
Abstract
IMPACT, an online, interactive, capacity-building intervention for professionals engaged in direct intimate partner violence (IPV) work, was evaluated for preliminary efficacy. The IMPACT intervention comprised 13 training modules developed using the Rotheram-Borus Common Factors approach to prevention program development. In total, 156 participants from a diverse range of organizational settings across the United States completed baseline assessments and were randomized to the IMPACT intervention or to the control condition. Participants completed a follow-up assessment 3 months after baseline. Compared with control participants, IMPACT participants significantly increased their general IPV-related knowledge and their self-efficacy to utilize best practice IPV prevention strategies; effect sizes for these outcomes were moderate to large, indicating that these results are meaningful for IPV prevention practice. No differences by condition were observed in other outcomes such as scenario-based skills implementation or utilization of IPV-related strategies in participants’ work. In addition, analyses showed that these findings were consistent across IPV prevention experience levels. Results suggest that IMPACT is flexible, generalizable, scalable, and a promising tool for disseminating IPV research into practice and helping to prevent IPV.
Introduction
Intimate partner violence (IPV), defined as physical, sexual, or psychological harm committed by a current or former intimate partner or spouse (Centers for Disease Control and Prevention [CDC], 2008), is a significant public health problem in the United States. Data from the 2010-2012 National Intimate Partner and Sexual Violence Survey indicates that approximately 27% of women and 11% of men have experienced sexual or physical violence or stalking by an intimate partner at some point in their lifetime (Smith et al., 2017); half of all men and women in the United States have experienced psychological aggression from an intimate partner (Black et al., 2011). In addition to the direct physical injuries suffered by IPV survivors, individuals who have experienced IPV are at increased risk for a range of adverse health outcomes (Black, 2011; Breiding, Black, & Ryan, 2008; Crofford, 2007; Leserman & Drossman, 2007). IPV is associated with psychological consequences, including anxiety, depression, posttraumatic stress, and suicidal ideation (Black, 2011; Warshaw, Brashler, & Gil, 2009). In addition, IPV survivors are at increased risk for negative social outcomes, including homelessness and social isolation (Heise & Garcia-Moreno, 2002; Plichta, 2004), and female survivors are more likely to engage in a variety of risk behaviors, including risky sexual behavior, substance abuse, and unhealthy diet-related behaviors (Roberts, Auinger, & Klein, 2005; Roberts, Klein, & Fisher, 2003; Silverman, Raj, Mucci, & Hathaway, 2001).
Since 2003, researchers and legislators have become increasingly focused not only on responding to IPV when it occurs, but also preventing IPV before it happens (National Center for Injury Prevention and Control, 2003). This shift in approach has been reinforced recently by the Affordable Care Act, which mandates insurance coverage for IPV screening and treatment services (Curry et al., 2018). Much is known about the etiology of IPV, and researchers have increasingly begun to target risk and protective factors in prevention programs (Knox, Lomonaco, & Alpert, 2009; Langhinrichsen-Rohlin & Capaldi, 2012; Martin et al., 2009; Whitaker et al., 2013). The CDC (2008) has identified community capacity building for the implementation of evidence-based primary prevention programs and policies as a key priority for IPV prevention.
IPV practitioners, including public health nurses, community education workers, IPV shelter staff, police officers, and social workers, are ideally positioned to put evidence-based IPV prevention programming into practice. Indeed, these frontline IPV professionals express the desire to learn more about how to identify, implement, and evaluate primary IPV prevention programs (Martin et al., 2009). However, they report receiving only cursory or no training in the underlying principles of prevention, the components of evidence-based prevention programs, and how to culturally adapt programs to their populations (Martin et al., 2009; Whitaker et al., 2007). A lack of training in cultural adaptation is especially troubling because IPV is not experienced homogenously, either within or across populations. Appropriate capacity-building tools need to provide practitioners with population-specific adaption tools, as well as training in how to tailor prevention programming to a specific individual’s needs (Lee, Sanders Thompson, & Mechanic, 2002). In addition, the majority of capacity-building tools developed for IPV practitioners have targeted medical professionals (e.g., residents, orthopedic surgeons, nurses), which does not reflect the broad array of professionals who do—or could do, with the right training—IPV prevention work (Sawyer, Coles, Williams, & Williams, 2016). Clearly, there is currently a critical need in the IPV prevention community for interventions that effectively disseminate what the research community has learned about IPV prevention to frontline IPV prevention professionals.
The dissemination of IPV prevention programming can be made more effective and efficient by utilizing methods that aim to identify components, principles, and strategies that are common across multiple evidence-based programs. This approach has been used across many fields, including HIV (Rotheram-Borus et al., 2009) and mental health challenge (Kidd, Davidson, & McKenzie, 2017) prevention. The Rotheram-Borus et al. (2009) Common Factors model identifies the key factors of HIV prevention programming that are associated with positive outcomes. Applied to IPV prevention, the model can help to identify key evidence-based best practices, using a social-ecological framework that grounds IPV in individual, community, and structural contexts (Cohen, Scribner, & Farley, 2000; Green, Richard, & Potvin, 1996) as well as core public health principles. The Common Factors model includes the following five factors: (a) uses an established framework to understand behavior change; (b) conveys information specific to particular issues or subpopulations; (c) builds cognitive, affective, and behavioral skills; (d) addresses structural barriers to behavior change; and (e) provides social support or tools to develop support to change behavior. This model can help to delineate the necessary components of effective IPV prevention programming. These necessary components can then be used to train IPV practitioners in cross-cutting, effective skills and strategies, rather than trying to teach them multiple evidence-based programs one-by-one, which is often prohibitive in terms of both cost and time resources.
