
Abstract
Sexual harassment (SH) and sexual assault (SA) continue to be a focus of prevention efforts in the U.S. military because of the prevalence and potential to affect the health and readiness of service members. Limited research exists on the association of SH and SA with coping behaviors, such as physical activity, within the military. Data including self-reported SA, SH, and physical activity were obtained from the Millennium Cohort Study, a longitudinal cohort study designed to examine the impact of military service on the health and well-being of service members. A hierarchical regression approach was applied to examine the association between SH or SA and subsequent physical activity levels. Hierarchical regression showed that, among those self-reporting recent SA, the odds of medium-high (300-449 min/week) and high physical activity levels (≥450 min/week) were significantly increased. Although the magnitude of these associations was attenuated with an increasing amount of adjustment, the odds of high physical activity levels remained statistically significant in the fully adjusted model (medium-high: odds ratio [OR] = 1.72, 95% confidence interval [CI] = [1.08, 2.73]; high: OR = 1.58, 95% CI = [1.02, 2.44]). We observed statistically significant negative associations between recent SH and medium-high physical activity levels in adjusted models (OR = 0.70, 95% CI = [0.54, 0.91]). The current results demonstrate that SA is generally associated with increased levels of physical activity among military service members. Analyzing the relationship between sexual trauma and physical activity is valuable because of the high prevalence of SH and SA in the military, long-term health implications including physical and emotional well-being, and potential impact on military readiness.
Sexual trauma, including sexual harassment (SH) and sexual assault (SA), remains a compelling concern among U.S. service members, military commanders, and Department of Defense (DoD) leadership (DoD, 2016; Gedney, Wood, Lundahl, & Butters, 2018; Godfrey et al., 2015; Holland, Rabelo, & Cortina, 2014). SH is defined as unsolicited sexual advances, requests for sexual favors, and other verbal or physical conduct of a sexual nature, whereas SA involves intentional sexual contact associated with the use of force, intimidation, or abuse of authority in the absence of consent (U.S. Department of the Army, 2014). According to the DoD, reports of SA in the military increased from 2,688 in 2007 to 6,083 in 2015 (DoD, 2011, 2016). Despite the large number of reported events, evidence suggests that the actual prevalence of SH and SA is much greater because these events are vastly underreported (Campbell & Raja, 2005). In 2016, the DoD estimated that 4.3% of servicewomen and 0.6% of servicemen had experienced SA in the previous 12 months (Office of People Analytics, 2017). According to the DoD’s 2015 annual report on SA, approximately 23% of service members who experienced an SA in 2014 reported the crime to leadership (DoD, 2016). This report also noted disparities in reporting by sex. Men appeared less willing to report being sexually assaulted than women; 38% of female victims reported their assault, whereas only about 10% of male victims reported the incident (DoD, 2016).
The military possesses several unique characteristics that likely affect the prevalence, reporting, and methods of coping in response to SH and SA. Although the majority of service members are male, the number of women in the services is rising, and their roles in combat are expanding (Carter, 2015). Nevertheless, the military continues to be a male dominant culture, which increases the risk of victimization and makes it difficult for both women and men to report SH and SA. There are options for service members to report SH and SA with or without confidentiality (U.S. Department of the Army, 2014). Despite significant military campaign efforts to perpetuate a cultural change, open disclosure of SH and SA continues to be associated with professional reprisal, ostracism, and maltreatment (Office of People Analytics, 2017). In addition, military SH and SA is frequently interpersonal with a victim knowing the perpetrator before the event and continuing to live and/or work in close proximity with that individual (Office of People Analytics, 2017). Military deployments during which units may be isolated is associated with an increased risk of SH and SA (LeardMann et al., 2013; Sadler, Booth, Torner, & Mengeling, 2017). Therefore, survivors of SH or SA who choose to continue to serve in the military must develop coping strategies to protect against ongoing feelings of vulnerability or fear of revictimization.
The potential impact of SH or SA in the military is immense because of both the levels of occurrence and potential physical and mental health outcomes affecting morale and readiness. Previous studies indicate that service members reporting SH or SA are more likely to report poorer mental and physical health (Godfrey et al., 2015; Kimerling, Gima, Smith, Street, & Frayne, 2007; Millegan, Wang, LeardMann, Miletich, & Street, 2016) and less likely to engage in preventive care (Lang et al., 2003; Resnick, Acierno, & Kilpatrick, 1997). In addition to poor health outcomes, Millegan et al. (2015) found that service members reporting recent SH or SA were more likely to report difficulties in work-related activities.
When an individual is injured physically and mentally as a result of SH or SA, the military unit often becomes dysfunctional, because it is losing a contributing member of the team. Unit cohesion and morale may also be negatively affected because the culture of trust has been violated. If service members cannot trust coworkers to protect against SH or SA, they may also be unable to trust that he or she will be protected from the enemy in the context of war. The military unit may no longer be able to accomplish its mission.
There is growing literature describing the mechanism by which SH and SA contribute to negative mental and physical health outcomes, one of which is through coping behaviors. Sexual trauma can impair one’s emotional regulation and ability to self-soothe (D’Andrea, Sharma, Zelechoski, & Spinazzola, 2011; Ullman, Peter-Hagene, & Relyea, 2014; van der Kolk, 1994). As a result, individuals use a variety of coping strategies to minimize negative symptoms and/or increase positive emotions. Some strategies can be considered maladaptive if they alleviate distress but result in behaviors that increase the risk of other negative outcomes. For example, literature exists on the relationship between SH and SA and unhealthy coping behaviors, including increased alcohol consumption, tobacco use, and illicit drug abuse (Bedard-Gilligan et al., 2013; Lawler, Ouimette, & Dahlstedt, 2005; Littleton, Horsley, John, & Nelson, 2007; Ullman, Relyea, Peter-Hagene, & Vasquez, 2013). Other studies have also associated sexual violence toward women with eating disorders and sudden changes in weight (Faravelli, Giugni, Salvatori, & Ricca, 2004; Laws & Golding, 1996).
