
Abstract
The primary aim of the current study was to examine the prevalence and correlates of self-reported sexual assault (SA) perpetration, defined as nonconsensual sexualized touching or attempted or completed oral, vaginal, or anal penetration since starting college among men, women, and gender nonconforming (GNC) students. A secondary aim was to examine the prevalence and correlates of self-reported sexual encounters when the respondent was unsure that their partner consented (ambiguous consent). In spring 2016, 1,671 randomly sampled students (67% response rate) at two interconnected urban undergraduate institutions participated in an online survey about sexual experiences and personal and social contextual correlates. Prevalence estimates for SA perpetration and ambiguous consent were estimated and logistic regression was used to test bivariate associations between these two outcomes and a range of potential correlates. Approximately 2% of students self-reported any SA perpetration and 9% reported any ambiguous consent experiences since starting college. Pre-college SA perpetration, past-year SA victimization, belief in and use of nonverbal consent strategies, binge drinking, and depression symptoms were associated with higher odds of both SA perpetration and ambiguous consent while at college. Hookups were associated with higher odds of ambiguous consent; family social support was associated with lower odds of ambiguous consent. Findings of similar correlates for SA perpetration and ambiguous consent point to prevention programming focused on verbal consent strategies, alcohol harm reduction approaches, and pre-college interventions.
Introduction
Sexual assault (SA), which refers to nonconsensual sexualized touching (e.g., fondling private parts), attempted penetration (e.g., oral, anal, or vaginal sex), or completed penetration, is a significant problem on college campuses with 20% to 25% of women and 8% of men reporting exposure to SA victimization (Banyard et al., 2007). SA survivors report a host of negative physical, mental health, and economic sequelae (Peterson, DeGue, Florence, & Lokey, 2017; Ullman & Brecklin, 2003); thus, preventing SA is of critical importance. However, existing prevention programs have met with limited success (DeGue et al., 2014), highlighting the value of better understanding characteristics of those who commit SA and the contexts in which SAs are occurring to more effectively tailor prevention efforts.
Rates of self-reported SA perpetration vary by the definitions, instruments, and time frames used, and most studies have focused on convenience samples of men. For example, studies employing the widely used Sexual Experiences Survey (Koss & Oros, 1982) suggest that 12.5% to 14.2% of college men report perpetrating SA via verbal coercion, drug/alcohol incapacitation, or physical force in the previous year (Abbey & McAuslan, 2004; White & Smith, 2004). When perpetration is assessed using the same definition and instrument but broadening the time frame to “since age 14,” 26% to 35% of college men report perpetration (Abbey & McAuslan, 2004; Abbey, McAuslan, & Ross, 1998; White & Smith, 2004). Using the Conflict Tactics Scale (CTS), studies have found that 26.7% to 29% of male students and 13% to 19.6% of female students report perpetrating verbally coerced penetration while only 2.4% of men and 1.8% of women report perpetrating physically forced penetration (Gámez-Guadix, Straus, & Hershberger, 2011; Hines & Saudino, 2003). The CTS does not assess drug/alcohol incapacitated assault, and women and gender nonconforming (GNC) students have not been included in perpetration studies using the socioeconomic status (SES); thus, rates of drug/alcohol incapacitated perpetration in female and GNC students are undocumented. Few studies report the prevalence of perpetration since starting college; however, a longitudinal study following nearly 800 college men over 4 years indicated that nearly 29% of male students reported some act of sexual aggression during the 4 years (Thompson, Swartout, & Koss, 2013). To prevent SA and better understand the epidemiology of perpetration, data from representative samples of male, female, and GNC students that focus on the college period are needed.
The confluence model of sexual aggression (Malamuth, Heavey, & Linz, 1996) proposes that perpetration occurs through two independent pathways: (a) impersonal sex, which reflects emotional detachment within sexual relationships, and (b) hostile masculinity, which reflects negative views and objectification of women. Rape-supportive peers may play a significant role in promoting both pathways by providing opportunities (e.g., fraternity parties) for impersonal, often drunken sex to take place and espousing hostile views of women (Schwartz & DeKeseredy, 1997). Although this model has value in explaining male perpetration against female victims, it is heavily gendered and thus may not adequately explain perpetration by nonmale individuals or perpetration against male or GNC victims. An ecological approach that includes individual, immediate social environment/interactions, and broader social attitudes may serve to better explain perpetration more broadly. Individual factors that have been associated with perpetration in prior work include a personal history of childhood sexual abuse (Gámez-Guadix et al., 2011; White & Smith, 2004); a history of SA perpetration (White & Smith, 2004); alcohol consumption (Abbey & McAuslan, 2004; Abbey, Wegner, Woerner, Pegram, & Pierce, 2014), particularly binge drinking (Carr & VanDeusen, 2004); pornography viewing (Carr & VanDeusen, 2004; White & Smith, 2004); and depression symptoms (Nguyen & Parkhill, 2014). Recent data suggest that immediate social environments like parties and bars may be more predictive of perpetration than individual factors like binge drinking (Testa & Cleveland, 2016). Social groups such as fraternities and athletic teams have been associated with increased risk for perpetration (Humphrey & Kahn, 2000; Murnen & Kohlman, 2007), perhaps by creating environments that encourage a large number of casual sex partners or hookups (Abbey & McAuslan, 2004) and promulgate antiquated notions about sexual consent (Warren, Swan, & Allen, 2015). These environments also are often characterized by broader social attitudes reflecting rape myths acceptance, more hostile views of women, and more traditional beliefs about masculinity that have been linked with heightened risk for perpetration (Carr & VanDeusen, 2004; Thompson et al., 2013). Although few studies have examined potential protective factors, social environments such as church attendance have been linked with decreased risk for perpetration because they are associated with reduced binge drinking (Kingree, Thompson, & Ruetz, 2017). Testing whether factors at each of these ecological levels are associated with risk for perpetration is a critical next step in understanding how to more effectively tailor prevention programs.
