
Abstract
Despite recent civil rights advances for sexual minority communities in the United States, disparities in violence victimization have increased in recent years. Polyvictimization, the experience of multiple types of violence, is common in the United States and may result in mental and physical health consequences above and beyond single-type victimization. However, disparities in polyvictimization among sexual minority young people remain understudied. The purpose of this article was to determine whether there were disparities in monovictimization and polyvictimization among sexual minority young people compared with their heterosexual peers. Data for this article were from The National Longitudinal Study of Adolescent to Adult Health, a nationally representative cohort study started in 1994. Participants reported their experiences with eight types of violence across child abuse, criminal assault, intimate partner violence (IPV), and sexual assault domains. We categorized individuals with no violence victimization as nonvictims, individuals with one form of victimization as monovictims, and individuals with multiple types of victimization as polyvictims. We then compared experiences of each type of victimization and overall monovictimization and polyvictimization by sexual orientation (n = 9,828). Among females, the proportions of individuals experiencing victimization by sexual orientation were significantly different for all forms of violence. Among males, criminal assault, IPV resulting in injury, and nonphysically and physically forced sexual assault differed by sexual orientation. Compared with 100% heterosexual peers, individuals who were mostly heterosexual had significantly increased odds of monovictimization and polyvictimization compared with no victimization. Bisexual individuals had significantly increased odds of polyvictimiztion, and mostly/100% homosexual individuals had significantly increased odds of monovictimization. Multiple victimization experiences may be a pathway to lifetime health disparities, so our findings may explain many of the health disparities experienced in sexual minority communities. It will be critical to develop and evaluate intervention and prevention programs to eliminate these disparities.
Sexual minority young people have been at substantially increased risk of violence victimization compared with their heterosexual peers (Katz-Wise & Hyde, 2012). Despite recent advances in sexual minority civil rights in many areas, the disparities in family and school-based violence victimization between sexual minority and heterosexual groups have increased in recent years (Katz-Wise & Hyde, 2012). In addition to violence directly related to homophobia, sexual minority youth also experience higher rates of violence that may not be directly attributable to homophobia (Langenderfer-Magruder, Walls, Whitfield, Brown, & Barrett, 2016). For example, intimate partner violence (IPV) and child maltreatment victimization rates are consistently the same or higher among sexual minority individuals compared with their heterosexual peers (Balsam, Rothblum, & Beauchaine, 2005).
Polyvictimization, defined as the experience of multiple types of victimization, and monovictimization, defined as the experience of a single type of victimization, are common in the United States (Hamby & Grych, 2013). In their early work on polyvictimization, Finklehor and colleagues found that 66% of participants in a nationally representative sample of youth in the United States were exposed to more than one type of violent victimization prior to age 18 (Turner, Finkelhor, & Ormrod, 2010). More recent research has found that 48% of children experience more than one type of violence victimization each year (Finkelhor, Turner, Shattuck, & Hamby, 2013). Psychological distress, psychiatric disorders, and delinquency are common among polyvictims and polyvictimization may be a better predictor of negative health and well-being outcomes than any single victimization experience (Cuevas, Finkelhor, Turner, & Ormrod, 2007; Finkelhor, Ormrod, & Turner, 2007; Turner, Shattuck, Finkelhor, & Hamby, 2015).