Understanding coping behaviors following SH and SA is essential to provide effective support to survivors. Physical activity is a coping behavior that is also an important part of military life. Career progression and reputation is dependent upon physical strength and stamina. It is considered to be a marker of combat readiness and the ability to endure the physical and psychological hardships of war. Poor physical performance is an early indicator to the individual, commanders, and the team that something is amiss. Examining level of physical activity as a coping mechanism for SH and SA is important because such activity can affect service members’ deployability and occupational success. Appropriate levels of physical activity can improve service members’ physical fitness and be very beneficial. Reduced physical activity could detrimentally affect service members’ physical fitness. Alternatively, excessive physical activity could also detrimentally affect fitness through fatigue, inadequate nutrition, or overuse injuries.
Physical activity is one of the recommended coping strategies for posttraumatic stress disorder (PTSD) patients and sexual trauma survivors because exercise helps individuals reduce stress, enhances a sense of control, and upregulates endorphins that contribute to positive mood (Anderson & Shivakumar, 2013; U.S. Department of Veterans Affairs, 2015). Studies have also found that exercise can effectively reduce mental health problems and suicide risk (Davidson, Babson, Bonn-Miller, Souter, & Vannoy, 2013; Manger & Motta, 2005). Engagement in physical activity, especially vigorous activity, has been associated with decreased odds of PTSD symptoms among U.S. service members (LeardMann et al., 2011). In addition, Medina et al. (2011) found that vigorous exercise was associated with reduced alcohol-related coping behaviors among trauma survivors.
Despite the beneficial health effects of exercise, many studies have observed decreased physical activity among individuals with PTSD compared with those without PTSD (Chwastiak, Rosenheck, & Kazis, 2011; Godfrey, Lindamer, Mostoufi, & Afari, 2013; Kozaric-Kovacic et al., 2009; Kukihara, Yamawaki, Uchiyama, Arai, & Horikawa, 2014; Zen, Whooley, Zhao, & Cohen, 2012). Lang et al. (2003) observed a similar declining pattern of physical activity among veterans with a history of sexual trauma. As most of these studies focused primarily on veteran populations, it is unclear if a similar pattern would be observed in current service members, particularly given the emphasis placed on physical fitness for military readiness. In this study, we examined physical activity levels in military service members after self-reported SH or SA, using a large prospective cohort study. By quantifying physical activity reported by SH or SA survivors and comparison groups, this study provides insight into how physical activity could be used as an indicator for appropriate or inappropriate coping behavior.
Method
Study Population
The Millennium Cohort Study, launched in 2001, is a longitudinal cohort study designed to examine any health impact of military service among U.S. service members. Details of the Millennium Cohort Study have previously been published (Gray et al., 2002; Ryan et al., 2007). The cohort includes four enrollment panels. Panel 1 was a population-based random sample of the U.S. military in October 2000, and Panels 2 to 4 focused on new accessions with 1 to 5 years of military service. After informed consent and completion of a baseline survey, participants received follow-up questionnaires approximately at 3-year intervals. This research was conducted in accordance with all applicable federal and institutional regulations governing protection of human subjects after approval by the institutional review boards at Naval Health Research Center and Uniformed Services University of the Health Sciences.
Physical activity related questions were first asked during the 2007-2008 survey cycle. For the purposes of these analyses, the 2007-2008 survey responses were referred to as “baseline,” while the 2011-2013 responses were referred to as “follow-up.” We restricted our study population to 34,645 Millennium Cohort Study participants from enrollment Panels 1 to 3. Eligible participants had to be on active duty or in the National Guard or Reserve (Guard/Reserve) components at survey completion during both the baseline and follow-up survey cycles and not report a childbirth or miscarriage in the 3 years prior to each survey, because pregnant active duty women do not have the same fitness standards as nonpregnant women. There are approximately 40 provider-based diagnoses or conditions listed in baseline or follow-up surveys covering multiple organ systems. As it would be highly unlikely for an individual to be told that he or she has all listed conditions, we excluded those individuals who endorsed all conditions (n = 22) from all analyses. We also excluded survey respondents with incomplete covariate data.
Outcome Variable
Self-reported physical activity levels were examined using participants’ estimated average number of minutes per day and days per week spent in moderate/light- or vigorous-intensity physical activity. Moderate/light-intensity activity was defined in the questionnaire as “exercise or work that causes light sweating or slight increases in breathing or heart rate.” Vigorous activity was defined as “exercise or work that causes heavy sweating or large increases in breathing or heart rate.” The total minutes of physical activity per week was calculated by combining moderate/light- and vigorous-intensity physical activity, where every minute of vigorous-intensity activity counted as 2 min of moderate/light-intensity activity, as defined in the 2008 Physical Activity Guidelines for Americans (U.S. Department of Health and Human Services [HHS], 2008). We then classified participants into one of the four categories based on minutes per week of physical activity: (a) low (<150 min/week), (b) medium (150 to <300 min/week), (c) medium-high (300 to <450 min/week), and (d) high (450+ min/week). The 150-min increment was selected as the threshold for low-level physical activity based on the 2008 Physical Activity Guidelines for Americans recommendation for exercising 150 min per week to maintain health and 300 min per week for additional health benefits (HHS, 2008). The medium level of physical activity (150 to <300 min/week) was selected as the reference group for all multinomial regression models.
Primary Exposure Variable
Self-reported SH or SA within the past 3 years was assessed at follow-up, which, by definition, would precede participants’ report of current physical activity. SH and SA were also asked during 2007-2008 survey cycle (baseline). However, as the main focus of our study was to examine any associations between recent SH/SA and physical activity, baseline SH/SA was not included in the statistical models. Participants were asked if, in the past 3 years, they “experienced sexual harassment” or “suffered forced sexual relations or sexual assault.” To align with previous research and due to statistical analysis requirements (cell size), sexual trauma was collapsed into three groups. Participants were categorized into one of the three groups: (a) no SH or SA, (b) SH only—endorsing SH but not endorsing SA, or (c) SA—endorsing SA with or without endorsing SH.
