
Abstract
The Domestic Violence Enhanced Home Visitation (DOVE) intervention used in the Perinatal Nurse Home Visiting Intervention Enhanced With mHealth Technology (RCT: R01HD071771) is a nurse-lead evidenced-based intervention that has been shown to decrease violence overtime. This summative mixed-methods impact evaluation is intended to provide insight to enhance the DOVE IPV protocol for screening and intervention by (a) identifying which core aspects of DOVE facilitated or inhibited its success and what was most critical to optimal IPV (intimate partner violence) screening and intervention practices, (b) informing how DOVE IPV screening and intervention were influenced by the experiences of home visitor (HV), and (c) identifying policy considerations and best practice recommendations for the DOVE protocol. Participants were HVs and managers (N = 13) in rural/urban home visiting programs delivering DOVE across three states. The sample had a mean age of 48.76. Three fourths were baccalaureate-prepared nurses with an average of 10.5 years of home visiting experience. The method used in this study was one-to-one qualitative in-depth interviews with HVs. Data were interpretively analyzed using Nvivo 10 to generate three themes. Participants endorsed screening women for IPV with DOVE being the approach of choice to facilitate IPV screening and intervening with women. HVs found DOVE helped enhance their IPV knowledge, screening, and intervening capabilities while filling an existing void in this type of preparation of HV nurses. Establishing a relationship with the women before initiating screening was an important aspect in delivering DOVE as was the training, support, and increased comfort level in addressing IPV. The evidence offers an understanding of which core aspects of DOVE contributed to its success and what was most critical to optimal IPV screening and intervention practices. Furthermore, this evaluation provided multilevel insights into how best to advance home visiting practices and policies when screening and intervening with perinatal women exposed to IPV.
Keywords
Violent intimate partner relationships present significant risks to the health of mothers and their children during the perinatal period and infancy. According to the Centers for Disease Control and Prevention (Breiding, Basile, Smith, Black, & Mahendra, 2015), intimate partner violence (IPV) is “physical violence, sexual violence, stalking and psychological aggression (including coercive tactics) by a current or former intimate partner (i.e. spouse, boyfriend/girlfriend, dating partner, or ongoing sexual partner)” (p. 11). An estimated 3% to 9% of women experience abuse while pregnant (Martin, Mackie, Kupper, Buescher, & Moracco, 2001; Saltzman, Johnson, Gilbert, & Goodwin, 2003), with higher rates for women who are younger or non-White (Agrawal, Ickovics, Lewis, Magriples, & Kershaw, 2014). Recent population-based research shows that pregnancy fails to offer protection against the most catastrophic outcome of IPV victimization. Intimate partner homicide is the fifth leading cause of death during pregnancy, with 2.2 to 6.2 homicides per 100,000 live births, a rate 1.84 times that of nonpregnant/postpartum women (Wallace, Hoyert, Williams, & Mendola, 2016). Being young, Black, undereducated, or not married increases the risk of pregnancy-associated homicide 2.34 to 5.57 times (Wallace et al., 2016). Infancy offers little immunity from the violence. Children less than 3 years of age represent 27.7% of child abuse cases, with the highest victimization rate for those under 1 year (U.S. Department of Health and Human Services, Administration for Children and Families, 2015).
Programs that couple IPV screening and intervention in the perinatal period are limited and few comprehensive evaluations of these programs exist (Hooker, Small, & Taft, 2016; Sharps et al., 2016), particularly from the health care providers’ (HCP) perspective. This study is part of a larger summative program evaluation of the Domestic Violence Enhanced Home Visitation (DOVE) phase 2 study (RCT: R01HD071771). DOVE is an IPV intervention to reduce “violence for women experiencing current violence or violence in the year before pregnancy, using community health nurse prenatal/postpartum home visitation by random assignment to the DOVE intervention or usual IPV care” (Sharps et al., 2016, p. 1130). Findings from the first DOVE trial revealed a significant decrease in IPV overtime from baseline through postpartum for women in the DOVE treatment group (Sharps et al., 2016). The aims of this study were to (a) identify which core aspects of DOVE facilitated or inhibited its success and what was most critical to optimal IPV screening and intervention practices, (b) inform how DOVE screening and intervention are influenced by the experiences of home visitors (HVs), and (c) identify policy considerations and best practices recommendations arising from the DOVE protocol.
Background and Significance
Impact of IPV in Perinatal Period
Perinatal IPV occurs in the year before, during, and/or after pregnancy (Sharps et al., 2016). It can result in a wide variety of long-term physical and mental health issues, in addition to direct trauma inflicted as the result of physical or sexual violence. Victims of IPV are more likely to experience insufficient or inconsistent prenatal care; have poor nutrition; inadequate weight gain; substance use including smoking, alcohol, and other substances; an increased prevalence of depression and stress; and sexual risk taking including inconsistent condom use, unplanned pregnancy, or abortion (Agrawal et al., 2014; Alhusen, Ray, Sharps, & Bullock, 2015; Kothari et al., 2016; Moats, Edwards, & Files, 2014). In addition, there is also an association between IPV and sexually transmitted infections or urinary tract infections, higher rates of suicide (Alhusen et al., 2015), and long-term health consequences occur even if the victim is able to leave the abuser (Black, 2011). Women abused during pregnancy are at higher risk of IPV 6 to 12 months after giving birth (Bianchi, McFarlane, Cesario, Symes, & Maddoux, 2016). Beyond physical and mental health issues, the social and economic costs of IPV during the perinatal period are high (Kirst et al., 2012). Health care costs for women who are abused are 33% to 42% higher than for non-abused women (Moats et al., 2014), with more than 25% of women who are injured requiring medical treatment (Black, 2011).
