiencing institutional betrayal (b = 1.90, p < .05); and older age at the time of the assault was associated with 1.10 times increased odds of reporting experiencing institutional betrayal (b = .09, p < .05). Of covariates, each unit increase in PTSD symptom severity was associated with 1.08 times increased odds of reporting experiencing institutional betrayal (b = .08, p = .01), and each unit increase in distress severity was associated with a .91 decreased odds of reporting experiencing institutional betrayal (b = −.09, p < .05; see Table 3).
Factors Predicting Likelihood of Experiencing Institutional Betrayal.
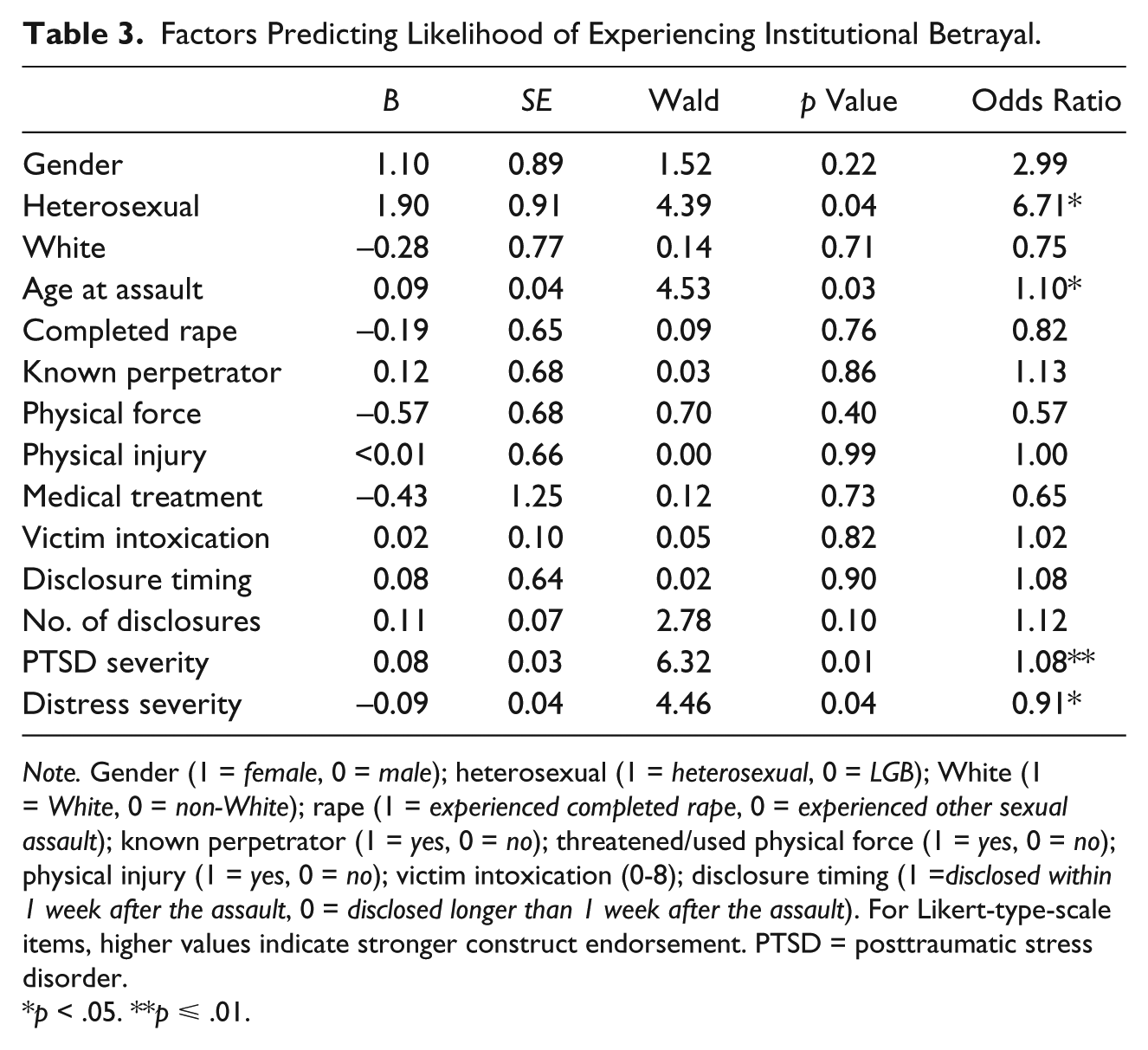
Note. Gender (1 = female, 0 = male); heterosexual (1 = heterosexual, 0 = LGB); White (1 = White, 0 = non-White); rape (1 = experienced completed rape, 0 = experienced other sexual assault); known perpetrator (1 = yes, 0 = no); threatened/used physical force (1 = yes, 0 = no); physical injury (1 = yes, 0 = no); victim intoxication (0-8); disclosure timing (1 =disclosed within 1 week after the assault, 0 = disclosed longer than 1 week after the assault). For Likert-type-scale items, higher values indicate stronger construct endorsement. PTSD = posttraumatic stress disorder.
p < .05. **p ⩽ .01.
