
Abstract
Posttraumatic stress disorder (PTSD) is a chronic, debilitating disorder that is associated with neural alterations in multiple brain regions. Neuroimaging studies have largely focused on gray matter abnormalities in PTSD, with less information known about the integrity of white matter tracts. Prior studies of brain white matter in PTSD have produced mixed results, likely due to differences in neuroimaging sequences and clinical variables. This study addressed this gap by examining the microstructural integrity of the corpus callosum, the largest white matter fiber bundle in the brain, using diffusion tensor imaging (DTI). Sixty adult females diagnosed with PTSD with a history of interpersonal violence were compared with 18 trauma-exposed controls. All participants underwent DTI using 1.5 T. MANOVA revealed significantly higher fractional anisotropy (FA; p = .012) in the genu of the corpus callosum (GCC) compared with the trauma-exposed controls. These results suggest the GCC to relate to PTSD symptomatology. Further studies of this mechanism may provide insight into improving treatment and prevention efforts.
Keywords
In studying a disorder with symptoms as heterogeneous as posttraumatic stress disorder (PTSD), considering underlying mechanisms is of particular importance. Neuroimaging offers a useful methodology to elucidate these mechanisms. Most neuroimaging research conducted on PTSD clusters has focused on gray matter, or unmyelinated neurons, examining both the activation and volume sizes of particular brain regions (O’Doherty, Chitty, Saddiqui, Bennett, & Lagopoulos, 2015; Saar-Ashkenazy et al., 2014; Villarreal et al., 2004; Woon, Sood, & Hedges, 2010). Within the PTSD literature, gray matter deficits have been connected to PTSD severity, altered fear extinction, emotion regulation, and cognitive deficits such as associative memory (O’Doherty et al., 2015; Saar-Ashkenazy et al., 2014).
While studying volume reduction and neural activation can provide useful information on brain circuitry within a disorder, they encompass only gray matter. Studying white matter (WM) tracts, which connect gray matter regions, is equally important. Namely, as interference in WM tracts can induce gray matter atrophy, findings related to WM tracts may provide insight into both the functionality and the efficiency of the brain. For example, WM abnormalities are related to loss in visuospatial ability (Muetzel et al., 2015), processing speed (Cremers et al., 2016; Hong et al., 2015), global cognition (Cremers et al., 2016; Marques, Soares, Magalhaes, Santos, Sousa, 2015), and executive functioning (Cremers et al., 2016). In addition, from a clinical psychology perspective, recent research on other psychiatric conditions has concluded that mental disorders (schizophrenia, Lee et al., 2013; bipolar disorder, Torgerson et al., 2013; depression, Zhu et al., 2011; PTSD, Sun et al., 2015) may be disruptive to WM, and thus, analyzing WM is necessary to fully understand the pathology, and thus treatment, of disorders such as PTSD.
Diffusion tensor imaging (DTI) measures the three-dimensional (3D) diffusion of water within the WM tracts of the brain in vivo (Alexander, Lee, Lazar, & Field, 2007; Mori & Zhang, 2006; Soares, Marques, Alves, & Sousa, 2013). Specifically, DTI depicts WM tractography by analyzing the speed and direction of water flow across the X, Y, and Z axes of brain regions. A 3D ellipsoid is formed, which allows researchers to depict and study the unidirectionality and efficiency of water flowing through WM tracts. Scalar metrics are then computed, which quantifies the unidirectionality of the diffusion. One traditional scalar metric is fractional anisotropy (FA), which ranges from 0 (isotropic diffusion) to 1 (anisotropic diffusion). FA is highly affected by myelination; the less myelinated a WM tract, the more available the intercellular space. With more space available, there is less unidirectional movement, which results in lower FA. The reverse is true as well; the more densely packed together the axons are, the more the diffusion of water is restricted and the greater the FA (Alexander et al., 2007; Feldman et al., 2014; Mori & Zhang, 2006; Soares et al., 2013). Few studies have examined WM tracks in an adult PTSD population.
