
Abstract
Research has identified two subtypes of posttraumatic stress disorder (PTSD); the traditional form that includes hyperarousal reactions, and the other involving ongoing dissociation. Dissociation has been reflected in the new diagnostic criteria for PTSD with the dissociative specification focused on the experience of high levels of depersonalization and/or derealization. PTSD that presents with ongoing dissociation appears to characterize complex cases of PTSD for individuals exposed to protracted trauma. Yet, our understanding of the role of dissociation in relation to PTSD symptoms is limited with inconsistent empirical findings. This study aims to elucidate the complex associations between trauma, dissociation, and trauma-relevant symptomatology. In total, 60 female interpersonal trauma survivors completed baseline measures of trauma and dissociation, and at least a week later, they completed self-report measures of state trauma intrusions, guilt, and anxiety before and after participating in a trauma recall task to examine dissociative tendencies on analogue trauma-related symptoms. After data collection, participants were categorized into two groups; individuals with multiple forms of lifetime interpersonal trauma versus individuals with trauma isolated to single-type trauma in childhood and/or adulthood. Results revealed trauma intrusions, guilt, and anxiety increased after trauma recall overall, though trauma groups differed in the manifestation of these outcomes. In addition, less depersonalization and greater derealization predicted increases in anxiety overall, though this only remained true for those exposed to multiple-type lifespan traumas. Results reveal dissociative tendencies may be most relevant in the processing of trauma-related material for those exposed to multiple types of trauma throughout the lifespan. Implications for treatment of trauma survivors with different clinical presentations are discussed.
Posttraumatic stress disorder (PTSD) can develop after experiencing a traumatic stressor, such as a severe accident, assault, disaster, or combat exposure, though those who experience interpersonal trauma or violent victimization have an increased risk for developing PTSD (Breslau et al., 1998; Brewin, Andrews, & Valentine, 2000; Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995; Resnick, Kilpatrick, Dansky, Saunders, & Best, 1993). PTSD was initially conceptualized as a fear-based syndrome acquired through learning processes in response to threatening stimuli that become overgeneralized and continually trigger an anxiety reaction. However, recent advances in research suggest PTSD is more than an intense state of fear, involving a complex dysfunctional emotion regulation system (Friedman, 2013). The PTSD diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) include a new symptom cluster characterized by altered cognitions and emotions, such as extreme guilt associated with trauma exposure, and a dissociative subtype that includes the additional presentation of depersonalization (i.e., experience of being an outside observer of or detached from oneself) and/or derealization (i.e., experience of unreality, distance, or distortion). Overall, PTSD is a complex phenomenon represented by a broad array of overt and covert behaviors in the form of reexperiencing symptoms, cognitive distortions and negative mood, avoidance, and hyperarousal, and the clinical picture is often complicated by associated features of dissociation, particularly, for survivors of chronic, interpersonal traumas (Herman, 1992).
New Diagnostic Features of PTSD
Research has revealed that many factors influence the course, severity, and nature of posttraumatic sequelae (Ozer, Best, Lipsey, & Weiss, 2003), with posttraumatic responses being the most predictive of symptom maintenance (Friedman, Resick, Bryant, & Brewin, 2011). It was originally proposed that posttraumatic stress symptoms persist if one uses maladaptive strategies to cope with trauma (Foa & Kozak, 1986). That is, the essence of trauma entails physical helplessness in which control is lost, and thus mental control becomes paramount in coping. Dissociation is such a psychological process, typically thought to be defensive, usually arising in response to a traumatic event (Putnam, 1993). Dissociation is described as a heterogenous construct with the central features involving “a significant change in normal consciousness or awareness that arises from reduced or altered access to one’s thoughts, feelings, perceptions, and/or memories” (Briere, Weathers, & Runtz, 2005, p. 221). As such, dissociation is one strategy used to maintain control by distancing oneself from one’s body and thoughts, especially, when active avoidance fails to reduce distress.
In addition, research has demonstrated that strong, negative cognitive–emotional factors such as guilt predict the maintenance of PTSD (Andrews, Brewin, Rose, & Kirk, 2000; DePrince, Zurbriggen, Chu, & Smart, 2010; Grey, Holmes, & Brewin, 2001; Reynolds & Brewin, 1998). Guilt may arise when one attempts to reconcile the event by perseverating on what they could have done differently to prevent the incident(s) in a way that leads them to blame themselves or others and, at the same time, prevents acceptance that the trauma has happened. In addition, guilt may reflect problematic beliefs about how the individual behaved or thought at the time of the trauma in a way that violates his or her personal values and general beliefs about self-worth (Resick & Schnike, 1993). There is overwhelming evidence that such maladaptive appraisals maintain the negative affect found in PTSD and are associated with impairment (Resick & Miller, 2009).
In summary, guilt and dissociative processes appear to maintain PTSD by directly producing negative emotions or motivating a series of coping responses intended to reduce perceived threat and anxiety in the short term. However, coping strategies aimed at avoiding trauma-related stimuli prevent emotional processing and have the paradoxical effect of enhancing reexperiencing symptoms (Wegner, Schneider, Carter, & White, 1987), maintaining anxiety in the long run. Reexperiencing symptoms such as intrusive memories are linked to poor long-term outcome as they may be one mechanism by which the experience of stress/anxiety extends beyond the traumatic stressor (e.g., Michael, Ehlers, Halligan, & Clark, 2005).