Despite substantial research to suggest sexual minority youth and adults experience higher rates of victimization (Katz-Wise & Hyde, 2012), the literature on polyvictimization among sexual minority young people is limited. Two papers were recently published on polyvictimization experiences reported in a national convenience sample of sexual and gender minority adolescents (Sterzing, Gartner, et al., 2019; Sterzing, Ratliff, Gartner, McGeough, & Johnson, 2017). Sterzing and colleagues recruited adolescents through Facebook, YouTube, and the online presences and physical facilities of 12 community organizations serving sexual and gender minority adolescents. Participants in this study reported their experiences with property victimization, bias- and nonbias-motivated physical assault, child maltreatment, sexual victimization, IPV, bullying, and indirect victimizations. The number of types of victimizations was summed to determine the number of victimizations experienced by the adolescents. Overall, victimization and polyvictimization were substantial among this population. Approximately 30% of cisgender (i.e., gender identity corresponds with sex at birth) sexual minority adolescents reported polyvictimization, which was defined as 10 or more different forms of victimization in the year prior to the study, and the mean number of types of victimization was 13.5 out of 39 possible types (Sterzing, Gartner, et al., 2019; Sterzing, Ratliff, et al., 2017). This study included only sexual and gender minority adolescents, so it is not clear how these experiences would have compared with those of heterosexual young people. There has, to our knowledge, been no examination of disparities in polyvictimization during childhood and young adulthood between sexual minority young people and their heterosexual peers. To address this limitation in the literature, the purpose of our article was to determine whether there were disparities in monovictimization and polyvictimization among sexual minority young adults compared with their heterosexual peers in a longitudinal sample representative of adolescents and young adults in the United States. By providing the research foundation for tailored and targeted mental health and violence prevention programs for the LGB (lesbian, gay, bisexual) communities, this work may be an important first step to improving the mental health and public health response to health disparities experienced by LGB communities.
Method
Study Population
We used data from The National Longitudinal Study of Adolescent to Adult Health (Add Health). In 1994, nearly 100,000 students completed a school-based survey. The Add Health team purposefully sampled a subset of 20,745 adolescents from the school-based sample to complete four waves of data collection from 1995 to 2008 (Carolina Population Center, 2009). Systematic sampling methods and stratification were used to ensure the selected schools and students were representative of the overall U.S. youth population (Carolina Population Center, 2009).
Individuals were excluded from the analyses on each type of violence for several reasons: nonparticipation in waves of data collection during which information about that type of violence was collected (ranges from 5,044 in Wave IV to 6,007 in Wave II), missing response to questions about that type of violence (<1% for each question), and missing response to the sexual orientation question during Wave IV (n = 69). Due to the small number (n = 71), we also excluded participants who reported they were not sexually attracted to either males or females.
For the monovictimization and polyvictimization analyses, participants must have participated in all four waves of data collection, responded to questions about each type of violence, and reported their sexual orientation during Wave IV. A total of 9,828 participants were included in the monovictimization and polyvictimization analyses.
Measures
Outcomes
This analysis focused on four types of victimization: child maltreatment, general criminal assault, IPV, and sexual assault. To examine overall polyvictimization reported across adolescence and young adulthood, we created four dichotomous variables indicative of any experience of each of the four types of victimization (child maltreatment, criminal assault, IPV, and sexual assault) and summed those variables (0 = no victimizations; 4 = all types of victimizations). We categorized participants who reported one type of victimization as monovictims and those who reported at least two types of victimizations as polyvictims. Additional details on the treatment of variables are available in appendix.
The measurement of each form of victimization occurred at different points across the four waves. Wave I occurred in 1994-1995 when participants were in Grades 7 to 12 (approximately 12-18 years old), with Wave II occurring during the next school year (approximately 13-18 years old). Wave III occurred in 2001-2002 when participants were between the ages of 18 and 26. Wave IV occurred in 2008 when participants were between the ages of 24 and 32. During Waves III and IV, participants reported whether they experienced physical or sexual child maltreatment at least once prior to age 18. We categorized participants who reported at least one experience prior to age 18 as victims of that type of violence. During all waves, participants reported their experiences with three types of criminal assault: “threatened with knife or gun,” “shot or stabbed,” and “jumped or beaten up.” We categorized participants who reported at least one experience in any of the four waves of data collection as victims of criminal assault. During Wave III and Wave IV, participants who were in a relationship during the prior 12 months reported their experiences with three types of IPV victimization: threats of or minor physical IPV, severe physical IPV, or IPV resulting in injury. We categorized participants who reported at least one experience of the form of IPV as victims of that type of IPV. Finally, participants reported their lifetime experiences with two types of sexual violence during Wave IV: physically forced sexual assault and nonphysically forced sexual assault (verbal pressure, threats of harm, being given intoxicants). We categorized participants who reported at least one experience of the type of sexual assault as victims of that type of sexual assault.