Newborns whose mothers are victims of IPV have been shown to exhibit higher rates of morbidity including low birth weight (LBW), preterm birth, small for gestational age (SGA), and neonatal mortality rates up to 8 times higher (Alhusen et al., 2015; Bailey, 2010; Black, 2011; Moats et al., 2014). LBW and preterm birth are leading causes of neonatal mortality and morbidity, and newborns who experience SGA are more likely to experience behavioral or developmental issues (Alhusen et al., 2015). Children of mothers abused during pregnancy are also more likely to experience negative behavioral outcomes like depression and withdrawal or anger and hostility (Bianchi et al., 2016). Children who witness or are exposed to IPV also have higher risk for abuse themselves, with as many as one third of youth who witness violence having been maltreated in the previous year (Hamby, Finkelhor, Turner, & Ormrod, 2010).
Conflicting Guidance on Screening
Screening for IPV continue to be debated (Bacchus et al., 2016a; McLennan & MacMillan, 2016; O’Doherty et al., 2015) and is often underutilized (Bianchi et al., 2016; de Boinville, 2013; Hooker & Taft, 2013). Furthermore, programs that couple IPV screening and intervention in the perinatal period are limited and few comprehensive evaluations of these programs exist (Hooker et al., 2016; Sharps et al., 2016), particularly from the HCPs’ perspective.
The 2010 U.S. Patient Protection and Affordable Care Act (PPACA) mandated insurance coverage for IPV screening and brief counseling at no additional cost (de Boinville, 2013). The U.S. Preventive Services Task Force’s (2018) final recommendation indicates that effective interventions for women exposed to IPV of childbearing age has a net benefit in reducing abuse and recommend screening these women and making referrals for intervention and services for those who screen positive. This recommendation is supported by the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN, 2015) and the American Congress of Obstetricians and Gynecologists (2012).
Yet, the World Health Organization (WHO) does not recommend universal screening, noting that evidence indicates that screening increases identification of abused women, but it has not been shown to reduce violence or improve health outcomes (WHO, 2013). However, the WHO does recommend that the antenatal setting may be appropriate for routine screening, given vulnerabilities due to pregnancy, and evidence indicating potential for improved health outcomes for these women. A 2015 Cochrane review also concluded that screening increases the identification of women experiencing IPV, particularly in the antenatal setting; however, they found no evidence of an effect on outcomes such as referral, ongoing exposure to violence, or harm because of screening (O’Doherty et al., 2015).
Multiple Barriers Result in Low Screening Rates
Barriers and failure to screen by HCPs have been contributed to many reasons that have resulted in a wide variation of screening rates (Bailey, 2010; Taft et al., 2015). Bailey’s (2010) review of literature examining the experience of IPV during pregnancy found a range of physician reported screening rates between 6.2% and 65%. Lack of time (AWHONN, 2015; Bailey, 2010; Bair-Merritt et al., 2014; Black, 2011; Kirst et al., 2012), lack of provider knowledge or training (Alhusen et al., 2015; AWHONN, 2015; Black, 2011; Kirst et al., 2012), and provider stress, discomfort, or feelings of inadequacy (Alhusen et al., 2015; Bailey, 2010; Bair-Merritt et al., 2014; Black, 2011; Eddy, Kilburn, Chang, Bullock, & Sharps, 2008) are the most frequently identified HCP barriers to screening for IPV. Other barriers include fear of offending patients (Alhusen et al., 2015; Black, 2011), perceived risk of interfering with provider–patient relationship (Eddy et al., 2008), or concern that screening may cause harm (Kirst et al., 2012). Providers’ personal experiences with abuse (Alhusen et al., 2015; Black, 2011) and frustration with client’s failure to disclose or respond to intervention (Alhusen et al., 2015; Bailey, 2010; Eddy et al., 2008) are additional barriers.
Lack of clear guidance on screening and lack of interventions to address IPV when identified (Alhusen et al., 2015; AWHONN, 2015; Bailey, 2010; Bair-Merritt et al., 2014; Black, 2011; Eddy et al., 2008; Kirst et al., 2012) present significant challenges to HCPs. In a longitudinal randomized control trial of maternal child health teams that mandated provider training and screening with postpartum women as part of usual care reported screening at higher proportions, and a significant sustained increase in safety planning than the comparison teams (Taft et al., 2015). Findings from this screening model support approaches that embedded robust IPV training and support of HCP which is critical given that the vast majority of abused women (76%) report having never been screened for IPV during pregnancy (Bianchi et al., 2016).
The DOVE
The DOVE intervention was tested in two multisite randomized control trials (RCT: NR009093 and R01HD071771). The first DOVE trial (n = 239) was conducted from 2006 to 2012 across 13 rural and one urban site with seven health agencies delivering DOVE and six offering their usual care (Sharps et al., 2016). The DOVE intervention included an evidence-based brochure that was used to provide structured abuse screening for IPV using the Abuse Assessment Screen (AAS; Parker & McFarlane, 1991) and the Women’s Experience With Battering (WEB) tool (Smith, Earp, & DeVellis, 1995), and a six-session empowerment intervention based on Dutton’s Empowerment Model (Parker, McFarlane, Soeken, Silva, & Reel, 1999). It was delivered primarily by home visiting nurses in two states as part of preexisting perinatal home visiting programs. Usual routine care of four to six prenatal visits and six to 12 postpartum visits up to 2 years was given to all women in the home visiting programs. HVs participating in DOVE received extensive initial and ongoing training and support on IPV, the cycle of violence, and the study training protocols. Each home session consisted of a review of a brochure on the cycle of violence, an assessment of risk factors of homicide using the danger assessment (Campbell, Webster, & Glass, 2009), review of available local and national resources, and safety planning specific to the needs of the client. With a brochure that provided a structured basis for each encounter, each HV was encouraged to modify the content of discussions to the experiences of the client and threat level within the home (Bacchus et al., 2016b). All HVs were to deliver the DOVE intervention 6 times during routine home visits, ideally divided equally between the pregnancy and early postpartum periods (Sharps et al., 2016). There was a significant reduction in IPV from baseline through 24 months postpartum (p < .01) after accounting for age and maternal depression (Sharps et al., 2016).