Current PTSD Subtypes
It has been proposed, and solidified in the current diagnostic manual, that there are two subtypes of PTSD: one that involves ongoing dissociation and the other more typical and traditional type of PTSD involving hyperarousal reactions (Friedman et al., 2011). The PTSD subtype involving ongoing dissociation may represent more complex cases of PTSD that involve more severe deficits in regulating emotional distress (Briere, 2006). Deficits in emotion regulation are among the most significant clinical sequelae for survivors of prolonged interpersonal trauma, particularly, for those exposed to prolonged trauma early in the life cycle (van der Kolk, Roth, Pelcovitz, Sunday, & Spinazzola, 2005). Indeed, research has found that those who experience trauma characterized as complex (i.e., childhood exposure to multiple traumatic events, often of an interpersonal nature), compared with traumas such as accidents and disasters, report higher levels of dissociation (Briere, 2006; Ginzburg et al., 2006). Thus, individuals who experience protracted, or complex, trauma may be at greater risk for suffering more “complex” forms of PTSD that involve dissociation (Alvarez et al., 2015).
Although dissociation has been conceptualized as an avoidance strategy to reduce the awareness of aversive emotions such as extreme anxiety (Powers, Cross, Fani, & Bradley, 2015), the role of dissociation in relation to posttraumatic reactions is complex. For example, one study reported recent survivors of rape with high peritraumatic dissociation (i.e., dissociation during or shortly after the trauma) showed a decrease in heart rate and skin conductance while talking about their trauma compared with an increase in physiological responding among those with low peritraumatic dissociation (Griffin, Resick, & Mechanic, 1997). In addition, neuroimaging studies suggest there may be distinctive prefrontal cortical responses to trauma memories corresponding to different emotional reactions to distress that distinguish individuals with dissociative and nondissociative PTSD responses (Lanius et al., 2010; Lanius, Bluhm, Lanius, & Pain 2006). In contrast, other studies have found that peritraumatic dissociation is not related to physiological responding in response to trauma cues (Kaufman et al., 2002).
It is important to note research has revealed persistent dissociation is a stronger predictor of PTSD than peritraumatic dissociation (Briere, Scott, Weathers, 2005; Murray, Ehlers, & Mayou, 2002), and different results in the literature may be related to differences in dissociation constructs being measured, as well as differences in trauma histories among participants. In one recent study, only persistent dissociation was related to greater posttraumatic symptoms of anxious arousal (Bennett, Modrowski, Kerig, & Chaplo, 2015). Furthermore, much of the current literature obscures clinically meaningful differences in the variability of dissociative phenomenology by perpetuating the notion of, and empirically investigating, dissociation as a unidimensional state. Much factor-analytic evidence suggests dissociation is a multifaceted collection of distinct but overlapping dimensions (Briere, Weathers, & Runtz, 2005). Notably, few studies have examined associations between posttraumatic symptomatology in lab studies capitalizing on the ability to assess in-the-moment analogue symptoms that can inform posttraumatic phenomenology. This is an especially critical endeavor given the new diagnostic criteria and a dearth of lab research examining new symptom criteria as it relates to traditional symptom criteria. Finally, it is important to examine derealization and depersonalization in this context for their relevance in illuminating differing outcomes for subsets of trauma survivors.
Study Aims
The aim of this study is to examine the effect of persistent dissociative tendencies of both depersonalization and derealization on analogue traumatic stress symptoms of anxious arousal, in combination with other analogue posttraumatic stress symptoms proposed to maintain PTSD (i.e., reexperiencing-intrusions and negative affect-guilt), following a trauma recall task among survivors with varying histories of lifespan interpersonal victimization. It is hypothesized that women with histories of multiple-type lifespan trauma (i.e., exposure to multiple forms of childhood trauma and revictimization in adulthood) will report higher levels of both depersonalization and derealization compared with women with single-type victimization histories isolated to childhood and/or adulthood. It is also hypothesized that controlling for trauma exposure type, trauma intrusions, and guilt will be associated with increases in anxiety after trauma recall, whereas depersonalization and derealization will be associated with decreases in anxiety. Finally, within-group processes will be explored to examine whether dissociation plays a more significant role in predicting increased anxiety for those with multiple-form lifespan trauma exposure compared with those with single-type victimization histories.
Method
Participants
Female interpersonal trauma survivors were recruited through flyers posted in the community (n = 53) and an online bulletin board at a large Midwestern university campus (n = 7). The average age of participants was 31.28 years (SD = 13.05), ranging from 18 to 67 years. Ten were Hispanic or Latino (16.7%). Half were Caucasian/White (50%; n = 30), whereas 31.7% were African American/Black (n = 19), 1.7% were American Indian or Alaskan Native (n = 1), 1.7% were Native Hawaiian/other Pacific Islander (n = 1), 5.0% were Biracial (n = 3), 1.7% reported Unknown (n = 1), and 6.7% declined to answer (n = 4). Most participants in the sample were heterosexual (85%; n = 51) and 40% were single (i.e., never married; n = 24). The majority of participants had some college or vocational school training (53.3%; n = 32), and the greatest proportion of participants reported a household income of US$15,000 or less (35%; n = 21).
Measures
Trauma history
Traumatic experiences and an index interpersonal traumatic event were identified using the Traumatic Life Events Questionnaire (TLEQ; Kubany et al., 2000), a 23-item broad-spectrum measure of trauma exposure. Respondents identify how many times they have experienced a particular event using the following rating scale: never, once, twice, 3 times, 4 times, 5 times, and more than 5 times. In one study utilizing a clinical sample, when compared with the single-item traumatic event assessment in the Structured Clinical Interview for DSM-IV (SCID: First, Spitzer, Gibbon, & Williams, 1998), the TLEQ produced a 9-fold higher rate of traumatic event identification (Peirce, Burke, Stoller, Neufeld, & Brooner, 2009). For the purposes of this study, only interpersonal traumas (i.e., an event in which another human being inflicts physical or psychological injury on another human being) were used to prescreen participants for inclusion criteria. Interpersonal traumas were selected using the same procedure as Frazier and colleagues (2009), with the exception of abortion, which is not conceptualized in this study as an intentionally caused trauma.
