
Abstract
Emerging research has shown that experiences of sexual violence are associated with cancer screening behaviors. However, to date, little attention has been given to the impact of sexual assault on cancer screening behaviors, particularly among men. To address this, we used data from the 2014 Kansas Behavioral Risk Factor Surveillance System. This survey is conducted annually via telephone. Logistic regressions were used to calculate odds of ever engaging (i.e., lifetime) in specific screening behaviors (clinical breast exam [CBE], mammogram, Pap test, colonoscopy/sigmoidoscopy, fecal occult blood test and prostate-specific antigen [PSA] test) and current compliance with cancer screening recommendations (CBE, mammogram, Pap test, colorectal cancer screening, and PSA test), with lifetime sexual assault as the independent variables. Colorectal cancer screening models were stratified by gender. All models adjusted for confounders. Sexual assault was associated with lower odds of ever receiving a PSA test and, for women, higher odds of ever receiving a colonoscopy or sigmoidoscopy. Sexual assault was associated with lower odds of current compliance with CBE, mammogram, Pap test, and PSA test screening recommendations. A history of sexual assault was associated with lower odds of current compliance with cancer screening procedures, with the notable exception of colorectal cancer screening. Less consistent patterns were seen for lifetime screenings. Results suggest that alternatives to currently recommended procedures (like self-collection of HPV [human papilloma virus] DNA) or modified screening procedures may be a promising route to increase current compliance with cancer screening among a population that may avoid these procedures due to pain or fear of retraumatization.
Introduction
Cancer screening makes the early detection and treatment of cancers possible. Although not all existing cancer screening procedures are equally effective (Jemal et al., 2015; Miller et al., 2014), population-wide screening has helped reduce incidence of more advanced disease (Meester et al., 2015; Myers et al., 2015; Vaccarella et al., 2014). Currently, there are cancer screening procedures that have been shown to reduce mortality from cancers of the breast (i.e., mammogram), cervix (i.e., Pap tests and HPV [human papilloma virus] testing), lung cancer (i.e., low-dose helical computed tomography), and colorectal cancer (CRC; colonoscopy, sigmoidoscopy, and fecal occult blood tests [FOBTs]) (National Cancer Institute, 2018). However, current screening compliance rates for some cancers, like CRC, are just below 60%, meaning many people are dying due to diseases that could be treated if diagnosed early (Meester et al., 2015). The reasons for not screening for cancer are multifaceted and include inconsistent recommendations by health care providers, lack of awareness of screening recommendations, health insurance status, decreased routine access to preventive care, and perceptions of pain or discomfort from undergoing screening, among others (Hsia et al., 2000; Keemers-Gels et al., 2000; Klabunde et al., 2005; Rutten, Nelson, & Meissner, 2004).
Sexual violence has been previously associated with likelihood of engaging in cancer screening among adults (Alcalá, Mitchell, & Keim-Malpass, 2018; Gandhi et al., 2010; Leite, Amorim, Primo, & Gigante, 2017). For example, women who experience childhood sexual abuse have higher odds of having a colonoscopy or sigmoidoscopy in their lifetimes and being currently compliant with CRC screening guidelines (Alcalá et al., 2018). However, childhood sexual abuse is not associated with odds of most other cancer screening behaviors and is sometimes associated with lower odds of screening, particularly in the case of cervical cancer (Alcalá, Mitchell, & Keim-Malpass, 2017; Alcalá et al., 2018; Alcalá, Keim-Malpass, & Mitchell, 2017; Farley, Golding, & Minkoff, 2002). Intimate partner violence is associated with lower odds of compliance with mammogram screening recommendations, but is not consistently associated with compliance with CRC or Pap test screening recommendations (Gandhi et al., 2010; Massetti, Townsend, Thomas, Basile, & Richardson, 2017). When examining a history of sexual violence (which could include childhood sexual abuse, intimate partner violence, and sexual assault), those with a history of sexual violence are less likely to be compliant with screening recommendations for mammograms, but no impact is seen for compliance with colorectal or prostate cancer screening recommendations (Watson-Johnson, Townsend, Basile, & Richardson, 2012). A review of studies examining the association between violence against women (which includes sexual and other types of violence) found that the evidence was inconclusive (Leite et al., 2017). Thus, available evidence suggests a complex relationship between sexual violence and cancer screening, where both the type of violence and the type of cancer screening are important to consider.