Aims of the current study were fourfold. First, we examined the prevalence of college SA perpetration among male, female, and GNC students. Second, we described characteristics of these perpetration incidents, including year in school at time of the incident, gender of the perpetrator and victim, relationship to victim, where incident occurred, and substance involvement. Third, we examined various ecological correlates of perpetration including individual-level factors such as demographics, victimization, perpetration experiences, binge drinking, psychological well-being, and traditional/rape-supportive attitudes and beliefs, and social and interpersonal factors such as relationship status, fraternity/sorority and athletics involvement, religious participation, and social support. SA on college campuses has garnered significant media attention recently and universities have developed policies and programming to increase awareness and reporting. Consequently, social desirability concerns or fear of negative consequences (legal or institutional) may increase students’ reluctance to report perpetration. To partially address this concern, the fourth aim was to report the prevalence and correlates of a broader outcome that was suggested by the undergraduate advisory board that reflected having sex when the respondent was unsure that their partner’s consent had been given (henceforth referred to as ambiguous consent).
Method
Participants and Procedures
Data were collected for the Sexual Health Initiative to Foster Transformation (SHIFT) study, a large mixed-methods investigation of SA and sexual health among undergraduates. In spring 2016, a stratified random sample of 2,500 students from two interrelated undergraduate institutions was drawn from the population of 9,616 undergraduates aged 18 to 29 years. These 2,500 students, who sampled to reflect the demographic composition of the broader undergraduate student body (Mellins et al., 2017), were invited via email to participate in a web-based survey, and 67% (n = 1,671) enrolled. Few demographic differences existed between those who enrolled and those who were sampled, suggesting that the obtained sample was similar to the full student body (Mellins et al., 2017). Analyses focused on 1,583 students who answered questions about SA perpetration and 1,589 students who answered the ambiguous consent question.
Students accessed the online survey via a personalized link either at our on-campus office (16%) or other location of their choosing (84%). The informed consent process described confidentiality, incentives, data handling procedures, and ability to refuse questions prior to the 35- to 40-min survey. Participants received US$40 in cash or electronic gift card as compensation for their time and effort. All procedures were approved by an institutional research board (IRB).
Measures
Outcomes
SA perpetration
A modified version of the Sexual Experiences Survey–Revised (Koss et al., 2007) was used to assess SA perpetration since starting college as well as during the last academic year by asking three behaviorally specific questions about (a) sexualized touching (touched, kissed, fondled, or grabbed in a sexual way, but did not attempt sex); (b) attempted oral, anal, or vaginal penetration; and (c) completed penetration without the other person’s consent or agreement. Each question included six subquestions about tactics used (verbal arguments, pressure, threats to end the relationship/spread rumors; expressing criticism, anger, or displeasure; incapacitation including taking advantage when the other was too drunk to consent, passed out, asleep, or otherwise incapacitated; threats of physical harm; physical force; and other tactics). Participants who reported any perpetration received follow-up questions about up to three of the “most significant” incidents including gender of the victim, type of act, relationship to victim, where they met the victim, where the assault occurred, and whether substances were used.
Ambiguous consent
Due to concerns that social desirability would result in underreporting of SA perpetration, our undergraduate student advisory board suggested including a broader item, “Since starting college, have you ever had sex when you were not sure your partner’s consent had been given?” to capture participants who may have engaged in nonconsensual sex but were reluctant to disclose for social desirability reasons.
Correlates at the individual level
Demographics
Participants reported their age, race (White, Black or African American, Asian, American Indian/Alaskan Native, Native Hawaiian/Pacific Islander, or other), Hispanic/Latinx ethnicity, year in school (freshman, sophomore, junior, senior, or beyond), problems paying for basic necessities (never, rarely or sometimes, often, or always), current gender identity (male, female, GNC: transmale/transman, transfemale/transwoman, genderqueer or GNC, other), and sexual orientation (asexual, pansexual, bisexual, queer, heterosexual, homosexual, or other sexual orientations). For analytic purposes and due to small cell sizes, students were categorized into four mutually exclusive groups: heterosexual, bisexual, homosexual, and other (asexual, pansexual, queer, or other).
Victimization and perpetration history
Sexual abuse was assessed with a yes/no item adapted from the Adverse Childhood Experiences study (Felitti et al., 1998): “During your childhood or adolescent years, did an adult or person at least 5 years older than you ever touch or fondle you or have you touch them in a sexual way? Or attempt to actually have oral, anal, or vaginal intercourse with you?” Victimization prior to college was assessed with a yes/no item: “Prior to enrolling, did you experience unwanted sexual contact?” Perpetration prior to college was assessed with a yes/no item: “Prior to enrolling, did you EVER have sexual contact with someone without their consent or agreement?”