Sexual orientation
Participants reported their sexual orientation during Wave IV of the study. The question “Please choose the description that best fits how you think about yourself” had five response options: “100% heterosexual (straight)”; “mostly heterosexual (straight), but somewhat attracted to people of your own sex”; “bisexual, that is, attracted to men and women equally”; “mostly homosexual (gay), but somewhat attracted to people of the opposite sex”; or “100% homosexual (gay).” As this question included both self-identification as a sexual minority and sexual attraction, it was not clear whether a smaller number of categories would be appropriate. We conducted a series of analyses to determine whether it was appropriate to combine any groups (e.g., heterosexual and mostly heterosexual or mostly heterosexual and bisexual). In doing so, we found that the experiences of mostly homosexual and 100% homosexual individuals were very similar. However, the experiences of mostly heterosexual and 100% heterosexual individual were significantly different. As a result, we combined the mostly homosexual and homosexual groups but left the bisexual, heterosexual, and mostly heterosexual groups separate.
Statistical Analysis
For all analyses, sexual orientation was the primary independent variable, and the dependent variable was violence victimization (single type or polyvictimization). We weighted and clustered all analyses by region and primary sampling unit to account for the complex survey design. We used bivariate analysis to estimate the distribution of each type of victimization by sexual orientation and Rao–Scott chi-square test to determine whether the proportion of individuals experiencing each type of victimization was equal across sexual orientation. Finally, we calculated the odds ratio (OR) for experiencing one type of victimization (monovictimization) or two or more types of victimization (polyvictimization) compared with no victimization using multinomial logistic regression. Models predicting single types of violence experiences were stratified by gender due to significant moderation by gender at α = .05. However, there was no evidence of moderation by gender in the monovictimization and polyvictimization analyses, so these were not stratified. We used SAS 9.4 for all analyses.
Results
Approximately half of the estimated population was female (50.0%; 95% confidence interval [CI]: [48.7, 51.3]) and half was male (50.0%; 95% CI: [48.7, 51.3]). A majority identified as 100% heterosexual (85.5%; 95% CI: [84.5, 86.7]), followed by mostly heterosexual but also somewhat attracted to the same sex (9.7%; 95% CI: [8.8, 10.5]). A smaller percentage of the estimated population identified as bisexual (1.5%; 95% CI: [1.2, 1.9]), mostly homosexual (0.8%; 95% CI: [0.6, 1.7]), or 100% homosexual (1.3%; 95% CI: [1.0, 1.6]).
Overall Victimization
Victimization was common among females but differed significantly based on sexual orientation (Table 1). For each type of violence, the proportion of victimized individuals was not equal across sexual orientation. For example, approximately 30% of 100% heterosexual and 100% or mostly homosexual females reported physical child abuse victimization, whereas 45.8% (95% CI: [41.0, 50.6]) of mostly heterosexual and 57.3% (95% CI: [45.0, 69.6]) of bisexual females reported physical child abuse victimization.
Estimated Victimization Percentages and Associations of Victimization and Sexual Orientation, by Gender.

Note. CI = confidence interval; IPV = intimate partner violence.
Percentage reporting victimization within each strata of sexual orientation.
Significant interaction between sexual orientation and gender (p < .05). *Rao–Scott χ2(3) p < .05.
The proportion of males who reported physical child abuse, sexual child abuse, threat/physical IPV, and severe physical IPV was equal across sexual orientation (Table 1). The proportion of male victims of criminal assault, injury due to IPV, and both nonphysically forced and physically forced sexual assault was significantly different across sexual orientation. The relationship between sexual orientation and victimization significantly differed between males and females for criminal assault and threats of/physical IPV, but did not significantly differ for other forms of violence.
