
Abstract
A wealth of empirical literature has documented that the experience of childhood maltreatment is related to an increased risk for the development of psychopathologies in adulthood. Empirical studies examining the factors that could possibly explain this relationship, however, remain sparse. The emerging literature on distress tolerance (DT) suggests that it could possibly act as an explanatory or mediating factor within this relationship. The current study, therefore, examined the mediating role of DT in the relationship between childhood maltreatment and psychopathology (posttraumatic stress disorder, depression, anxiety, and alcohol use) in adulthood in a university student population sample (N = 642). Results showed that childhood maltreatment was positively associated with caseness for all mental health outcomes under investigation. It was also found that individuals with higher levels of DT were less likely to experience adverse mental health outcomes. The results of the mediation analysis indicated that the exposure to childhood maltreatment remained associated with elevated risk for being in the symptomatic group across mental health outcomes, and that DT significantly mediated this relationship. These results provide insight into the relationship between childhood maltreatment and mental ill-health later in life, highlighting the importance of considering DT as a potential risk and resilience factor in this relationship.
Introduction
Despite widespread acknowledgment of the impact of childhood maltreatment on adult mental health, relatively few studies have sought to disentangle this relationship. Childhood maltreatment has been defined by Leeb, Paulozzi, Melanson, Simon, and Arias (2008) as an act, which may endanger the safety or well-being of a child through acts of commission (e.g., physical, sexual, and emotional abuse) or acts of omission (e.g., inadequate supervision, exposure to violent environments). Childhood maltreatment remains a pressing issue in the United Kingdom, where findings from a nationally representative household survey conducted by the National Society for the Prevention of Cruelty to Children (NSPCC) in 2009 indicated that approximately 5.9% of children below the age of 11 years experienced some form of severe maltreatment (e.g., contact sexual abuse, frequent physical abuse resulting in injuries, and prolonged periods of neglect). This figure rises to 8.9% for reports of any maltreatment incident by a parent or guardian (Radford et al., 2011). Furthermore, a review of meta-analytic studies estimated that the global prevalence of childhood maltreatment (experienced before the age of 18) was 12.7% for sexual abuse, 22.6% for physical abuse, 36.3% for emotional abuse, 16.3% for physical neglect, and 18.4% for emotional neglect (Stoltenborgh, Bakermans-Kranenburg, Alink, & IJzendoorn, 2015).
A strong link between childhood maltreatment and adverse mental health outcomes in adulthood has been consistently demonstrated in the literature (e.g., Kessler et al., 2010; Lang, Stein, Kennedy, & Foy, 2004; MacMillan et al., 2001; Springer, Sheridan, Kuo, & Carnes, 2007). Findings from the World Mental Health Survey conducted across 21 countries indicate that childhood maltreatment is associated with increased risk for developing any Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) disorder across all sociocultural samples (Kessler et al., 2010). A large body of literature has showed that childhood maltreatment may be specifically linked with chronic posttraumatic stress disorder (PTSD) symptomology (Marshall-Berenz, Vujanovic, Bonn-Miller, Bernstein, & Zvolensky, 2010), depression (Khan et al., 2015), anxiety (Nanda, Reichert, Jones, & Flannery-Schroeder, 2016), and alcohol use disorders (Elliott et al., 2014).
It has been suggested that due to the long-term and pervasive negative impact of childhood maltreatment on adult psychopathology, there may be factors, not yet fully understood, that affect this relationship (Kessler et al., 2010). Few studies have, however, sought to disentangle the nature of the mechanisms potentially maintaining this effect (Hardy et al., 2016). Understanding the intervening variables between established relationships within the social sciences greatly benefits understanding of observed relationships and how they are realized (Baron & Kenny, 1986). Recently, researchers have started examining the influence of indirect psychological factors in this relationship by implementing mediation analyses to examine how a variable may partially explain an observed relationship (Baron & Kenny, 1986). For example, Shevlin, McElroy, and Murphy (2015) examined the role of loneliness and found it to significantly mediate the relationship between childhood maltreatment and psychopathology.
Distress tolerance (DT), defined as the subjective or objective ability to remain resilient to adverse internal states and external events (Leyro, Bernstein, Vujanovic, McLeish, & Zvolensky, 2011), has also been noted as a potential mediating factor in the relationship between childhood maltreatment and adult psychopathology. The concept of DT is particularly salient in the study of traumatic stress reactions as greater understanding is sought of the mechanisms by which individuals subsequently develop mental health issues or display resilience. Marshall-Berenz et al. (2010) argued that individual-perceived ability to tolerate adverse emotional states following traumatic exposure and peritraumatic coping strategies in relation to PTSD symptomology, specifically avoidance behaviors, may influence the trajectory of symptom development and treatment outcome. Further to this, traumatic exposure in childhood has been shown to affect subsequent emotion regulation and psychopathological outcomes (Cook et al., 2005). It is, hence, argued that traumatic exposure in childhood could potentially result in disruption to the development of effective DT strategies (Briere & Elliott, 2003) and, therefore, lead to distress intolerance or low DT.