Pornography viewing
Participants received a single item about frequency of viewing pornographic material (magazines, movies, and/or Internet sites) with responses from never to daily/almost daily (Carroll et al., 2008). At least weekly viewers were those who reported weekly or daily/almost daily viewing.
Binge drinking and frequency of drinking/drug use prior to sex
An item from the Alcohol Use Disorders Identification Test (AUDIT; Saunders, Aasland, Babor, De la Fuente, & Grant, 1993) asked “how frequently participants consumed six or more drinks on a single occasion” with the following responses: never, less than monthly, monthly, weekly, and daily/almost daily. At least weekly binge drinkers were those who reported weekly or daily/almost daily binge drinking. Participants were asked how frequently they had used alcohol or drugs during or immediately prior to having sex in the past 3 months with five response options ranging from never to all of the time. Those who reported use at least half the time or more were coded as positive for alcohol or drug use prior to sex.
Psychological well-being
The Patient Health Questionnaire–9 (PHQ-9; Kroenke, Spitzer, & Williams, 2001) assessed past 2-week depression symptoms (current α = .88), with possible scores ranging from 0 to 27 and higher scores reflecting worse depression. Scores of 5 to 9 reflect mild depression. The Generalized Anxiety Disorder–7 (GAD-7) (Spitzer, Kroenke, Williams, & Löwe, 2006) scale assessed past 2-week anxiety symptoms (current α = .91) with possible scores ranging from 0 to 21 and higher scores reflecting worse anxiety. Scores close to 5 reflect mild anxiety. The 10-item Rosenberg Self-Esteem Scale (Rosenberg, 1965) was used to assess self-esteem, with possible scores ranging from 0 to 30 and higher scores reflecting worse self-esteem (current α = .90). Scores above 15 reflect low self-esteem.
Traditional and rape-supportive beliefs and attitudes
Seven items from the “she lied” and “he didn’t mean to” subscales of the Illinois Rape Myths Acceptance scale (Payne, Lonsway, & Fitzgerald, 1999) were summed (current Cronbach’s α = .89) to assess rape myths (i.e., misperceptions about who is responsible for rape or SA). Possible scores ranged from 7 to 35 with higher scores reflecting greater acceptance of rape myths. Ten items from the Hostility Toward Women Scale (Lonsway & Fitzgerald, 1995) were summed (current α = .72) to assess negative attitudes or beliefs about women. Possible scores ranged from 10 to 50 with higher scores reflecting greater hostility toward women. Four items from the Traditional Attitudes About Men Scale (McCreary, Saucier, & Courtenay, 2005) were summed to assess traditional masculinity (e.g., ideas that men must be physically strong and not display signs of weakness; current α = .89). Possible scores ranged from 4 to 20 with higher scores reflecting more traditional beliefs about masculinity. Five items from the Sexual Consent Norms subscale of the Sexual Consent Scale–Revised (SCS-R; Humphreys & Brousseau, 2010) were summed to assess beliefs about sexual consent (current α = .67). A sample item is “I think that asking for consent verbally is awkward.” Possible scores ranged from 5 to 25 with higher scores reflecting lower beliefs in the importance of asking for consent verbally.
Correlates at the social/interpersonal level
Sexual relationships
Participants were asked about having had the following romantic or sexual relationships since starting college: steady/serious or exclusive/monogamous; onetime or ongoing hookups; or no relationship. Mutually exclusive groups were created so those who reported any hookup were classified as having hookups (even if they also had steady or exclusive relationships) whereas those who reported only steady or exclusive relationships or no relationship were classified accordingly.
Use of nonverbal consent tactics
Five items from the Indirect Behavioral Approaches to Consent subscale of the SCS-R (Humphreys & Brousseau, 2010) were summed (current α = .53) to reflect use of verbal consent behaviors. A sample item is “Typically, I communicate sexual consent to my partner using nonverbal signals and body language.” Possible scores ranged from 5 to 25 with higher scores reflecting less frequent engagement in verbal consent behaviors.
Fraternity/sorority and athletic team participation
As part of a larger question about campus activities, participants were asked (yes/no) whether they had ever been (a) a fraternity/sorority member or (b) on a varsity athletic team. For this article, we focused only on these two activities given their association with perpetration in previous studies (Murnen & Kohlman, 2007).
Perceived social support
Five Likert-type items from the Perceived Social Support From Family and Friends (PSS-FR; Procidano & Heller, 1983) were averaged to reflect support from family (current α = .94), and 10 yes/no items from the PSS-FR were averaged to reflect support from friends (current α = .86). Possible scores for family and friend social support ranged from 1 to 5 and 0 to 1, respectively. Higher scores on both reflected greater perceived social support.
Statistical Analysis
All analyses were conducted in SAS version 9.4. Prevalence of perpetration was estimated overall and separately among men, women, and GNC students and characteristics of perpetration incidents were described. Separate logistic regressions yielded odds ratios (ORs) and 95% confidence intervals (CIs) that reflected bivariate associations between any perpetration and the potential correlates; covariates were not included in any models. Prevalence of ambiguous consent also was estimated overall and separately by gender, and bivariate associations between ambiguous consent and all correlates were estimated. To ensure that findings observed for ambiguous consent were not driven by the small number of participants who reported both ambiguous consent and perpetration (n = 9), a sensitivity analysis removing all participants who reported any perpetration was conducted.