Polyvictimization
The 100% heterosexual sample was split approximately evenly between nonvictims, monovictims (single-type victimization), and polyvictims (multiple-type victimization) (Figure 1). In contrast, approximately 75% of the mostly heterosexual and mostly/100% homosexual sample experienced at least one form of violence. Nearly 85% of the bisexual sample experienced at least one form of violence, and more than 60% were polyvictims. In multinomial regression models comparing monovictimization or polyvictimization with no victimization, individuals who identified as mostly heterosexual were at significantly increased odds of being a monovictim or polyvictim compared with heterosexuals (Table 2). In contrast, compared with no victimization, bisexual (OR: 3.13; 95% CI: [1.62, 6.05]) individuals were at significantly increased odds of polyvictimization compared with heterosexual individuals and mostly/100% homosexual individuals were at significantly increased odds of monovictimization (OR: 1.76; 95% CI: [1.06, 2.89]).
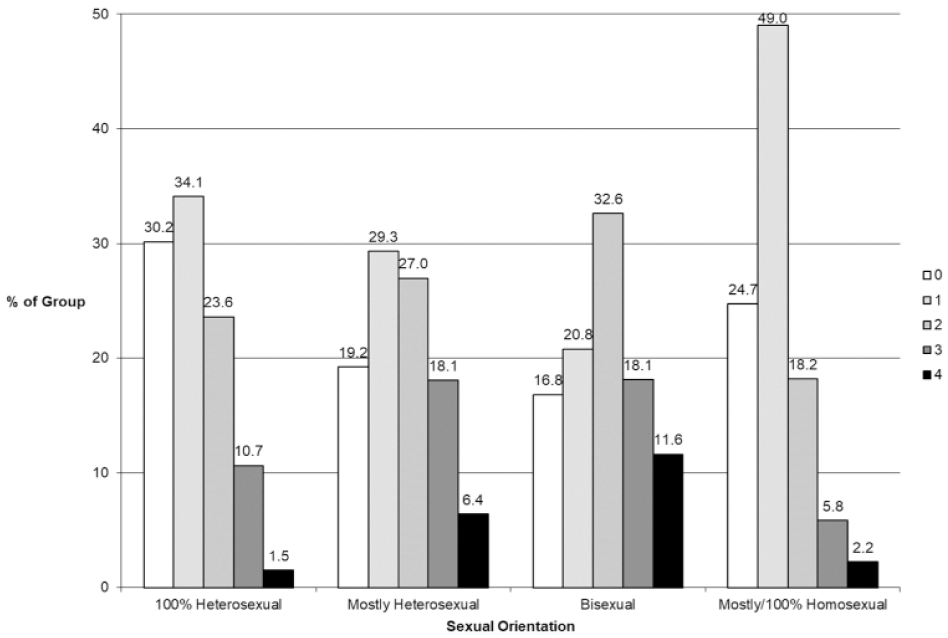
Summed number of types of violence experienced by sexual orientation.
Odds of Monovictimization or Polyvictimization by Sexual Orientation.