Demographic and military characteristics
The Defense Manpower Data Center (DMDC) provided the following demographic and military information: sex, birth year (pre-1960, 1960-1969, 1970-1979, and 1980 and later), race/ethnicity (non-Hispanic White, non-Hispanic Black, or other), military component (active duty or Guard/Reserve), separation after baseline survey (yes/no), military pay grade (junior enlisted, noncommissioned officer, or officer), and service branch (Army, Navy/Coast Guard, Air Force, or Marine Corps). Education (less than a bachelor’s degree or bachelor’s or higher degree) and marital status (single, separated/divorced/widowed, or married) were self-reported. Combat exposure (deployed with combat, deployed without combat, or non-deployed) was assessed using military deployment data from DMDC and participants’ responses to key experiences included in the Millennium Cohort Study survey instrument based on the Walter Reed Army Institute of Research Land Combat Study combat measure (Kim, Kok, Thomas, Hoge, & Riviere, 2012). A variable indicating Millennium Cohort Study enrollment panel (1, 2, and 3) was also included. All covariates were measured at baseline.
Health behaviors
Health behaviors of interest, assessed using self-reported data, included smoking, alcohol consumption, bulimia nervosa, and binge eating, as well as baseline physical activity. These health behaviors were selected as potential coping strategies used by trauma survivors. Including these potential coping behaviors as covariates in multivariable models allowed examination of any association(s) between SH and SA and physical activity, while controlling for these other factors. Participants who had smoked at least 100 cigarettes in their lifetime and had not successfully quit smoking were categorized as current smokers. Former smokers were categorized as those who had smoked at least 100 cigarettes in their lifetime, but had quit successfully. Nonsmokers were those who had not smoked 100 cigarettes in their lifetime. Participants who answered that in the past year they “never” drank alcohol were categorized as nondrinkers. Those who endorsed drinking “rarely” were defined as infrequent drinkers, and those who reported drinking “monthly” or more often were categorized as “regular drinkers.” Eating disorder symptoms were assessed using the eating disorder module from the patient health questionnaire (PHQ), a standard instrument embedded in the Millennium Cohort Study questionnaire (Spitzer, Kroenke, & Williams, 1999). This eight-item module has been validated as a screening tool for bulimia nervosa and binge eating disorder (Striegel-Moore et al., 2010). Bulimia nervosa was defined as self-reporting loss of control over eating and consuming unusually large amounts of food as frequently as twice a week for the last 3 months plus endorsing at least one compensatory behavior—vomiting, taking laxatives more than twice the recommended dose, fasting, or exercising > 1 hr to avoid gaining weight after binge eating (American Psychiatric Association [APA], 2000). Binge eating disorder was defined as self-reporting loss of control over eating and consuming unusually large amounts of food as frequently as twice a week for the last 3 months, but not engaging in any of the aforementioned compensatory behaviors as often as twice a week.
Comorbid health problems
Comorbid health problems of interest were selected based on potential associations with physical activity identified in the published literature, including depression, PTSD, anxiety, life stressors, asthma, hypertension, sleep apnea, schizophrenia, and thyroid conditions. All were assessed at either the 2007-2008 survey cycle, or for Panels 1 and 2, from an earlier survey cycle, if those data were available. Depression, based on the nine-item PHQ depression scale, was deemed present if participants endorsed five or more depression items “more than half the days” or “nearly every day,” with at least one being “little interest or pleasure in doing things” or “feeling down, depressed or hopeless” (Spitzer et al., 1999). PTSD was based on self-reported responses to PTSD Checklist–Civilian Version, a standardized 17-item instrument embedded in the Millennium Cohort Study questionnaire (Weathers, Litz, Herman, Huska, & Keane, 1993). A positive screen was defined as reporting “moderate” or greater on enough items (i.e., at least one intrusion symptom, three avoidance symptoms, and two hyperarousal symptoms), mirroring the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000). Anxiety was identified if participants screened positive for either panic syndrome (seven items) or other anxiety syndrome (15 items) on the PHQ. Panic syndrome was defined as participants endorsing all four anxiety attack-related questions and at least four listed symptoms. Other anxiety syndrome was defined as participants endorsing experiencing “feeling nervous, anxious, on edge, or worrying a lot about different things” and at least three of the six listed anxiety symptoms on more than half the days in the past month. Life stressors were evaluated using a modified version of the social readjustment scale (Holmes & Rahe, 1967). The total number of stressors was calculated based on participants’ responses to questions about divorce/separation, major financial problems, physical assault, illness or death of a family member or loved one, and a disabling illness or injury. Asthma, hypertension, sleep apnea, schizophrenia, and thyroid condition were assessed using self-reported provider-based diagnoses.
Statistical Analysis
We conducted descriptive analyses comparing baseline demographic and military service characteristics, as well as medical comorbidities, by SH and SA status. A hierarchical regression approach was applied to examine any association(s) between SH and SA and subsequent physical activity levels. This approach was applied to examine groups of predictor variables and their impact on physical activity. First, an unadjusted multinomial regression was used to investigate any association of SH and SA with physical activity. We then used a series of multivariable multinomial regression models to further examine any association of SH and SA with physical activity by first including only (a) demographic and military characteristics, followed by (b) demographic/military characteristics and health behaviors, and finally the full model with (c) demographic/military characteristics, health behaviors, and comorbid health symptoms/conditions. This stepwise approach gives further insight into how these groups of variables influence the relationship of SH and SA with subsequent physical activity. Statistical analyses were performed using SAS software, Version 9.4.
