
Abstract
Prior research has indicated the significant overlap between risky alcohol use and intimate partner violence (IPV) among couples. However, few studies have explicitly examined the intersection of alcohol use and IPV among distressed couples (e.g., couples seeking couples therapy). The current study aimed to (a) examine how couples presenting to couple therapy experience alcohol use, IPV, and the co-occurrence of both alcohol use and IPV and (b) the effect of the intersection of alcohol use and IPV in couples on relational functioning. Archival data collected from 71 couples presenting to couple therapy at a University training clinic were used to explore the research aims. Data analysis procedures included univariate statistics to characterize the sample and bivariate statistics to examine the research aims. Findings indicated that 16.9% of couples screened positive for both alcohol use and IPV and that there were significant group differences in relational functioning among females in the sample. These findings indicate the potential need for universal alcohol and IPV screening among clinicians working with couples.
Introduction
Alcohol use and intimate partner violence (IPV) are two public health issues that affect both individuals and relationships. In examining alcohol use and IPV independent of one another, prior research has indicated that approximately half of people 12 years old and older reported current alcohol use (Substance Abuse and Mental Health Services Administration, 2017), and 35.6% women and 28.5% of men having ever experienced IPV (Black et al., 2011). These issues are even more problematic when examined together, with alcohol consumption by one partner reportedly occurring in 15% of IPV incidents and alcohol consumption by both partners reportedly occurring in an additional 15% of IPV incidents (Reingle, Jennings, Connell, Businelle, & Chartier, 2014). Moreover, de Bruijn and de Graaf (2016) identified that “The literature offered robust evidence that men and women’s alcohol use increases the likelihood of perpetrating physical violence” (p. 142). While research recognizes the link between these two public health problems, research specifically examining the comorbid impact within couples is less common.
Alcohol use and IPV have been shown in prior research to independently affect relational dynamics. Specifically, IPV victimization has been linked to decreases in relationship satisfaction in at least one of the members of the couple (Ackerman & Field, 2011; Hammett, Ulloa, Castaneda, & Hokoda, 2017; Shortt, Capaldi, Kim, & Laurent, 2010). Alcohol use has also been shown to negatively affect relationship satisfaction, especially for female partners (Birditt, Cranford, Manalel, & Antonucci, 2016; Khaddouma et al., 2016; Leonard & Eiden, 2007). These findings have been even more robust for discordant alcohol use couples, defined as couples in which only one member of the couple engages in alcohol use (Birditt et al., 2016; Khaddouma et al., 2016; Leonard & Eiden, 2007), and in couples in which excessive drinking occurs, defined as hazardous due to frequency or duration of use (Leonard & Eiden, 2007).
There is a relative dearth of research concurrently examining the variables of alcohol use, IPV, and relational functioning among treatment-seeking couples. There is a significant amount of literature on integrative and traditional behavioral couples therapy models and their utility with couples experiencing alcohol use (Baucom, Sevier, Eldridge, Doss, & Christensen, 2011; Powers, Vedel, & Emmelkamp, 2008), research from Stith and McCollum (2011; Stith, McCollum, & Rosen, 2011) regarding couples therapy for IPV, and research on integrated substance abuse–IPV treatment for individuals (Easton et al., 2007; Klostermann, Kelley, Mignone, Pusateri, & Fals-Stewart, 2010). However, research examining alcohol use and IPV concurrently among couples presenting to conjoint treatment is missing. The current study aims to fill that gap.
Current Study
While the literature shows a clear linkage between alcohol use, IPV, and relational outcomes, alcohol use and IPV are often approached independent of one another in both research and clinical realms. Clinicians and scholars need to know how alcohol use and IPV intersect among distressed couples (e.g., those presenting to couple therapy) to better inform clinical and scholarly practices. As such, the current article examined how couples presenting to couple therapy experience alcohol use and IPV, and how the presence of alcohol use and/or IPV effects relational functioning, operationalized as perceived relationship satisfaction, consensus, and cohesion, among these couples. Thus, the goal of the current article was to examine the following research aims:
Method
Participants and Procedure
The current study used archival data from clients who presented to at least one session of conjoint couple therapy for a nonsubstance use presenting concern between March 2016 and December 2016. A total of 93 couples sought out services and, of those, 71 couples had complete data files for the variables of interest. Original data were collected from participants who self-referred for services at a graduate training clinic at a Midwestern University. Both members of the couple presented to the initial session and completed an intake assessment in which information about demographics, individual and relational functioning, alcohol consumption, IPV, and adverse childhood events were queried. Each member of the couple completed the instruments independently. For the present study, archived data relevant to the current research questions were downloaded, cleaned, and de-identified. To note, the data available were data designed as part of a clinical intake assessment, thus limiting the data points available to those collected as part of the intake process. This study protocol was reviewed and approved by the institution’s institutional review board (IRB).