Results
Sample Characteristics
Participants were male (40.8%), female (57.8%), and GNC (1.6%) students aged 18 to 29 years. Slightly more than half (54.8%) were between the ages of 18 and 20, with relatively even distribution across year in school (freshman, sophomores, juniors, and seniors). Race/ethnicity was as follows: 43.5% were non-Hispanic White, 8.4% Black, 15.1% Hispanic, 23.6% Asian, and 9.5% Other. Just under half reported rarely or sometimes (40.8%) or often or always (7%) having difficulty paying for basic necessities.
Prevalence of SA Perpetration
Since starting college, 2.1% of the sample (n = 34) reported any perpetration; the most common form was sexualized touching (n = 27), whereas the least common was completed penetration (n = 8). Approximately 3.3% (n = 21 of 632) of men, 1.4% (n = 13 of 921) of women, and 0% (n = 0 of 26) GNC students reported any perpetration. Compared with women, men reported a higher prevalence of unwanted touching (0.9% vs. 3.0%; Fisher’s exact χ2, p = .0024) but an equivalent prevalence of completed penetration (0.5% for both). Overall, 1.3% of the sample (2.1% of men and 0.9% of women) reported any perpetration since the start of the academic year. Because zero GNC students reported perpetration, characteristics of incidents and correlates of perpetration could not be examined in this group.
Characteristics of SA Perpetration Incidents
Among the 34 students reporting perpetration, additional questions were asked for the “most significant” incidents as defined by the students who could answer these follow-up questions on up to three incidents. Most students only answered questions on one incident; thus, data were available for 37 total incidents (Table 1). Most incidents occurred when the perpetrator was a freshman with decreasing incidents reported over time, which could in part reflect that all participants had not experienced all years of college yet. More than half of incidents involved sexualized touching only, whereas a smaller, equivalent number involved attempted and completed penetration. Many incidents involved taking advantage while the victim was incapacitated but lies, threats, or verbal pressure and showing displeasure, criticizing, or getting angry were also common. For male perpetrators, most victims were female, whereas for female perpetrators, most victims were male. Perpetrators identified many victims as friends, but casual sex partners and intimate partners were also reported. Two thirds met the victim at college, and two thirds of incidents occurred on campus, primarily in a dorm. Substance use by the perpetrator was reported in more than half of incidents.
Characteristics of “Most Significant” Sexual Assault Perpetration Incidents (n = 37).
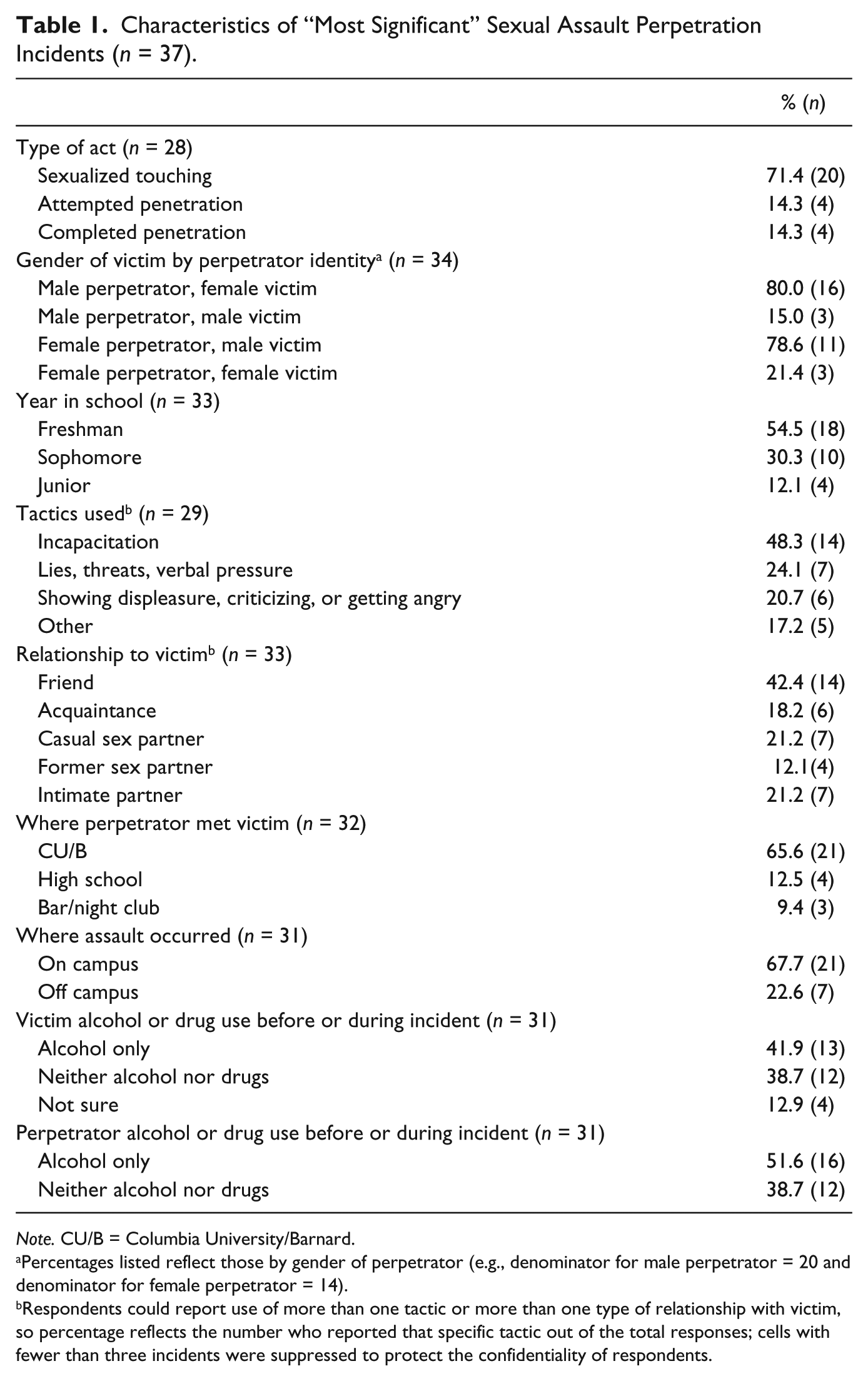
Note. CU/B = Columbia University/Barnard.