The second DOVE trial (HD071771) (2012-2016) was expanded to three states with both rural and urban locations. The second trial tested delivery of the DOVE screening and DOVE intervention using an mHealth application delivered on a tablet device compared with the original pen and paper versions of the same screening and intervention (cycle of violence, danger assessment, and safety planning; Bacchus et al., 2016b). HVs followed the same routine home visiting procedures as they did in DOVE 1, and they were present when women randomized to the mHealth group and used the tablet for the delivery of the screening and the DOVE intervention. For women randomized to the paper and pen group, the HV delivered both the screening and the DOVE intervention face-to-face. DOVE research coordinators provided comprehensive on-site training to all HVs that involved an overview of IPV, a video demonstrating HV use of DOVE in a three-segment case scenario, and role-playing exercises using practice cases. Following initial training, all HVs were provided refresher training as needed and supportive ad hoc consultations by the research coordinators.
Formative evaluation results from mothers and HVs from the second trial focused primarily on the use of technology (Bacchus et al., 2016a). The purpose of this article is to present this study’s findings with the intent of providing valuable practice and policy insights and recommendations about the use of DOVE for IPV screening and intervention and second, its overall benefit for HVs, families, other HCPs, and programs.
Method
This study is part of a summative mixed-methods impact evaluation conducted on the DOVE protocol using a qualitative interpretive design. Study protocol, consent form, and recruitment materials were approved by the University of Virginia Institutional Review Board (IRB). Between May 2015 and January 2016, 67 HVs and managers were contacted. The DOVE research coordinator provided a list of active HVs and their contact information from every site and helped to disseminate recruitment fliers. These efforts yielded 15 participants, with two unable to attend scheduled interviews. Ultimately, 13 HVs participated. Large HV caseloads, heavy complex work-loads, and the fact that most HVs are in the field and do not come into the office on a regular basis contributed to limited availability and/or time for their participation in this study. After obtaining informed consent, the PI (principal investigator) conducted in-person hour-long interviews at each site using a semistructured interview guide containing 13 open-ended questions with prompts.
Analysis
All interviews were digitally recorded, transcribed verbatim then analyzed and coded using Nvivo 10. Transcripts were first reviewed separately by the PI and one of the co-authors who then met after the initial review to compare codes. Both individuals had identified similar, and in some instances identical, codes which were used to develop nodes for analysis. Data were then thematically analyzed (Fereday & Muir-Cochraine, 2006; Patton, 2002) and interpreted by both the PI and co-author based on the identified nodes. From this process, nine core nodes and 27 subcategories of nodes evolved to inductively generate emergent (axial codes) and convergent (selective) codes. Throughout this inductive process, the data were interpreted concurrently to formulate relationships between the larger data and emerging patterns (Thorne, 2008) that created themes. Themes were confirmed by both the PI and co-author during multiple encounters to ensure credibility and increase accuracy of the analysis.
Sample
Most of the convenience sample came from two sites (n = 6; n = 5) with two from a third site; all of the HVs were predominantly from rural sites with only two from an urban site that was located in the third state. All participants were female and the majority (76%) self-identified as White with the remainder identifying as Black, Hispanic, or Asian. The mean age of HVs was 48.76. Seventy-six percent had a minimum bachelor’s education. The HVs averaged 10.5 years of home visiting experience and carried an average caseload of 29.8 family cases, ranging between 12 and 95 families. Eleven of the HVs were nurses. Most reported none or very little targeted experience supporting women exposed to IPV before being involved with DOVE.
Results
These findings are based on the thematic analysis of 13 HV who participated in the DOVE trial and consented to this study. Analysis of the interview data revealed three main themes: (a) leveraging the utility of screening and intervention, (b) creating an empowering platform for nurses and families, and (c) enhancing and promoting the quality of current and future practice.
Leveraging the Utility of Screening and Intervention
Several participants spoke not only of the importance of screening and intervening with women for IPV but also found added benefits to screening that extend its more traditional use as only a tool for identifying IPV exposure. HVs found that the screening process opened doors for conversations that might not otherwise have happened. Finding out whether or not a woman has been exposed to IPV is critical, as is the conversation that screening generates about violence against women which raises awareness of the issue. That conversation helps to protect women by teaching them how to be and stay safe regardless of whether or not they had experienced IPV. For those who do screen positive for IPV exposure, the DOVE intervention serves to reinforce keeping women safe.
From this perspective, screening offers multiple uses beyond its intended purpose of identifying abused women. It can be an important tool for health promotion and to share information about IPV. Participants identified that screening women for IPV gave them the opportunity to promote healthy relationships and discuss what an abusive relationship is.