An additional way to maximize efficiency in dissemination is to use online platforms to teach IPV prevention common factors. While in-person trainings are still widely used in IPV prevention, web-based capacity-building products can be effective education tools (Harris et al., 2002; Short, Suprenant, & Harris, 2006; Zaher, Keough, & Ratnapalan, 2014) that are easily accessible, self-paced, and readily distributed to a wider group of IPV practitioners, across geographical areas and professional affiliations.
Few, if any, programs have been developed to build primary and secondary prevention capacity among the broad array of IPV practitioners. The goal of this study was to evaluate whether IMPACT, a multimedia, interactive, online training program for IPV practitioners, increased IPV-related knowledge, skills, and effective behavior. Programs that build practitioner capacity to identify and implement IPV-related best practices and strategies, delivered online, have the potential to increase critical skills among significant numbers of practitioners and thereby prevent IPV among the many clients, patients, and students with whom practitioners interact.
Method
Participants and Setting
IPV prevention professionals in the United States who were actively involved in direct prevention work were recruited via email between February and May 2017. Professionals were eligible for the study if they met the following criteria: (a) living in the United States; (b) 18 years (19 in Alabama) or older; (c) currently working in IPV prevention, directly with clients, patients, or students (outside of a degree program) at least once per week; (d) working in direct IPV prevention for at least 3 months; (e) regular access to a computer and the Internet; (f) planning to work in direct IPV prevention for at least the next 3 months. To reach a wide range of IPV prevention professionals, “IPV prevention” was broadly defined, including IPV prevention work in counseling, legal work, medical care, shelter work, and school-based prevention programming, provided that the work was directly with clients, patients, or students. Participants in the study were living and employed in 18 different states, comprising all major geographic areas in the United States. Participants completed all study-related procedures via phone or online, from their home or place of employment.
Procedures
All study procedures were approved by the Sociometrics Corporation Institutional Review Board. Study staff reached out via phone and email to all 51 state-level domestic violence and sexual assault coalitions in the United States for assistance with recruiting IPV prevention professionals. Coalitions that agreed to assist with recruitment emailed a brief description of the study, including study staff contact information, to their member organizations. Interested IPV prevention professionals contacted study staff by email. Study staff then spoke with potential participants by phone to determine their eligibility to enroll in the study. During the screening phone call, study staff asked interested individuals about the nature and scope of their work, to ensure that they were currently engaged in direct IPV prevention work (at primary, secondary, or tertiary levels of prevention) with clients, patients, or students. Individuals who met eligibility criteria provided written informed consent. Participants were recruited until enrollment goals were met, at which point they completed a baseline assessment.
After completing the baseline assessment, participants were randomly assigned to the experimental intervention condition (IMPACT), or the standard training control condition (CONTROL). Participants in the IMPACT condition submitted feedback surveys following their completion of each intervention component. Participants in both conditions completed a follow-up assessment 3 months after baseline.
Demographic characteristics, work status (baseline only), and knowledge, skills, and behavioral constructs (baseline and 3-month follow-up) were measured using an online survey, administered via SurveyMonkey. Participants completed these assessments in approximately 45 to 60 minutes, and IMPACT intervention condition participants completed feedback surveys in approximately 5 to 10 minutes. Participants who completed the baseline assessment were compensated US$100; those who completed the 3-month follow-up assessment were compensated US$150. IMPACT intervention condition participants who completed all intervention components and feedback surveys were compensated an additional US$150.
Figure 1 shows the flow of participants through the study: a total of 187 IPV prevention professionals were screened for eligibility; 164 of those met eligibility criteria to participate. Of the eligible professionals, 156 (95%) provided informed consent, enrolled in the study, completed baseline, and were randomly assigned to either the IMPACT intervention or CONTROL condition. Preliminary analyses showed no significant difference by study condition in the percentage of participants lost to follow-up. In addition, compared with retained participants, participants who were lost to follow-up did not significantly differ by study condition on any of the baseline study measures (demographic factors and knowledge, skills, and behaviors).

Flow of participants through the study.
Study Conditions
The IMPACT intervention content was developed using a multistep process centered on the goal of discerning a set of evidence-based best practices from the fields of public health and IPV prevention. Throughout, the process was informed by the Common Factors model (Rotheram-Borus et al., 2009) for prevention program development. The first step involved an extensive literature review to identify evidence-based IPV prevention interventions, using a strict set of selection criteria (e.g., theory-based program, rigorous evaluation methods, desirable behavioral outcomes). The second step involved reviewing selected evidence-based programs and creating a framework of factors (e.g., theoretical model used, information conveyed, skills taught, method of teaching utilized) that were common to many, if not all, of the programs. In the third step, this framework was presented to a scientific panel of experts in the field of IPV. The panel recommended a final set of common factors, or themes, based on their expertise and the strength of the supporting evidence. These factors were used as the organizing foundation for developing the IMPACT intervention. A detailed description of the IMPACT intervention, and its development through formative research and prototype feasibility studies, is described elsewhere (Drabkin et al., in prep.).
The IMPACT intervention consists of 13 multimedia, online training modules. Each module comprises a video as well as one or more handouts, factsheets, exercises, and other interactive tools. The module videos range in length from approximately 15 to 30 minutes. The modules were designed to increase the capacity of IPV prevention professionals who work in a variety of different roles (e.g., peer counselors, therapists, shelter staff, medical advocates, prevention educators) to effectively implement evidence-based IPV prevention programs. The goal of the modules is to increase IPV prevention professionals’ knowledge and skills, leading to changes in their prevention-related behavior; the modules contain evidence-based information, examples from IPV prevention interventions that have been proven effective, and live skills demonstrations. The modules were developed to be easily accessible online, via smartphone, computer, or tablet, on IPV professionals’ own time, at their own pace.