Posttraumatic stress
The PTSD Checklist–Civilian Version (PCL-C; Weathers, Litz, Huska, & Keane, 1994) was used to assess PTSD symptoms to examine clinical levels of symptomatology. The PCL-C is a 17-item self-report scale for posttraumatic stress based on Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria. Items are rated from 1 (not at all) to 5 (extremely). A total severity score is obtained by summing the scores from each of the 17 items. A score of 44 is recommended as a cut point for PTSD-positive participants in community samples (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996). The PCL-C demonstrates adequate internal consistency, ranging from .92 to .96 in community samples. Internal consistency in this sample was α = .95.
Dissociation
The Multiscale Dissociation Inventory (MDI; Briere, 2002) is a 30-item self-report measure of dissociative symptomatology that measures six different types of dissociative responses, including disengagement, depersonalization, derealization, emotional constriction, memory disturbance, and identity dissociation. Research with clinical and nonclinical populations indicates that the MDI does tap relatively independent types of dissociative response that correlate in expected directions with the MDI scales (Briere, Weathers, & Runtz, 2005). Items are rated according to its frequency of occurrence over the prior month, using a scale ranging from 1 (never) to 5 (very often). Raw scores on the MDI can be converted to t scores that allow for empirically based clinical interpretation of a respondent’s actual level of dissociative disturbance (i.e., t score at or above 80), though some have suggested that t scores over 66 are indicative of a highly dissociative state (Mitchell, 2006), and others have interpreted t scores of 70 to 89 as elevated dissociative responses that may or may not be clinically meaningful (Galovski & Resick, 2008). The MDI has been found to have good psychometric qualities in both the normative and validated samples; internal consistencies range from .74 (memory disturbance) to .94 (emotional constriction; Briere, 2002). For the purposes of this study, only the derealization (“Feeling like you were in a dream”) and depersonalization (“Your body feeling like it was someone else’s”) subscales were used. Internal consistencies for the derealization and depersonalization subscales were α = .83 and α = .92, respectively.
Trauma intrusions
The Thought Listing Procedure
Three trained research assistants coded TLP intrusion frequencies. First, all thought listings were divided into “thought units” by the two authors, primarily using each clause as an individual thought. All thought units were coded as either trauma intrusions or other thoughts by coders who were blind to study hypotheses. Coders were provided with summaries of each participant’s trauma experience to make accurate codes. Coders generated a frequency score of trauma-related thoughts for each participant using consensus coding, supervised by the first author. Individual variability in the number of thoughts listed across participants was controlled for by calculating the percentage of trauma intrusions relative to all thoughts listed. The percentage score was used as the trauma intrusion frequency variable for this study.
Guilt
The Positive and Negative Affect Schedule–Expanded Form (PANAS-X; Watson & Clark, 1999) assesses 13 affective states. Each item is rated on a 5-point scale from 1 (very slightly or not at all) to 5 (extremely). A total mean score is created by summing all items corresponding to that scale and then dividing by the number of scale items, with higher scores indicating higher degrees of affectivity on that dimension. The PANAS-X scales are sensitive to changing internal and external circumstances and can be used validly to assess short-term state affect and fluctuations in mood (Watson & Clark, 1999). For the purposes of this study, only the 6-item Basic Negative Emotions of Guilt (“Blameworthy”) subscale was utilized. The median internal consistency across 11 samples has consistently shown adequate reliabilities, median α = .88. Internal consistencies for guilt at T1 and T2 were α = .85 and α = .92, respectively.
Anxiety
The Beck Anxiety Inventory (BAI; Beck & Steer, 1993) was used to assess state anxiety. It is a 21-item self-report questionnaire used to measure anxiety severity. Items consist of questions pertaining to how the individual has been feeling in the last week. However, for the purposes of this study, the directions were adapted so that participants were asked to rate their immediate level of anxiety. Items are rated from 0 (Not at all) to 3 (Severely) and totaled to a maximum score of 63. Scores represent minimal (0-7), mild (8-15), moderate (16-25), or severe (26-63) anxiety. The BAI has demonstrated high internal consistency (α = .92). Internal consistencies for Time 1 and Time 2 anxiety were .92 and .94, respectively.
Procedure
Community and student participants were prescreened through telephone and undergraduate classroom mass testing, respectively, to determine eligibility. Women aged 18 years and above who endorsed being the victim of assaultive violence (i.e., sexual and/or physical assault) were enrolled. Only women were included to avoid introducing gender influences on posttraumatic stress symptomatology (e.g., Tolin & Foa, 2006). Participants were excluded from participation if (a) the last incident of the identified trauma occurred before the age of 16 years, to reduce the potential of introducing developmental trauma effects into the study, and (b) the trauma occurred within the last 3 months, as this group of individuals could have been coping with a high degree of acute stress (Rothbaum, Foa, Riggs, Murdock, & Walsh, 1992). PTSD diagnosis was not an inclusion criterion to get a representative sample of interpersonal trauma survivors experiencing varying levels of posttraumatic stress as subthreshold PTSD can be as impairing as full PTSD (Zlotnick, Franklin, & Zimmerman, 2002).