Of the WM areas examined, the corpus callosum (CC) has been among the most well studied. The CC is a vital tract that connects the two cerebral hemispheres and enables interhemispheric communication. The CC is known to facilitate high-level cognitive functioning such as memory (Ahmed, Spottiswoode, Carey, Stein, & Seedat, 2012; Kaufman et al., 2003). Specifically, abnormalities in the CC have been connected to deficits in associative memory, likely through impaired hemispheric encoding/retrieval (Saar-Ashkenazy et al., 2014). In addition, the CC has been associated with the processing of emotional stimuli (Ahmed et al., 2012; Kaufman et al., 2003).
Decreased volume in the CC (Kaufman et al., 2003; Rinne-Albers, van der Wee, Lamers-Winkelman, & Vermeiren, 2013) has been consistently related to PTSD in studies of children and adolescents (Rinne-Albers et al., 2013; Saar-Ashkenazy et al., 2014; Teicher et al., 2003; Villarreal et al., 2004). However, one adolescent study showed an increase in CC volume when compared with a healthy control group (Ahmed, Ras, & Seedat, 2012). It has been speculated that CC integrity may be affected in PTSD via a preexisting diathesis factor, one in which genetic factors make individuals vulnerable to developing PTSD by negatively affecting the interhemispheric communication and multisensory processing of novel stimuli (Villarreal et al., 2004).
Only two studies to our knowledge have examined DTI indices of the CC in an adult PTSD sample. When examining the CC, studies typically divide the CC into three subareas: the genu (GCC), body (BCC), and splenium (SCC). Zhang et al. (2015) investigated 14 young adults with PTSD as a result of a coal mining accident and determined PTSD to be related to lower FA in the GCC compared with a healthy control group. In addition, Sun et al. (2015) studied 15 adult individuals who received DTI scans within 2 days of a motor vehicle accident (MVA) and met criteria for PTSD 6 months later. Consistent with the prior study, lower FA was shown specifically in the GCC in individuals with PTSD compared with a trauma-exposed sample (Sun et al., 2015). However, both of these studies were limited by small sample sizes. Moreover, both studies utilized samples in which the trauma involved an accident (MVA and coal mine explosion). As such, results may not be generalizable to other trauma types and/or may be confounded by brain injury.
This study attempts to address these gaps in the literature by examining the effects of interpersonal violence on CC integrity in women. To our knowledge, this is the first study to examine the effects of PTSD on WM exclusively as a result of an interpersonal trauma (sexual abuse, childhood abuse, sexual assault, domestic violence). Interpersonal trauma is common, especially among women (Breslau, 2002; Flett, Kazantzis, Long, MacDonald, & Millar, 2004), making this a relevant research population. As the first study examining this, replication studies are needed. The need is exacerbated by the use of Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) criteria, which was used to reflect the measures used in data collection.
Based on the results of the prior two studies (Sun et al., 2015; Zhang et al., 2015), we hypothesized that women who met DSM-IV-TR criteria for PTSD will display lower FA in the CC. Furthermore, because the CC is known to facilitate memory function (Saar-Ashkenazy et al., 2014) and affect emotional processing (Ahmed et al., 2012; Kaufman et al., 2003), we hypothesized that DTI abnormalities within the CC would correspond strongly to reexperiencing symptoms, as they consist of unwanted thoughts and memories of the traumatic event, including nightmares, flashbacks, and other upsetting memories (APA, 2000).
Method
Participants
Sixty right-handed women with a DSM-IV-TR diagnosis of PTSD resulting from an interpersonal trauma history were recruited via advertisements and consented to participate in the study. Right-handed individuals were chosen as handedness has been linked to brain lateralization; differences in lateralization could thus confound results. In addition, 18 right-handed women with an interpersonal trauma history, but no current or lifetime history of PTSD, were recruited as a trauma-exposed healthy control group. Comparing PTSD with a trauma-exposed control group allows for more accurate implications about the effects of PTSD (as opposed to trauma more generally) and correlates of resilience. Clinical and demographic information is reported in Table 1.
Participant Demographics.