IMPACT modules fall into two general categories: modules designed for use by all IPV professionals (seven modules), and modules designed for use by IPV professionals who work with specific populations (six modules). Table 1 shows the IMPACT module titles in each category. To emulate IPV prevention professionals’ real-world continuing education needs and practices, the study team assigned all intervention participants to complete the seven modules designed for all professionals; the study team also assigned participants to complete other modules that were relevant to the populations that they were working with at the time of enrollment in the study (one to six modules). Participants had the option to review other modules to which they were not specifically assigned, if they so chose; participants only provided feedback about the modules to which they were assigned. While study staff verified that participants logged in to view the modules, it is not known how long participants spent viewing each of their assigned modules.
IMPACT Intervention Module Titles, by Category.
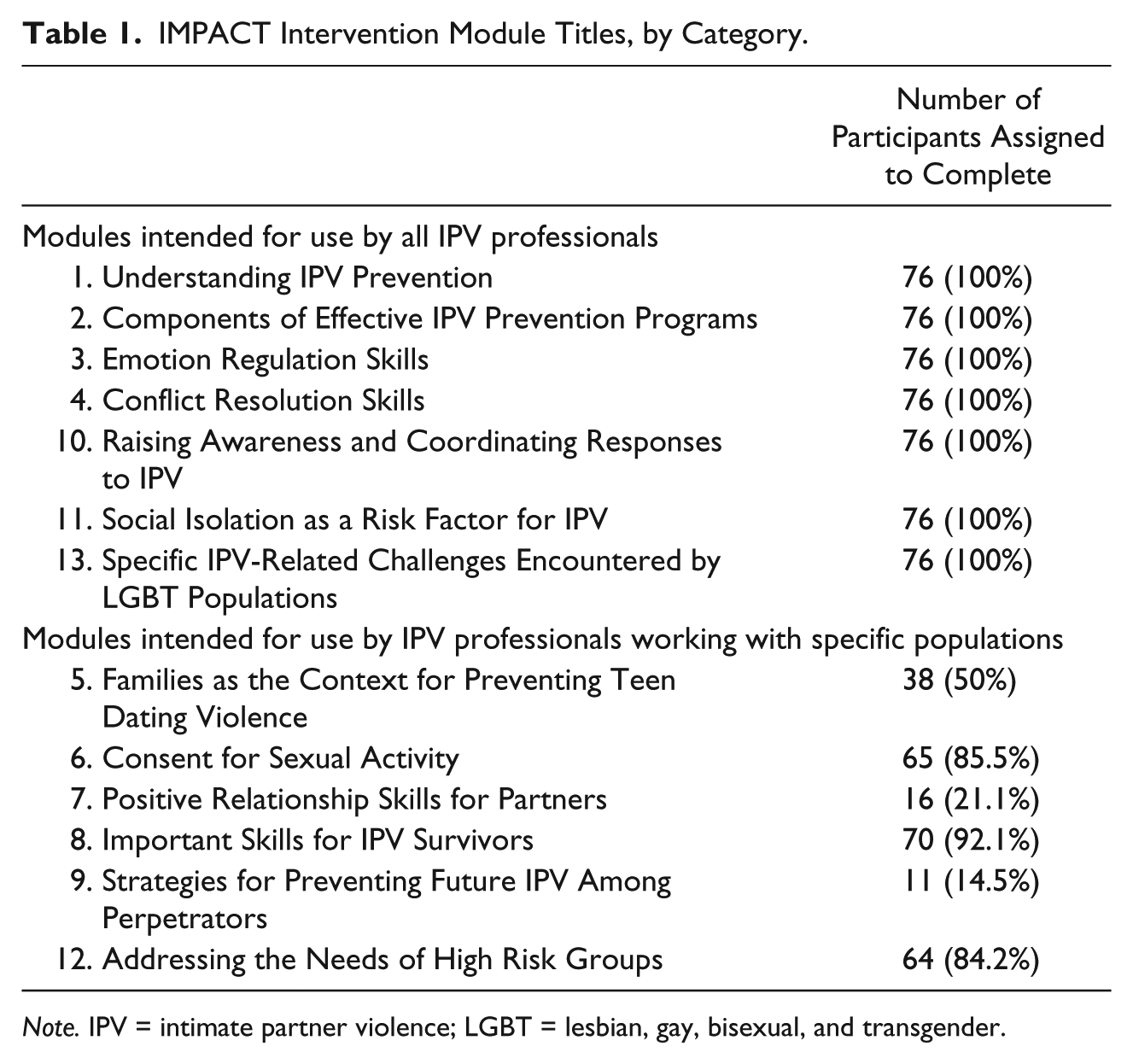
Note. IPV = intimate partner violence; LGBT = lesbian, gay, bisexual, and transgender.
Intervention condition participants were given access to the modules online for a period of 5 weeks after baseline survey completion. Participants varied in the amount of time spent completing intervention tasks. Participants filled out a table to track their completion of their assigned modules, and the modules’ corresponding feedback surveys. Participants’ completion rate of the intervention components was high, with 72 (95%) completing all of their assigned intervention components, one (1%) completing at least one intervention component but not all assigned components, and three (4%) completing no intervention components. Following an intent-to-treat analysis of the outcomes, participants were retained in the study without regard for intervention exposure.
The CONTROL condition did not receive any intervention as part of the study. However, participants in both the IMPACT and CONTROL conditions were free to participate in any IPV-related trainings offered by their own, or by other, organizations.
Measures
Demographic and work characteristics
During the screening assessment, two demographic and work status variables were measured: age and length of time (number of years) worked in direct IPV prevention. Length of time worked in direct IPV prevention was dichotomized (≤ 3 years, > 3 years) and also examined continuously. At the baseline assessment, several additional demographic and work status variables were measured, including gender identity (male, female, other-specified), race/ethnicity, educational attainment, name of the organization currently employing participant to do IPV prevention work (dummy coded), type of employing organization, and size of employing organization (number of employees).