Percentages listed reflect those by gender of perpetrator (e.g., denominator for male perpetrator = 20 and denominator for female perpetrator = 14).
Respondents could report use of more than one tactic or more than one type of relationship with victim, so percentage reflects the number who reported that specific tactic out of the total responses; cells with fewer than three incidents were suppressed to protect the confidentiality of respondents.
Statistically Significant Correlates of SA Perpetration
As shown in Table 2, correlates of perpetration included past-year sexual victimization (OR = 3.0), SA perpetration prior to college (OR = 5.5), monthly binge drinking (OR = 2.3), higher depression (OR = 2.0), higher levels of traditional masculinity (OR = 1.5), and greater belief in nonverbal consent communication (OR = 2.1). Social/interpersonal correlates included more use of nonverbal consent strategies (OR = 3.4).
Bivariate Logistic Regression Analyses Examining Correlates of Any Sexual Assault Perpetration.
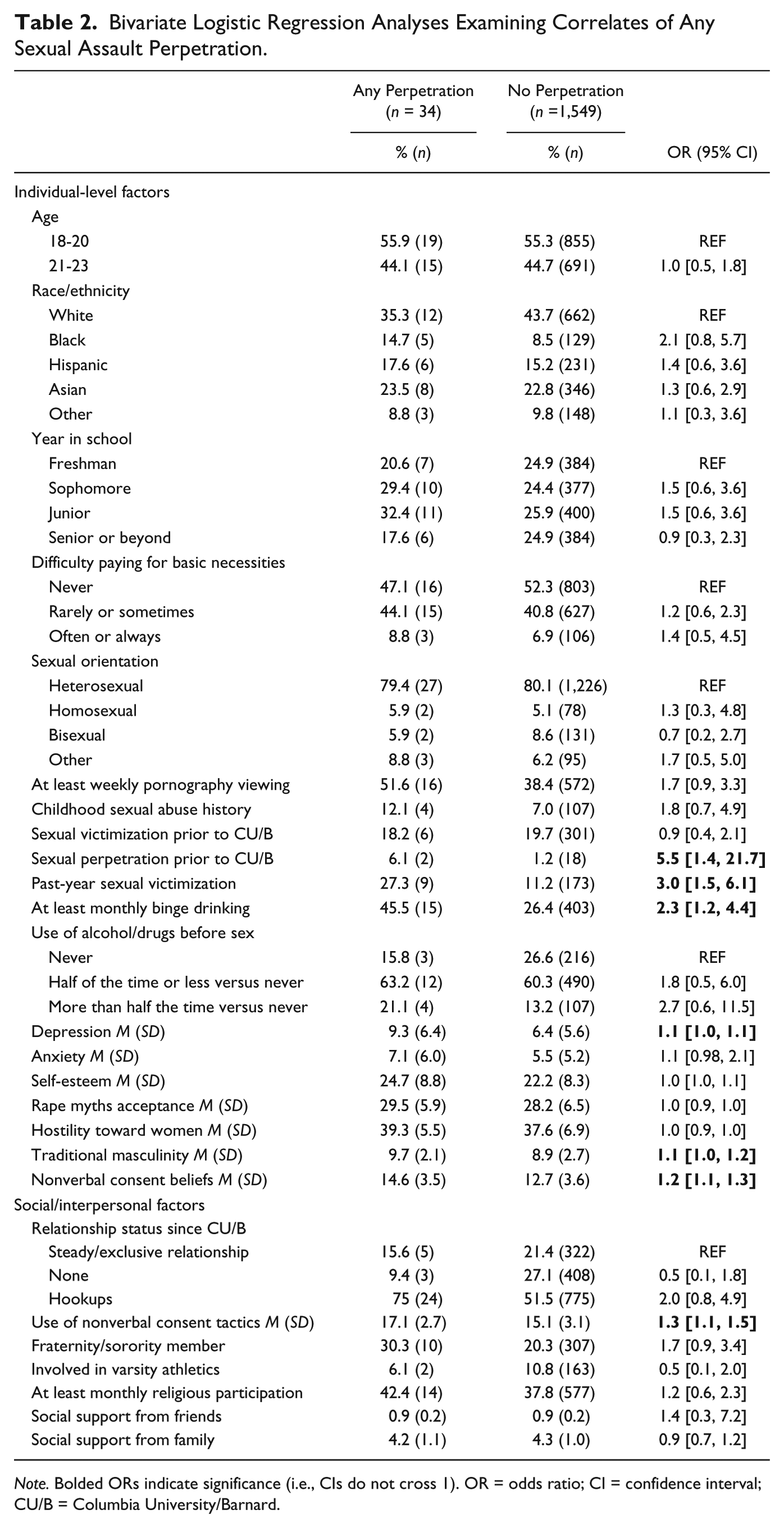
Note. Bolded ORs indicate significance (i.e., CIs do not cross 1). OR = odds ratio; CI = confidence interval; CU/B = Columbia University/Barnard.