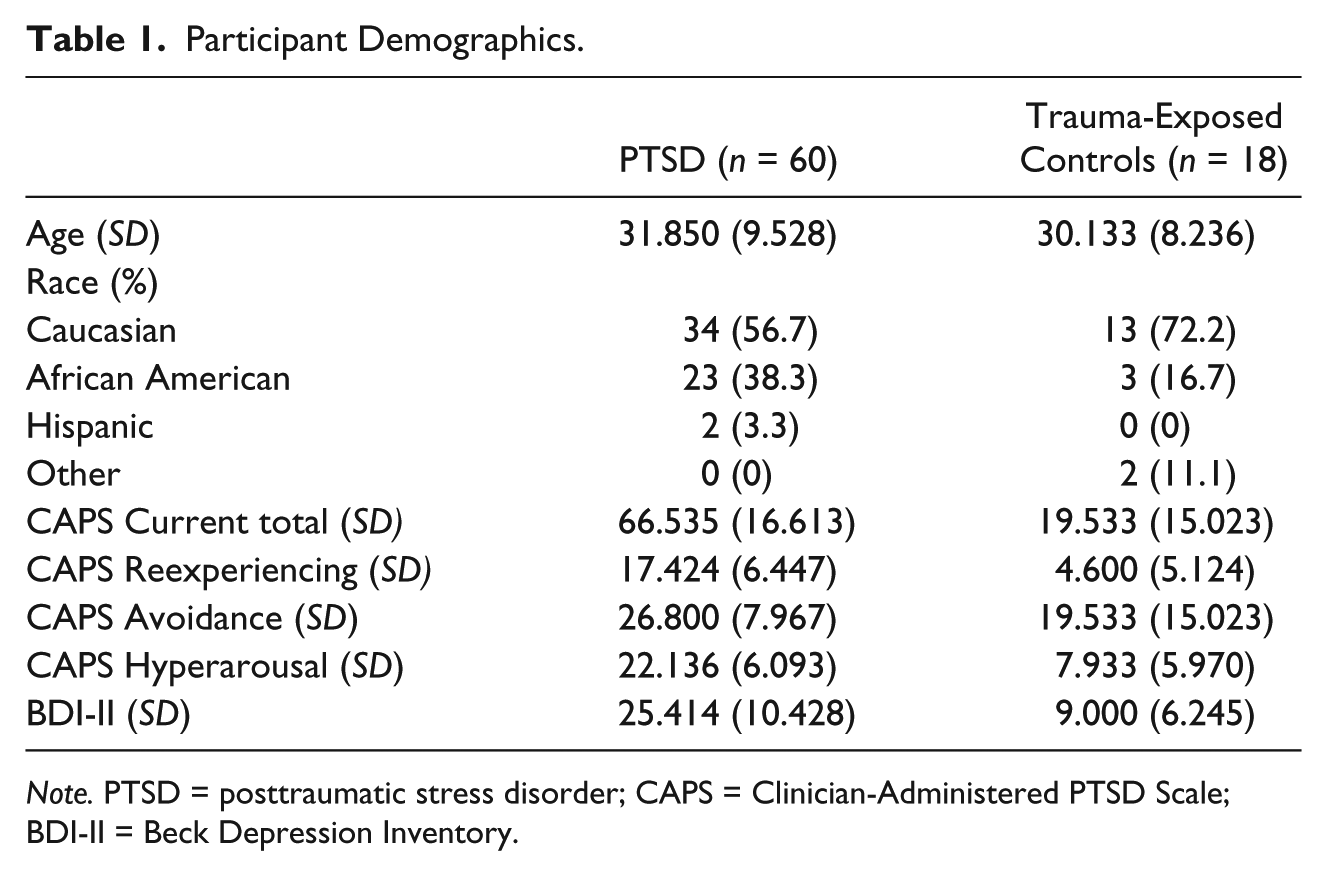
Note. PTSD = posttraumatic stress disorder; CAPS = Clinician-Administered PTSD Scale; BDI-II = Beck Depression Inventory.
Exclusion criteria consisted of (a) a diagnosis of a neurological disorder such as dementia, stroke, brain tumors, seizure disorder, multiple sclerosis, or encephalopathy Parkinson’s disease; (b) current comorbid alcohol or substance use disorder, schizophrenia or other psychotic disorder, obsessive-compulsive disorder (OCD), or bipolar disorder; (c) currently being administered with psychotropic drugs or drugs that affect the central nervous system (CNS) such as beta-blockers, mood stabilizers, antipsychotics, or other antidepressants; (d) active suicidal risk as assessed by the investigator; (e) significant cognitive limitations that may interfere with testing procedures; (f) history of head injuries; and (g) implanted devices (such as a pacemaker) or other metallic objects that are contraindicated for a magnetic resonance imaging (MRI). Participants provided written informed consent and were compensated for their time.