Results
Of the 151,567 service members who were enrolled in Panels 1 to 3, 94,041 were in active duty or Guard/Reserve components at baseline. Among these 94,041 participants, 10,316 reported a childbirth or miscarriage 3 years prior to the completion of baseline or follow-up surveys. Of the 83,725 eligible participants, 29,453 did not complete a follow-up survey, 22 endorsed every disease listed on baseline or follow-up surveys, and 19,605 had missing covariate, exposure, or outcome data and were excluded. Therefore, 34,645 participants remained in our study population.
Of the 34,645 study participants, 687 (1.98%) reported recent SH only, and 204 (0.59%) reported recent SA at follow-up. Participants who reported SH or SA were more likely to have reported previous SH or SA at baseline (p < .001; Table 1). Those reporting SH only or SA at follow-up were more likely to be female, younger (birth year 1980 or later), less educated, not married, enrolled in most recent panel studied (Panel 3), in the U.S. Army, junior enlisted, and without deployment experience (all ps < .001; Table 1). In addition, participants reporting SH or SA were more likely to endorse more life stressors and comorbid health symptoms/conditions, including depression, anxiety, PTSD, and asthma, at baseline (all ps < .001; Table 2). Self-reported baseline physical activity levels were not significantly different across SH only and SA groups (p > .05). However, we observed statistically significant differences in physical activity at follow-up across categories of SH only and SA, such that participants reporting SH or SA were more likely to report either low or high levels of physical activity (p < .001; Table 3).
Baseline SH and SA Exposure, Physical Activity, and Demographic and Military Characteristics of Study Population.
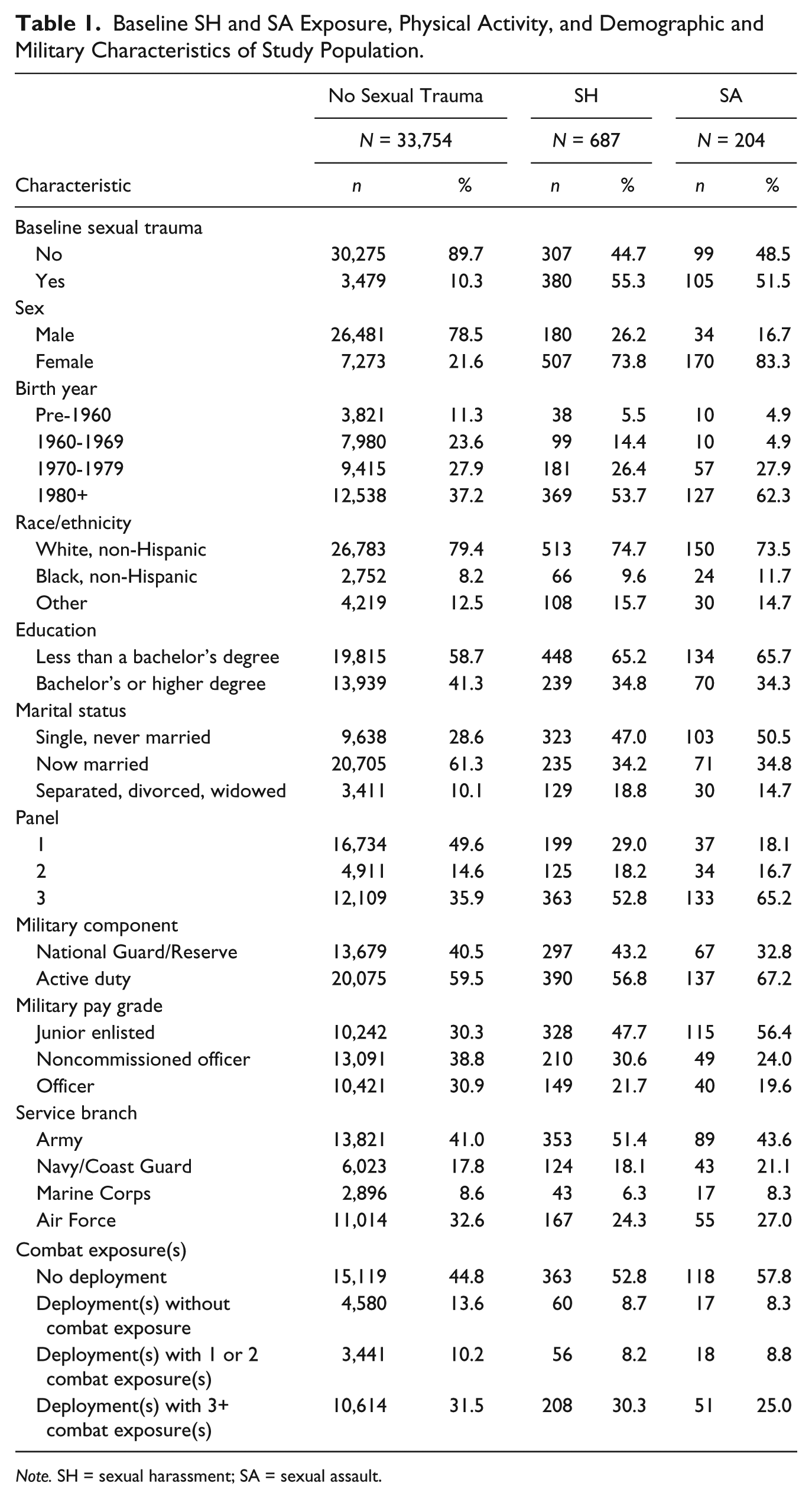
Note. SH = sexual harassment; SA = sexual assault.
Baseline Risk Behaviors and Health Conditions of Study Population in Relation to Recent SH Only and SA Exposure.