I’d just say my most positive feeling about it [screening] is that it’s a very good springboard. It’s an opening no matter if it’s a positive screen or a negative screen, it’s a very good springboard into the topic of healthy relationships and um and in the cases where you know, where it is a positive screen . . . doing interventions and it’s just kind of flows well, and its, it’s what we want to do because this person is a mom and we want to help end the cycle of violence. (HV, rural)
As a mechanism for prevention, HVs felt that screening was helpful for women who may have had a past history of abuse talk with them with regard to avoiding abuse in future relationships. For women in an abusive relationship, screening enabled them to define the relationship as abusive, creating a gateway for exploring options to enhance their safety, assess their level of danger, and access community resources. It was also an important way for women with no abuse history to get information that could be useful in the future and that they can share with other friends and family members. Through DOVE, women were taught to recognize abusive patterns and behaviors which they could use for themselves or share with other women as described by one of the HV’s: . . . what I do is, I still find a way to bring it in there and how I go about it is . . . I’m glad that this is not something that you’ve had to deal with in your life, but you may have a girlfriend or a family member that you might notice something’s just not quite right, and you’ll be talking to her so let me tell you what the cycle is and it may trigger something with your friend and then know that there is a shelter here in town . . . (HV, rural)
Screening became a way to increase knowledge and awareness of IPV in the lives of very vulnerable families and brought this knowledge and awareness to the forefront of nursing practice. Many HVs spoke of screening enhancing their “intuition” about potential abuse issues that might not have been as apparent in their family caseload; through DOVE they became attuned to the various and subtle ways that abuse takes shape in families. This HV (rural) explains, “I think it’s increased our own awareness of uh domestic violence issues.” Another remarked, . . . you know I have a greater acuity to pay attention to the whole person and I try to do that anyway but I, I think that without the intervention research going on and us participating in it, that I may not have noticed that, you know.
She felt that DOVE helped “being more uh attuned to situations um things that don’t seem quite right, just being more aware . . . more sensitive to it (HV, rural).
Prior to DOVE some HVs admittedly did not have IPV on the forefront of their radar. They would conduct home visits without a systematic approach to identify and intervene with abused women, unaware that they were attempting to treat symptoms (depression, stress, anxiety) while abuse exposure remained an unexplored root cause negatively affecting health outcomes. One HV acknowledged that we didn’t have a framework within our program to talk about it [IPV] or to even say where it fit in . . . [DOVE] made it more formal, you know IPV more on the same level with prenatal depression . . . early childhood delays those kinds of things. (HV manager, rural)
In some cases, HVs identified that they had been using a scaled back screening tool that did not pick up on the more insidious aspects of IPV and hence created false negative screens that were only caught when DOVE screening tools were used.
. . . well I mean we have a relationship assessment tool that we administer at the beginning of the relationship, right before the mom is due . . . it’s not as sensitive of a tool . . . um so my very first client that I screened she was negative on the RAT [Relationship Assessment Tool] and then came up positive on the WEB [DOVE tool], so I might have eventually figured that out somewhere down the line anyway. (HV, urban)
Approaches used in the past by some of the HVs included IPV screening only, stopping short of any intervention. The DOVE intervention pamphlet is a resource that supports HVs in intervening with abused women and was viewed as an essential component of DOVE. It has been described as the key to DOVE’s success as this HV (rural) explained, “it doesn’t matter if we identify a problem if we don’t have a solution; it does matter if we identify a problem but the most important part is the solution to the problem.” The HVs found that the breadth of the information contained within the pamphlet very useful in increasing their knowledge and awareness and also gave them concrete information to offer women. This allowed the HVs to have resources at their fingertips to immediately help abused women and their children. HVs also used the DOVE intervention to teach women exposed to IPV that they are not alone, they have options, and to increase a woman’s awareness of danger signs of abusive relationships.
Creating an Empowering Platform for Nurses and Families
One of the most empowering aspects of DOVE for the HVs was gaining knowledge and having a clear process for responding to women who screen positive for IPV. HVs felt that this “increased confidence” in their ability to support women exposed to IPV. The routineness of the screening and intervention created less angst and more comfort for the HVs. What occurred was a normalization of the conversation about IPV and how to respond to it through the repetition of using DOVE with every family. One participant mentioned she was so comfortable with screening that . . . we can walk through [names large store] and I’m going to go up and ask that girl if she’s been hit, kicked, slapped or otherwise abused this year because it just comes out of our mouths . . . It doesn’t freak us out the way it used to. (manager, rural)
Discomfort with IPV screening is a known barrier that HCPs need to overcome. With the support of DOVE, HV were able to overcome this obstacle mostly due to its predictable approach in initiating discussion about IPV, then responding and intervening with families experiencing IPV. Having a standardized approach serves to mitigate the anticipatory distress caused by not knowing how to approach the topic of IPV and what to do if a woman is being exposed to IPV. Furthermore, participants from sites where supervisors and colleagues regularly practice debriefing as a group or one-on-one feel that this practice gave them an additional layer of support needed for adopting IPV screening and interventions.
The majority of HVs affectionately spoke of the DOVE coordinator who was seen as an integral part of DOVE’s successful implementation and often they expressed gratitude for the ongoing support and intensive training the coordinator provided.
I’ve learned a lot from the training, you know sometimes it’s one of those things, you know that, for example, in nursing school you don’t really talk about. (HV, urban) I definitely think the training that I received I mean was probably the, you know utmost importance and help for me. (HV, rural) I think having like the training of you know well what is it, and how do you handle it and what are the resources here in (name’s county) is very important . . . um . . . I don’t think if I would have had that training I, I mean I don’t think I’m the best nurse at this, but I think it’s made me a better nurse at it. (HV, urban)
Clearly training was deemed to be a critical tool across all sites that enhanced HV comfort and support to deliver DOVE IPV screening and intervention. However, beyond the training provided the coordinators’ relationship with the sites was paramount.