Emerging evidence suggests that individuals with a history of sexual violence may deliberately avoid cancer screening to avoid retraumatization brought about by screening procedures. For example, among women with histories of childhood sexual abuse, facets of the cervical cancer screening procedure can be triggering or retraumatizing (Gesink & Nattel, 2015). In particular, the context in which the screening procedure takes place may remind women of their prior abuse and the Pap smear procedure itself may parallel their experiences of sexual abuse (Cadman, Waller, Ashdown-Barr, & Szarewski, 2012). However, to date, this research has not examined if individuals with histories of sexual violence may avoid other cancer screening procedures for similar reasons.
To date, when existing literature has examined the impact of sexual violence on cancer screening, the focus has been primarily limited to the impact of childhood sexual abuse and broad measures of sexual violence. That is, child sexual abuse will encompass only sexual violence occurring when the victim is below 18 years, while sexual violence is a broad category encompassing a wide range of violence (i.e., childhood sexual abuse, sexual assault, and so on; Rape, Abuse & Incest National Network, 2018). As a result, experiences like sexual assault have remained under examined. Although sexual assault falls under the umbrella of sexual violence, it only includes sexual contact or behavior occurring without the explicit consent of the victim (Rape, Abuse & Incest National Network, 2018), even if the victim is a child (Murray, Nguyen, & Cohen, 2014). Specifically, sexual assault encompasses rape, attempted rape, and fondling or unwanted touching occurring without the victim’s consent (e.g., through use of force, incapacitation, coercion, or threats; Rape, Abuse & Incest National Network, 2018). Furthermore, existing research has overwhelmingly focused on current compliance with screening recommendations for women, thus ignoring ever screening (i.e., lifetime screening) and the cancer screening behaviors of men. Also, when various screening modalities exist to detect a particular cancer (such as breast cancer or CRC), the various modalities are not examined as independent outcomes. Independent assessment may be important since not all modalities are equally invasive (as is the case with the various CRC screening options) or are not equally recommended by experts (as is the case for clinical breast exams [CBEs] and mammograms).
In addition, much of the research into the impact of sexual violence on cancer screening utilizes data collected before the implementation of the Patient Protection and Affordable Care Act (ACA). This is important because the ACA improved access to cancer screening by improving insurance coverage and eliminating patient cost-sharing for some procedures recommended by the U.S. Preventive Services Task Force (USPSTF) for most private insurance patients and all Medicare patients, including many cancer screening procedures (Sabik & Adunlin, 2017). As such, improved access to screening and lower costs barriers to screening have resulted due to the ACA (Sabik & Adunlin, 2017). Consequently, the newly insured and the lower financial barriers among the insured create an opportunity to update existing research on the impact of sexual violence on cancer screening for the ACA era.
To address gaps in knowledge, the present study examined the impact of sexual assault on current and lifetime cancer screening, for a variety of screening procedures. These distinctions are important to make given the growing body of research showing that sexual violence is associated with increased odds of cancer (Coker, Hopenhayn, DeSimone, Bush, & Crofford, 2009; Nanthana & Nopporn, 2014).
Method
Data
Data for this study come from the 2014 Kansas Behavioral Risk Factor Surveillance System (BRFSS). This survey of adults, aged 18 years and older, in Kansas was conducted via telephone (both cell phones and landlines), using random-digit-dial. The BRFSS is administered annually and includes a core set of questions that match other state BRFSS surveys. Kansas, like other states, has optional question modules that are administered as the state chooses to. A total of 13,356 respondents participated in the survey and were 21 years or older (i.e., the age at which cancer screening is first recommended). Of these, 11,207 had complete data for the sexual assault variables.