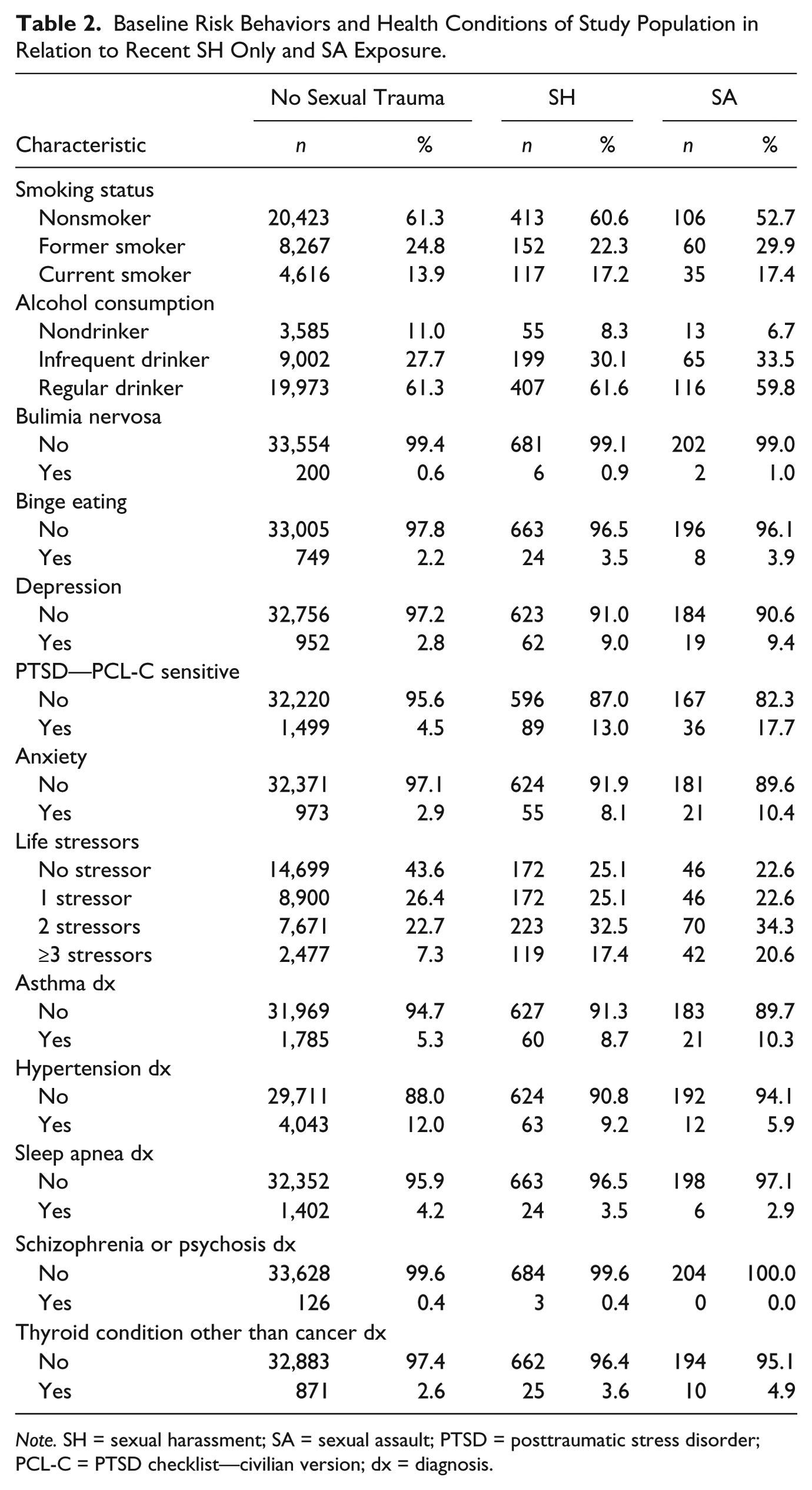
Note. SH = sexual harassment; SA = sexual assault; PTSD = posttraumatic stress disorder; PCL-C = PTSD checklist—civilian version; dx = diagnosis.
Self-Reported Physical Activity Levels at Baseline and Follow-Up Across Recent SH and SA Groups.
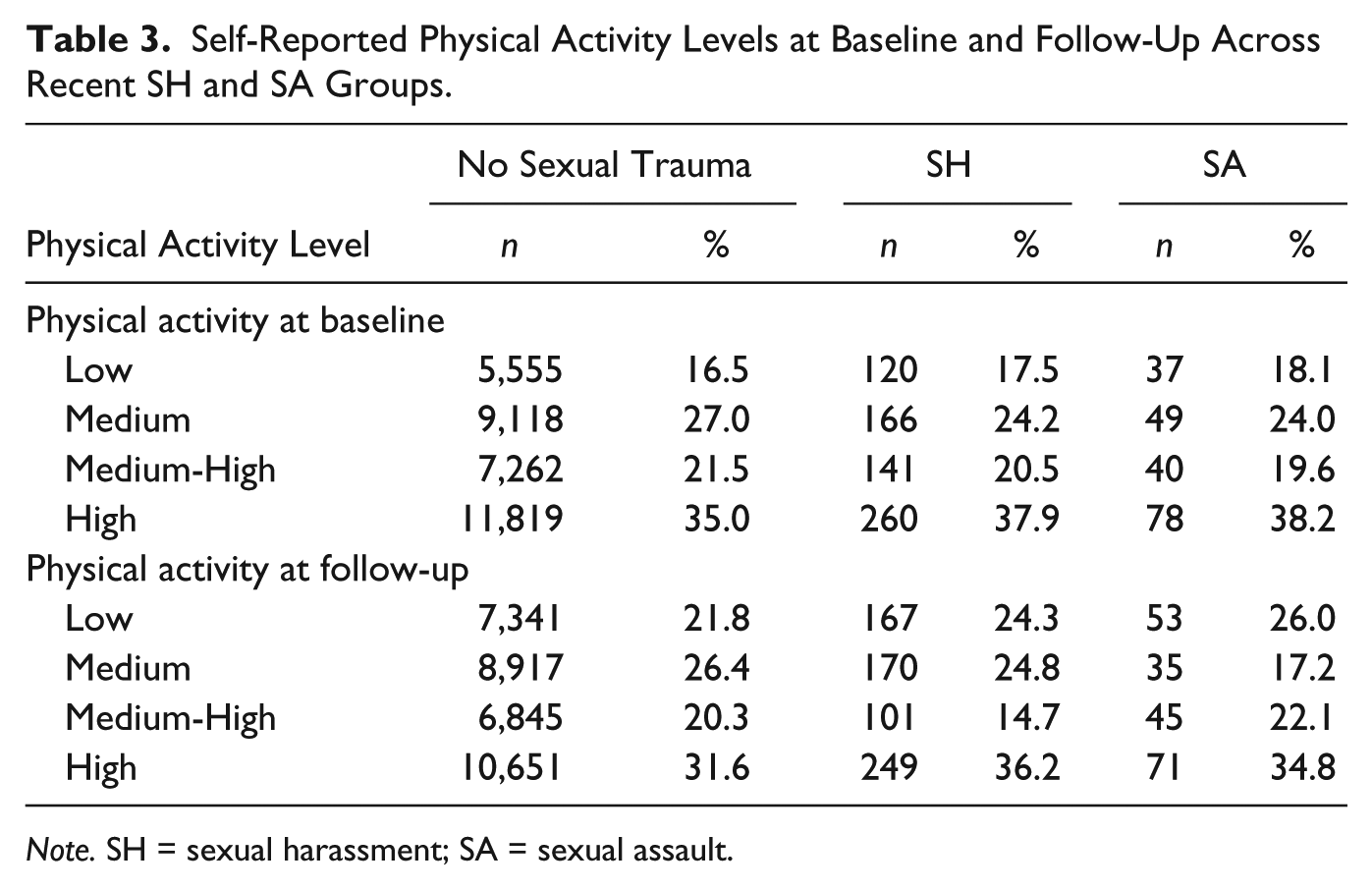
Note. SH = sexual harassment; SA = sexual assault.
Hierarchical regression models showed that among those self-reporting recent SA, the odds of engaging in high physical activity levels were significantly increased (Table 4). Overall, participants who reported recent SA were more likely to report 300 min/week or more physical activity. Although the magnitude of these associations attenuated