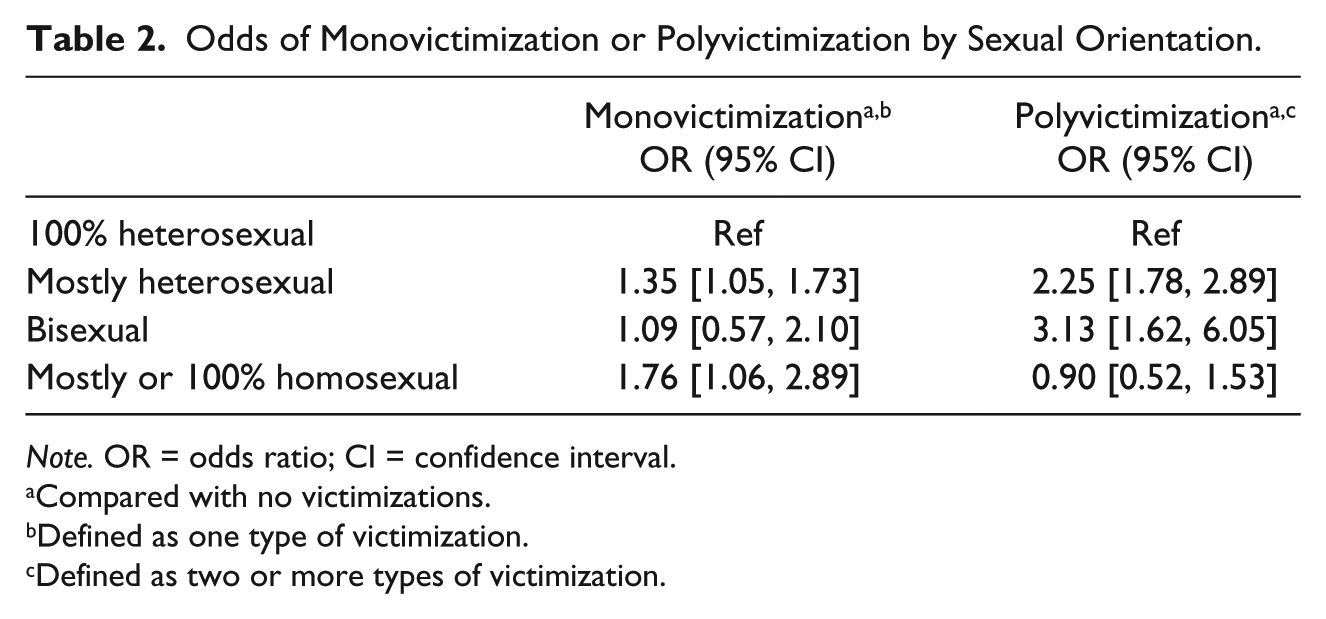
Note. OR = odds ratio; CI = confidence interval.
Compared with no victimizations.
Defined as one type of victimization.
Defined as two or more types of victimization.
Discussion
The purpose of this analysis was to determine whether sexual minority adolescents and young adults experienced higher rates of victimization, particularly polyvictimization, compared with their heterosexual peers. Overall, sexual minority participants reported more violence victimization than their heterosexual peers. Bisexual individuals experienced violence at the highest rate. Nearly 85% of bisexual individuals experienced at least one form of violence and more than 60% were polyvictims. This finding is consistent with that of Sterzing, Gartner, et al. (2019), which was bisexual individuals consistently reported higher rates of victimization and polyvictimization than gay or lesbian peers.
Less is known about the victimization experiences of mostly heterosexual individuals (M. S. Friedman et al., 2011). However, the emerging literature suggests violence experiences among mostly heterosexual individuals are different from heterosexual individuals. For example, mostly hetereosexual women are approximately half as likely to be spanked or hit with a belt during childhood as heterosexual women, but their rates of being beaten or neglected are substantially higher (Alvy, Hughes, Kristjanson, & Wilsnack, 2013). Similarly, mostly heterosexual women were more likely to have been a victim of sexual abuse (Austin, Roberts, Corliss, & Molnar, 2008). In our study, individuals who identified as mostly heterosexual also had consistently high rates of violence victimization and experienced significantly higher odds of monovictimization and polyvictimization compared with heterosexual individuals. Almost a third of mostly heterosexual individuals experienced monovictimization and nearly half experienced polyvictimization.
Individuals who identified as mostly/100% homosexual were, overall, not at significantly increased odds of polyvictimization. However, monovictimization was significantly higher among mostly/100% homosexual individuals compared with heterosexual peers, which is consistent with the literature on disparities in child maltreatment, IPV, and sexual violence among sexual minority individuals (Andersen & Blosnich, 2013; Balsam et al., 2005).