Discussion
Following a sexual assault, survivors may turn to larger institutions for support, assistance, or justice, only to be met with inaction, mismanagement, or retribution. Institutional betrayal has been found to predict symptoms of PTSD, anxiety, and depression, dissociation, suicide attempts, physical health, and sexual dysfunction (Monteith et al., 2016; Smith, 2014; Smith & Freyd, 2013), although to date it is unclear which survivors are most at risk for experiencing institutional betrayal. Bivariate analyses from an unpublished dissertation suggest that the likelihood of experiencing institutional betrayal is not influenced by race, socioeconomic status, or gender (Smith, 2016), although these analyses do not consider potential confounding effects. In addition, some research has suggested that women and students who identify as LGB may experience more instances of institutional betrayal (Smith, 2016; Smith et al., 2016), although these findings rely on bivariate analyses or only address the extent of betrayal experienced (i.e., number of betrayal instances) rather than who is at risk. To address this gap, the current study used logistic regression to examine risk factors for experiencing institutional betrayal.
We found several characteristics predicted an increased likelihood of reporting experiencing institutional betrayal. First, although sexual orientation was a significant predictor of institutional betrayal risk as hypothesized, the direction of the relationship was contrary to predictions. Specifically, survivors who identified as heterosexual were 6.71 times more likely to report experiencing institutional betrayal compared to survivors who identified as LGB, a finding that seems to contract previous literature by Smith and colleagues (2016) that found that students who identified as LGB reported more instances of institutional betrayal even after controlling for higher rates of sexual violence. Of note, their findings did not account for other covariates like age, assault characteristics, or mental health outcomes, and involved a university sample. Although many of the participants in the current sample identified a university as the institution responsible for betrayal, our sample was not exclusively university-based, which may explain contradicting findings. In addition, whereas LGB status was associated with more instances of perceived institutional betrayal in the study by Smith and colleagues (2016), the current study examined institutional betrayal dichotomously, or the likelihood of whether a survivor experienced any form of perceived institutional betrayal. Given this, it is possible that individuals who identify as LGB are marginally less likely to experience institutional betrayal, but when they do experience it, the betrayal tends to be more severe. LGB participants may also be less likely to seek support from institutions out of fear of being mistreated and thus may only appear to be at decreased risk in the current sample because of this reduced contact with institutions. Definitive conclusions should not be drawn, however, until findings are replicated.
Consistent with hypotheses, age at the time of the assault predicted institutional betrayal, such that survivors who were older at the time of the assault were more likely to report experiencing institutional betrayal. All participants in the sample experienced sexual assault after the age of 14 and the most commonly identified institution in the current sample was a university, so it is intuitive that survivors who report experiencing institutional betrayal would be older and closer to college age. Older survivors may also have more contact with and greater trust in institutions, as evidenced by literature that older survivors are more likely to immediately disclose to law enforcement than younger survivors (Chen & Ullman, 2010). Survivors victimized in their early teenage years may be at less risk for institutional betrayal because they have less contact with formal providers and institutions. For example, whereas Starzynski, Ullman, Filipas, and Townsend (2005) found that approximately 60% of adult survivors disclosed to formal support providers, only 8.3% of high school seniors talked to professionals about the abuse and only 6.8% reported the abuse to social authorities or law enforcement (Priebe & Svedin, 2008). Rather, children aged 14 to 17 appear far more likely to disclose to peers than other recipients (Kogan, 2004).