Participants who met inclusion criteria at the prescreening were asked to complete self-report questionnaires online to obtain information on demographics, trauma history, and dissociation (both depersonalization and derealization) at baseline. Participants provided consent online, and participants who did not have access to a computer or the Internet completed the online questionnaire in the research lab. The questionnaire took approximately 30 min to complete. Community participants were paid US$10 for their time, and student participants were given course credit. Both student and community participants were contacted via phone or email to schedule a lab session at least a week after they had completed the online questionnaire.
The mean number of days between the online questionnaire and lab session was 15.14, ranging from 7 to 61. The lab session took approximately one and a half hours to complete. Community participants received an additional US$30, and student participants received additional course credit. The lab session began by having participants complete the BAI, PANAS-X, and TLP to obtain preinterview (T1) state anxiety, state guilt, and trauma intrusions, respectively.
Next, the first author administered a trauma processing task (adapted version of the Catastrophizing Interview [CI]; Davey & Levy, 1998; Vasey & Borkovec, 1992) on the index interpersonal trauma. The CI assesses perseverative thinking about a worrisome topic, in this case the index trauma (i.e., interpersonal trauma identified by the participant as the worst experienced), in an iterative fashion by asking interviewees to elaborate their concerns repeatedly until they adequately address their concern. Participants are reminded every seven steps they can stop the interview once they explored all concerns. The interview served to remind participants of their traumatic experience and its consequences in a detailed fashion, thus setting the occasion for trauma-related symptomatology. The CI was conducted by a master’s level clinical psychology student trained in trauma-informed clinical interviewing and research ethics. Participants who appeared visibly distressed during the CI were assessed by the interviewer, and procedures were in place to consult with a licensed clinical psychologist if potential risk issues were disclosed. Seven participants became tearful during the CI, and all participants expressed a desire to move forward with the study. No participants disclosed risk issues.
After the CI, participants completed the BAI, PANAS-X, and TLP to obtain a postinterview (T2) assessment. The study concluded by having participants read an uplifting short story to remove potential negative residual effects from revisiting trauma memories. The true story was about a 76-year-old grandmother who received her college degree after delaying her education for 42 years to raise a family. Participants were instructed to enter the positive mood state before reading a story, as demand characteristics intensify mood induction (Westermann, Spies, Stahl, & Hesse, 1996). Instructions were as follows: “This story is intended to promote a positive mood in the reader. Please read the story while feeling positive.” Following study completion, participants were thanked for their participation and given a debriefing form. The debriefing form included a brief rationale for the study, the researchers’ contact information to report questions and concerns, and a list of community mental health agencies to address any mental health concerns. No adverse events were reported as a result of this study.
Trauma group coding
At the conclusion of the study, the first author coded participants into one of two victimization groups based on endorsement of particular items on the TLEQ. All participants had adulthood victimization, as this was one criterion for study inclusion. The single-type trauma group category was based off the extent of childhood victimization experienced, such that those with just one type of childhood victimization (sexual assault, physical assault, or witnessing family violence) or no childhood victimization were placed into this group. The multiple-type lifespan trauma group consisted of participants who experienced multiple forms of childhood victimization in addition to adulthood victimization.
Data Analyses
IBM SPSS Version 24 was used for statistical analyses. Descriptive statistics examined trauma history, posttraumatic stress severity and PTSD diagnosis, and clinical levels of depersonalization and derealization. Before hypothesis testing, independent samples t tests were assessed for potential differences in trauma intrusions, guilt, and anxiety between T1 and T2. Given the bimodal outcome of trauma intrusions, it was dichotomized to represent no increase (n = 36; 60%) versus an increase (n = 24; 40%) in trauma intrusions. Change scores were calculated for both guilt (i.e., T2 guilt minus T1 guilt) and anxiety (i.e., T2 anxiety minus T1 anxiety).
Independent samples t test were also used to assess for potential differences in anxiety and guilt between the trauma groups at both T1 and T2. Furthermore, paired-samples t tests were used to assess for potential differences between T1 and T2 anxiety and guilt among each trauma group. A chi-square analysis assessed for potential differences in trauma intrusions from T1 to T2 between the trauma groups.
To test Hypothesis 1, two independent samples t tests were used to examine differences between women with histories of multiple-type lifespan trauma and single-type trauma in (a) baseline clinical levels of depersonalization and (b) baseline clinical levels of derealization. To test Hypothesis 2, a hierarchical linear regression analysis was used to examine the unique contributions of depersonalization and derealization in predicting increased anxiety after trauma recall, over and above trauma intrusions and guilt, controlling for trauma exposure group. Group status was entered on Step 1; increased trauma intrusions and guilt were entered on Step 2; baseline derealization and depersonalization were entered on Step 3. To test Hypothesis 3, two hierarchical linear regression analyses were used to examine the unique contributions of depersonalization and derealization in predicting increased anxiety after trauma recall, over and above trauma intrusions and guilt within (a) those with single-type victimization histories and (b) those with multiple-form lifespan trauma exposure.
Results
Descriptive Statistics: Trauma and Posttraumatic Sequelae
Participants reported experiencing numerous interpersonal traumas. The modal trauma reported was intimate partner violence by 86.67% of the sample (n = 52). Most participants fell into the single-type trauma group (n = 32; 53.3%), and 46.7% (n = 28) fell into the multiple-type lifespan trauma group.