More specifically, exposure to trauma in childhood may interfere with the development of self-regulation/resilience (Dunn, Nishimi, Powers, & Bradley, 2017). It is argued that maladaptive states may become traits through altered neurobiology and developmental engraining (Perry, Pollard, Blakley, Baker, & Vigilante, 1995). In this sense, it is argued that DT serves as a proxy measure of maladaptive internal regulation processes, influenced by the presence of trauma and influencing the development of psychopathological symptoms later in life. Moreover, when faced with distress or adverse situations, individuals with low DT may be more likely to engage in maladaptive responses, such as avoidant coping, which serve as negative reinforcement strategies (e.g., avoiding negative emotions). Avoidance alleviates distress, which, in turn, leads to and reinforces more avoidance behaviors. Conversely, individuals with high levels of DT may be better able to cope with their negative emotions and less likely to engage in maladaptive responses (Leyro, Zvolensky, & Bernstein, 2010). Therefore, if an individual with low DT experiences a traumatic event, he or she may be more likely to attempt to minimize his or her distress by employing maladaptive coping strategies and subsequently more likely to experience psychopathological symptoms (Leyro et al., 2010).
This theory has been supported by studies, which showed that individuals with low DT are more likely to developed eating disorders (Anestis, Selby, Fink, & Joiner, 2007) and engage in drug and alcohol abuse (Buckner, Keough, & Schmidt, 2007) or self-harm behaviors (Chapman, Gratz, & Brown, 2006), all of which could be considered affect avoidant coping strategies and indicative of issues with DT. In recent years, researchers have consistently documented the role of DT in the development of specific mental health outcomes, such as trauma-related disorders, anxiety, depression, and problematic substance use. For example, in relation to PTSD, Vujanovic, Bon-Miller, Potter, Marshall-Berenz, and Zvolensky (2011) found that lower individual levels of DT were positively associated with several symptom clusters of PTSD, as well as overall symptom severity, in a sample of trauma-exposed adults. Similarly, Marshall-Berenz et al. (2010) found that DT explained 6% of the variance in PTSD symptom severity, while controlling for traumatic experiences and sociodemographic characteristics. Similar results have been reported in a vast majority of the existing studies examining the link between DT and PTSD (Vujanovic, Bon-Miller et al., 2011; Banducci, Connolly, Vujanovic, Alvarez, & Bonn-Miller, 2017).
In relation to anxiety disorders, Keough, Riccardi, Timpano, Mitchell, and Schmidt (2010) reported that, in a sample of university students, there was a significant negative association between DT and a wide range of anxiety-related symptoms, including those that characterize social anxiety, obsessive compulsive disorder, and panic disorder. Similar results were reported in a study assessing treatment-seeking university students with primary diagnoses of anxiety disorders; lower levels of DT predicted generalized anxiety disorder (GAD), social anxiety, and obsessive compulsive disorder, but not panic disorder (Laposa, Collimore, Hawley, & Rector, 2015). Indeed, Leyro et al. (2010) argued that DT is conceptually linked to anxiety as those low in DT are more likely to fail to reconcile feelings of distress and have these feelings perpetuate. In this sense, it can be argued that low DT may result in psychopathological outcomes in the form of generalized anxiety disorders.
Depression has also been found to be associated with DT. Both the general population and clinical studies have found that individuals with higher levels of depression symptoms exhibit lower levels of DT (Barnhofer, Brennan, Crane, Duggan, & Williams, 2014; Keough et al., 2010; Peterson, Davis-Becker, & Fischer, 2014). For example, Barnhofer et al. (2014) found that lower levels of DT among survivors of childhood abuse were significantly associated with persistent depressive symptoms. Those with higher DT were more likely to be in the remitting symptom group. Further to this, research has shown that stressful life events throughout adolescence affect those with lower DT more greatly, with this group more likely to suffer subsequent depressive symptoms (Felton et al., 2019). It is believed that DT is established in childhood, and this may have implication for subsequent mental health trajectories (Felton et al., 2019).
Taken together, the extant literature suggests that childhood maltreatment is associated with poor adult mental health, and that low DT is a risk factor for mental ill-health. The aim of the current study was to extend this area of research by examining DT as a mediator of the relationship between childhood maltreatment and adult mental health outcomes. There is greater emerging precedent to examine the indirect relationship between childhood maltreatment and psychopathology, understanding the mechanisms of this relationship (see Shevlin et al., 2015). Research has applied mediation methods to the study of trauma and mental health outcomes with a proposed manifest variable of an underlying trait, that is, assessing maladaptive coping as a mediator (Choi et al., 2015). Extant theoretical perspectives on DT suggest that this may qualify the development and maintenance for psychopathology (Leyro et al., 2010). This investigation, therefore, seeks to extend understanding of the relationship between childhood maltreatment and trauma, applying mediation methodology to the manifest concept of DT to further understand the posttrauma development of psychopathology.