The current study also found that each unit increase in PTSD severity was associated with a 1.10 times increased odds of experiencing institutional betrayal. Not surprisingly, previous research has found that betrayal trauma exacerbates posttraumatic symptomatology (Freyd, 1999, 2001) and that institutional betrayal, specifically, predicts increased PTSD in victims of military sexual trauma (Monteith et al., 2016). The negative cognitive impact of betrayal trauma, much like the traumatic event itself, is experienced in the form of shattered assumptions and unexpected betrayal (Freyd, 1996). In some cases, survivors must continue functioning within the institution that betrayed them, such as with survivors of military sexual trauma, leading to a continued experience of betrayal over time. However, it also likely that greater PTSD symptom severity predicts an increased likelihood for mistreatment and betrayal. A longitudinal study conducted by Ullman and Peter-Hagene (2016) found that negative reactions to survivors not only predict increased PTSD symptoms, but that these increased symptoms predict future negative reactions, perhaps because symptom severity and negative affect has been found to elicit negative responses from others (Coates, Wortman, & Abbey, 1979; Coyne, 1976; Sacco & Dunn, 1990). In addition, individuals suffering from increased PTSD may be more likely to perceive betrayal due to trauma appraisals; however, although the items on the IBQ.2 range in subjectivity, the measure includes several forms of betrayal that are arguably more objective, such as suggesting the experience might affect the institution’s reputation or retaliating against the victim (e.g., loss of privileges or status). The association between PTSD and institutional betrayal clearly warrants further investigation, including in studies utilizing longitudinal designs, to better parse out the directionality of the relationship. Likely, the relationship between institutional betrayal and PTSD is bidirectional.
Unexpectedly, less symptom distress predicted an increased risk for institutional betrayal. This finding contradicts previous research that has linked institutional betrayal to increased anxiety and depression (Smith & Freyd, 2013), but may be a function of statistical suppression. Statistical suppression occurs when an independent variable does not explain unique variance in the dependent variable but accounts for enough irrelevant variance in the model that the effect of another independent variable is increased (Maassen & Bakker, 2001). At the bivariate level, institutional betrayal was associated with greater symptom distress, yet this relationship was reversed at the multivariate level with the inclusion of other effects—a pattern often indicative of suppression. Due to the overlap between PTSD and symptoms of anxiety and depression (i.e., symptom distress), it seems likely that PTSD acted as a suppressor in this case; however, future research is needed to replicate this finding.
In an unpublished dissertation, Smith (2016) found that the likelihood of experiencing institutional betrayal was not influenced by race or gender, and these findings were replicated in the current study. Contrary to predictions, the likelihood of reporting experiencing institutional betrayal was not found to be predicted by whether the unwanted sexual experience was completed rape, whether the perpetrator was known, use of physical force, physical injury, whether medical treatment was sought, victim intoxication, timing of first disclosure, or frequency of disclosure, after accounting for the effects of sexual orientation, age, and mental health.
Limitations
Findings of the current study are limited by the reliance on a convenience sample of MTurk workers, who may not be representative of the overall population. Previous research has found, however, that MTurk workers provide responses comparable to other populations (Paolacci, Chandler, & Ipeirotis, 2010) and provide a greater variety of potential betraying institutions, whereas studies using only undergraduate college populations may be more likely to include only betrayal by universities. Although other betraying institutions are represented in our sample, the vast majority of identified institutions were universities and thus findings from the current study may not generalize to other institutions, like religious organizations or the military.
Future Directions
In addition to replication of all findings, future research on institutional betrayal is needed with more representation of nonuniversity institutions to determine whether risk factors are similar across institutions. Survivors of military sexual trauma may, for example, have unique risk factors for institutional betrayal such as military rank given the unique demands of the job. Most importantly, as described previously, longitudinal research is needed to better parse out the directionality of significant relationships, including the relationship between PTSD and institutional betrayal. As discussed, many relationships are likely bidirectional and empirical support of these longitudinal trajectories will allow for more definitive conclusions about which survivors are most at risk for institutional betrayal.
Conclusion
Whereas other studies have helped to highlight the detrimental impact of betrayal experiences (Monteith et al., 2016; Smith et al., 206; Smith & Freyd, 2013), the current study is, to the authors’ knowledge, the first to the likelihood of experiencing institutional betrayal. Survivors who experience more severe PTSD and turning against reactions from others, in addition to survivors who are older and disclose more frequently, are at the greatest risk for reporting experiencing institutional betrayal. Mental health professionals available to members of institutions, such as university counselors or military psychologists, should be cognizant of these risk factors when working with survivors who are considering disclosing their experience to the institution. Moreover, institutions would benefit from psychoeducation and training about situations in which they may be more likely to engage in behaviors perceived as betrayal by survivors, in addition to making support interventions available to survivors who believe that they have experienced institutional betrayal. As institutional policies and procedures continue to attract needed attention and scrutiny, increased knowledge of cases that are more likely to elicit betrayal responses is crucial so that institutions can work to reduce this likelihood and promote a safer, less hostile environment for survivors seeking support and justice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.