Intimate partner violence was the modal index trauma identified on the CI (46.67%; n = 28). Adult sexual assault was the second most frequently reported index trauma (20%; n = 12), followed by adolescent (after age of 15 years) sexual assault (13.33%; n = 8), adolescent (after age of 15 years) physical abuse by caregivers (10%; n = 6), and being robbed with a weapon (6.67%; n = 4). Two participants reported other types of traumas that fell into a different category: one reported being kidnapped with a weapon (1.67%; n = 1); the other reported being the victim of attempted murder (1.67%; n = 1). The last time the index event occurred averaged approximately 9.47 (SD = 9.85) years prior to the interview, ranging from 3 months to 38 years prior. Many participants (n = 16; 26.67%) reported the index trauma occurred within the last year, and the majority (n = 32; 53.33%) reported the index trauma occurred within the last 5 years.
Posttraumatic stress symptom severity on the PCL had a mean score of 37.90 (SD = 16.24), ranging from 17 to 85. Using a cutoff score of 44 (Blanchard et al., 1996), 29.8% of participants would be classified as PTSD positive, which is in the range of the conditional risk of PTSD given exposure to assaultive violence (i.e., 26%; Resnick et al., 1993). An equal proportion of participants who fell in the multiple-type lifespan trauma (n = 12) and single-type trauma (n = 10) groups met criteria for PTSD, χ2(1) = 0.91, p = .340.
The average level of dissociation was just under the clinical threshold for both depersonalization (t score: M = 73.65, SD = 32.69) and derealization (t score: M = 71.29, SD = 23.28), though in the range of elevated dissociative responses. Using a t score cutoff of 80 to represent clinical levels of dissociative disturbance (Briere, 2002), 35% and 32.3% of this sample would be classified as having clinical levels of depersonalization and derealization, respectively. Average raw scores on both depersonalization (M = 8.22, SD = 4.26) and derealization (M = 9.54, SD = 4.21) subscales were higher than those reported in both a normative sample and in an incarcerated population with high levels of childhood and adulthood interpersonal violence exposure (Dietrich, 2003), though similar to those reported in a pretreatment sample of 150 female interpersonal trauma survivors enrolled in a randomized controlled trial for trauma-focused therapy (Resick, Suvak, Johnides, Mitchell, & Iverson, 2012).
Dissociation and analogue Traumatic Stress Symptomatology
From T1 to T2, anxiety, t(59) = 3.35, p = .001; guilt, t(59) = 2.74, p = .008; and trauma intrusions, t(59) = 3.45, p = .001, significantly increased for the full sample (see Table 1). Anxiety increased from “minimal” (M = 5.37) to “mild” (M = 8.52). Forty percent of participants reported increased trauma intrusions, ranging from .72% (n = 1) of their TLP to 58.82% (n = 1) of their TLP being represented by trauma intrusions.
Mean Scores on Baseline Dissociation and Analogue Posttraumatic Stress Variables at Time 1 and Time 2, and Change in Mean Scores Between Study Assessments (N = 60).
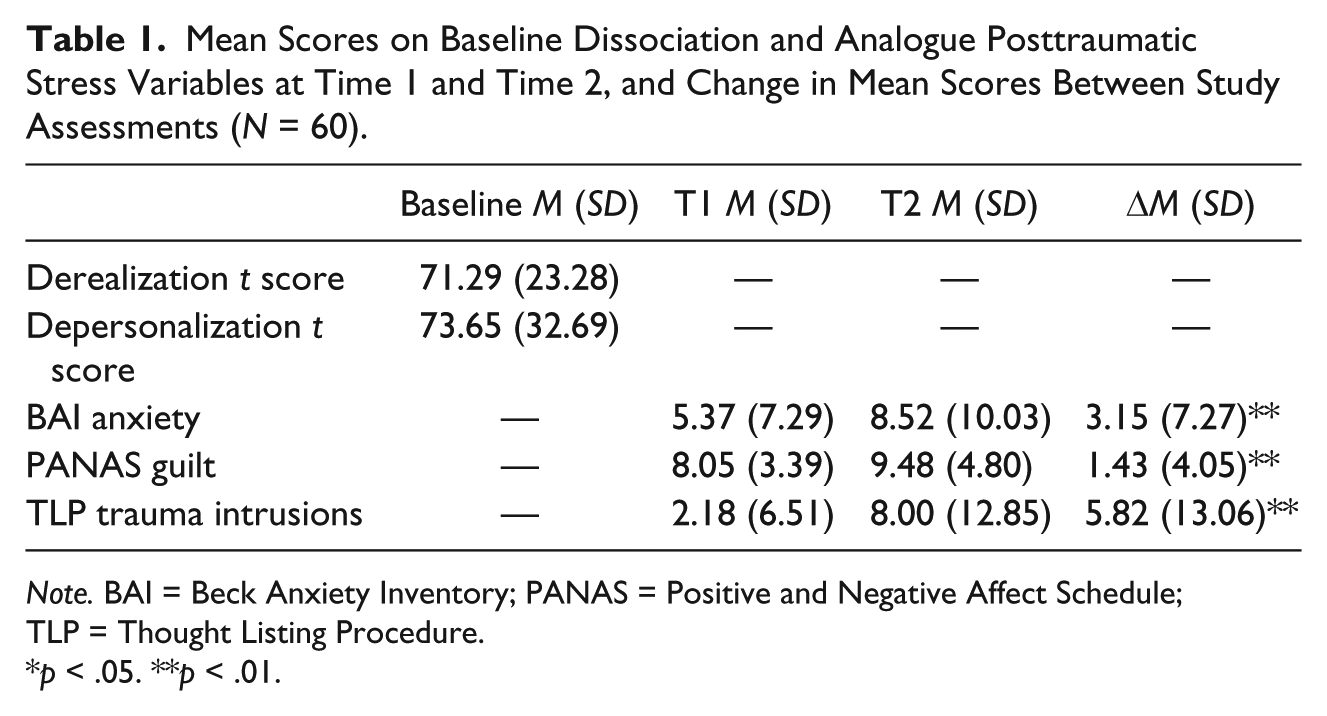
Note. BAI = Beck Anxiety Inventory; PANAS = Positive and Negative Affect Schedule; TLP = Thought Listing Procedure.
p < .05. **p < .01.