Measures
The independent variable under examination was lifetime experience of sexual assault. The 2014 Kansas BRFSS included a sexual violence module that assessed this outcome. Respondents were first asked if they were in a safe place to answer questions about sexual violence. Those who said they were not, were not asked about their experiences with sexual violence and were not included in the present analyses. Those who said they were in a safe space were asked, “Has anyone ever had sex with you after you said or showed that you didn’t want them to or without consent?” Respondents were told that unwanted sex included “putting anything into your vagina [if female], anus, or mouth or making you do these things to them after you said or showed that you didn’t want to” and included being unable to consent for any reason (i.e., intoxication, sleep, fear of punishment or violence). Those responding affirmatively to the question were coded as having experienced sexual assault. Although earlier iterations of the sexual violence module in the BRFSS have included more questions about specific acts of sexual violence (Choudhary, Coben, & Bossarte, 2008; Watson-Johnson et al., 2012), this was not the case for the 2014 Kansas BRFSS. As a result, we use the term sexual assault to describe the outcome, as it more accurately describes the scope of this sexual violence module.
Dependent variables were comprised of measures of current compliance with cancer screening recommendations and ever screening (i.e., lifetime screening). Respondents were asked if they had ever received a particular screening procedure and then asked to indicate the number of years since they had received the procedure to determine if they were currently compliant with screening recommendations. Current compliance was based on screening recommendations in 2014, the time the data were collected (American Cancer Society, 2017; USPSTF, 2008). Variables were constructed to approximate screening recommendations, put forth by the American Cancer Society and the USPSTF. At the time of data collection, regular prostate-specific antigen (PSA) tests were not recommended and a strong recommendation for CBE on an annual basis (American Cancer Society, 2017) was not made. Current compliance measures were (a) CRC screening (via FOBT, colonoscopy, or sigmoidoscopy) for women aged 50 to 75 years, (b) CRC screening for men aged 50 to 75 years, (c) PSA test for men aged 40 years and older within the past 2 years, (d) CBE for women aged 40 years and older within the past year, (e) mammogram for women aged 40 years and older within the past 2 years, and (f) Pap test for women aged 21 to 65 years within the past 3 years. Ever screening measures were (a) PSA test for men aged 40 years and older, (b) CBE for women aged 40 years and older, (c) mammogram for women aged 40 years and older, (d) Pap test for women aged 21 years and older, (e) FOBT for women aged 50 years and older, (f) FOBT for men aged 50 years and older, (g) colonoscopy or sigmoidoscopy for women aged 50 years and older, and (h) colonoscopy or sigmoidoscopy for men aged 50 years and older. This coding was consistent with a prior study (Alcalá et al., 2018). Although the USPSTF has recommended co-testing (Pap testing plus HPV testing) for women aged 30 to 65 years since 2012, women were only asked about Pap testing when data were collected (USPSTF, 2018).
Several variables were included in multivariable analyses as potential confounders. Age (in years) was measured as a continuous variable. Race/ethnicity (non-Latino White vs. other race), educational attainment (less than high school, high school, or equivalent and more than high school), insurance status (insured vs. uninsured), lifetime cancer diagnoses (yes vs. no), and language of questionnaire administration (English vs. Spanish) were measured using categorical variables.
Analyses
Statistical analyses were conducted using Stata 14.2. Survey weights were used to account for complex survey design. Sample means and frequencies were calculated for study variables, as appropriate. Logistic regression models were used to calculate adjusted odds ratios (AOR) and 95% confidence intervals (CIs) of engaging in all cancer screening outcomes, from sexual assault. All analyses were restricted to relevant age groups and to complete data for that analyses. Logistic regression models accounted for confounders.
Results
Table 1 shows the weighted sample characteristics. Ever screening rates were highest for Pap tests (95.27%) and lowest for FOBT among men (33.80%). Current compliance rates were highest for mammograms (71.38%) and lowest for PSA tests (45.61%). Almost 9% of respondents reported having ever experienced sexual assault (8.88%). Rates were much higher for women (15.49%) than for men (2.0%) (not shown in table). On average, respondents were slightly younger than 50 years of age. Most respondents had more than a high school education, were insured, were female, took the survey in English, and had never received a cancer diagnosis. Because the survey was weighted to be representative of the adult population of Kansas, demographic characteristics are consistent with the study population.