with increasing number of covariates included in the model, the odds of high physical activity levels remained statistically significant in the fully adjusted model (medium-high activity: OR = 1.72, 95% CI = [1.08, 2.73]; high activity: OR = 1.58, 95% CI = [1.02, 2.44]). SA was also associated with low levels of physical activity (< 150 min/week) in Models 1 to 3 of the hierarchical regression. However, after controlling for other mental health disorders in Model 4, this association was not statistically significant.
Unadjusted and Adjusted ORs for Physical Activity Levels (REF = medium).
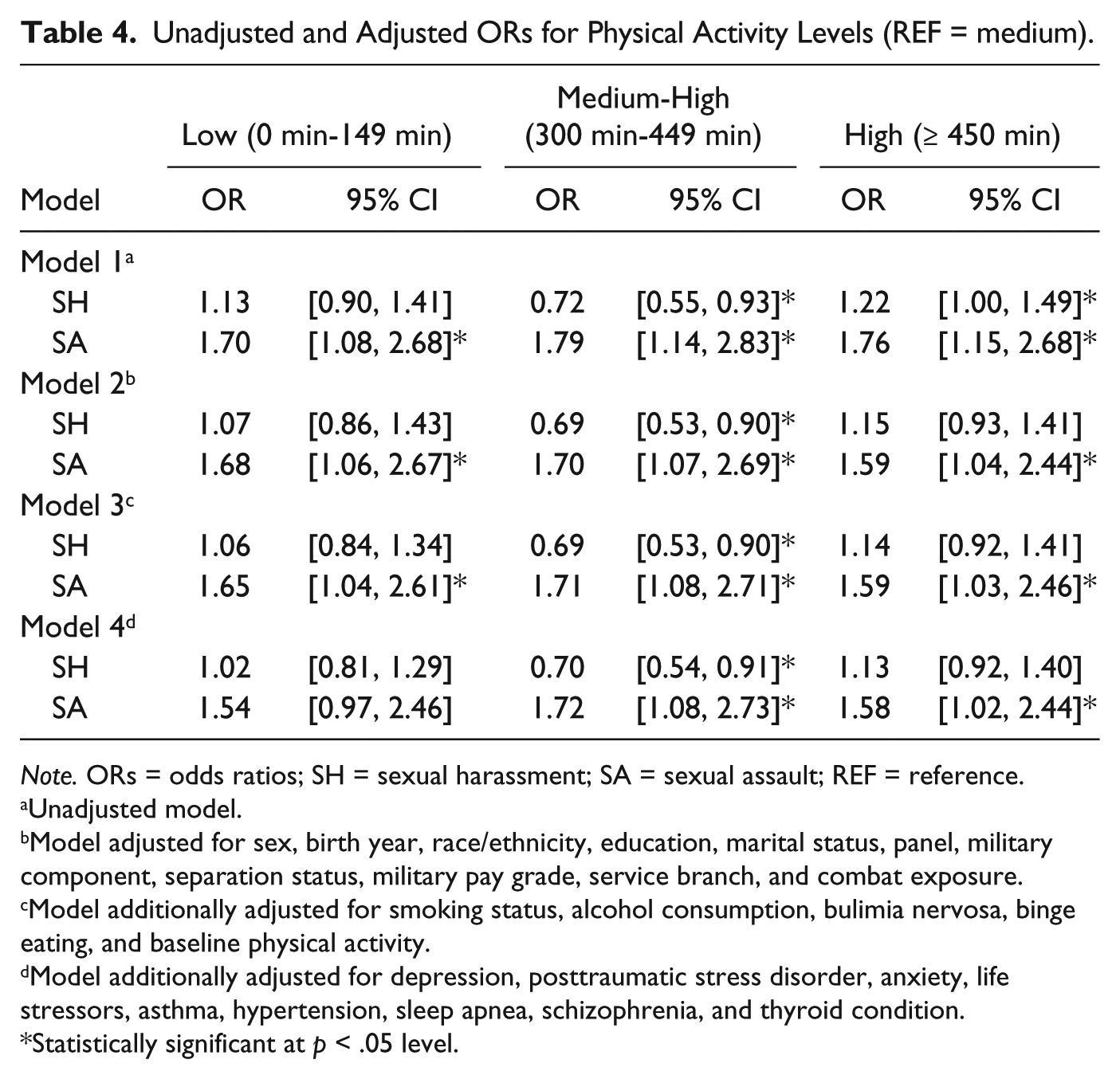
Note. ORs = odds ratios; SH = sexual harassment; SA = sexual assault; REF = reference.