. . . well and um you know she’s just, any questions we have and really she kind of keeps us on our toes as well, you know in a, in a very nurturing and positive way, but she didn’t let us get, you know off on the wayside. The other thing is we consider ourselves such a small part of it, we don’t have that many families but I think it’s accurate, she’s made us realize or that we are a pretty big part of, of this. (HV manager, rural)
HV awareness of the critical role they as HCPs play in addressing IPV become more pronounced as a result of DOVE, and the impact of DOVE on the lives of the women they serve was pronounced. Several HVs fondly reflected how using DOVE helped to “reveal strengths” particularly for very vulnerable mothers with an array of adverse life experiences. HVs spoke of DOVE being an important vehicle for showing women options. It was a tool for encouraging and supporting woman as they start to use and apply those options to change their lives because as one HV notes DOVE is “busting up the foundation”; one riddled with cumulative trauma histories and family dysfunction.
. . . to actually fill it out and be willing to say, yeah you know this is going on opens the door for all of it to just start what I call kind of um busting up all of that bad foundation so we can together lay one where, a realistic one because you are someone, you are a valid person, you do matter, you are worth more. (HV, rural)
Among many of DOVE’s empowering attributes is that it promotes women’s self-efficacy, self-esteem, and their sense of self-worth simply by giving women the power of knowledge in how to respond when and if a violent situation arises.
In stages and in other parts it sets up the goal, long term short term goal process with them because if I can successfully do this then I can now begin to integrate that into other areas of my life . . . this is doable for every area of my life. (HV, rural)
Women learn what “red flags” to look for in their current or future relationships. A HV (rural) described the importance of “not letting women off the hook” when they identify abuse in a past relationship. Instead it’s an opportunity to say “ . . . let’s talk about your past, why you might be drawn that way, what can be a red flag?” which this HV attributed to DOVE as the catalyst for taking that “extra step” which otherwise “might not have been taken.” So even if the woman is not presently in an abusive relationship it does not mean that she won’t be. For women who are in abusive relationships DOVE intervention offers hope. One HV remarked, . . . for the ones who have screened positive you know and didn’t want to talk about it um, I, I think that again it’s given them options to know they don’t have to, they don’t have to be, they’re not stuck as it may seem. (HV, rural)
Another participant shared that the intervention gave young women the “opportunity to begin to believe that they can get out of it” (HV, urban).
Routine discussions of IPV elevate it to the forefront as a topic “that has to be talked about . . . has to be normalized, not the acceptance of it, but the rejection of it.” This HV felt strongly that as we begin to look at IPV we . . . reject it [IPV] as normal and say this is not normal, this is not acceptable, then you’re going to see a different side of how men treat women, interact with women, how women expect to be treated, and expect to be interacted with. (HV, rural)
Such transformative effects speak to DOVE’s impact beyond a woman’s current circumstance. Successfully addressing abuse empowers women to feel they can achieve success in other aspects of their life. Despite the many empowering properties of DOVE, consideration for the capacity of the local community to support women’s help seeking is one aspect that DOVE’s referral component cannot account for. This does not mean that referrals should not occur. It simply means that however well intended, DOVE’s ability to intervene is limited by contextual factors beyond the control of the intervention such as scarcity of local resources and transportation particularly in rural communities.
“Transportation is a big, big issue, um if the client doesn’t have a car or a means to get to the safe house then that’s the big, the big deal and I have several of those.”
“How do you work around that?”
“You don’t most of the time, you know unless the police sometimes will take them”
Sadly, this situation is not unique and can be disheartening even for the most ardent advocate.
Enhancing and Promoting Quality of Current and Future Practice
When HVs knew that their upcoming visit would involve the use of DOVE, many discussed specifically preparing for that visit by ensuring they review DOVE materials in advance to get into the mind-set to discuss IPV. What HVs realized is that even with training and routine use of DOVE, diligence requires they refresh their knowledge to deal with whatever disclosure and follow-up might occur. This HV (urban) identified that “we (HV) need to stay educated on interpersonal violence, you know we need to continue to get um education on that. You just don’t go to one seminar and then you know it all.”
Sufficient preparation was essential to quality delivery of DOVE screening and intervention and to respond effectively to an IPV positive screen. How HVs respond to disclosures of abuse can potentially have adverse consequences for women. Therefore, IPV screening and intervening was approached by the HVs with a seriousness warranted given the severity and impact of the issue in the lives of women exposed to it. Being unprepared, not knowing what to say or what resources are available in the community, how to assess danger and how to help women safety plan, was seen as an unacceptable practice. Participants spoke of their desire to have up to date information about local resources for abused women in their community. Knowledge of local resources to support women became an expectation embedded into the HVs practices as a direct result of implementing DOVE.
Well I think um since we’re doing DOVE it makes us more aware of our need to stay informed about what resources there are in the area, um you know . . . what’s new, what’s gone away because that happens as well. (HV, rural)
DOVE enhanced the quality of HV screening practices in its consistent and systematic approach to IPV screening and intervening. This systematic approach provided HVs a fairly standardized approach to introducing and conducting screening and in the delivery of the intervention where “everybody had the same information, and were doing the same thing” (HV, rural). One HV noted that they appreciated the DOVE approach in helping alleviate their fear of not knowing what to do, particularly with a disclosure of IPV as most of their prior exposure was limited to screening only. The implementation of DOVE with all women created consistency that HVs found comforting in its routineness and normalization of IPV screening and intervention.
Formalizing DOVE as a routine part of HV’s practice was seen by some HVs as key to helping decrease stigma and exposing IPV. Still, in the routineness of this process it is equally important for HVs to have as network of support for themselves to debrief, address vicarious trauma or past history of personal trauma. As one HV manager (rural) wisely advised, . . . my number one would be . . . you have to be real with yourself, be honest with yourself, if you have not, if you have not buried that [your own past history of abuse] then you, you may need counseling to deal with it. Before you, you know . . . on the plane what do they say, get your own oxygen first then help somebody else because you cannot, you cannot help a person effectively from a broken place.