Sample Characteristics for Kansas BRFSS 2014 Adults 21+ (N = 11,207).

Note. Responses are limited to all respondents aged 21 and above, unless otherwise noted. Sample size represents unweighted sample. BRFSS = Behavioral Risk Factor Surveillance System; PSA = prostate-specific antigen.
Table 2 shows odds of current compliance with cancer screening for prostate, breast, and cervical cancer screening recommendations, with sexual assault as the independent variable. Sexual assault was associated with 51% lower odds of PSA screening (AOR = 0.49, 95% CI = [0.25, 0.99]), 27% lower odds of CBE (AOR = 0.73, 95% CI = [0.58, 0.90]), 30% lower odds of mammogram (AOR = 0.70, 95% CI = [0.56, 0.87]), and 31% lower odds of Pap test (AOR = 0.69, 95% CI = [0.56, 0.84]). Sexual assault was not associated with odds of CRC screening for women (AOR = 1.19, 95% CI = [0.90, 1.57]) or men (AOR = 0.96, 95% CI = [0.46, 1.97]). For all outcomes except Pap tests among women, increasing age was associated with higher odds of cancer screening. Being insured and having more than a high school education were associated with higher odds of all current compliance outcomes. Race/ethnicity were not associated with any outcome.
Odds of Being Currently Compliant With Cancer Screening Recommendations, Kansas BRFSS 2014.
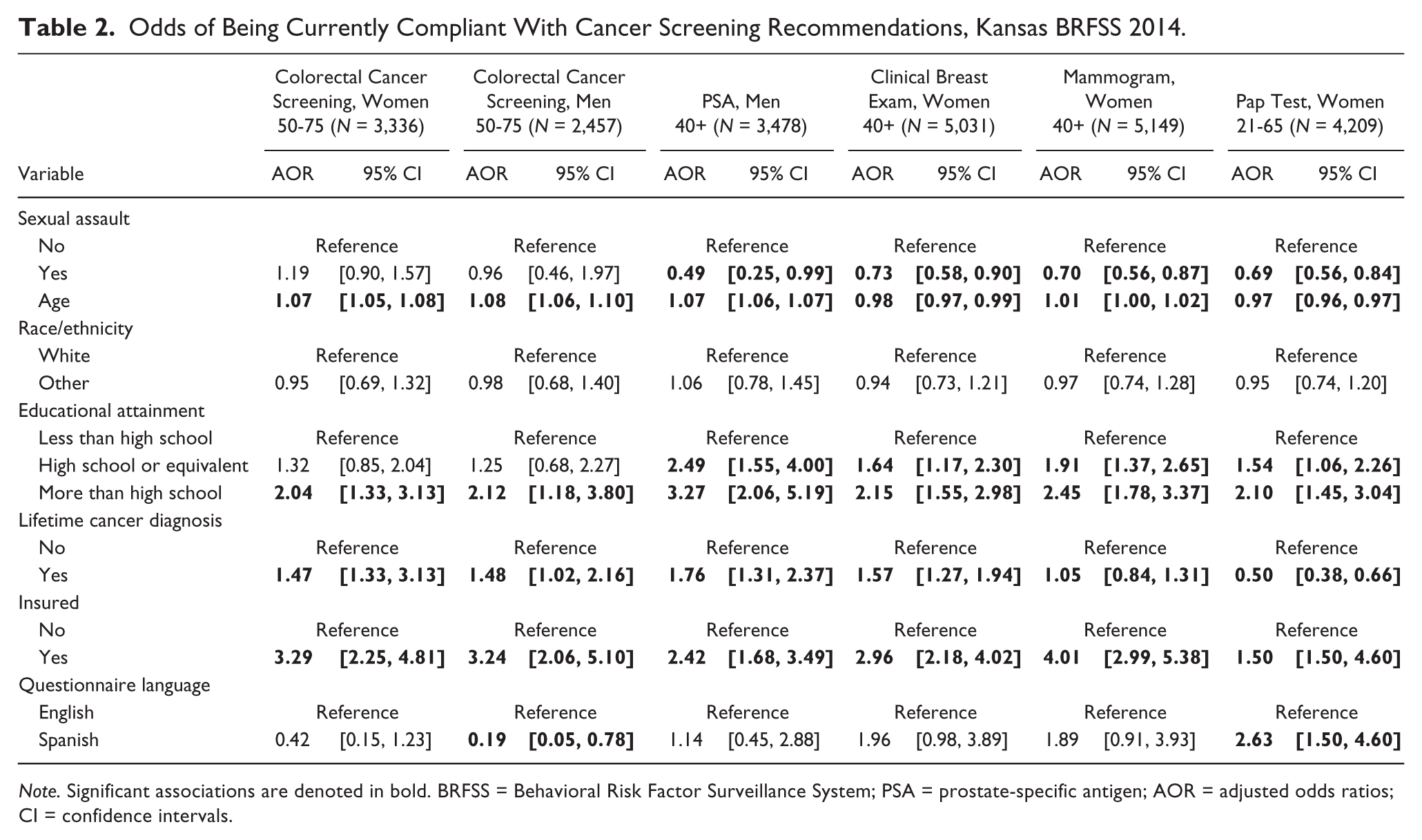
Note. Significant associations are denoted in bold. BRFSS = Behavioral Risk Factor Surveillance System; PSA = prostate-specific antigen; AOR = adjusted odds ratios; CI = confidence intervals.
Table 3 shows odds of lifetime cancer screening for prostate, breast, and cervical cancers, with sexual assault as the independent variable. Sexual assault was associated with 57% lower odds of PSA screening (AOR = 0.43, 95% CI = [0.22, 0.85]). Sexual assault was not associated with odds of CBE (AOR = 0.94, 95% CI = [0.58, 1.51]), mammogram (AOR = 0.95, 95% CI = [0.67, 1.33]), or Pap test (AOR = 1.06, 95% CI = [0.65, 1.73]). For all outcomes except CBE, increasing age was associated with higher odds of cancer screening. Having more than a high school education was associated with higher odds of all current compliance outcomes. Race/ethnicity and questionnaire language were not associated with any outcome.