There were no significant differences in anxiety, guilt, or trauma intrusions at T1 or T2 between the trauma groups (ps > .05). Notably, within groups, the multiple-type lifespan trauma group reported increased guilt, t(27) = 3.30, p = .003, and marginally significant increased anxiety, t(27) = 2.01, p = .055, from T1 to T2. Alternatively, the single-type trauma group reported neither an increase in anxiety, t(31) = 1.38, p = .177, nor guilt, t(31) = 1.89, p = .068. There was no difference in trauma intrusions produced after trauma recall between the trauma groups, χ2(1) = 1.35, p = .245.
Partially consistent with Hypothesis 1, there was a significant difference in baseline clinical depersonalization, t(58) = 2.17, p = .034, between the multiple-type lifespan trauma (M = 83.14, SD = 65.43) and single-type trauma (M = 65.34, SD = 26.14) groups, but no difference in baseline clinical derealization, t(58) = 0.74, p = .462.
Correlation analyses for the relations between dissociation (depersonalization and derealization) with changes in posttraumatic stress symptoatology (anxiety, guilt, and trauma intrusions) can be found in Table 2. A hierarchical linear regression analysis predicting increased anxiety (i.e., T2 minus T1) was conducted to test Hypothesis 2. The overall model was significant, F(5, 58) = 4.32, p = .002, and accounted for 22.3% of the variance in increased anxiety (see Table 3). Increases in trauma intrusions and guilt added significant variance above group status (∆R2 =.12, p = .028), and dissociation added significant variance at Step 2 (∆R2 =.11, p = .020). Increased guilt (β = .35, p = .007), less depersonalization (β = −.47, p = .016), and greater derealization (β = .53, p = .006) predicted increased anxiety. In the final step, trauma group continued to exert a significant influence on anxiety; the multiple-type trauma group reported greater increased anxiety.
Correlation Matrix of Dissociation and Changes in Posttraumatic Stress Symptomatology (N = 60).

Note. BAI = Beck Anxiety Inventory; PANAS = Positive and Negative Affect Schedule; TLP = Thought Listing Procedure.
p < .05. **p < .01. ***p < .001.
Hierarchical Linear Regression Analysis Predicting Changes in Anxiety (N = 60).
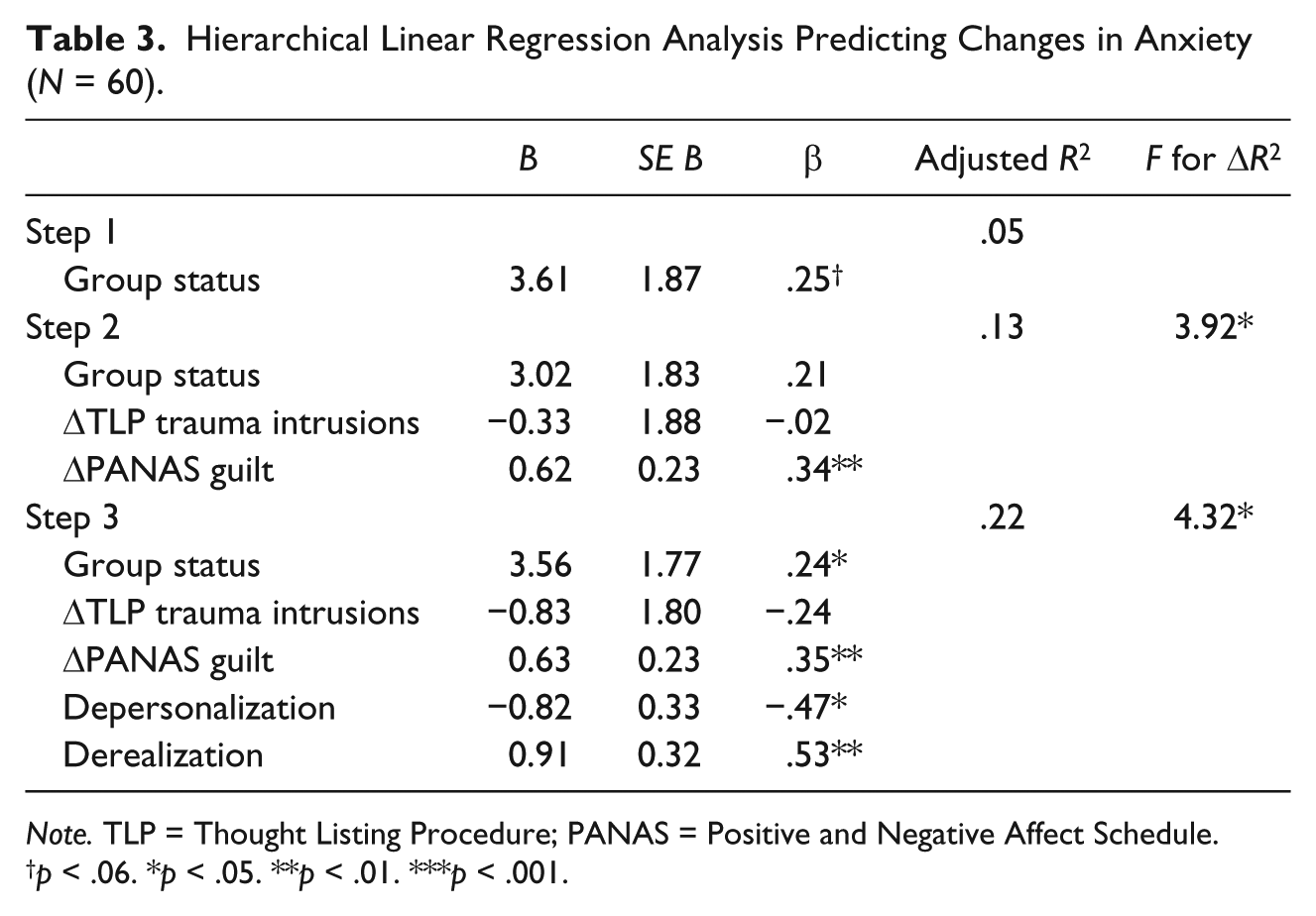
Note. TLP = Thought Listing Procedure; PANAS = Positive and Negative Affect Schedule.