Unadjusted model.
Model adjusted for sex, birth year, race/ethnicity, education, marital status, panel, military component, separation status, military pay grade, service branch, and combat exposure.
Model additionally adjusted for smoking status, alcohol consumption, bulimia nervosa, binge eating, and baseline physical activity.
Model additionally adjusted for depression, posttraumatic stress disorder, anxiety, life stressors, asthma, hypertension, sleep apnea, schizophrenia, and thyroid condition.
Statistically significant at p < .05 level.
In unadjusted models, SH was associated with higher odds of high physical activity, although this association did not remain significant in all subsequent adjusted models. In addition, we observed a statistically significant negative association between SH and medium-high physical activity levels in all four models. The observed associations between SH and lower odds of medium-high physical activity levels were consistent across unadjusted and adjusted models, and the magnitude of associations was not influenced by the addition of covariates in the models.
Discussion
Although there is a large body of literature examining SH and SA in military populations, to our knowledge, any association of SH and SA with physical activity among current service members has not been fully explored. Therefore, our study contributes to the generation of hypotheses that are important for understanding relationships of SA and SH with physical activity in a military population. Physical activity can be a coping behavior in response to trauma that is also an important marker of optimal functioning in the military profession. Poor physical performance may be an early indicator to commanders and the unit that an individual is not ready to engage in combat or endure the physical and psychological adversities associated with war. A decline in physical performance can arise both from lack of exercise and from excessive training resulting in fatigue, poor nutrition, or overuse injuries.
Our findings indicate that personnel who experience recent SA are more likely to report higher levels of physical activity compared with those without recent SH or SA. Although the magnitude of this association decreased after adjustment for demographic, military, medical conditions, and behavioral factors, the relationship remained statistically significant. In addition, those experiencing recent SA were more likely to report lower physical activity compared with those without recent SH or SA, but this association was no longer statistically significant after adjusting for mental health conditions.
The relationship between SH and physical activity was quite different from SA and physical activity. Among those who self-reported recent SH compared with no SH or SA, the odds of engaging in mid-level physical activity were significantly lower. The observed lower odds of medium-high physical activity among SH survivors and higher odds of low physical activity among SA survivors was consistent with previously reported reduction in vigorous physical activity among veterans with a history of sexual trauma (Lang et al., 2003).
It is notable that the association between SA and low physical activity was no longer significant after the addition of mental health conditions to the model. This could be due to known associations between mental health conditions and lower levels of physical activity (Chwastiak et al., 2011; Godfrey et al., 2013; Kozaric-Kovacic et al., 2009; Kukihara et al., 2014; Lang et al., 2003; Zen et al., 2012). The association between higher levels of physical activity and SA differs from what has been observed in a veteran population (Lang et al., 2003). However, it is aligned with our hypothesis that the military population may be more likely to utilize exercise as a coping behavior. The potential career consequences, including forced separation from military service, of using illicit drugs or alcohol as coping mechanisms could deter service members from these alternative maladaptive strategies and encourage the use of exercise instead. Although it may at first seem counterintuitive for SA to be associated with increased odds of reporting both low and high physical activity, these findings could represent two distinct subpopulations. There may be a subset of individuals who cope with sexual trauma by increasing their exercise, while another subset decreases their activity, which may possibly be due to comorbid depression or other mental health conditions.
Although we conceptualize exercise as a positive coping mechanism, too much exercise can also be maladaptive in some individuals. Although there is no guideline for how much exercise is considered unhealthy, elevated levels of physical activity maintained over time can be a source of concern. For example, excessive exercise may contribute to injury from overuse or deterioration of performance from overtraining (Falvey et al., 2009).
Our study found that those who experienced SH only had decreased odds of reporting medium-high levels of physical activity, despite an observed increase in odds among those who experienced assaults, compared with those who reported neither SH nor SA. It is reasonable to assume that the level of distress and subsequent coping strategy utilized may be different among individuals exposed to SH versus SA. SA involves a loss of control of one’s body, which perpetuates a feeling of powerlessness (Lucero, 2015). It is possible that individuals experiencing SA employ a higher level of distress as motivation to exercise more to diffuse anxiety or anger, regain confidence, and reinstate a sense of control over their bodies and their lives. The consistently significant associations between SA and the highest level of physical activity in our study support this hypothesis.
Our results that SH survivors had reduced odds of reporting medium-high levels of physical activity align with previous studies where SH had long-term negative mental and physical health effects (Godfrey et al., 2015; Kimerling et al., 2007; Millegan et al., 2016). Most importantly, without good coping strategies, individuals could be at a greater risk of more severe health effects (Bal, Van Oost, De Bourdeaudhuij, & Crombez, 2003). We found that participants who reported recent SH or SA were more likely to have previous SH and SA experiences, indicating that prolonged and/or repeated exposure was common among victims. Other studies have identified that risk for negative health outcomes with repeated traumatic events increases linearly with cumulative exposure over time (Anda et al., 2006; D’Andrea et al., 2011; Sledjeski, Speisman, & Dierker, 2008).