Odds of Ever Screened for Prostate, Breast, and Cervical Cancer, Kansas BRFSS 2014.
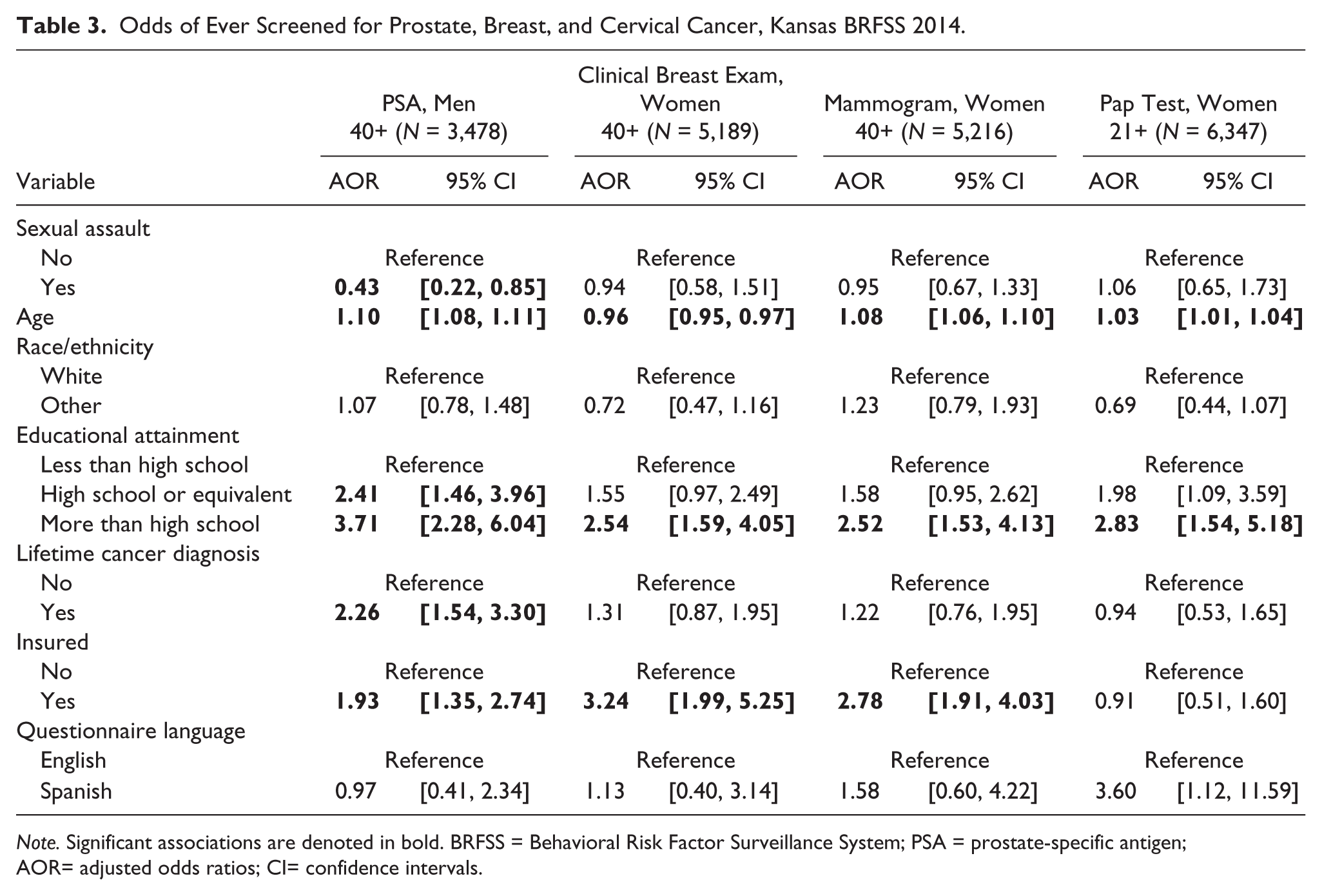
Note. Significant associations are denoted in bold. BRFSS = Behavioral Risk Factor Surveillance System; PSA = prostate-specific antigen; AOR= adjusted odds ratios; CI= confidence intervals.
Table 4 shows odds of lifetime use of FOBT or either colonoscopy or sigmoidoscopy to screen with sexual assault as the independent variable. Sexual assault was not associated with odds of FOBT use for either women (AOR = 1.02, 95% CI = [0.79, 1.30]), or men (AOR = 1.43, 95% CI = [0.70, 2.93]). Sexual assault was associated with 34% higher odds of colonoscopy or sigmoidoscopy for women (AOR = 1.34, 95% CI = [1.02, 1.75]), but not associated with odds of colonoscopy or sigmoidoscopy for men (AOR = 1.18, 95% CI = [0.55, 2.55]). For all outcomes except CBE, increasing age was associated with higher odds of cancer screening. Being insured and having more than a high school education were associated with higher odds of all outcomes. Race/ethnicity were not associated with any outcome.
Odds of Ever Screened for Colorectal Cancer, Kansas BRFSS 2014.