p < .06. *p < .05. **p < .01. ***p < .001.
To examine within-group processes, separate hierarchical linear regression analyses were performed for each group (Table 4). Only increased guilt (β = .54, p = .004) was uniquely associated with increased anxiety for the single-type trauma group. Like the full sample, for the multiple-type lifespan trauma group, greater derealization predicted increased anxiety (β = .64, p = .035), whereas greater depersonalization predicted decreased anxiety (β = −.60, p = .044).
Hierarchical Linear Regression Analysis Predicting Changes in Anxiety Between Single-Type Trauma and Multiple-Type Lifespan Trauma Group (N = 60).

Note. TLP = Thought Listing Procedure; PANAS = Positive and Negative Affect Schedule.
p < .05. **p < .01. ***p < .001.
Discussion
The aim of the present study was to examine the complex associations between interpersonal trauma victimization, dissociative tendencies, and trauma-relevant symptomatology, following a trauma recall task. In a sample that was selected based on exposure to interpersonal trauma in adulthood, we found a sizable minority of the sample (43%) reported exposure to not just one form of childhood trauma but multiple forms of childhood trauma. Although disconcerting, these numbers were not unexpected and adds yet another observation of how early exposure to trauma, particularly, multiple forms of trauma exposure in childhood, enhances risk for revictimization in late adolescence and adulthood (Friedman et al., 2011). Continued empirical investigation of individuals with this pattern of victimization may support the contention that this subset of the trauma-exposed population largely accounts for the faction of PTSD-affected individuals with dissociative tendencies as originally proposed by Herman (1992), and more recently observed by Alvarez et al. (2015). This study further attempted to replicate the impact of victimization history on dissociation, as well as examine the impact of guilt, trauma intrusions, and dissociation on analogue trauma symptoms (i.e., changes in anxiety following a trauma recall task) among a sample of individuals with complex trauma histories.
As predicted, among participants with exposure to interpersonal trauma in adulthood, participants who also reported a history of exposure to multiple forms of trauma in childhood reported greater baseline depersonalization than participants without exposure to childhood trauma, or childhood exposure that was isolated to one form of trauma. Contrary to expectations, group differences were not observed in regard to derealization. As two forms of dissociative tendencies, both of which have been connected to childhood exposure to trauma (Briere, 2006; Ginzburg et al., 2006), it is unclear why only depersonalization was greater among those with more complex histories. One possible explanation for these findings is the inclusionary criteria for this study was exposure to interpersonal trauma in adulthood, and thus, every participant had at least one personal event in which their physical body was targeted for harm by a perpetrator. The corporeal nature of interpersonal victimization may have a greater impact on depersonalization processes in which the focus is on removal from one’s bodily experiences, particularly, among those exposed to multiple forms of interpersonal victimization across the lifespan, committed by multiple perpetrators.
Following the trauma recall task, self-reported anxiety, guilt, and trauma-related intrusions increased in the full sample. These results provide continued support for use of the CI as an effective lab-based, trauma recall task. Notably, these increases seem largely driven by changes observed within the multiple-type lifespan trauma group, as increased guilt and anxiety were shown for this group when within-group changes were examined, and no significant changes in anxiety or guilt were observed for the single-type trauma group. These results are not accounted for by greater prevalence of PTSD symptomatology or diagnostic status, as PTSD severity did not differ as a function of trauma group membership. Instead, the results suggest that something unique to recurrent childhood trauma exposure enhances risk for analogue symptoms, at least in the present study. Additional research to replicate this finding is needed.