Another HV emphasized the importance of having a “small group” of peers to debrief with while another stressed the importance of having weekly meeting to “get together and debrief.” The DOVE coordinator was also mentioned as a critical part of this support network.
Incorporating DOVE helped HVs become more holistically attuned to the families they support as it refined their perspective to notice things that they might not have noticed before and shed light on a stark reality that could have otherwise been overlooked. They now know “what to look for” (HV, rural). Another HV (rural) states, I’ve been surprised myself with the screen sometimes um someone that I would give the screen to that I would have just almost assumed and no history of domestic violence and introduced this, I see it and I’m like wow okay this is really something we need to talk about . . . it wouldn’t have happened if we hadn’t had the DOVE tool.
Moreover when compared to other screening tools that had been used in the past with families HV found that DOVE screening tools demonstrate greater sensitivity in identifying abused women.
I mean the [home visiting program] had their, their paperwork is good, I
mean their questionnaire is good, it gets good information, but it’s rather
limited um and by introducing the WEB scale . . . I think that adds more to
gain in depth information because again, you know women don’t
understand that these behaviors, you know, if he can look at you and terrify
you that’s a sign . . . and they don’t, they think that’s just how it’s supposed
to be . . . So the WEB scale . . . and we didn’t do the WEB scale before we
started DOVE, so um I think that’s been beneficial. (HV, rural)
Fundamentally HVs supported DOVE yet still there were challenges. The research components proved to be an obstacle confronting the HVs before they could even initiate screening. Consistent with IRB protocol, every woman had to provide informed consent to participate in DOVE; a process that HVs found to be lengthy and arduous and off putting to women.
. . . well I mean the thing that a lot of them don’t like is the, you know the process of the consent. It’s again very long and tedious and I kind of get tired of it and then a lot of them, some of them that might have been okay with doing the study, it takes so long to go through the steps that sometimes they’re like oh I’m not interested, you know they don’t want to, they’ll even decline to sign the consent form to do it because they’re just tired of it. (HV, rural)
This sentiment was also conveyed by other HVs and continued to be expressed in discussing another study requirement of up to 24-month participation that includes six follow-up interviews with the women participating in DOVE by the study coordinator.
. . . initially I would just let them hear the entire consent form, statement or I would let them read the entire statement and I find out that’s really cumbersome and a lot of them kind of lose interest in the middle . . . I can tell that they already lost interest here or they pick on certain phrases, they’re fixed on them. For instance like one lady asked me after listening to that “well it sounds like it’s so long, they talk about eighteen months” . . . I have to explain again because they fixate on that eighteen months and they, you know they kind of feel like they have to commit to this thing so long. (HV, urban)
Another challenge encountered by HVs arose predominantly in rural communities where the use of the tablet posed challenges due to limited or unavailable Internet services, which is required for the tablet to function. Without having paper copies of the tool available as a backup, use of the tablet in such instances would create an obstacle for proceeding with planned screening. Moreover, paper copies were seen as a valued aspect of DOVE because of its discreteness. One HV mentioned that when she took out the tablet during her visit it drew unwanted attention: “ . . . to get that tablet out it’s like ‘oh my gosh she gets to play with a tablet!’” Whereas using paper the HV can just “slip it in” even with other people in the room “having had absolutely no idea what she [the woman] was doing because I [the HV] could entertain them or sway them, or talk about anything else” (HV, rural).
The benefits of DOVE outweighed the identified challenges in terms of outcomes for the women (Sharps et al., 2016) but also in terms of sustainability of DOVE being adopted as a program versus a research study by some of the sites. For example, with DOVE, IPV awareness and information about important community resources and referrals became a more pronounced aspect of HV practice. This HV notes “I’ve learned there are a lot more resources out there for women than I might have even thought of before and you kind of feel good that you can let them know about that.” Such emphasis elevated IPV to a priority health issue for HVs who see IPV as a precursor undermining many of the social determinants of health challenges faced by their families (i.e., poverty, housing, social support, social exclusion and isolation) and a prime opportunity to address current and potential abuse in the lives of already high-risk families. Best said by one HV (rural)—“ . . . it [DOVE] revalidates the need for this to be ongoing and, and everybody’s responsibility. [Meaning]Everybody’s [responsibility], from the doctor, to the family nurse practitioner, to the hospital, to everybody.” Some HVs saw the potential of DOVE’s approach in moving practice forward by providing a framework to screen and intervene across settings for other forms of abuse (childhood) and varied populations (teens). One HV (urban) even suggested evolving DOVE fundamentals to create a teaching tool for men (the fathers they inadvertently encounter during visits) about abusive and healthy relationships. See Table 1 for additional HV responses that correspond to the components of DOVE and suggest how DOVE helped facilitate and enhance their practice.
DOVE Components and Select HV Responses.