Prevalence of Ambiguous Consent
Overall, 9% (n = 144) said yes to the ambiguous consent item with 9.7% of women (n = 90), 7.8% of men (n = 50), and 15.4% of GNC students (n = 4) reporting ambiguous consent. Approximately 26.5% (n = 9) of those who reported any perpetration also reported ambiguous consent.
Statistically Significant Correlates of Ambiguous Consent
As shown in Table 3, correlates of ambiguous consent included older age (OR = 1.4 for those 21 years or older vs. 18-20 years); higher year in school (OR = 1.7-2.6); identifying as Hispanic (vs. White; OR = 1.5); rarely/sometimes (OR = 1.4) or often/always (OR = 2.4) having difficulty paying for basic necessities (vs. never); identifying as homosexual (OR = 2.3) or other sexual orientation (OR = 2.4) versus heterosexual; experiencing childhood sexual abuse (OR = 3.0) and sexual victimization prior to college (OR = 2.2) as well as within the past academic year (OR = 5.1); reporting perpetration prior to college (OR = 3.5); monthly binge drinking (OR = 2.2); more frequent use of alcohol/drugs before sex (OR = 2.2); worse depression (OR = 1.8), anxiety (OR = 1.5), and self-esteem (OR = 1.7); and higher rape myths acceptance (OR = 1.4) and greater belief in nonverbal consent practices (OR = 1.3). Social/interpersonal correlates included having hookups (vs. steady/exclusive relationships; OR = 4.7) since starting college, use of nonverbal consent tactics (OR = 1.7), and fraternity/sorority participation (OR = 1.8). Sensitivity analyses on the ambiguous consent outcome excluding all 34 participants who reported any perpetration revealed similar patterns of findings to those observed for ambiguous consent in the broader sample, suggesting that results were not driven by those who reported perpetration. Analyses are available upon request.
Bivariate Logistic Regression Analyses Examining Correlates of Ambiguous Consent.
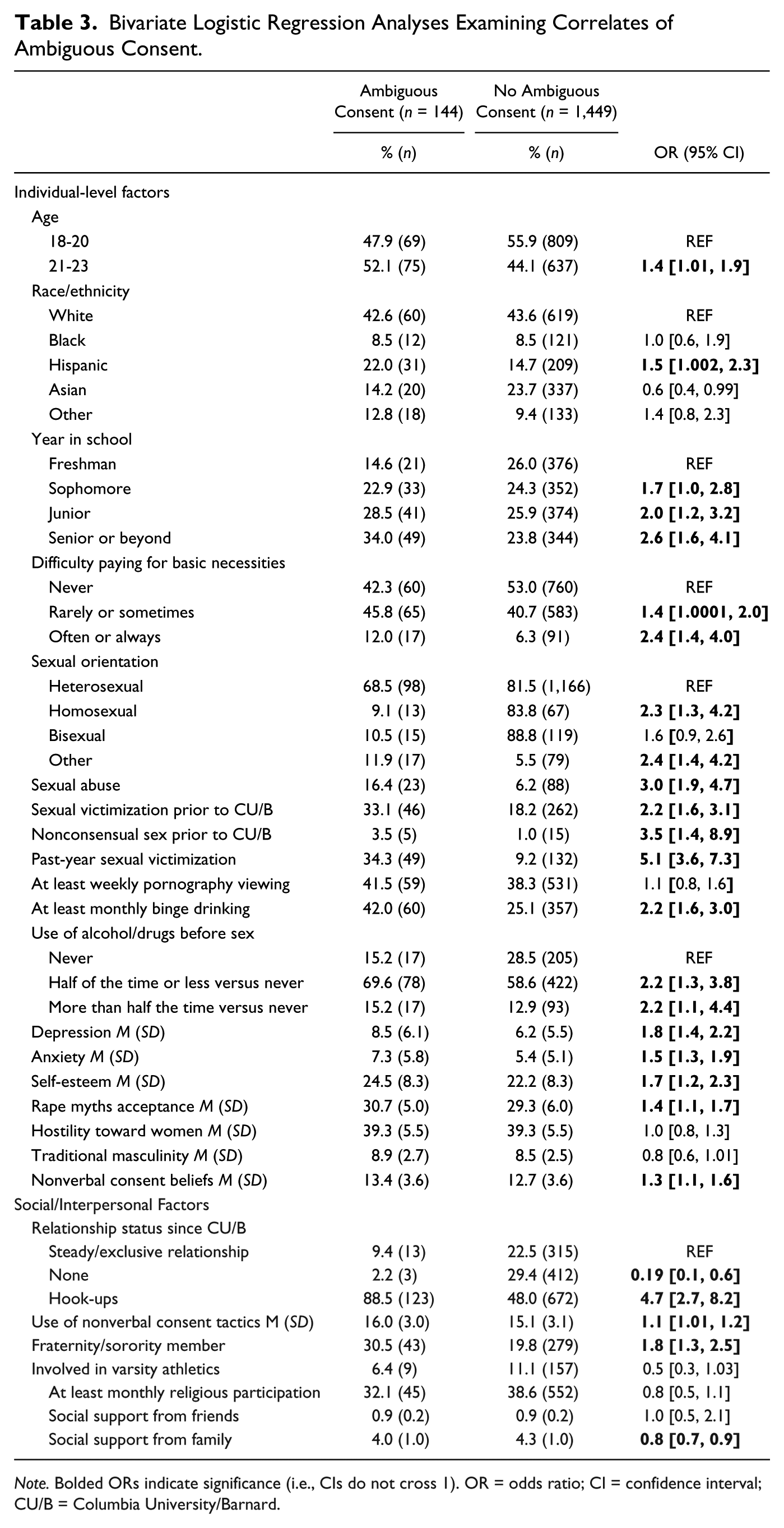
Note. Bolded ORs indicate significance (i.e., CIs do not cross 1). OR = odds ratio; CI = confidence interval; CU/B = Columbia University/Barnard.
Discussion
This study examined the prevalence and correlates of SA perpetration and ambiguous consent in a large, representative sample of male, female, and GNC students. Overall, a very small percentage, 2.1%, reported any SA perpetration since starting college although a higher percentage, 9%, reported ambiguous consent. Common individual-level correlates of both outcomes included past-year SA victimization, pre-college SA perpetration, binge drinking, and depression symptoms, while social and interpersonal correlates that were common to both outcomes included belief in and use of nonverbal consent strategies. The overlap in these correlates across outcomes suggests some validity to consider ambiguous consent as a broad proxy for perpetration given concerns about underreporting and social desirability with direct asking about perpetration.
Compared with previous work showing that 12.5% to 14.2% of male students reported any perpetration within the previous year (Abbey & McAuslan, 2004; Abbey et al., 1998), only 2.1% of men in the current study reported any past-year perpetration. It is highly unlikely that actual rates of perpetration are declining as victimization rates using the same instrument in this same sample appear stable and consistent with prior work (Mellins et al., 2017). Many of the studies finding higher prevalence of college SA perpetration were conducted more than a decade ago; thus, it is possible that recent public conversations and policies about SA, including mandated training on consent, have led to a shift in attitudes, whereby increased stigmatization of