To the best of our knowledge, no previous study has examined the role of DT as a mediator of this relationship. Understanding the possible role of DT in the relationship between childhood maltreatment and adult mental health could have important implications for planning both prevention and intervention programs. The following was hypothesized:
Method
Procedure and Participants
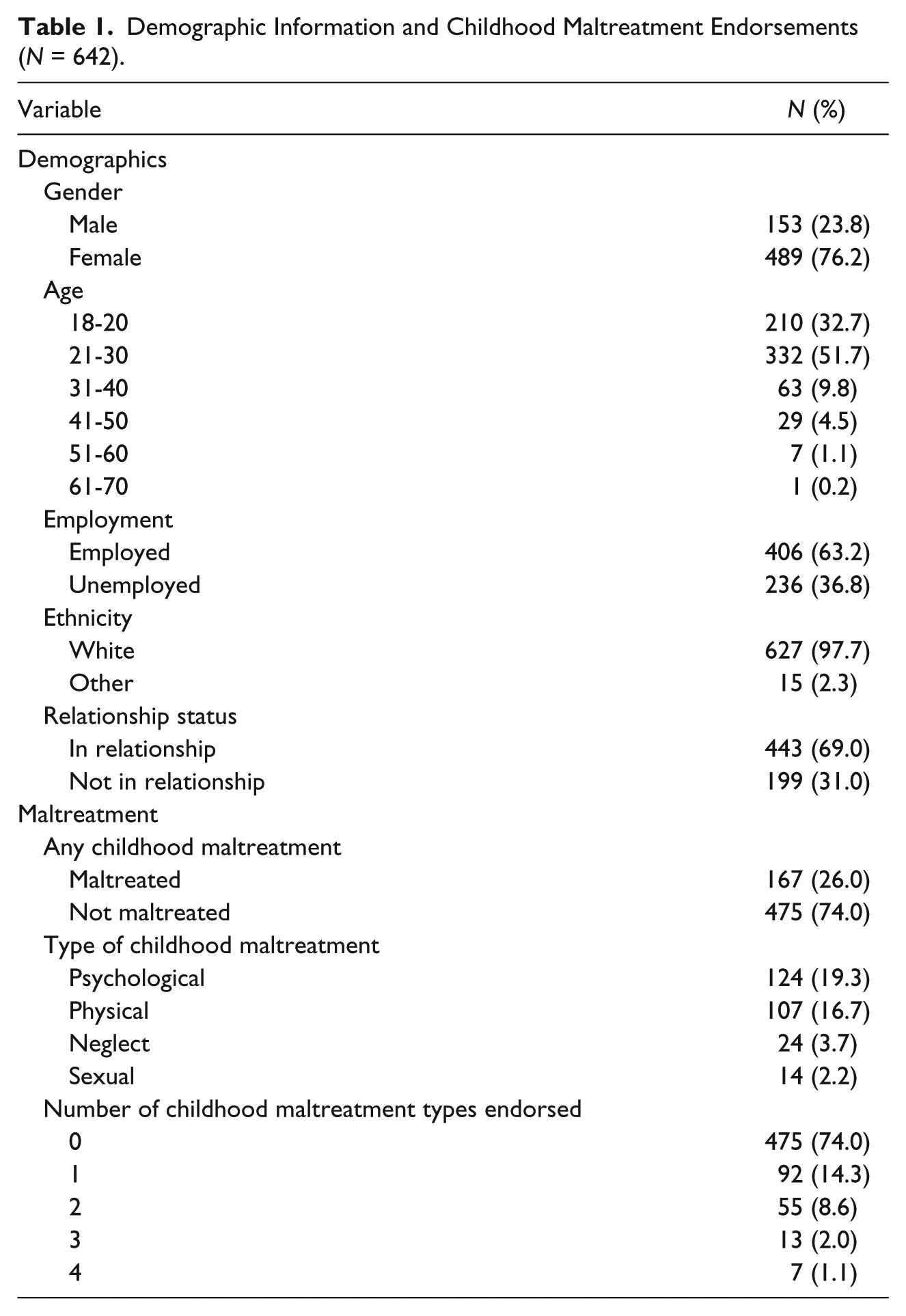
This study was conducted as part of a larger scheme of research examining the effects of intimate partner violence on mental health outcomes among students attending a university in Northern Ireland between October 2014 and March 2015. All procedures were approved by the institutional ethics committee. Participants were recruited via an email including a weblink to complete an online survey via Qualtrics. Reminders were sent once a month over a period of 6 months and monthly incentives of a £50 Amazon voucher were offered. The time required to complete the survey was approximately 20 to 30 min. A total of 25,000 emails were distributed with a response rate of 6% (N = 1,416). Participants who did not answer the relevant measures for this study and those who were missing 20% or more data on any of the relevant measures were excluded (n = 508). An additional 25 cases were excluded due to missing demographic information, and the remaining amount of missing data (0.31%) was estimated using the expectation maximization algorithm in SPSS. The effective sample was composed of 642 students (153 males and 489 females) aged between 18 and 61 years (M = 24.59 years, SD = 7.46 years). The majority were White (97.7%), currently in some form of employment (63.2%), and currently in a relationship (69.0%). Full demographic information is displayed in Table 1.
Demographic Information and Childhood Maltreatment Endorsements (N = 642).