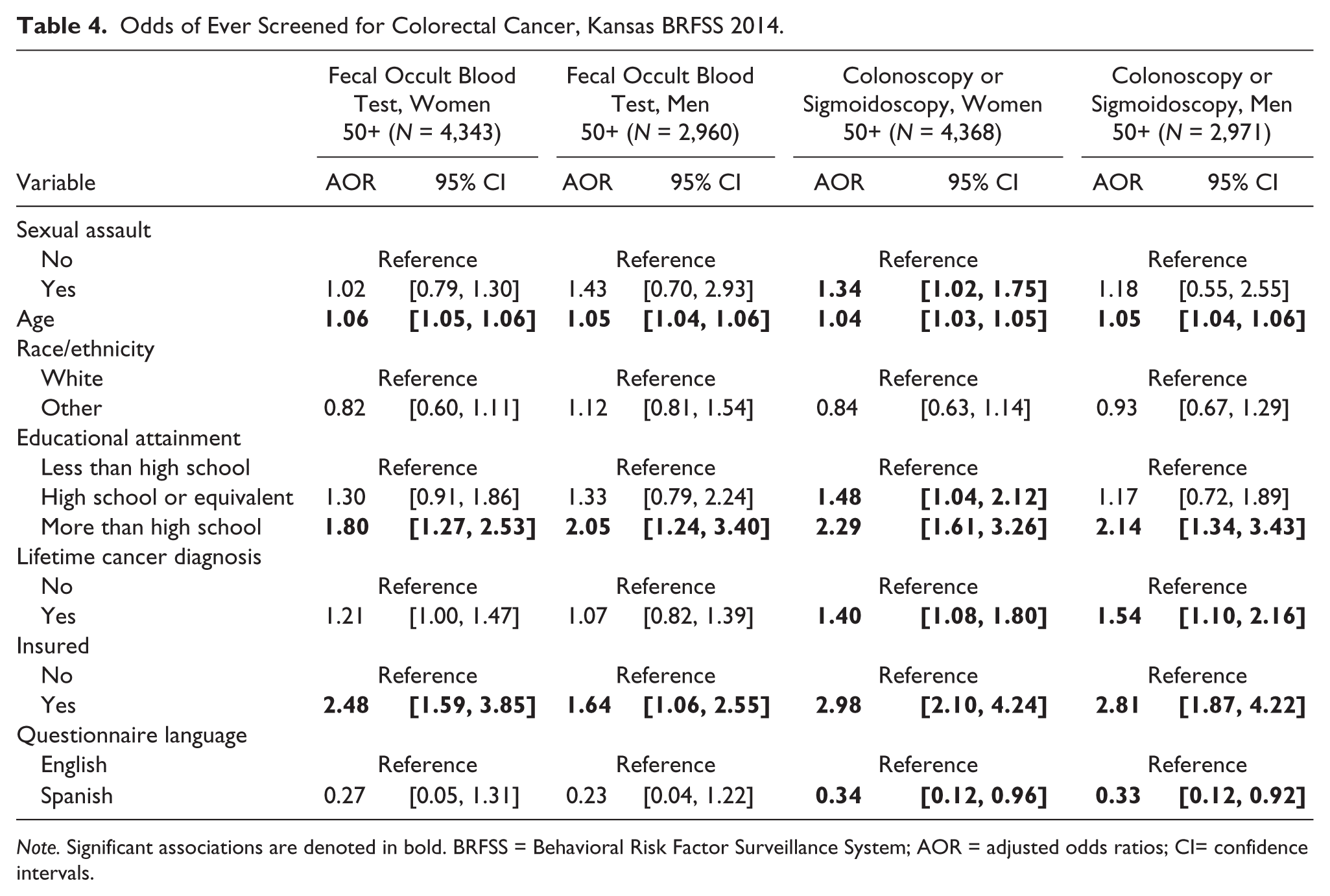
Note. Significant associations are denoted in bold. BRFSS = Behavioral Risk Factor Surveillance System; AOR = adjusted odds ratios; CI= confidence intervals.