Implications
In light of prior findings that multiple victimization experiences may be a pathway to lifetime health disparities (Andersen, Zou, & Blosnich, 2015), our findings on monovictimization and polyvictimization disparities may explain many of the mental and physical health disparities experienced in the sexual minority communities. Higher rates of victimization may also be compounded by issues with availability of support services, including issues with foster care placement in childhood and lack of shelters for IPV available to the sexual minority communities (Carvalho, Lewis, Derlega, Winstead, & Viggiano, 2011; Hines & Douglas, 2011; Pattavina, Hirschel, Buzawa, Faggiani, & Bentley, 2007; Saewyc, Skay, Pettingell, & Reis, 2006). In addition, experience of and recovery from violent victimization may be complicated by social and internalized stigma associated with sexual orientation.
Research on developing prevention and intervention programs is necessary and must consider sexual orientation. Bisexual individuals experience the highest rates of violence and also the most significant mental and physical health disparities (M. R. Friedman et al., 2014; Sterzing, Gartner, et al., 2019). Given the stigma among the heterosexual and homosexual communities related to bisexuality, it may be particularly important to tailor programs to the bisexual community (Bostwick, Boyd, Hughes, West, & McCabe, 2014). In addition, more research is necessary to understand mostly heterosexual as a sexual orientation distinct from bisexuality and heterosexuality. The literature recognizing mostly heterosexual is small but growing. Our findings contribute to this body of literature that suggests individuals who identify as mostly heterosexual experience different risks than individuals who identify as heterosexual, including higher rates of adverse childhood experiences, sexually transmitted diseases, earlier sexual initiation, increased tobacco and alcohol use, more frequent disordered eating behaviors, and higher rates of depression and suicidality (Austin et al., 2008; Austin, Ziyadeh, Fisher, et al., 2004; Austin, Ziyadeh, Kahn, et al., 2004; Corliss, Rosario, Wypij, Fisher, & Austin, 2008; Marshal et al., 2013; Zou & Andersen, 2015). Violence victimization may be a cause or consequence of these health disparities, and it is important to better understand the experiences of individuals who identify as sexual minorities, including those who identify as mostly heterosexual.
Additional consideration must also be given to the impact of the political and social environment on the relationship between sexual orientation and polyvictimization. As of May 2017, relationships between females were illegal in 45 countries and relationships between males were illegal in 72 countries, including eight countries that implemented the death penalty due to sexual orientation–related crimes (e.g., sodomy, homosexual acts, or buggery) (Carroll & Ramón Mendos, 2017). In contrast, only 72 countries banned sexual orientation–related employment discrimination, 24 recognized same-sex marriage, and 26 recognized joint adoption by same-sex couples (Carroll & Ramón Mendos, 2017). Other formal and informal differences in the treatment of sexual minorities around the world, such as access to education and ability to openly discuss sexual relationships, also differ and likely influence the social acceptance of violence against the LGB community (Padilla, del Aguila, & Parker, 2007). Given these differences in the sociopolitical environment around the world, additional research on the relationship between sexual orientation and polyvictimization may be necessary to determine similarities and differences between the United States and other locations.
Limitations
This analysis has several limitations. First, we were limited to examination of the types of victimization experiences collected and the data collection methods in the Add Health Study. It would have been beneficial to examine other forms of victimization, such as bullying, property victimization, or witnessing violence, or to use the measurement tools commonly used to study polyvictimization, such as the Juvenile Victimization Questionnaire (JVQ; Hamby, Finkelhor, Turner, & Kracke, 2011). As a result, the prevalence rates of this study are not directly comparable to other studies of polyvictimization. In addition, the IPV during Wave IV and the criminal assault questions across all waves used the prior year as the reference period, which did not allow for capture of the full range of experience during the 14 years of the study. The child maltreatment and sexual assault questions asked about any lifetime victimization, which allowed for reporting of experience across the lifespan but may introduce recall bias due to the extended reference period.