Measures
The Clinician-Administered PTSD Scale–IV (CAPS-IV; Blake et al., 1998; Blake et al., 1995) was used to assess DSM-IV-TR PTSD symptoms. The CAPS-IV is a 25-item semi-structured interview that examines both frequency and intensity of PTSD symptoms (0-4 scale). The CAPS-IV has high interrater reliability (.92-1.00 for frequency, .93-.98 for intensity; Hovens et al., 1994), test–retest reliability (.77-.96 for symptom clusters, .90-.98 for total score), and internal consistency (.85-.87 for symptom clusters, .94 for total score; Blake et al., 1995). Based on prior research (Orr et al., 1997), participants in the PTSD group must have had a CAPS score above 45 and should have met the original scoring criteria by Blake et al. (1995), indicating a PTSD symptom to be present if the frequency is rated as 1 or higher and the intensity is rated as 2 or higher.
For the purposes of covariates, depression was measured using the Beck Depression Inventory, Second Edition (BDI-II; Beck, Steer, & Brown, 1996). The BDI-II is a 21-item self-report instrument gauging the severity of symptoms of depression in the last 2 weeks as listed in DSM-IV-TR. Respondents answer using a 4-point scale ranging from 0 to 3. The BDI-II has shown high reliability and validity across populations (Y. P. Wang & Gorenstein, 2013). In addition, to measure anxiety symptoms, the Mood and Anxiety Symptom Questionnaire (MASQ) was utilized. Based on the tripartite model of affect, the MASQ is divided into three scales that measure depressive symptoms, anxious symptoms, and mixed symptoms. The MASQ demonstrates high sensitivity/specificity and clinical utility (Buckby, Yung, Cosgrave, & Killackey, 2007). In this study, to account for the covariate of anxiety, only the anxiety scale entitled anxious arousal was used.
Imaging Acquisition
A Siemens 3 T TrioTim MRI scanner (Erlangen, Germany) was used to collect DTI scans. First, participants received a T1 3D magnetization-prepared rapid gradient echo image (MP-RAGE). With a 1 × 1 × 1 resolution, the structural images were gathered using a sagittal 3D T1-weighted sequence with a repetition time (TR) of 2.4 s, an inversion time (TI) of 1,000 ms, a flip angle of 8°, and a time-to-echo (TE) of 3.13 ms. For DTI, the b value was set at 1,400 s/mm2 with an acquisition of a reference image (b = 0). One acquisition included 25 transverse slices, 25 directions, 2 mm thickness (no gap), and an in-plane resolution of 2 × 2 mm2. A second DTI scan was conducted for each participant to serve as a backup in the event of artifacts.
Image Analysis
T1 Images were first inspected for any obvious abnormalities (e.g., enlarged ventricles, cysts, tumors, hyperintensities) by an MRI technician. This study used a whole brain analysis, with imaging data preprocessed with FMRIB Software Library (FSL) to account for asynchronous slice acquisition and odd/even slice intensity differences from interleaving. Images were then corrected for spatial distortion using an eddy current correction (Friston, Williams, Howard, Frackowiak, & Turner, 1996; Snyder, 1996). A brain mask for the data was then produced to ensure that areas outside the scans were ignored. Finally, tensors were fitted using the generated brain mask.
Processing was done using the ENIGMA protocol, which is described elsewhere (Jahanshad et al., 2013) and is available online (http://enigma.ini.usc.edu/protocols/dti-protocols/). Briefly, the data were processed using FSL’s tract-based spatial statistics (TBSS; http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/TBSS) and were altered to show individual FA values on the hand-segmented ENIGMA-DTI skeleton mask. After extracting the skeletonized WM and projections of individual FA values, ENIGMA tract-wise regions of interest were transferred to extract the mean FA across the full skeleton and average FA values for the regions of interest (ROIs). ROIs included the three subareas of the CC: GCC, SCC, and BCC. Images were then examined again to ensure no artifacts or abnormalities.