Intervention usability
Intervention group participants provided feedback about the usability of the intervention by completing a series of nine questions regarding their thoughts about, and experiences with each of the IMPACT modules (e.g., “Viewing IMPACT module 12 will be beneficial to me professionally,” “I found IMPACT module 12 to be engaging,” and “How likely are you to recommend IMPACT module 12 to a professional colleague?”). Usability questions were developed based on user experience design principles to assess participants’ perceptions of the modules. After completing each of their assigned intervention modules, IMPACT participants rated their responses on 5-point Likert-type scales appropriate to each question (e.g., “1 = strongly disagree to 5 = strongly agree,” “1 = very unlikely to 5 = very likely”). A mean score was calculated, averaging both within the questions for each intervention module, and across all modules; higher values indicated greater intervention usability (alpha = 0.88).
IPV-related knowledge
At both baseline and 3-month follow-up, participants answered a series of questions that evaluated their knowledge of IPV prevention-related topics. These questions were developed in consultation with the Scientist Expert Panel that helped select and refine the content for the IMPACT modules. Questions were designed to map onto the key domains covered by the IMPACT modules, including general IPV and public health prevention knowledge, as well as population-specific knowledge (e.g., IPV prevention work with youth). The questions asked in the current study were pilot tested with 23 IPV prevention professionals; pilot testing resulted in five to six questions corresponding to each of the IMPACT modules, with questions retained for the current study based on Cronbach’s alphas and item-total correlations. All participants completed a set of general knowledge questions (e.g., “Which of the following is true about IPV in lesbian, gay, bisexual, and transgender [LGBT] vs. heterosexual relationships?” “Which of the following are examples of community-level risk factors for IPV?” and “The law enforcement approach typically involves strategies at what level of prevention?”). Participants also answered questions specific to the populations they were working with at the time of enrollment in the study (e.g., “It is usually obvious when a person feels coerced into sexual activity,” “A Safety Plan for female IPV survivors should include which of the following components:,” and “It is more effective to work directly with teens to prevent dating violence, rather than with their caregivers.”). Questions followed either a True/False or multiple-choice format. A General Knowledge score and a Specific Knowledge score were computed for each participant, by taking the percentage of correct responses participants gave relative to all the general and population-specific knowledge questions, respectively.
IPV-related skills
At both baseline and 3-month follow-up, participants’ ability to apply specific IPV prevention-related skills were measured by two types of questions. The first type asked participants to report how confident they felt to implement a particular skill (e.g., “How confident do you feel in your ability to teach caregivers specific communication strategies to talk effectively with their teens about dating?”); participants rated how confident they felt on a scale from 0% to 100%. In the second type of question, participants were presented with a brief IPV-related scenario and then asked what the appropriate approach for the prevention professional would be in that situation (multiple-choice response format).
All participants completed a set of general skills questions, as well as skills questions specific to the populations they were working with at the time of enrollment in the study. Two sets of scores were calculated for all participants. The first set comprised a General IPV Skills Self-Efficacy score, calculated by taking the mean of all participants’ confidence on general IPV prevention-related skills responses (alpha = 0.89; range = 34%-96%); and a General Skills Implementation score, calculated by taking the percentage of correct responses participants gave relative to all the general skills implementation questions. The second set comprised a Specific IPV Skills Self-Efficacy score, and a Specific Skills Implementation score. The Specific Skills Self-Efficacy score was calculated by taking the mean of all participants’ confidence on population-specific IPV prevention-related skills responses (alpha = 0.87; range = 42%-100%). The Specific Skills Implementation score was calculated by taking the percentage of correct responses participants gave relative to all the population-specific skills implementation questions.
IPV prevention-related behavior
At both baseline and 3-month follow-up, participants were asked a series of questions about whether or not they had used specific evidence-based IPV prevention strategies in their work over the previous 3 months (Yes or No). Participants were asked to report on their use of both general IPV prevention-related strategies (e.g., “Did you teach people an effective emotion regulation strategy?” “Did you teach people any key skills they need to positively resolve a conflict?”) and population-specific strategies (e.g., “Did you use any techniques to help survivors identify and challenge negative automatic thoughts?” “Did you use any motivational interviewing techniques to help perpetrators engage in IPV prevention work?”). Two scores were calculated for participants. A General IPV Behavior score was calculated by taking the percentage of “yes” responses participants gave to general IPV prevention-related strategy use questions, and a Specific IPV Behavior score was calculated by taking the percentage of “yes” responses participants gave, relative to all population-specific strategy use questions.
For all calculated scores, a higher score indicated greater or better IPV-related knowledge, skills, and behavior.
Analysis
Descriptive analyses were conducted to examine the baseline characteristics of the total sample and by study condition. The two study conditions were compared based on demographic factors, work characteristics, and outcomes variables of interest. Wald chi-square tests were used to compare categorical variables; t tests were used to compare continuous variables. To determine whether the dropout rate differed by study condition or by baseline outcome variables, a two-sample test of equal proportions was calculated; no differences were found.
To assess change in the knowledge, skills, and behavioral outcomes by condition, we employed multilevel modeling using the MIXED procedure in SPSS (IBM Corporation, Chicago, IL). Multilevel modeling accounts for multiple sources of nonindependence in the data (i.e., longitudinal data, with participants assessed at multiple time points; multiple outcome variables assessed for each participant; multiple participants employed at the same organization). Within this framework, separate models were fit to test whether study condition predicted each of the outcome variables of interest, with participants (Level 1) nested within organizations (Level 2), and models specified to account for repeated measures on participants over time. This method uses full information maximum likelihood estimation on all the data available for each participant; all randomized participants’ data were included, regardless of the number of assessments that were completed. Loss to follow-up was the only source of missing data, as all participants who completed baseline and 3-month follow-up answered all questions. While recruitment methods were not designed to enroll a certain number of participants from the same organizations, multiple practitioners employed by the same organizations did participate (study staff capped the number of participants from each organization at 5, to limit cross-contamination). Analytic methods therefore included participants’ employing organization as a Level 2 variable, to account for the possibility that participants from the same organization had more similar IPV-related knowledge, skills, and behavior than participants from different organizations (i.e., nonindependence).