perpetration has increased social desirability bias in reporting. This may be particularly true at the campus from which these data were collected (e.g., a student carried her mattress around for the duration of her college experience to protest the administration’s handling of her SA case); however, research from other universities is critical to support or refute this hypothesis. To partially address concerns about stigma and underreporting, we included a question at the suggestion of the undergraduate advisory board about sex when one’s partner may not have consented and did indeed find that a larger percentage (9%) of the sample endorsed this item; thus, this broader wording may be less stigmatizing and prone to social desirability issues. Underreporting of sexual perpetration on these self-report measures has been found recently by other research teams as well. For example, men who were told their responses were being monitored by a lie detector–type test were 6.5 times more likely than men who were not told their responses were being monitored to report illegal SA strategies on the SES (Strang & Peterson, 2016). Thus, the perpetration estimates obtained here may reflect the small percentage of students who are not deterred from reporting due to social desirability concerns rather than the actual percentage of students who perpetrated SA. Another, albeit unlikely possibility is that the measurement of sexual perpetration in the current study led to reduced reporting. Specifically, the SES-R’s six separate questions for attempted and completed oral, vaginal, and anal penetration were reduced to two questions—one about attempted penetration and one about completed penetration—and each question included all three penetration types. These modifications are unlikely to have impacted prevalence estimates; however, as noted previously, identical modifications to the victimization questions with this same sample did not result in reduced reporting (Mellins et al., 2017).
Men were twice as likely to report perpetration compared with women, which is consistent with studies examining verbal coercion and forced SA using the CTS (Gámez-Guadix et al., 2011). Given that women are reporting some sexually aggressive behavior, explanatory models that are heavily gendered such as the confluence model of sexual aggression (Malamuth et al., 1996) may need to be expanded to adequately explain female perpetrators. No GNC students reported perpetration, which may reflect the small percentage of GNC students in our sample. When ambiguous consent prevalence was examined by gender, GNC students had the highest prevalence (15.4%), although this represented only four GNC students. GNC students may be less likely to ask for verbal consent due to fear of rejection. They also may be more attuned to sexual boundaries and what constitutes consent given that they were more likely to report SA victimization in a previous paper (Mellins et al., 2017). Women (9.7%) and men (7.4%) also reported higher prevalence of ambiguous consent than perpetration. Female college students are more likely than male students to conceptualize consent as an active, verbal process (Jozkowski, Peterson, Sanders, Dennis, & Reece, 2014); however, few students actually use affirmative verbal consent when engaging in sex (Hirsch et al., 2018). Consequently, although this item was intended to capture students who were unwilling to report perpetration due to social desirability concerns, it is possible that this item also captured students who were aware that their behavior did not meet verbal consent standards, but they may not necessarily have had sex that was unwanted by the other party.