Next, the number of sexual minority participants in this study, although generally in line with other national estimates (Gates, 2011), limited the analysis. Despite the very large sample size, the low number of sexual minority participants, combined with the relative rarity of some forms of violence, may have limited the statistical power of the estimates. Future studies may find it useful to oversample sexual minority participants to increase the statistical power of the analysis. In addition, these low cell sizes also precluded examination of how intersectional identities, such as race, ethnicity, socioeconomic status, or weight, interacted with sexual orientation to influence victimization, which may be an important next step to understanding how vulnerable populations experience polyvictimization.
Finally, due to data limitations, we could not evaluate gender identity as a potential factor. Previous research has demonstrated a link between gender identity and higher likelihood of violence exposure wherein transgender individuals are more likely to experience all forms of violence (Stotzer, 2009), so the polyvictimization experiences of transgender individuals may also differ from cisgender sexual minority peers.
Conclusion
Even with these limitations, the findings of this study highlight an important public health issue. Our findings corroborate previous research findings wherein sexual minority men and women experienced higher levels of several types of violence victimization, including child maltreatment, IPV, and criminal assault (Ard & Makadon, 2011; Balsam et al., 2005; Kulkin, Williams, Borne, de la Bretonne, & Laurendine, 2007; Robin et al., 2002; Saewyc et al., 2006; Sterzing, Gartner, et al., 2019; Sterzing, Ratliff, et al., 2017). Confusion about sexual identity and forced outing, as well as social stigma related to sexual minority status, has been identified as contributing to higher rates of victimization among sexual minority individuals (Goldberg, Matte, MacMillan, & Hudspith, 2003; Hatzenbuehler et al., 2014; Kulkin et al., 2007) and could potentially explain higher rates of polyvictimization as well.
Given the litany of health disparities associated with sexual minority status, it is crucial to understand the effects of polyvictimization on health outcomes among sexuality minority communities and how these effects compare to single violence exposures. Furthermore, it is critical that future research provide the empirical foundation for intervention programs to address these disparities in violence victimization and health outcomes.
Footnotes
Appendix
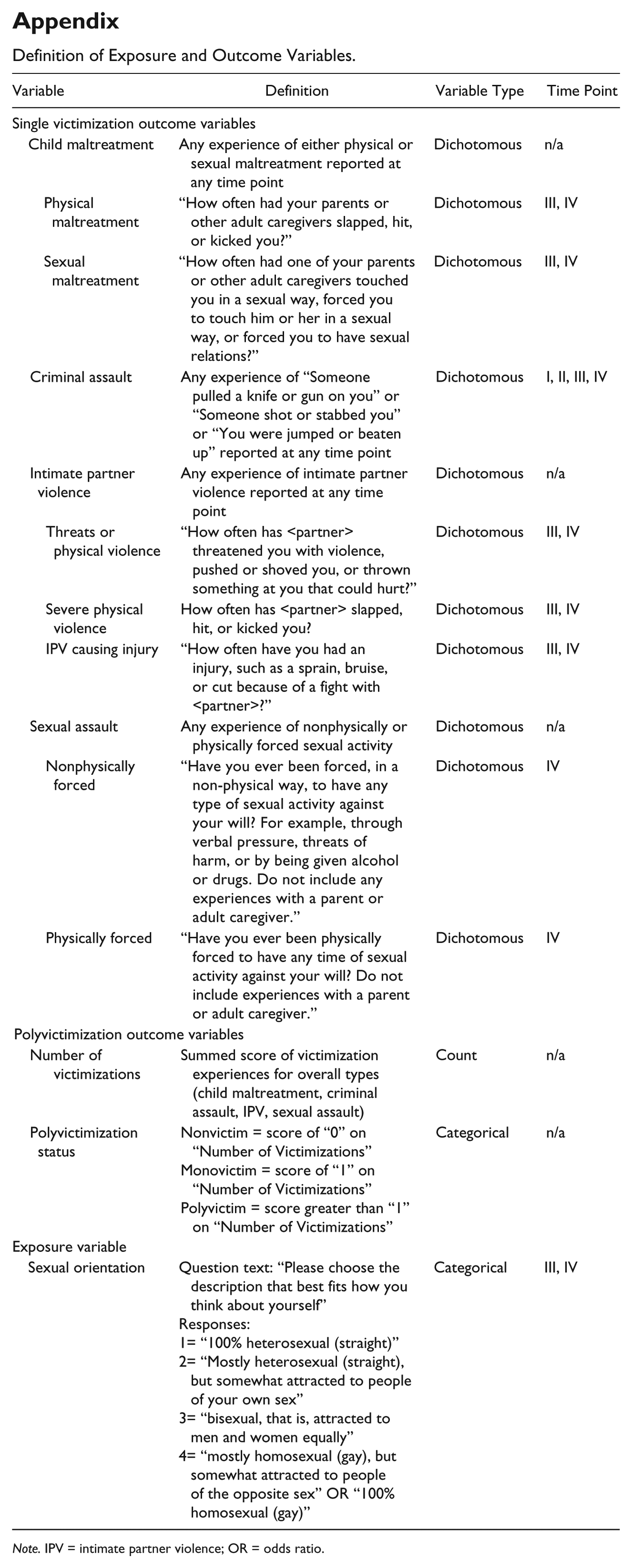
Definition of Exposure and Outcome Variables.