Separate longitudinal models were fit for each of the eight knowledge (two dependent variables), skills (four dependent variables), and behavior (two dependent variables) outcomes. Each model contained three independent variables: (a) assessment point, with baseline as the reference; (b) intervention condition; and (c) a time by condition interaction term. To examine moderation of any observed effect of the intervention on the outcome variables, models also included interaction terms between study condition and number of years worked in IPV prevention (dichotomized to 3 years or less, or > 3 years).
Results
Sample Characteristics at Baseline
At baseline, there were no statistically significant differences by study condition in demographic characteristics or IPV-related knowledge, skills, and behavior (see Table 2). The mean age of the sample was 35.7 (SD = 10.7). Most of the sample was female (89.7%), White (80.8%), and had achieved a higher education degree (92.3%). More than a third (41.0%) of the sample reported having worked in direct IPV prevention for 3 years or less. Most participants (60.3%) were employed by moderately sized (11-50 employees) organizations to do IPV prevention work. Participants reported doing IPV prevention work in a variety of different settings (e.g., general social service agency, hospital, high school, police department, mental health–focused agency, IPV shelter), with nearly all (95.2%) working in multiple settings.
Demographic Characteristics and IPV-Related Knowledge, Skills, and Behavior of the Sample at Baseline, by Study Condition.
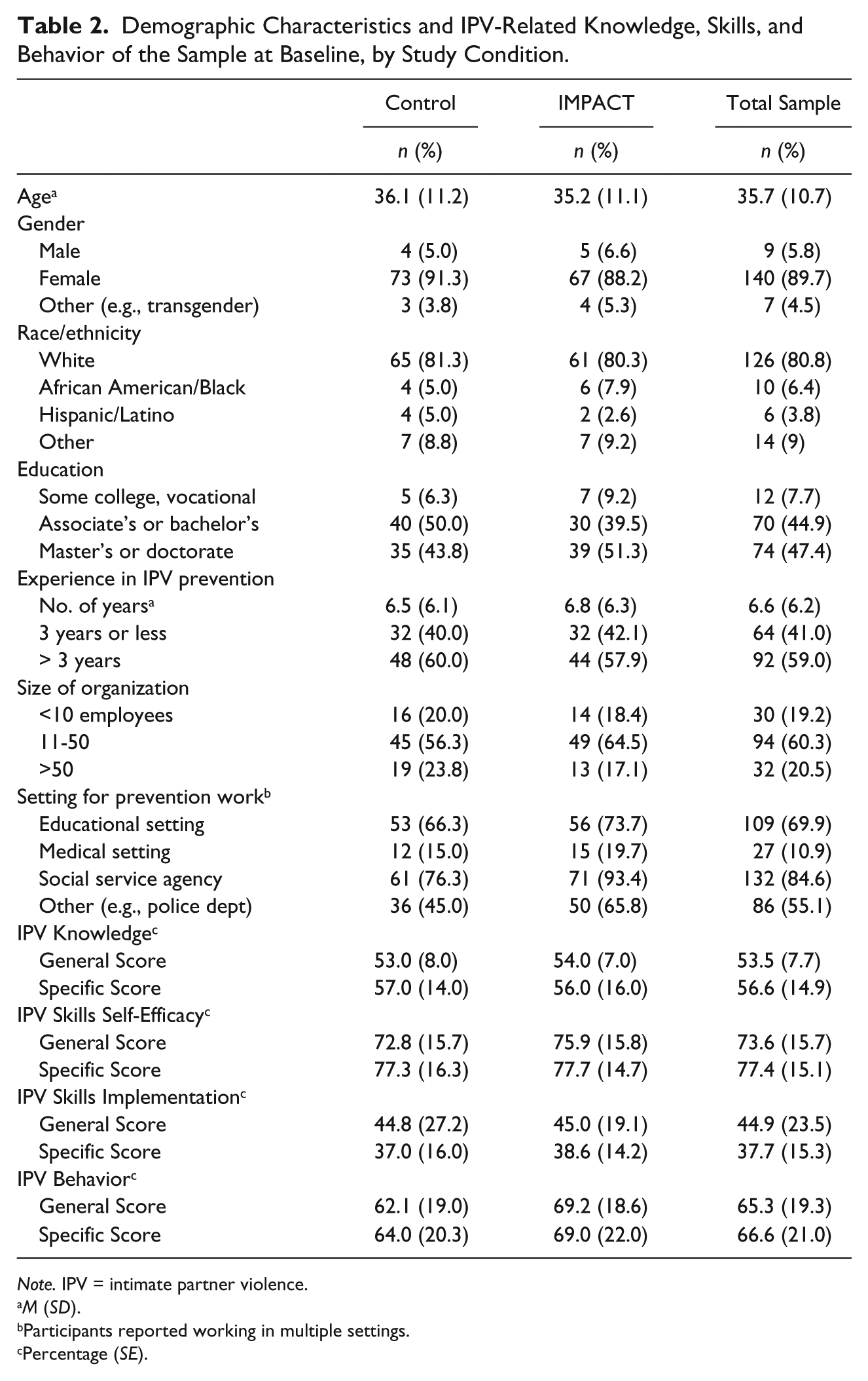
Note. IPV = intimate partner violence.
M (SD).
Participants reported working in multiple settings.
Percentage (SE).