Measures
Demographics
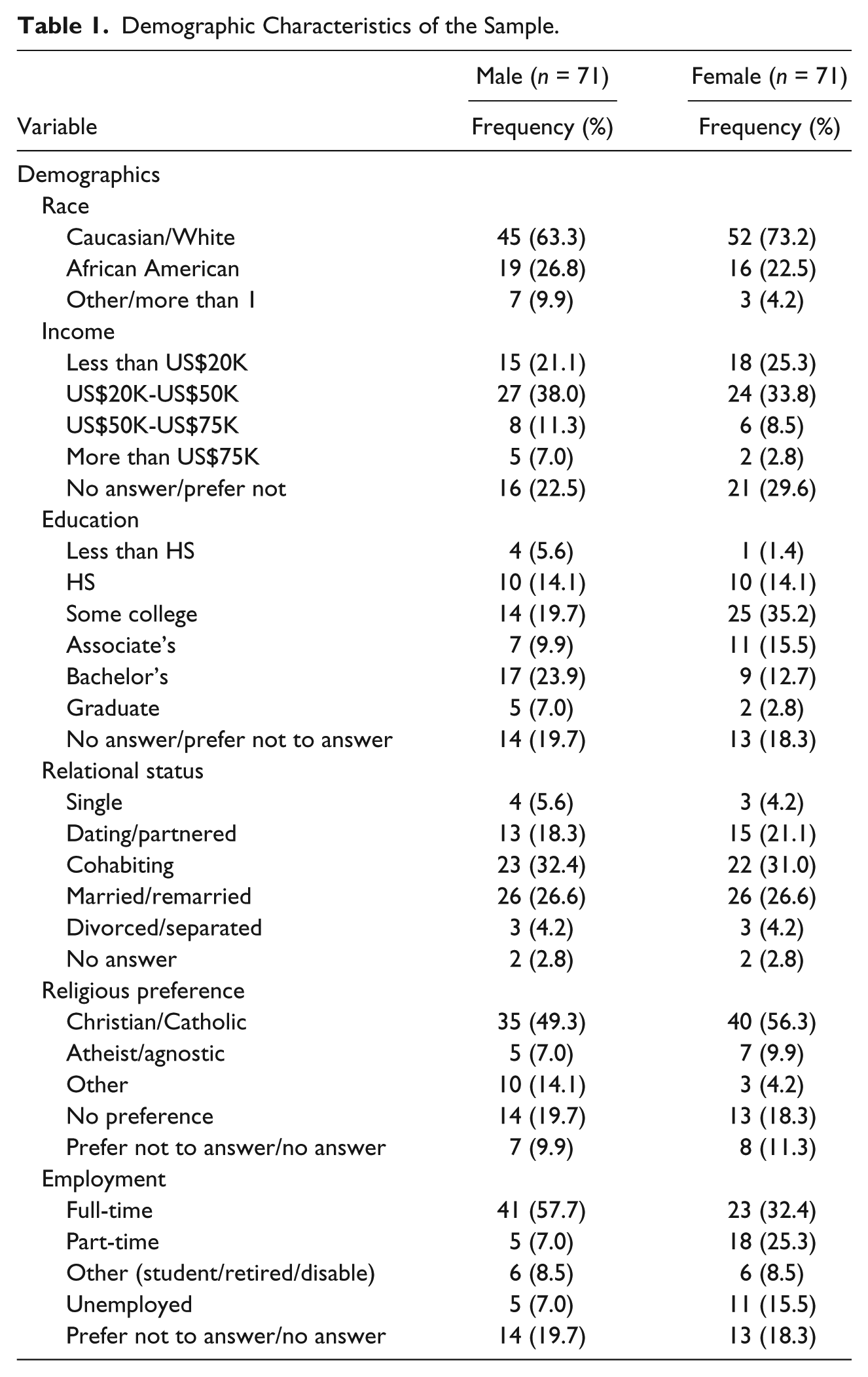
Respondents self-reported on gender (male or female), race/ethnicity (Caucasian/White; African American/Black; Asian American, Latino; Arab American; Other; more than one race/ethnicity; prefer not to answer), annual household income (less than US$20,000, between US$20,000 and US$50,000, between US$50,000 and US$75,000, or more than US$75,000), highest level of education completed (less than high school, completed high school, some college, associated degree, bachelor’s degree, graduate degree, or prefer not to answer), employment status (full-time, part-time, retired, student, disabled, unemployed, or prefer not to answer), relational status (single, dating, partnered, living together/cohabiting, married, separated, remarried, divorced, or prefer not to answer), and religious preference (Christian, Catholic, atheist, agnostic, Hindu, Buddhist, other, no preference, or prefer not to answer). Due to the distribution of the data, some of the categories were condensed and are referenced in Table 1.