Measures
Sociodemographic characteristics relevant to the current study included participants’ sex, age, and relationship status, which were included as covariates in the analyses. Relationship status was included as a proxy of social support as this has been shown to protect against the development of psychopathology among university students (Braithwaite, Delevi, & Fincham, 2010). Relationship status was binary coded as 1 = in a relationship (dating, cohabiting, married) or 2 = not in relationship (single, widowed, separated, divorced). Students were also asked about their ethnicity; however, because 97.7% of the effective sample reported their ethnicity as White (see Table 1), this variable was excluded from the analyses.
Childhood maltreatment was assessed using four items developed for the current study based on the measurements used by Christoffersen, Armour, Lasgaard, Andersen, and Elklit (2013). The current study collapsed the original 24 items examining the presence of abuse used by Christoffersen et al. (2013) into their respective maltreatment categories: neglect, physical assault, psychological abuse, and sexual abuse before the age of 12, which is a cutoff commonly used in childhood maltreatment research (see Holt, Buckley, & Whelan, 2008). The items used in the current study were worded as follows:
neglect (e.g., left alone in the house for days, starved due to lack of food, made to wear dirty clothes),
physical assaults (e.g., slapped, punched, kicked, beaten with objects, left with marks and bruising),
psychological (e.g., humiliated in public, called names, made to feel unwanted/unloved/worthless), and
sexual assaults (e.g., experienced sexual touching, attempted, forced or completed intercourse, other sexual behaviors).
Response options were never, hardly ever, occasionally, sometimes, frequently, almost always, and don’t know. These responses were recoded into binary positive or negative endorsements of maltreatment exposure. Response options never or hardly ever were coded as negative endorsements (“not maltreated”), because those who experience maltreatment in a single instance, or the duration of maltreatment is less than 7 days, have previously been found to significantly differ in terms of mental health outcomes from those who experience sustained abuse and neglect (see Bagley & Mallick, 2000). Response options occasionally to almost always were coded as positive endorsements (“maltreated”) and the response option don’t know was coded as missing.
Traumatic exposure was assessed using the Stressful Life Events Screening Questionnaire (SLESQ; Goodman, Corcoran, Turner, Yuan, & Green, 1998). The SLESQ is a 13-item screening measure of individual stressful and potentially traumatic exposure to specific stressors (e.g., abuse, assault, and the threat of harm) and other general perceived threats to individual safety (e.g., warzone exposure or any event not described by the previous items). Responses are coded as “yes” or “no” for each stressful exposure.
PTSD was assessed using the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013; PCL-5; Weathers et al., 2013). The PCL-5 is a 20-item inventory assessing the presence of PTSD symptomatology as outlined by the DSM-5 (American Psychological Association, 2013). Questions ask respondents to report to what extent (0 = not at all to 4 = extremely) they have been bothered by specific symptoms of PTSD in the past month in relation to their perceived worst traumatic event identified through SLESQ. Total scores range from 0 to 80. The current study used the recommended cutoff score of 33 (Weathers et al., 2013) to divide participants into symptomatic and nonsymptomatic PTSD groups. The PCL-5 has demonstrated good internal consistency, reliability, and validity in a variety of studies across numerous populations (Sveen, Bondjers, & Willebrand, 2016) and had a good internal consistency in the current sample (α = .96).
Depression was assessed using the Patient Health Questionnaire–9 (PHQ-9; Kroenke, Spitzer, & Williams, 2001). Each item within the PHQ-9 is based on one of the nine DSM-IV symptoms for major depressive disorder. Responses range from 0 (not at all) to 3 (nearly every day) and reflect the frequency of symptoms experienced in the previous 2 weeks. Total scores can range from 0 to 27 and a cutoff score of 10 was used to categorize participants into symptomatic and nonsymptomatic depression groups (Kroenke et al., 2001). The internal consistency of PHQ-9 was good in the current sample (α = .92).
Anxiety was assessed using the Generalized Anxiety Disorder–7 (GAD-7) screener (Spitzer, Kroenke, Williams, & Löwe, 2006). The GAD-7 is a seven-item questionnaire examining the frequency of various behavioral symptoms of anxiety over the past 2 weeks. Scores range from 0 (not at all) to 3 (nearly every day), yielding a possible score range of 0 to 21. GAD-7 has been found to be a reliable measure of anxiety in the general population (Löwe et al., 2008) and in the current sample, it had good internal consistency (α = .92). A cutoff score of 10 was used to categorize participants into symptomatic and nonsymptomatic anxiety groups based on the recommendations of Spitzer et al. (2006).
Alcohol use was assessed using the Alcohol Use Disorders Identification Test (AUDIT; Babor, Higgins-Biddle, Saunders, & Monteiro, 2001), which is a 10-item measure assessing the respondents’ dependence on alcohol and harmful and hazardous alcohol use. In the United Kingdom, 72% of undergraduate students have been found to engage in frequent binge drinking behaviors (Balodis, Potenza, & Olmstead, 2009), and we, therefore, utilized the cutoff score of 10 (possible range = 0-40) to categorize participants into problematic and nonproblematic alcohol use groups. The AUDIT has been shown to display sufficient reliability and validity as a screening tool to identify possible hazardous and harmful alcohol use (Daeppen, Yersin, Landry, Pécoud, & Decrey, 2000). The internal reliability in the current study was good (α = .82).