Discussion
This population-based study demonstrated that lifetime experiences of sexual assault are, for the most part, associated with lower rates of cancer screening behaviors. Broadly, results suggested that the sexual assault had a negative impact on current compliance with most cancer screening procedures (with the exception of CRC screening). Conversely, the pattern for lifetime screening was less consistent, with higher odds of screening for some procedures observed for some outcomes. Most often, however, sexual assault was not associated with lifetime screening, even when it was associated with current compliance with the same type of screening procedures. Reasons for this discrepancy are unknown, but previous research has hypothesized that experiences of childhood sexual abuse may discourage repeat cervical cancer screenings because initial screenings may be retraumatizing and thus make future screenings uncomfortable (Alcalá, Mitchell, & Keim-Malpass, 2017). The physical pain and discomfort commonly reported during some cancer screening procedures (Dzuba et al., 2002; Keemers-Gels et al., 2000) may be a particularly effective deterrent to screening among those with a history of sexual assault. To ameliorate this, health care providers may consider screening procedures that are less invasive. For example, self-collection of HPV DNA has been associated with lower reports of pain relative to Pap tests (Dzuba et al., 2002). Although self-collection has lower sensitivity and specificity than physician collected samples (Arbyn et al., 2014), self-collection may still be a preferable screening modality for women who have experienced sexual assault and are not compliant with cervical cancer screening guidelines. Similarly, qualitative research among women with a history of childhood sexual abuse suggests that sharing of control, between a patient and a provider, during cervical cancer screening may be beneficial (Cadman et al., 2012).
This research expanded what is known about the impact of sexual violence on men. Partly because men experience sexual assault at lower rates than women (Finkelhor, Shattuck, Turner, & Hamby, 2014; Sorenson & Siegel, 1992), this has received less attention than sexual assault among women. Our study showed that men are less likely to be currently compliant or have ever screened for prostate cancer, via PSA, if they have experienced a sexual assault. Sexual assault was not associated with current compliance for CRC screening for either men or women; however, women were more likely to have ever received a colonoscopy if they had experienced sexual assault, while men were not. As a result, there may be gender-specific responses to sexual assault that need additional investigation, particularly because sexual assaults appear to “promote” screening among women.
Finally, across models, education emerged as the most consistent predictor of cancer screening. That is, higher educational attainment was associated with higher odds of lifetime cancer screening and current compliance with cancer screening guidelines. This is consistent with prior research (Damiani et al., 2015; Willems & Bracke, 2018). Prior work suggests education may make individuals more aware of their risk, increase their knowledge of health issues, and yield improved understanding of health information, like screening guidelines (Damiani et al., 2015). Although we cannot examine which of these mechanisms explain the association between education and cancer screening in this study, we can show that sexual assault is independently associated with cancer screening. Relatedly, having health insurance was associated with higher rates of undergoing most screening procedures, underscoring the importance of access to health care in cancer prevention, and the importance of eliminating all barriers to health insurance. These findings suggests that future work should consider past experiences and not just demographic characteristics when examining correlates of screening.
There are several limitations that one must consider when interpreting the results of the current study. First, the BRFSS is cross-sectional, and thus subject to biases including recall bias. Furthermore, directionality of the relationship between sexual assault and cancer screening cannot be established, although we lack a theoretical reason to suspect that the temporal sequence is the opposite of what was examined in the present study. Second, while we were able to examine lifetime use of two different CRC screening procedures, the BRFSS questions do not permit for the same analyses for current compliance with CRC screening recommendations. Third, because the data from this study are limited to one state, our findings may not generalize to other states, particularly those that are more racially diverse.
Conclusion
Despite limitations, our study provides insight into the largely negative impact of sexual assault on cancer screening. For population health, this is important to understand given the myriad of adverse health consequences faced by those with a history of sexual assault (Campbell, Dworkin, & Cabral, 2009; Golding, 1999). As the evidence showing an association between sexual violence and cancer screening continues to grow, efforts are needed to both understand why associations depend both on the abuse and screening in question. Furthermore, for clinical research, evaluating the impact of providing multiple screening options (particularly in the case of cervical cancer) appears to be a logical next step in ensuring barriers to cancer screening are reduced among an already vulnerable population. Finally, our study showed that even in an environment where costs of screening had lowered and access to screening had improved, sexual assault was an important correlate of current cancer screening compliance. As such, researchers and policy makers must consider other means to improve utilization of cancer screening for vulnerable populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.