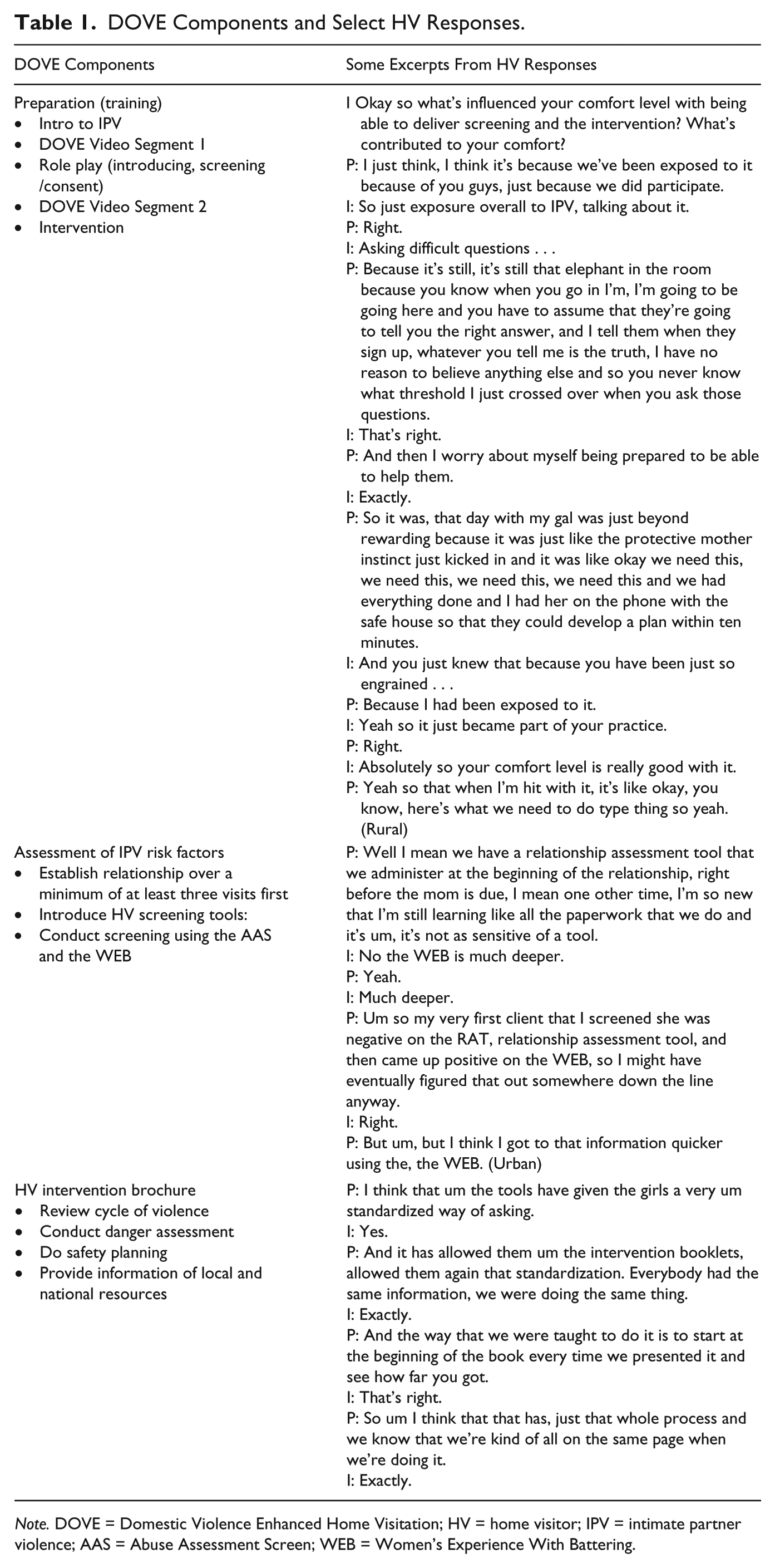
Note. DOVE = Domestic Violence Enhanced Home Visitation; HV = home visitor; IPV = intimate partner violence; AAS = Abuse Assessment Screen; WEB = Women’s Experience With Battering.
Discussion
DOVE did decrease repeat IPV (Sharps et al., 2016). This is incredibly important as few IPV interventions in the health care system that have been rigorously tested exist, and many of those that have do not show significant decreases in violence (Feder, Wathen, & McMillan, 2013; Ramsay et al., 2009). Several HVs found DOVE screening and intervention to be an important part of their routine practice and a welcome addition to their home visits. It was fairly simple to integrate with minimal modification. The results underscored the positive impact that participating in DOVE had on HVs such as increasing their understanding of IPV and its impacts and increasing their confidence in using new skills to intervene with families experiencing IPV. Multiple implications for practice and policy are derived from evaluation findings: (a) Dove screening that used both the AAS (Parker & McFarlane, 1991) and the WEB (Smith et al., 1995) was more effective in identifying IPV than other screening strategies; (b) core components of the DOVE intervention were confirmed by HVs to be pillars to the success of intervening with women who are currently exposed to IPV and for those who could be exposed in the future; (c) DOVE screening and intervention were appealing to HCPs in its sensitivity in being able to identify women exposed to IPV and in its simple, easy to use format; (d) DOVE provides a structured quick intervention in tablet form if desired which can be used if HV encounter a yes that goes beyond just warm referrals; (e) DOVE’s introduction into routine practice can occur with relative seamless integration; (f) DOVE is a critical instrument for helping women to “break up the foundation” of their past; and (g) DOVE’s design allows for flexible use that holds promise for adaptation in other settings (primary care clinics, obstetrical offices) and other populations, particularly teens and others exposed to dating relationships.
Stockl (2014) asserts that a supportive organizational environment demonstrated by “high-level administration endorsements, budget and staff-time” (2014, p. 240) to screen is necessary to effectively screen women for IPV. This study shows that having a support network for providers to turn to either within their organization and/or with IPV expert trainers was imperative to fostering HVs comfort with DOVE and minimize vicarious trauma and emotional burnout. Institutional support for the program, and both the DOVE research coordinator role and manager/peer support were instrumental in providing this kind of support. As a result, HVs had space to debrief, opportunity to problem solve challenging encounters, share information and resources, and stay abreast of current practices and resolve questions or concerns.