DT was assessed using the Distress Tolerance Scale (DTS; Simons & Gaher, 2005). The DTS is a 15-item inventory measuring the subjective psychological distress experienced by the individual. Each item is rated on a scale from 1 to 5, with one item reverse coded and, hence, negatively scored. Total scores may range from 0 to 70. Higher total scores indicate greater perceived ability to withstand adverse psychological states, whereas lower scores indicate a perceived inability to withstand such states. The DTS has been shown to possess good psychometric properties, demonstrating high convergent and discriminant validity, and high internal consistency in both university student and clinical populations (Marshall-Berenz et al., 2010; Simons & Gaher, 2005). In the current study, it had good internal consistency (α = .94).
Analytic Plan
Background characteristics, specifically age, gender, and relationship status, were controlled for in the analysis, as these constructs have previously been shown to influence psychopathology (see World Health Organization, 2014). For example, gender differences have previously been noted between the mental health sequel following traumatic exposure, with females reporting more emotional difficulties and anxiety symptoms and males reporting greater suicidal ideation and alcohol and substance use disorders (Afifi, 2007; Chaplin, Hong, Bergquist, & Sinha, 2008). Males have also been found to report higher levels of DT than females (Simons & Gaher, 2005). In addition, age was included as a covariate, because older individuals have been found to report more affective symptomology and fewer behavioral difficulties than younger individuals (Afifi, 2007; Kiejna et al., 2015).
The current study implemented a similar analytic model to the work of Shevlin et al. (2015), who examined loneliness as a mediating variable of the relationship between childhood maltreatment and psychopathology. Three regression models were specified and tested using the robust maximum likelihood estimator in Mplus 7.3 (Muthén & Muthén, 1998-2015). Model 1 was a multivariate logistic regression model and contained the binary coded mental health outcomes (PTSD, depression, anxiety, alcohol use), which were regressed on the childhood maltreatment variable. Childhood maltreatment was binary coded with “not maltreated” being the reference category. At this stage, the demographic variables were added to the model as covariates, but their paths to the mental health outcomes were fixed to zero. DT was also added as a mediator, but its paths to the dependent variables (mental health outcomes), and from the predictor variables (childhood maltreatment and covariates), were fixed to zero. This was implemented for the purposes of conducting chi-square difference tests for direct comparison of the different models. In Model 2, the paths from the covariates to the mental health outcomes were freely estimated, but the paths to and from DT remained fixed. For gender, “female” was the reference category and for relationship status, the reference category was “in a relationship.” Age was entered into the model as a continuous variable. This model similarly represented a multivariate logistic regression. Finally, Model 3 was the full mediation model, in which the paths to and from DT were freely estimated (see Figure 1). DT was entered into the model as a continuous variable. The effects from childhood maltreatment and the covariates to DT were linear regressions, and the paths from DT to the mental health outcomes were logistic regressions. Chi-square difference tests were used to compare Model 1 versus Model 2 and Model 2 versus Model 3 to determine the best fitting model. All models are depicted in Figure 1.
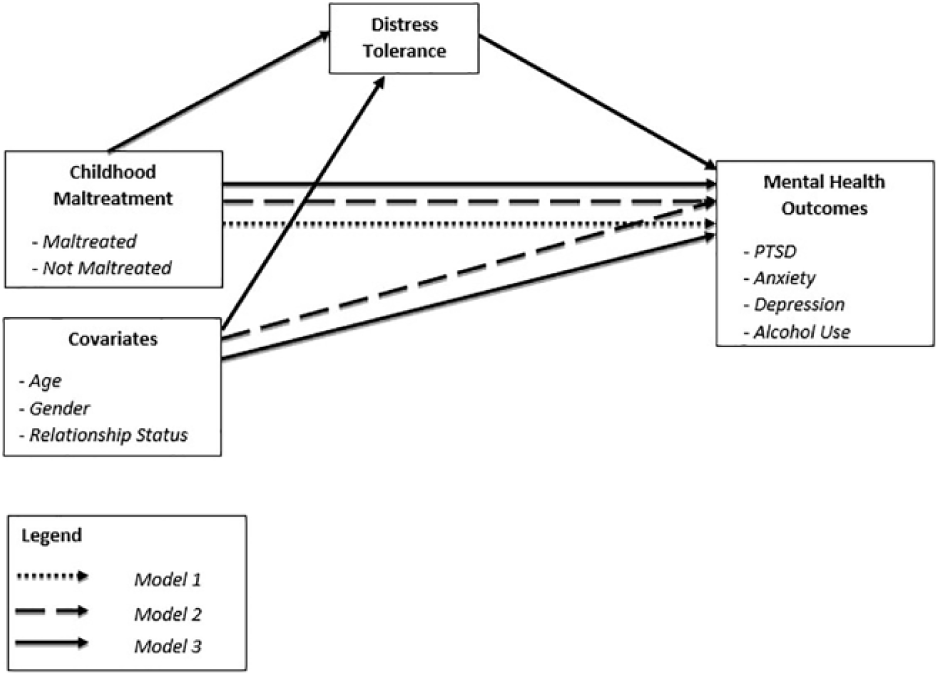
Conceptual model diagram.