Statistical Analysis
Extracted mean FA values were exported into IBM SPSS Statistics 21.0 for analysis (SPSS, Inc., Chicago, IL). First, CC subarea and PTSD data were screened; outliers were checked for with z scores and normality with the Shapiro–Wilk Test and Levene’s test of homogeneity of variance. Differences in CC white matter integrity (WMI) between the PTSD group and trauma-exposed control group were investigated using MANOVA. Between-subject effects were examined to determine which specific subarea was significantly related to trauma symptoms, with Cohen’s d used to measure effect size. To identify any potential covariates, correlations were conducted between each CC subarea and age, race, education, depression symptoms, and anxiety symptoms. Covariates were screened for linearity using group scatter plots, for homoscedasticity by plotting standardized residuals, and for homogeneity of regression slopes. If necessary, MANCOVA was then conducted with previously identified significant covariates (p < .005) included. Between-subject effects were examined.
Regression analyses were then conducted between overall/symptom cluster PTSD severity for the total sample and any significant CC areas to identify the relationship between PTSD symptom clusters and CC WMI. Two separate regressions were conducted, one with overall PTSD symptom severity and another with the three symptom clusters, to avoid issues of multicollinearity. A Bonferroni correction was applied to account for multiple testing, and a new significance threshold was established (.05/4 = .0125).
Results
Table 2 shows FA values for the whole CC and the three subareas by group. MANCOVA was not significant (p = .171), indicating that the PTSD and trauma-exposed groups did not differ significantly when considering all three subareas as a whole. When examining by subarea, unadjusted between-subjects analyses revealed significantly higher FA in the GCC—F(1, 76) = 4.340, p = .041; effect size of .56; Cohen, 1988—in the PTSD group. FA in the SCC and BCC in the PTSD group were not significantly different from the trauma-exposed controls. Testing for potential covariates, age was significantly related to GCC FA scores (r = −.283, p = .012). Race, education, depression symptoms, and anxiety symptoms were not related to FA scores. Following adjusted analyses (age), the significant effect of group on GCC FA scores, F(2, 75) = 6.061, p = .004, remained. Age was significantly related to GCC FA scores, F(1, 75) = 7.416, p = .008, such that FA scores decreased with increasing age.
Corpus Callosum FA values.

Note. FA = fractional anisotropy; PTSD = posttraumatic stress disorder.
Significant difference between groups (p < .05)
Examination of PTSD severity using a regression indicated that PTSD severity was not related to FA in the GCC. Reexperiencing symptoms was positively related to FA in the GCC (b = .358, p = .034). However, the results were no longer statistically significant after correcting for multiple comparisons.
Discussion
This study examined whether adult women with PTSD showed abnormal WMI in the CC compared with trauma-exposed controls. This is the first study to our knowledge to examine the effects of PTSD on WM exclusively as a result of an interpersonal trauma (sexual abuse, childhood abuse, sexual assault, domestic violence), an important gap to fill due to the high prevalence and severity of interpersonal trauma. Namely, interpersonal trauma is common, especially among women (Breslau, 2002; Flett et al., 2004) and people with severe mental illness (Mauritz, Goossens, Draijer, & van Achterberg, 2013). Furthermore, interpersonal traumas are strongly linked to PTSD (Nishith, Mechanic, & Resick, 2000), more so than noninterpersonal traumas (Breslau, 2002; Luthra et al., 2009).
Our finding of higher FA in the GCC (rather than lower FA) in women with PTSD was inconsistent with our hypothesis. The medium effect size (Cohen’s d = 0.56) reinforces this finding. It is important to recognize that, although lower levels of FA are typically thought of as represented of dysfunction, abnormal levels in either direction can indicate dysfunction depending on the brain region (Soares et al., 2013). This could be due to the limited number of DTI studies examining PTSD. Specifically, there are few DTI studies examining the CC in PTSD, and those studies that have been conducted are limited by small sample sizes. Furthermore, studies of gray matter have also resulted in divergent findings, as both smaller (Rinne-Albers et al., 2013; Teicher et al., 2003) and larger (Ahmed et al., 2012) CC volumes have been associated with PTSD. Finally, prior DTI research of other brain regions has shown conflicting results, as some studies have found lower FA in the cingulum (Fani et al., 2012; M. J. Kim et al., 2005; S. J. Kim et al., 2007; H. H. Wang et al., 2010) to relate to PTSD, while other investigators have found higher FA in the cingulum (Abe et al., 2006; Kennis et al., 2015).