Demographic Characteristics of the Sample.
Alcohol use
Alcohol use was assessed using the Alcohol Use Disorders Identification Test–Consumption (AUDIT-C; Bush, Kivlahan, McDonell, Fihn, & Bradley, 1998). The AUDIT-C consists of three questions aimed at screening for hazardous drinking (e.g., frequency, quantity, and binge drinking). The scores range from 0 to 12. A score of 4 or more indicates a positive screen for males, and a score of 3 or more indicates a positive screen for females. The AUDIT-C score was tallied for each member of the couple, and couples were categorized based on dyadic use pattern (e.g., neither partner screened positive, both partners screened positive, only female partner screened positive, and only male partner screened positive).
IPV
IPV was assessed using the HITS (Sherin, Sinacore, Li, Zitter, & Shakil, 1998). The HITS assessment consists of four questions assessing for IPV (hurts, insults, threatens to harm, and screams), and the scores range from 4 to 20. Any score above 10 indicates a positive screen for IPV. For the current study, the HITS summary score was calculated for each member and each member was categorized as screening positive or negative. Couples were categorized into four groups (no IPV, female screened positive, male screened positive, both members screened positive).
Intersection of alcohol use and IPV
The scores from the AUDIT-C and HITS were combined to create four groups, including (a) couples who did not screen positive for either alcohol use or IPV, (b) couples of whom at least one partner screened positive for IPV but not for alcohol use, (c) couples of whom at least one partner screened positive for alcohol use but not for IPV, and (d) couples of whom at least one partner screened positive for IPV and at least one partner screened positive for alcohol use. These four groups were included in one variable for use in the ANOVA models.
Relational functioning
Relational functioning was assessed using the Revised Dyadic Adjustment Scale (RDAS; Busby, Christensen, Crane, & Larson, 1995). This assessment consists of 14 questions and aims to measure relationship satisfaction. There are three subscales (consensus, satisfaction, and cohesion) within the RDAS. The total score was used to assess overall relationship quality, with scores under 47 indicating relational distress and score 48 and over representing nondistress (ranging from 0 to 69).
Data Analysis Plan
The first research aim was to examine how couples presenting to couple therapy experience alcohol use, IPV, and co-occurrence of both alcohol use and IPV. To analyze this aim, frequencies for alcohol use, IPV, and the intersection of alcohol use and IPV were calculated for males, females, and the couple unit. The second research aim was to examine the effect of the intersection of alcohol use and IPV in couples on relational functioning. ANOVA analyses were used to identify group differences in relational functioning based on couple grouping (alcohol only, IPV only, both alcohol and IPV, or neither). A Bonferroni post hoc test was conducted to examine the direction of any significant relationships found in the ANOVA.
Results
Research Aim 1: Examining Alcohol Use, IPV, and Co-Occurrence
For alcohol use, 15 (21.1%) couples had both members screen positive for hazardous alcohol use, eight (11.3%) couples had only the female screen positive, eight (11.3%) couples had only the male screen positive, and 40 (56.3%) couples consisted of both members who did not screen positive on the AUDIT-C. For each member of the couple, 23 (32.4%) males and 23 (32.4%) females screened positive on the AUDIT-C. Average scores were 2.58 (SD = 2.35) for males and 2.17 (SD = 1.95) for females.