The present study also sought to examine the simultaneous positive influence of guilt and intrusions, and negative influence of dissociation, on analogue stress symptoms following a trauma recall task, after controlling for trauma exposure group. As anticipated, guilt had a positive association with changes in anxiety, whereas depersonalization had a negative association with changes in anxiety. That is, greater guilt was associated with increased anxiety, whereas greater depersonalization was associated with decreased anxiety. These associations align with previous research demonstrating the deleterious effects of guilt (Andrews et al., 2000; DePrince et al., 2010; Grey et al., 2001; Reynolds & Brewin, 1998) and shed light on a potential protective effect of depersonalization on posttraumatic stress symptoms, the latter of which are likely short term in impact. Contrary to expectations, derealization had a significant positive impact such that greater baseline derealization was associated with greater increases in anxiety. These results are surprising, as the broad category of dissociation is typically considered to be an immediate buffer against negative affectivity among trauma-exposed individuals; yet, the more narrow aspect of derealization actually enhanced anxiety once the impacts of trauma history, intrusions, guilt, and depersonalization were partialed out. These novel results afforded by simultaneously considering multiple dimensions of dissociation indicate that feeling removed from one’s body may feel protective among interpersonal trauma survivors when reminded of the event, but feeling as though one’s environment is not real actually enhances anxiety. Among this sample of interpersonal trauma survivors, a tendency toward feeling removed from reality, questioning the veracity of one’s surroundings, may have a disorienting quality that enhances anxiety when one may need to feel the most grounded. This is among the first studies to reveal an opposing influence of domains of dissociation on traumatic stress symptoms.
Within-group regression models revealed dissociation results from the full sample were, once again, likely driven by associations observed within the multiple-type lifespan group. That is, when the model was conducted with only the multiple-type lifespan group, the negative association between depersonalization and anxiety, and the positive association between derealization and anxiety, remained significant. Although the direction of these relations were the same for the single-type trauma group, the impact of the dissociation variables was no longer significant. When within-group models were run, guilt was no longer a significant predictor of increased anxiety for the multiple-type lifespan trauma group. It is possible the strong impact of dissociation for this group trumped the effects of guilt, as this group’s symptomatology may be more driven by dissociative processes learned as coping mechanisms throughout childhood. Overall, results suggest the dissociative subtype of PTSD reflected in the DSM-5 may be most relevant for those with multiple types of lifetime trauma and may be a new approach to conceptualizing complex PTSD (Friedman, 2013).
These findings expand the research literature by demonstrating how complex trauma and dissociative tendencies are involved in the processing of trauma-related material. The tendency of trauma clients to dissociate needs to be considered when treating trauma-related distress. For example, Foa and Hearst-Ikeda (1996) concluded that therapeutic techniques directly aimed at reducing dissociation are necessary in the treatment of posttraumatic stress among clients who dissociate during exposure therapy. The findings in this study suggest that this may be particularly relevant for individuals with a history of multiple forms of childhood trauma with subsequent revictimization in adulthood. For these individuals, exposure to trauma reminders led to a greater increase in anxiety. The results may lend incremental support to the 4-D model of trauma-related dissociation (Frewen & Lanius, 2014), in that significant trauma in childhood may be associated with trauma-related altered states of consciousness. Perhaps, the most surprising of the results was the opposing impacts of depersonalization and derealization, as depersonalization reduced anxiety and derealization increased anxiety. As the purpose of exposure therapies is to raise anxiety, so that clients have an opportunity to habituate to heightened arousal, depersonalization may thwart therapeutic progress among individuals whose anxiety is buffered by dissociative processes. Alternatively, derealization may be less problematic in the exposure therapy room as it does not seem to buffer against increases in anxiety. Results show that we may be at a nascent level of understanding when it comes to the potentially differential impacts of varying dissociative content or processes.
The current study must be considered in light of its limitations. The sample size was small and comprised of both community and college student participants, with a wide range in age, which can affect the ability to detect important between and within group effects on study variables. This variability in demographics allowed for the inclusion of participants with varying trauma histories, though some demographics (e.g., college student, older age) may have been associated with less distress. Furthermore, the impact of gender on reactions to childhood victimization experiences is an area in significant need of exploration, and which we were unable to examine here given that the sample was comprised only of female survivors. Replication with a larger sample comprised of both men and women will be particularly informative. The current sample was characterized by a high degree of trauma exposure occurring anywhere between 3 months and 38 years prior to the study, with most participants indicating multiple forms of exposure, as well as exposure across both childhood and adulthood. This may have led to a number of ceiling effects that could be rectified with a sample of participants with greater diversity in overall trauma load and a more restricted time range of trauma exposure. Furthermore, trauma was categorized as a function of exposure to different types of trauma, and repeated exposure within types of trauma was not captured in the categorization of the trauma groups. It is possible that individuals in this study who experienced recurrent sexual abuse as a child from a caregiver (a trauma history that many would consider “complex”) were classified in the same group as individuals with an isolated experience of assault as an adult. This limitation is a persistent problem within the traumatology field; namely, the difficulty with quantifying and categorizing trauma histories that are often complicated and repetitive. Relatedly, there was a gap in time between the assessment of trauma and lab session; participants could have been revictimized within this time frame, redefining which trauma group they belong to. Furthermore, the complicated impact of depersonalization needs further investigation. Although it seemed to show a buffering effect in regard to anxiety in this study, the long-term payoff of that strategy was not captured in the present study. Collection of follow-up data in the days and/or weeks after the trauma recall task would have assisted in determining whether the impact of depersonalization on more immediate affect had long-term adverse consequences in the area of intrusions, guilt, negative affectivity, or personal/interpersonal functioning. Finally, the sample was mixed in regard to diagnostic status for both PTSD and dissociation. Samples comprised of PTSD positive participants, and/or samples with an overall greater level of dissociation, may provide differing results. Despite its limitations, the current study revealed important information regarding the potentially opposing impact of depersonalization and derealization on analogue trauma symptoms. Replication and extension is strongly needed to elucidate the often discussed, yet narrowly understood, impact of dissociation on posttrauma functioning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by the Center for the Study of Family Violence and Sexual Assault at Northern Illinois University as part of a dissertation grant awarded to the first author.