Training and support for HVs offered by DOVE research coordinators was a key factor in its success and enabling comfort with screening. This is supported by studies that endorse the provision of health professional IPV training and education primarily given its positive effect on increasing provider comfort (Borowsky & Ireland, 2002; Furniss, McCaffrey, Parnelll, & Rovi, 2007; Mezey, Bacchus, Haworth, & Bewley, 2003). Provider comfort is important for the uptake of policy recommendations such as the PPACA’s screening requirement for IPV.
Communication and building client rapport was identified in a preliminary evaluation of DOVE as an important facilitator of the screening and intervention process (Bacchus et al., 2016a). HVs in this study clearly recognized that interpersonal relationships were critical facilitators to the ongoing delivery of IPV screening and intervention with vulnerable families. Several HVs identified that given the nature of the content discussed as part of DOVE that they did not initiate the DOVE protocol until they had first conducted prior visits with the families and built trust.
HVs in this study noted that often they were the only HCP working with a client who had ever broached the subject of domestic violence. This is especially concerning for low-income, underresourced women with limited access to health care services and multiple vulnerabilities. Furthermore, screening increases the identification of abuse (Thackeray, Stelzner, Downs, & Miller, 2007). Routinely offering ongoing (vs. one-time) IPV screening and intervention, particularly in home visiting programs and other health care settings that offer repeated client contacts, holds the potential to increase access to services and supports for some of the most vulnerable families. Routine screening was also shown to increase provider comfort with the process of screening and intervention.
Technology facilitated the screening process for clients and was generally acceptable by HVs. Earlier evaluation indicates it was also acceptable to younger female clients (Bacchus et al., 2016b). DOVE’s versatility in offering two screening approaches appealed to younger clients who appeared more open and comfortable using the tablets. Paper-and-pencil screening was still a good option for nurses with less technical comfort, and definitely a necessary option for rural communities with limited or no Internet receptivity. It also allowed nurses to circumvent the presence of family members interested in tablet technology (including potential perpetrators).
In addition, DOVE was seen as an invaluable way to educate women about IPV that exemplifies a primary prevention approach versus a reactive one after violence occurs. HVs saw the screening component as opening the door to discussing IPV that provides a springboard for discussions about healthy relationships, the cycle of violence, and locally available community resources that support abused women. Several HVs felt the DOVE intervention served well as an education and awareness teaching tool, even for those not experiencing IPV. Women then become empowered to share this knowledge with friends or family members who might be experiencing IPV or use it themselves in the future.
Conclusion
The need to advocate for practices that couple screening and intervention is apparent. Screening alone does not provide sufficient support for women who may need additional supports, resources, and knowledge to live violence life. Therefore, HCPs must have the proper training and use a robust intervention (both screening and intervention) that extends the minimal screening and brief counseling approach recommended by the U.S. Task Force (Moyer, 2013).
DOVE offers health professionals a standardized way to move beyond screening and brief counseling basics to a more effective method that complements their existing practice. Particularly at the clinical/practice level, such a protocol has been shown to be important in fostering providers practices (Allen et al., 2012; Alvarez, Fedock, Grace, & Campbell, 2016; Borowsky & Ireland, 2002). DOVE’s robust HV training improved HCPs knowledge, skills, and abilities related to IPV screening and intervening. This, in turn, helped HVs overcome the well-known practice challenge presented by the complexity of engaging in conversations about abuse and having to navigate this conversation in the home environment where abusers or other family members are often present.
Our strong encouragement of farther reaching IPV screening and intervention leads us to consider the community resource needs of abused women and a community’s capacity to address these needs. It makes sense to consider, and findings from HV interviews support, the need for attention to social supports at the community level, and to explore logical ways in which services between IPV supports and HCPs can be coordinated to sustain these efforts. Resources for women exposed to IPV also need to encompass behavioral health interventions designed specifically for this population.
DOVE holds promise as a process for IPV screening and intervention that could be adapted across settings and various system access points, not just in prenatal settings and programs but also in postpartum visits and infant parenting programs. Consideration for using DOVE across settings would require some minor modifications to meet the needs of the organization, the setting, and the targeted population. However, adopting DOVE without disrupting its fundamental principles of screening and intervention ensures a standardized approach, which is necessary to maximize the benefits of the program.
The PPACA recommends IPV screening and brief counseling in well woman visits (Moyer, 2013) without identifying a protocol or endorsing an approach for doing so. DOVE could be that brief counseling protocol not yet offered to providers systematically. It is strongly recommended that future federal health care policy maintain a screening mandate with the added component of intervention (beyond brief counseling) as an essential service covered by insurance. Federally funded programs could help establish appropriate reimbursement level for both screening and intervention, which is important for sustainability and uptake of DOVE or similar protocols coupling screening and intervention. Policy and practice directions for IPV screening should incorporate trauma-informed approaches (Burnett & Bacchus, 2016), such as DOVE which is felt to be of particular importance in the case of history of trauma (Chisholm, Bullock & Ferguson, 2017).
DOVE has shown to be a promising IPV prevention, health promotion, and health education strategy for all women, not just those who screen positive for IPV. The utility of DOVE as a broad public health intervention will encourage IPV assessments, promoting and normalizing IPV awareness and enhancing awareness of all providers who screen for IPV.
Footnotes
Acknowledgements
We thank all of the home visiting programs and HVs (home visitors) who participated in this study. Thank you to the National Institutes of Health (NIH) Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the University of Virginia and Johns Hopkins Schools of Nursing for their support of this research. Special thank you to the DOVE (Domestic Violence Enhanced Home Visitation) research team for your expertise and contributions to this study.
Authors’ Note
Donna Schminkey is now affiliated with department of Nursing at James Madison University in Harrisonburg.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institutes of Health (NIH) Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) through a minority supplement to NIH grant number 4 R01 HD071771-05.