Results
Descriptive statistics of the effective sample on childhood maltreatment, DT, and the mental health outcomes are shown in Tables 1 and 2. The majority of participants endorsed no experience of childhood maltreatment (n = 475, 74.0%), with 11.7% of participants experiencing two or more forms of childhood maltreatment. Among those who experienced any maltreatment, the mean number of different types of childhood maltreatment experienced was 1.61 (SD = 0.81). The mean DT score for participants who endorsed childhood maltreatment was 37.21 (SD = 14.95, median = 37.00) and for participants who did not endorse childhood maltreatment, it was 41.71 (SD = 15.88, median = 43.00). Data were found to be not normally distributed; hence, the Mann–Whitney U test was used, showing that this difference was significant (U = 32,799.50, p < .001).
Descriptive Statistics and Bivariate Correlations Between DT and the Mental Health Outcomes.
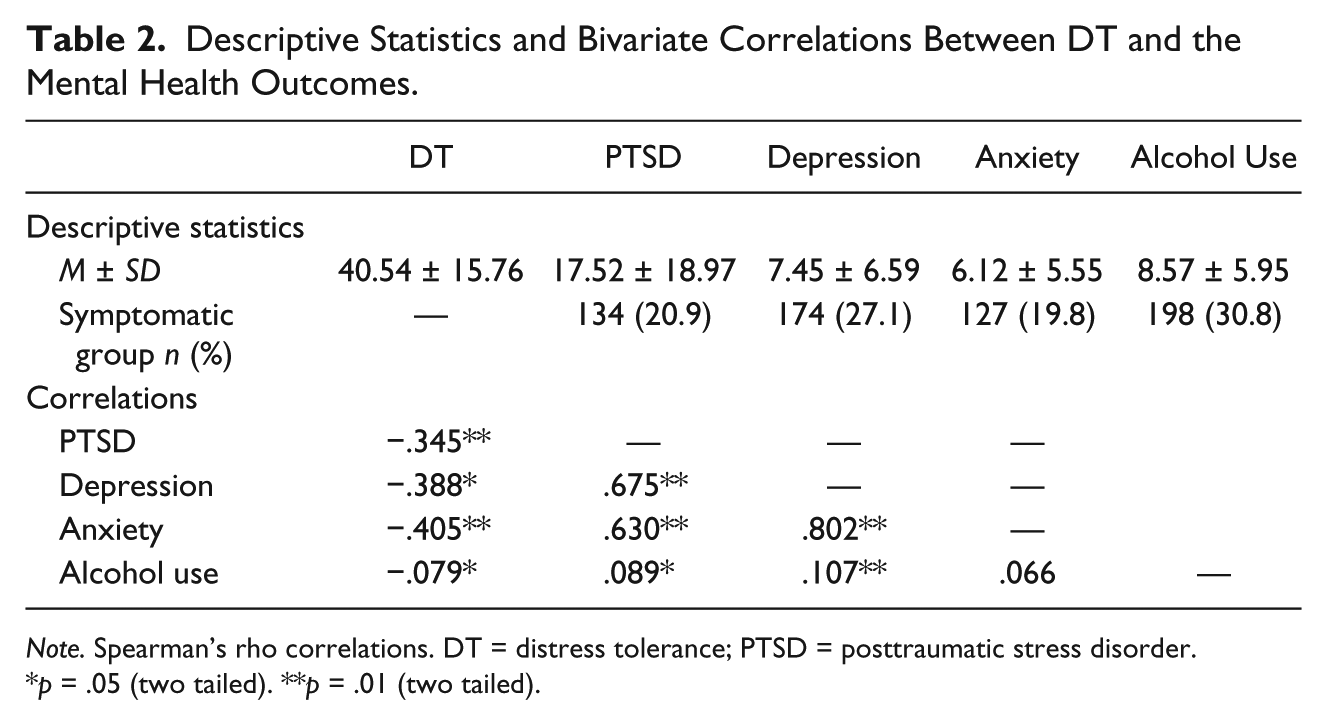
Note. Spearman’s rho correlations. DT = distress tolerance; PTSD = posttraumatic stress disorder.
p = .05 (two tailed). **p = .01 (two tailed).
Table 3 shows the results of the regression analyses and the estimates for the indirect effects through DT. In Model 1, childhood maltreatment was found to significantly predict all mental health outcomes, suggesting that the likelihood of having a probable diagnosis of PTSD, depression, anxiety, or alcohol use disorder is increased for those reporting childhood maltreatment. In Model 2, where covariates were introduced, childhood maltreatment remained a significant predictor of all mental health outcomes (see Table 3). This model provided a significantly better fit than Model 1, which did not include the covariates (∆χ2 = 55.483, ∆df = 12, p < .001). A number of covariates were found to significantly predict the mental health outcomes. Females and those who were currently not in a relationship were significantly more likely to have a probable PTSD diagnosis, females and younger individuals were more likely to meet the criteria for major depression, and males, younger individuals, and those currently not in a relationship were significantly more likely to have a probable alcohol use disorder (see Table 3 for odds ratios).