Results from the current study may also have differing results due to differences in the sample compared with prior research. This study is the first to our knowledge of WM to exclusively study PTSD as a result of an interpersonal trauma. As mentioned, trauma type in PTSD research has shown significant differences with respect to varying PTSD symptoms and severity (Haldane & Nickerson, 2016; Wanklyn et al., 2016). As such, trauma type may affect the neural presentation, and results may not be consistent with prior studies focused on natural disasters (Li et al., 2016; H. H. Wang et al., 2010), combat (Costanzo et al., 2016; Schuff et al., 2011), or a combination of trauma types (Fani et al., 2012). In addition, this sample also consisted entirely of women. Sex has been shown to be predictive of differences in the presentation of PTSD (Rinne-Albers et al., 2013). This is especially relevant because of the two previous adult studies of the CC in PTSD, one (Sun et al., 2015) used an all-male sample. In addition, of the two previous DTI studies that have examined the CC, one featured a sample with DTI acquisition occurring within 2 days of trauma exposure (Sun et al., 2015), while the other compared PTSD victims with nontraumatized healthy controls (Zhang et al., 2015). Time since trauma as well as different comparison groups (trauma-exposed vs. no history of trauma) may affect brain signatures. Thus, the scantiness of the literature and uniqueness of our sample may have contributed to differences from prior studies.
As GCC FA scores decreased with increasing age, results from the current study also suggest the relationship between GCC FA and PTSD symptomatology may be less apparent in older age. This aligns with previous research which suggests that findings from the CC may be largely age-dependent (Zhang et al., 2015), as the CC has been observed to develop in the mid-20s (Pujol, Vendrell, Junqué, Martí-Vilaltra, & Capdevila, 1993). Furthermore, the GCC has also been associated with decreasing FA in normal aging, and thus, this finding may be a normal effect above and beyond PTSD (Abe et al., 2002).
Combined together, these results suggest that the GCC may be of particular interest in the etiology, prevention, and treatment of PTSD. Future research should connect other possible PTSD etiological factors such as disruptions in fear circuitry (Keding & Herringa, 2015; Shin & Handwerger, 2009) and hypothalamic–pituitary–adrenal axis (Kuhlman, Vargas, Geiss, & Lopez-Duran, 2015; Mehta & Binder, 2012) to WMI in the GCC to better understand PTSD mechanisms. Furthermore, with the inclusion of a trauma-exposed control group, results suggest the GCC may be an important area to investigate resilience when exposed to a traumatic event. The literature surrounding trauma resilience has largely not bridged translational findings to behavior components known to relate to resilience, such as positive affectivity, cognitive flexibility, religious coping, social support, emotion regulation, and self-efficacy (Yehuda, Flory, Southwick, & Charney, 2006). Future research should explore what factors, both biological and behavioral, may influence the vulnerability of WMI changes in the GCC. Finally, the WMI of the GCC may be an important area to examine treatment efficacy. Future studies should examine the changes that occur in the GCC over psychological or pharmacological treatment or how WMI in the GCC relates to treatment outcome.
Although this study has important implications for future research, it is not without limitations. This study was restricted to women, and as such, results cannot be generalized to men. Furthermore, while comparing with a trauma-unexposed group allowed for useful implications about resilience, this study lacks a trauma-unexposed group. This limits implications as they relate to the effects of trauma more generally. In addition, while this study provides value in studying interpersonal violence, it does not distinguish between various types of interpersonal trauma (sexual abuse, childhood abuse, sexual assault, domestic violence). Similarly, this study does not have access to time since last trauma, which may be informative to neural developmental trajectories. Future studies should study these types more specifically. Finally, this study used Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) criteria, and results may not fully reflect a sample with a PTSD diagnosis from Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). Thus, these results are a preliminary step in understanding a complicated research area, with replication studies necessary to provide further generalizability to diverse populations.
Despite these limitations, this study suggests a relationship between the WMI of the GCC and PTSD symptoms in women victimized by interpersonal violence, with these changes lessening apparently at older age. Future studies should examine the association between the GCC and PTSD etiology and maintenance. In addition, future studies should investigate how the GCC is affected by psychological and pharmaceutical intervention, as this may direct prevention and treatment efforts.
Footnotes
Authors’ Note
Robert Paul is also affiliated with University of Missouri–St. Louis, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.