Consistent with prior work on perpetration (Abbey et al., 2014; Nguyen & Parkhill, 2014; Warren et al., 2015; White & Smith, 2004), several individual-level correlates including prior history of perpetration, binge drinking, and depression symptoms as well as social- and interpersonal-level correlates such as nonverbal consent beliefs and use of nonverbal consent tactics were associated with both perpetration and ambiguous consent in the current sample. Findings suggest a strong need for perpetrator interventions prior to college enrollment as well as harm reduction approaches to binge drinking and mental health treatment during college. In addition, prevention programming targeting consent beliefs and practices should be emphasized.
Contrary to prior work, pornography viewing at the individual level and varsity athletic participation at the interpersonal level were not associated with either outcome. Prior work has suggested that violent pornography specifically has been associated with reduced likelihood of bystander intervention for men (Foubert & Bridges, 2017); thus, violent pornography may be more important to assess than overall pornography viewing frequency. In terms of athletics, there is wide variation in social prestige of different teams both within and across universities; however, all sports were considered together here, potentially masking differences in perpetration risk among subgroups.
Some correlates, including sexual minority status, precollege sexual victimization, anxiety, poor self-esteem, and fraternity/sorority participation, were only associated with ambiguous consent but not perpetration. Although the low sample size for perpetration may have limited statistical power to detect associations, sexual minority students report more use of nonverbal compared with verbal behaviors to indicate consent (Beres, Herold, & Maitland, 2004), which may in part account for the high prevalence of ambiguous consent reported here. Similarly, prior assault victims may be more attuned to consent as a result of their own experiences and therefore more likely to report ambiguous consent. Anxiety and poor self-esteem may contribute to confusion and ambiguity in sexual encounters by making people less assertive, or heightened anxiety and worse self-esteem may be a function of having ambiguous sexual encounters. Finally, fraternity/sorority members may have more exposure to social situations in which alcohol or drugs are commonly used prior to sex and sexual consent is perhaps not attuned to as carefully.
Clinical Implications
Three novel findings with intervention potential emerged. First, perpetrators and those reporting ambiguous consent also may be coping with recent victimization experiences. Although temporal sequencing is unclear, data suggest a need for programs for survivors to consider that students who are likely to perpetrate assault or report ambiguous consent also may have victimization experiences. Typically, perpetrators are not allowed into safe spaces for victims of SA—yet students who are both victims and perpetrators may then not have any devoted space for addressing their concerns and difficulties. Second, students who reported hookups were more likely to report ambiguous consent, suggesting that engaging in casual sexual relationships may increase risk for nonconsensual sex. Developing programming to help students negotiate their sexual relationships and boundaries to have safe, healthy, and wanted sex may be important. Third, higher levels of perceived family social support were associated with lower odds of ambiguous consent. Social support has been considered an important factor in victims recovery from SA (Ullman, 1999), but the current findings highlight the potential importance of strengthening family bonds to reduce the likelihood of engaging in nonconsensual sex.
Limitations
Findings should be considered in the context of study limitations. First, data were cross-sectional, precluding conclusions about temporal sequencing. Longitudinal studies are critical to better understand predictors of perpetration and ambiguous consent. Second, although the ambiguous consent question may measure perpetration that students do not want to admit, it also may be capturing sex that did not involve explicit verbal consent, but was not unwanted by the other. This question also was narrow in that it only asked about potentially nonconsensual sex (vs. sexual touching more broadly). Third, measures like the SES-R were adapted for brevity (e.g., we did not ask separate questions for oral vs. anal vs. vaginal penetration, but rather asked one question across all three types), which may have influenced the obtained estimates; however, use of this adapted measure to assess victimization has yielded estimates that are consistent with previous literature (Mellins et al., 2017). Fourth, although we reported on the prevalence of perpetration and ambiguous consent among GNC students, correlates could not be separately examined among GNC students due to the small sample size in our study (n = 26). Fifth, the perpetration sample size was small (n = 34), suggesting that correlates should be interpreted with caution and replication is necessary. Finally, although students in the current study were representative of the demographics of the university, findings may not generalize to other universities.
Despite these limitations, this study illuminates correlates of SA perpetration and ambiguous consent. Findings suggest similar correlates for perpetration and ambiguous consent that are consistent with previous studies and point to a need to consider precollege interventions as well as alcohol harm reduction approaches and formal training around sexual consent practices, which may be improved by strengthening family bonds. Finally, many victim-centered clinics have strict “no perpetrators” policies; thus, universities should consider how to provide services to perpetrators who also may have victimization histories.
Footnotes
Acknowledgements
The authors thank our research participants; the Undergraduate Advisory Board; Columbia University, and the entire SHIFT team who contributed to the development and implementation of this ambitious effort, particularly our quantitative research assistants Karimata Bah and Stephanie Benson.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Columbia University through generous support from multiple donors.