Participants demonstrated a moderate level of both general and population-specific IPV-related knowledge at baseline (53.5% and 56.6% correct responses on the General and Specific Knowledge Scores, respectively). Participants felt quite confident in their ability to use both general and population-specific best practice strategies in their IPV prevention work (73.6% and 77.4% confidence on the General and Specific Skills Self-Efficacy Scores, respectively). They showed moderate ability to apply general IPV-related best practice strategies to real-world scenarios (44.9% correct responses on the General Skills Implementation Score), and moderately low ability to apply population-specific best practice strategies (37.7% correct responses on the Specific Skills Implementation Score). Participants reported having used a moderate number of best practice strategies in their IPV prevention work in the 3 months prior to baseline (65.3% and 66.6% of queried general and population-specific strategies, respectively).
Intervention Usability
Almost all (95.0%) intervention participants completed feedback surveys for all of their assigned training modules. The mean feedback scores for each intervention training module, and for the modules as a whole, are presented in Table 3. In general, feedback from participants was positive, with a mean score for all training modules combined of 3.9 (SD = 0.8) out of a possible 5.0 (for the highest level of usability). Intervention training module usability was very similar for the groups of general and population-specific training modules (M = 3.8 and 3.9, respectively).
Participant Feedback Scores for Intervention Training Modules.
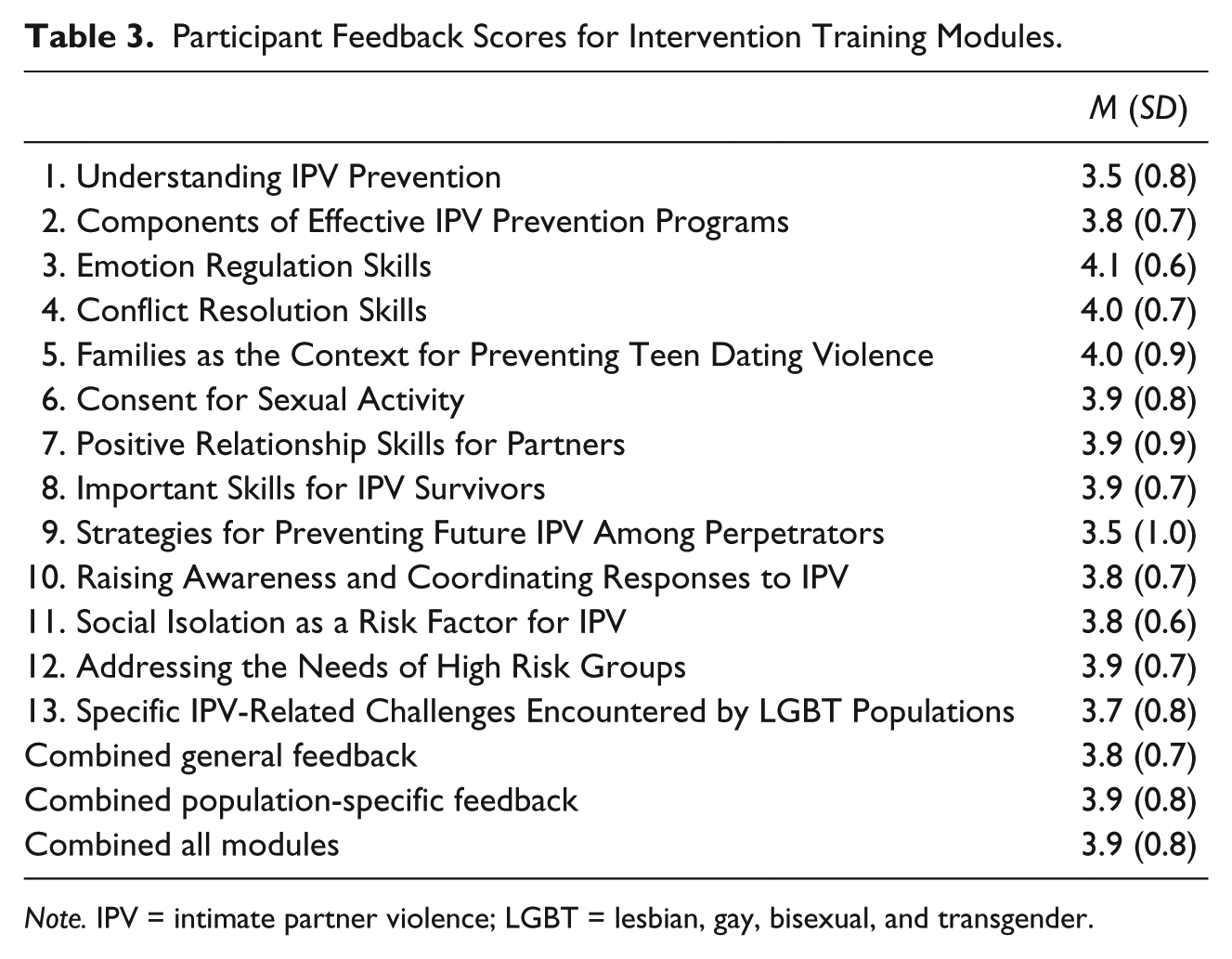
Note. IPV = intimate partner violence; LGBT = lesbian, gay, bisexual, and transgender.
Longitudinal Intervention Effects on Knowledge, Skills, and Behavior
Analyses demonstrated that there were no significant differences in the general or population-specific scores for knowledge, skills self-efficacy or implementation, or behavior by condition at baseline. The parameter estimates in Table 4 indicate that the mean scores across most outcome domains did not change significantly over time during the course of the study. The exception was specific skills implementation, which increased significantly (βtime = 34.9, p < .001) between baseline and 3-month follow-up for all participants, regardless of study condition. In addition, the time by condition interaction was not significant for the specific knowledge, skills, or behavior scores. However, a significant time by condition interaction was observed for general knowledge (βtime×condition = 170.8, p < .001), and both general (βtime×condition = 10.6, p < .001) and specific (βtime×condition = 12.0, p < .001) skills self-efficacy scores. These results indicate that participants in the IMPACT intervention condition increased their general knowledge and their general and population-specific skills self-efficacy at a greater rate than those in the control condition.