ORs and CIs for the Direct and Indirect Effects.

Note. OR = odds ratio; CI = confidence interval; PTSD = posttraumatic stress disorder; DT = distress tolerance.
p < .05. **p < .01. ***p < .001.
Model 3 (see Figure 1), which included the covariates and the mediator, provided a significantly better fit than Model 2 (∆χ2 = 240.982, ∆df = 8, p < .001). The odds ratios for the direct effects of childhood maltreatment on the mental health outcomes remained significant, but were reduced, ranging from 1.562, 95% confidence interval (CI) = 1.054-2.315, for alcohol use disorder to 3.493 (95% CI = 2.242-5.443) for PTSD. PTSD and depression were further significantly predicted by female gender and alcohol use was significantly predicted by younger age, male gender, and not being in a relationship (See Table 3 for odds ratios). In addition, it was found that the indirect paths from childhood maltreatment through DT to the mental health outcomes were all statistically significant. Together with the reduced odds ratios for the direct effects of childhood maltreatment on the mental health outcomes, the results suggest that DT is a significant mediator of this relationship; as DT increases, the likelihood of having a probable diagnosis of any of the mental health outcomes decreases.
Discussion
The primary aim of this study was to extend the existing knowledge regarding the relationships between childhood maltreatment, DT, and mental ill-health by examining DT as a possible mediating variable. First, the rates of childhood maltreatment in the sample showed that 475 (74%) respondents did not endorse any experience of childhood maltreatment. This concurs with previous literature, which has found that the majority of the population do not experience childhood maltreatment or victimization (Burns, Lagdon, Boyda, & Armour, 2016). Of those who positively endorsed experiencing a form of childhood maltreatment, 16.7% endorsed physical abuse, 19.3% endorsed psychological abuse, 2.2% endorsed sexual abuse, and 3.7% endorsed neglect. The rates of these specific abuse and neglect experiences were considerably lower than the worldwide prevalence rates estimated by Stoltenborgh et al. (2015). However, the difference in prevalence rates could be due to differing populations, definitions of abuse, and the measurement of maltreatment. It should also be noted that the current sample was drawn from a university student population and those who have experienced childhood maltreatment may be less likely to attend higher education institutions, due to the negative impacts of childhood maltreatment on educational achievement and mental health (Romano, Babchishin, Marquis, & Fréchette, 2015).
When examining the relationship between childhood maltreatment and the mental health outcomes, the results revealed that childhood maltreatment was associated with an increased likelihood for the development of PTSD, depression, anxiety, and problematic alcohol use, thus supporting our hypothesis. These findings are consistent with a large body of evidence that links childhood maltreatment to adult psychopathology (e.g., Armour et al., 2016, 2014; Kessler et al., 2010; Lauterbach & Armour, 2016; McLafferty et al., 2015; Murphy, Shevlin, Armour, Elklit, & Christoffersen, 2014; Springer et al., 2007).
The results also demonstrated that higher DT was associated with a decreased likelihood of experiencing symptoms of the four mental health disorders under investigation, again supporting our hypothesis. This suggests that higher levels of DT could be a protective factor against PTSD, depression, anxiety, and alcohol use disorder. This finding is consistent with previous research, which has evidenced that low DT is associated with an increased risk for various forms of mental health disorders in adulthood (Leyro et al., 2011; Vujanovic, Bon-miller, et al., 2011). Furthermore, as previously noted, the link between low DT and psychopathology could partly be explained by the use of maladaptive coping strategies, such as alcohol misuse. It has been argued that individuals with higher DT would be expected to cope more readily with adverse situations and emotional states, thus being protected from the development of psychopathology (Leyro et al., 2011). However, those experiencing low DT are at elevated risk of increased negative appraisals and reduced ability to be resilient to distressing trauma-related symptoms (Resick, Monson, & Chard, 2007). This, in turn, may increase the risk of using maladaptive coping strategies (Leyro et al., 2011), such as avoidance behaviors (Fetzner, Peluso, & Asmundson, 2014) or substance use (Buckner et al., 2007). For example, Fetzner et al. (2014) found that low DT specifically predicted avoidance and reexperiencing PTSD symptoms. The authors described the relationship as a self-perpetuating cycle, in which an individual with low DT, who had experienced a trauma, has a lowered perceived ability to effectively cope with reexperiencing symptoms. In this sense, individuals may be argued to use avoidance strategies, which perpetuate or maintain the reexperiencing symptoms (Fetzner et al., 2014). Consistent with this argument, Jeffries, McLeish, Kraemer, Avallone, and Fleming (2016) found that low DT significantly predicted suppression, rumination, and avoidance.