For IPV, eight (11.3%) couples had both members screen positive for IPV, seven (9.9%) couples had only the female screen positive for IPV, six (8.5%) couples had only the male screen positive for IPV, and 50 (70.4%) couples consisted of both members who did not screen positive on the HITS. For each member of the couple, 14 (19.7%) males and 15 (21.1%) females screened positive. Average scores on the HITS were 7.32 (SD = 2.53) for males and 7.30 (SD = 2.90) for females.
Results examining the frequencies of couples in each group (alcohol only, IPV only, both alcohol and IP, or neither) indicated that 12 (16.9%) couples screened positive for alcohol use and IPV, 20 (28.2%) couples screened positive only for alcohol use, eight (11.3%) couples screened positive only for IPV, and 31 (43.7%) couples did not screen positive for alcohol use or IPV.
In examining the RDAS scores for all participants, the average score for males was 41.73 (SD = 10.19, range = 18-62) and the average score for females was 39.20 (SD = 11.29, range = 11-63). Within the neither alcohol nor IPV group, the average scores for males was 42.81 (SD = 11.44) and the average score for females was 42.84 (SD = 10.34). For the IPV only group, the average score for males was 35.75 (SD = 4.46) and the average score for females was 34.88 (SD = 10.64). For the alcohol only group, the average score for males was 42.55 (SD = 9.99) and the average score for females was 41.15 (SD = 10.17). For the group experiencing both alcohol and IPV, the average score for males was 41.58 (SD = 9.42) and the average score for females was 29.42 (SD = 10.34).
Research Aim 2: Association Between Alcohol Use, IPV, and Relational Functioning
Two one-way ANOVAs by gender were conducted to examine the association between relational functioning and the different couples groups (including either alcohol or IPV only, both alcohol and IPV, or neither). Results showed that there was not a significant effect between any couple group and the males’ RDAS scores, F(3, 67) = 1.08, p = .363 (see Table 2). Results showed that there was a significant effect between the groups and the females’ RDAS scores, F(3, 67) = 5.58, p < .01 (see Table 3). Post hoc analyses (Bonferroni) indicated a significantly positive relationship for the RDAS scores for females in the alcohol-only group as compared with the alcohol and IPV group, meaning the alcohol-only group scored higher on the RDAS as compared with the alcohol and IPV group (mean difference = 11.73). Post hoc analyses also indicated a significant positive relationship for the RDAS scores for females between the neither group and the alcohol and IPV group, meaning that the neither group reported significantly higher RDAS scores as compared with the alcohol and IPV group (mean difference 13.42).
ANOVA of Male RDAS by Couple Grouping.
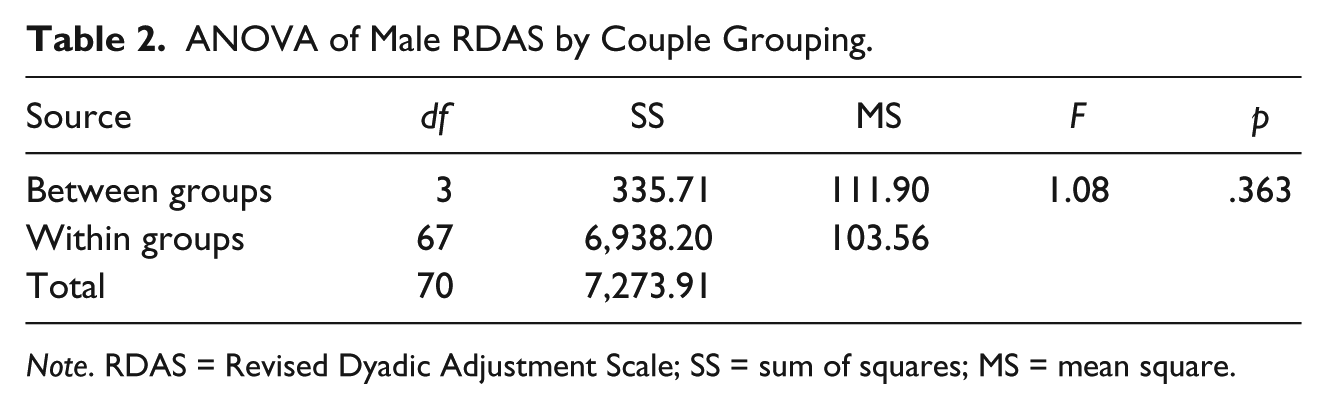
Note. RDAS = Revised Dyadic Adjustment Scale; SS = sum of squares; MS = mean square.