Adjusted Fixed Effect Parameter Estimates for Intimate Partner Violence–Related Knowledge, Skills, and Behavior Scores Using a Longitudinal Random Effects Model.
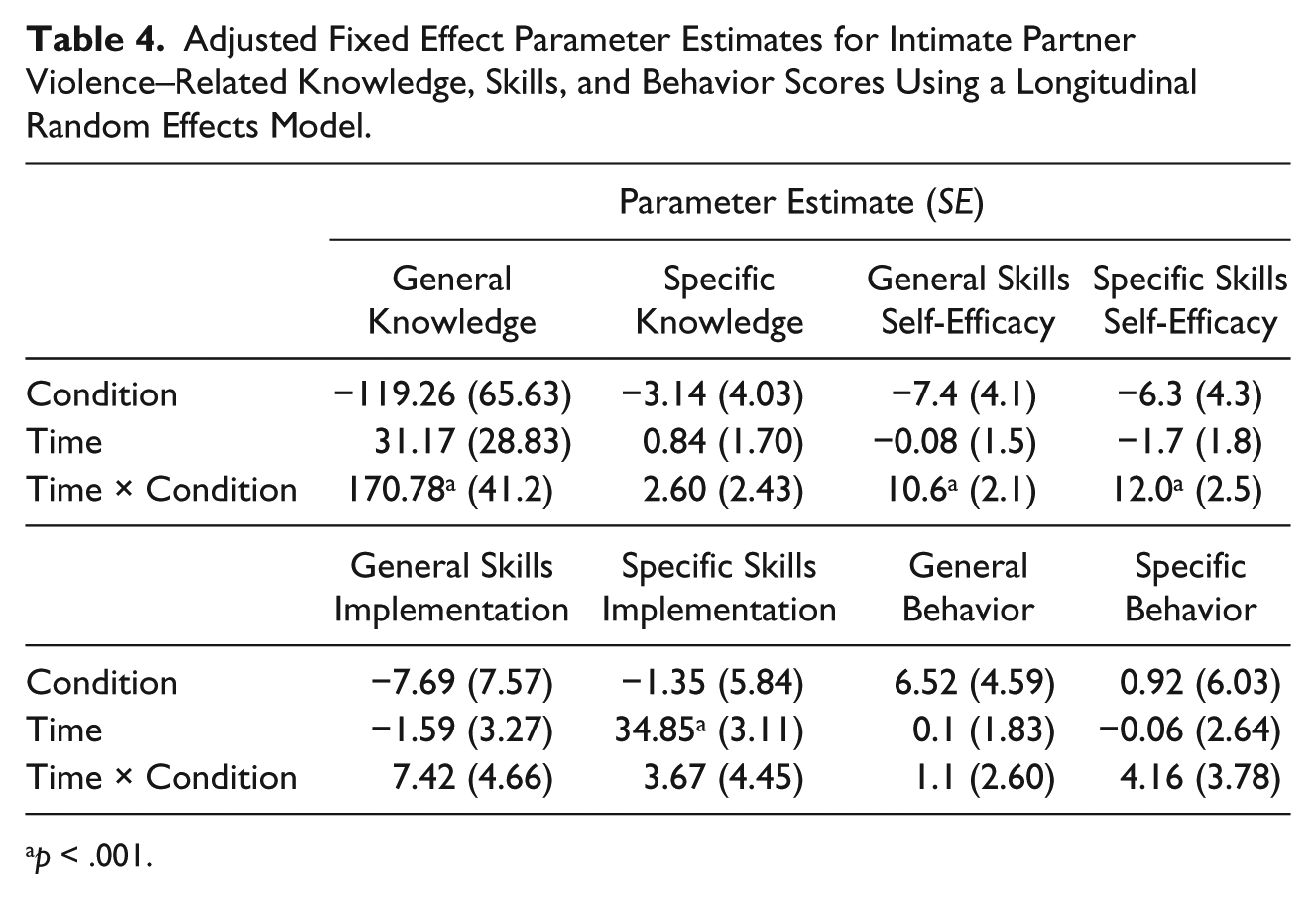
p < .001.
Moderation analyses examining whether results differed by participants’ years of experience in IPV prevention demonstrated no effect on any of the longitudinal models; for parsimony, the variables indicating IPV prevention experience level, and its interaction with study condition, were removed from the models.