In addition, survivors of SA and SH are more likely to experience poorer mental and physical health. Reductions in physical activity may be an example of behaviors that can contribute to negative mental and physical health consequences. For example, we found that SH survivors had reduced odds of reporting medium-high levels of physical activity, which has the potential of affecting long-term physical and emotional well-being. Negative coping behaviors in the context of stressful situations, including SH and SA, could hinder mission readiness, whereas maintaining appropriate levels of physical activity is known to positively affect physical and psychological health (Mahmood, Levy, Vasan, & Wang, 2014; Pollock et al., 1998). Our study provides useful information on how individuals cope with SH and SA.
Limitations to the study should be considered. First, underreporting of SH and SA is common and could reduce the power and observed effect size of the associations examined in our study. However, participants were informed that all responses reported on Millennium Cohort Study surveys are held confidential, which is likely to minimize such underreporting. Underreporting could also be rooted in misclassification of SH and SA due to poor recall or a failure to properly classify the traumatic event. Missing data were also a limitation in this study. Subjects with missing information on variables of interest were excluded from analyses, but the physical activity and reports of recent sexual trauma did not differ between these excluded individuals and study participants (data not shown). Furthermore, Littman et al. (2010) previously assessed nonresponse bias in the Millennium Cohort Study and concluded that selected measures were not significantly affected by nonresponse. Therefore, the amount of missing data in this study could have reduced statistical power, but was not likely to have biased our findings. In addition, the level of physical activity used as a coping mechanism may change during the initial weeks after trauma compared with months or years following trauma. Such temporal effects are difficult to determine using these data, because time between exposure and outcome could vary between a few days to 3 years. Service members may also overestimate the amount of physical activity they perform due to miscalculation, poor recall, or negative impression management, because there is considerable pressure placed on service members to maintain fitness standards. Because existing data from an ongoing large cohort study were analyzed, data from behaviorally specific questions could not be used for this study. However, military personnel are required to participate in training on these topics to bolster prevention efforts. They are more likely to be familiar with these concepts than the general population without specific training in these topics.
Only two time points of physical activity were available in the current study. Future studies examining trajectories of fitness may be useful to identify changes in physical activity and their temporal relationship with sexual trauma. As a result of this information, therapeutic interventions could be identified to help service members monitor physical activity used as a coping behavior, as well as encourage other positive coping strategies to help survivors manage stress.
Current and former U.S. military service members constitute a large, diverse component of the U.S. population (approximately 10%). However, the results of this study may not be generalizable to civilian populations due to unique aspects of the military. Military culture promotes personal effectiveness and prioritizes physical fitness. It is possible that increases in physical activity are due to bolstering one’s capacity for physical self-defense or focusing on occupational success that may be linked to the military culture. However, there is no particular reason that these increases would be differential by sexual trauma status. Due to the nature of the study (e.g., data from an ongoing large cohort study), differences in individual experiences of SA and SH could not be determined. However, given the higher prevalence of SA and SH among women compared with men, we conducted analyses stratified by gender, although no substantive differences were found.
Our study also has important strengths. Although previous studies examined the relationship between physical activity levels and PTSD symptoms (Chwastiak et al., 2011; Godfrey et al., 2013; Kozaric-Kovacic et al., 2009; Kukihara et al., 2014; Zen et al., 2012), ours was the first to exclusively examine the relationship of SH and SA with physical activity among current service members. Previous studies have found the Millennium Cohort Study to be reasonably representative of the military as a whole (Riddle et al., 2007; Ryan et al., 2007; Smith, Smith, Gray, & Ryan, 2007). Given the available sample size, we were able to examine and control for a variety of behavioral, demographic, and military characteristics. The questionnaire used in the Millennium Cohort Study allowed us to quantify frequency and duration of physical activity and new-onset SA and SH occurring between baseline and follow-up surveys. We were also able to exclude those who do not have the same fitness standards, such as women who recently gave birth or had a miscarriage.
The results of this study are important because of the high number of reported events of SA and SH in the military. Findings from this current study, and other future work, may help to better inform prevention efforts and increase understanding of outcomes associated with sexual trauma. Our study findings are noteworthy because sexual trauma survivors may have difficulty adapting to unique stressors found in the military. The military requires service members to maintain a high level of performance despite ongoing stressful or dangerous environments, particularly in deployed settings. Therefore, the unique military lifestyle necessitates psychological hardiness and healthy coping styles to maintain mission readiness. Our findings are an important step in identifying subpopulations of sexual trauma survivors that differ by coping behaviors. In particular, the current study highlights how coping responses among current military members may be particularly intertwined with physical activity.
Footnotes
Acknowledgements
The authors thank the entire Millennium Cohort Study team from the Deployment Health Research Department, Naval Health Research Center, San Diego, as well as cohort members, and the Management Information Division, U.S. Defense Manpower Data Center, Seaside, CA, for providing data; we also appreciate support from Military Operational Medicine Research Program, U.S. Army Medical Research and Materiel Command, and the Henry M. Jackson Foundation for the Advancement of Military Medicine, Bethesda, MD.
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, Uniformed Services University of the Health Sciences, nor the U.S. Government. The study protocol was approved by the Naval Health Research Center Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human subjects. Research data were derived from an approved Naval Health Research Center, Institutional Review Board protocol number NHRC.2000.0007.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I, Connie Thomas as the corresponding author, am a military service member. This work was prepared in addition to my official duties. Title 17, U.S.C. §105 provides that copyright protection under this title is not available for any work of the U.S. Government. Title 17, U.S.C. §101 defines a U.S. Government work as work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties. Report Number 18-35 was supported by the U.S. Navy Bureau of Medicine and Surgery under work unit no. 60002.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Millennium Cohort Study is funded through the Defense Health Program, Veterans Affairs, and Military Operational Medicine Research Program of the U.S. Army Medical Research and Materiel Command (work unit 60002).