ANOVA of Female RDAS by Couple Grouping.

Note. RDAS = Revised Dyadic Adjustment Scale; SS = sum of squares; MS = mean square.
Additionally, a repeated-measures ANOVA was conducted to examine the the associations between partner scores on the RDAS by couple grouping. Repeated meaures analysis is conducted in order to account for the non-independence of the data between dyads who have a relationship beyond their involvement in the research study (e.g. couples; Kenny, Kashy, & Cook, 2006). Findings from the repeated measures ANOVA indicated a significant effect between the couple grouping and the partner RDAS scores, F(3, 67) = 2.99, p < .05.
Discussion
While there is a substantial amount of literature reporting on the significant co-occurrence of IPV and alcohol use when examining individual risk factors, less attention has been paid to the overlap of these two public health issues and how they affect relational functioning among distressed couples. As such, the current study filled a gap in the literature by examining (a) the frequencies of alcohol use and IPV among couples seeking couples therapy and (b) the association between alcohol use, IPV, and relational functioning. Several implications can be drawn from the findings.
In reference to the first research aim, findings from the current study indicated that over half of all couples in the sample reported experiencing either hazardous alcohol use, IPV, or both. Specifically, 16.4% of the couples screened positive for both risky alcohol use and IPV. These results seem consistent with prior literature that demonstrates that in 15% of IPV cases, alcohol use is reported in one partner (Reingle et al., 2014). These results further support the ethical and clinical need to screen for both of these public health concerns in every couple that reports to therapy regardless of the presenting issue, given that both alcohol use and IPV are relatively common occurrences within couples.
Regarding the second research aim, results from the ANOVA and related post hoc analysis indicated there were significant differences in relational functioning between groups for female scores, but not for males. This is consistent with prior research, which has found that IPV (Ackerman, 2012; Ackerman & Field, 2011) and alcohol use (Leonard & Eiden, 2007) tend to affect relationship satisfaction to a greater degree for women than for men. Interestingly, this study found that the greatest distress was experienced in couples in whom alcohol use and IPV were co-occurring, as compared with either being present alone or neither being present. This provides additional support for the assertion that these two public health problems should be addressed concurrently, especially in couples presenting to therapy.
While the current study adds to the literature by examining how couples who are seeking couple therapy experience both alcohol use and IPV, several limitations must be noted. First, the data used for the present analyses were archival data, thereby limiting the analyses to the variables originally collected. Specifically, both alcohol use and IPV were measured using self-report screening assessments, which are limited in providing additional contextual information about these potential problem behaviors (such as frequency, severity, etc.). In addition, the sample included couples who self-referred themselves to couple treatment, thereby limiting the generalizability of the results to couples who may have more insight about their overall distress, as compared with couples in the general population. Furthermore, our data included only cross-sectional data, and we cannot draw implications related to the temporal nature of the relationship between alcohol use and IPV from the data. Moreover, the only substance that was tested in this study was alcohol use, while it is recognized that there may be comorbidity between IPV and additional substance use that may not have been captured by this study. Finally, due to the sample size, the impact of additional demographic variables such as race/ethnicity were not able to be examined in this study. Future research is needed that can more thoroughly examine these research questions within the context of diversity in couples presenting to couples therapy, including interracial couples, intercultural couples, and same-sex couples.
Despite these limitations, the current findings give some direction for practical application and possible future research. The findings show the importance of universal screening for both alcohol use and IPV, and for practitioners to be knowledgeable in the impact of these public health issues on the individuals and couples they may be working with. The current findings also open up multiple future research directions, including more in-depth dyadic data analysis that examines concordance and discordance of alcohol use and IPV, an exploration of the linkage between other substances and IPV in couples, the role of intersectionality on how couples experience both substance use and IPV, and the potential impact of alcohol use and IPV on family functioning beyond the couple subsystem.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.