| Variable | Definition | Variable Type | Time Point |
|---|---|---|---|
| Single victimization outcome variables | |||
| Child maltreatment | Any experience of either physical or sexual maltreatment reported at any time point | Dichotomous | n/a |
| Physical maltreatment | “How often had your parents or other adult caregivers slapped, hit, or kicked you?” | Dichotomous | III, IV |
| Sexual maltreatment | “How often had one of your parents or other adult caregivers touched you in a sexual way, forced you to touch him or her in a sexual way, or forced you to have sexual relations?” | Dichotomous | III, IV |
| Criminal assault | Any experience of “Someone pulled a knife or gun on you” or “Someone shot or stabbed you” or “You were jumped or beaten up” reported at any time point | Dichotomous | I, II, III, IV |
| Intimate partner violence | Any experience of intimate partner violence reported at any time point | Dichotomous | n/a |
| Threats or physical violence | “How often has <partner> threatened you with violence, pushed or shoved you, or thrown something at you that could hurt?” | Dichotomous | III, IV |
| Severe physical violence | How often has <partner> slapped, hit, or kicked you? | Dichotomous | III, IV |
| IPV causing injury | “How often have you had an injury, such as a sprain, bruise, or cut because of a fight with <partner>?” | Dichotomous | III, IV |
| Sexual assault | Any experience of nonphysically or physically forced sexual activity | Dichotomous | n/a |
| Nonphysically forced | “Have you ever been forced, in a non-physical way, to have any type of sexual activity against your will? For example, through verbal pressure, threats of harm, or by being given alcohol or drugs. Do not include any experiences with a parent or adult caregiver.” | Dichotomous | IV |
| Physically forced | “Have you ever been physically forced to have any time of sexual activity against your will? Do not include experiences with a parent or adult caregiver.” | Dichotomous | IV |
| Polyvictimization outcome variables | |||
| Number of victimizations | Summed score of victimization experiences for overall types (child maltreatment, criminal assault, IPV, sexual assault) | Count | n/a |
| Polyvictimization status | Nonvictim = score of “0” on “Number of
Victimizations” Monovictim = score of “1” on “Number of Victimizations” Polyvictim = score greater than “1” on “Number of Victimizations” |
Categorical | n/a |
| Exposure variable | |||
| Sexual orientation | Question text: “Please choose the description that best
fits how you think about
yourself” Responses: 1= “100% heterosexual (straight)” 2= “Mostly heterosexual (straight), but somewhat attracted to people of your own sex” 3= “bisexual, that is, attracted to men and women equally” 4= “mostly homosexual (gay), but somewhat attracted to people of the opposite sex” OR “100% homosexual (gay)” |
Categorical | III, IV |
Note. IPV = intimate partner violence; OR = odds ratio.
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. No direct support was received from grant P01-HD31921 for this analysis.