Although previous studies have found that low DT is associated with poor mental health (Greenberg, Martindale, Collum, & Dolan, 2014; Keough et al., 2010; Marshall-Berenz et al., 2010), to the best of our knowledge, the role of DT as a mediator in the relationship between childhood maltreatment and adult mental health, has not been previously explored. As predicted, the current study found that when DT was introduced into the model as a mediator, the strength of the relationship between childhood maltreatment and the negative mental health outcomes was reduced, supporting the hypothesis of DT as a significant mediator. This finding concurs with previous research, which showed that DT mediated the relationship between trauma exposure and the use of alcohol as a coping strategy in an adult community sample (Vujanovic, Marshal Berenz, & Zvolensky, 2011). Similarly, Holliday, Pedersen, and Leventhal (2016) found that in a sample of trauma-exposed veterans, DT mediated the relationship between trauma exposure and alcohol use. Although examining different populations and outcomes, the similarity in the results of these two studies and the current study suggests that higher DT results in lower rates of negative mental health outcomes and it could, therefore, serve as a protective factor in the relationship between childhood maltreatment and later psychopathology. Further to this, this study compliments and extends the existing literature base examining the context of childhood maltreatment as a potentially traumatic exposure influencing trait levels of DT, which, in turn, may influence the development of psychopathology.
Implications
These findings have important implications for the development and implementation of intervention and prevention strategies that could be used specifically to assist childhood trauma survivors with lower DT to cope with their traumatic experiences. Furthermore, findings emphasize the importance of building resilience, which in the face of adversity, could protect against the development of adverse mental health outcomes. If replicated in future studies, assessment of DT could be integrated within initial clinical assessments of survivors of childhood maltreatment to possibly establish the risk of developing adverse mental health outcomes. Prevention strategies could then incorporate elements of teaching or enhancing DT. Indeed, teaching DT skills within dialectical behavior therapy for the treatment of borderline personality disorder is argued to address emotion dysregulation, which is considered central in the development of borderline personality symptoms (Lynch, Chapman, Rosenthal, Kuo, & Linehan, 2006) that are often linked to childhood maltreatment (Hecht, Cicchetti, Rogosch, & Crick, 2014). Similar training could be delivered to youth who have experienced childhood maltreatment to lessen their chances of developing negative mental health outcomes.
Limitations and Future Research
The results of this study should be considered in light of some notable limitations. First, due to the cross-sectional design of this study, the temporal order of childhood maltreatment and the onset of psychopathology could not be formally established, although it could be inferred, given that childhood maltreatment was assessed in relation to the first 12 years of life and psychopathological symptomology was assessed in relation to the past few weeks/months. In addition, the construct of DT currently lacks a unified theory and, although widely regarded as a stable trait, there is little evidence to indicate its stability across the life span, as much of the existing research in this area is cross sectional (Leyro et al., 2010). Future studies should, therefore, employ longitudinal designs. Third, experience of trauma beyond the age of 12 was not controlled for, as it was not possible to establish from the measures used in the current study, whether the traumatic experiences reported in the SLESQ were the same or different to the ones queried with the four childhood maltreatment questions. It should, however, be noted that previous research has demonstrated a significant association between childhood maltreatment and mental ill-health even when other lifetime trauma is controlled for (Khoury, Tang, Bradley, Cubells, & Ressler, 2010; Spertus, Yehuda, Wong, Halligan, & Seremetis, 2003). Evidence, however, exists to suggest that those who experience childhood maltreatment are at increased risk of subsequent victimizations (Coid et al., 2001), which could compound the effects on mental ill-health. Future studies should utilize measures that clearly differentiate between the childhood and adulthood traumatic experiences. Fourth, all constructs in the current study were assessed using self-report measures and although commonly used in psychological literature, poor memory of childhood maltreatment has been evidenced before (Williams, 1994) and could possibly lead to inaccurate results. However, it has been reported that in psychotic patients, retrospective self-reporting of childhood sexual abuse remained consistent over 7 years, and had good convergent validity with clinical case notes (Fisher et al., 2013). Fifth, the sample was predominantly White and female, and generalizations to predominantly male samples or other racial backgrounds should, therefore, only be made with caution. The current study controlled for gender in all analyses; however, future studies may decide to employ techniques, such as moderated mediation, to further disentangle the effects of gender in this context. Sixth, the current investigation utilized a university student sample, which reduces the generalizability of the findings to other populations (Henrich, Heine, & Norenzayan, 2010). Replications with clinical and other nonclinical samples are warranted. Finally, the survey had a low response rate of 6%. The reason for this could be respondent fatigue, as the survey was advertised several weeks into the winter semester. Moreover, surveys advertised via emails and administered online are generally associated with lower response rates (Nulty, 2008). This, in turn, has implications for generalizing the results to all university students.
Conclusion
Despite limitations, the current study provides the first examination of the role of DT as a possible mediator of the relationship between childhood maltreatment and mental ill-health in adulthood. The results demonstrate that in a sample of university students from Northern Ireland, DT is a significant mediator of the relationship between childhood maltreatment and adult psychopathology. As such, the current study provides new insights into the relationship between childhood trauma and adult mental health by identifying DT as a possible risk and resilience factor in the well-established relationship. Further research in this area will be needed to provide more specific recommendations for intervention and prevention strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.