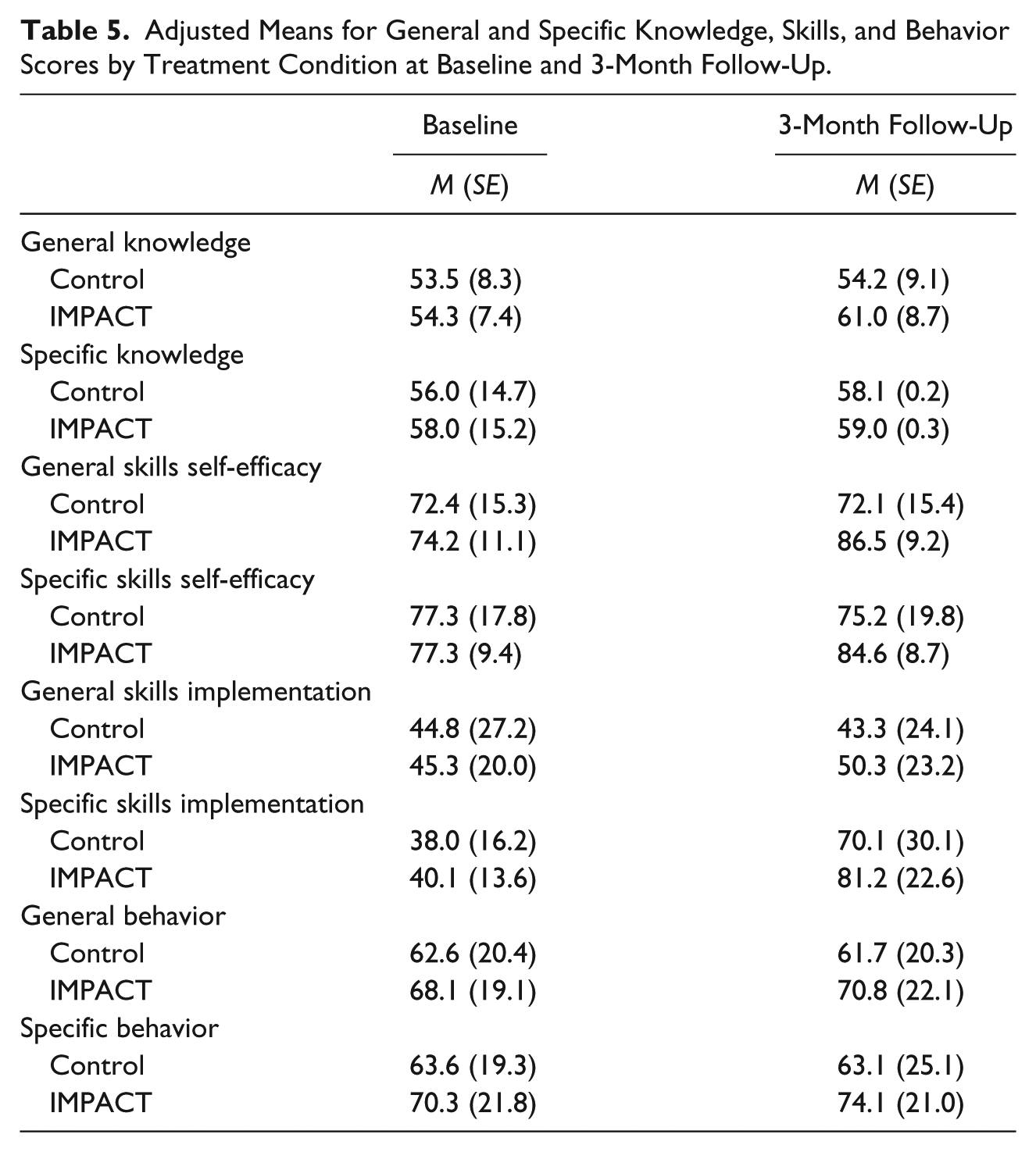
Adjusted means and standard errors for all general and specific knowledge, skills, and behavior scores by condition at baseline and 3-month follow-up are presented in Table 5. Effect sizes for the general knowledge (Cohen’s d = 0.76), and the general (Cohen’s d = 1.14) and specific (Cohen’s d = 0.62) skills self-efficacy scores were calculated using the adjusted means and standard errors (J. Cohen, 1988).
Adjusted Means for General and Specific Knowledge, Skills, and Behavior Scores by Treatment Condition at Baseline and 3-Month Follow-Up.
Discussion
The IMPACT intervention, a set of multimedia, interactive, online training modules for professionals engaged in direct IPV prevention work, was shown to increase participants’ general knowledge, and their confidence in their ability to use both general and population-specific best practice strategies (skills self-efficacy) over the 3-month study period. IMPACT did not achieve significant increases in participants’ population-specific knowledge, or in their general or specific skills implementation or behavior. These results suggest that the IMPACT intervention is capable of increasing participants’ knowledge about general IPV- and prevention-related topics and their self-efficacy to use both general IPV and population-specific best practice strategies in their prevention work; moderate to large effect sizes demonstrate that these results are meaningful for IPV prevention practice.
These results are notable in light of the relatively short follow-up period and the fact that the intervention was delivered online. IPV prevention professionals need easy-to-use, accessible capacity-building tools that provide a bridge between science and practice. This study shows that IMPACT, delivered online at professionals’ own pace, can be efficacious in increasing the knowledge and self-confidence to use learned best practice strategies that may help professionals prevent IPV among the clients, patients, and students with whom they work.
Participants in the study were highly heterogeneous, representing a wide range of professional titles and duties, organizational sizes and settings, educational backgrounds, and geographical areas. Notably, while several participants indicated in feedback surveys that the IMPACT modules are especially appropriate for IPV professionals who are new to the field, analyses showed no moderating effects of experience level. This suggests that IMPACT can increase knowledge and self-efficacy for science-based IPV-related best practice strategies for all professionals, regardless of how long they have been engaged in IPV prevention work. Thus, the potential reach and uptake for IMPACT is high, and results from this study are likely generalizable to a variety of different IPV prevention professionals and settings.
This study has several potential limitations. First, the length of follow-up was relatively short (3 months from baseline); it is unclear whether the observed increases in knowledge and self-efficacy were sustained over a longer period of time. The short length of follow-up may also provide an explanation for why IMPACT did not demonstrate increases in participants’ use of IPV-related best practice strategies: they may simply not have had sufficient time and opportunity to implement more of the strategies they learned via IMPACT. This may be especially true because some participants completed the 3-month follow-up only 6 weeks after completing the intervention. Future research could extend the length of follow-up to evaluate whether IMPACT produces lasting changes in IPV-related knowledge and self-efficacy, and to provide a longer time period in which to observe behavior change. Second, the study did not utilize blinded condition assignment, which may have resulted in differential responses to the self-reported self-efficacy and behavior questions; this presents a potential threat to the internal validity of the study. Third, it is possible that participants’ completion of other IPV-related training during the course of the study may have influenced their reported knowledge, skills, and IPV-related behavior. While participation in other non-IMPACT IPV training did not differ by study condition, the diversity of non-IMPACT training titles precluded an analysis of whether training type differed by condition. Another potential threat to external validity is selection bias, as professionals who were sufficiently motivated to participate in the study may not be representative of the broader IPV prevention professional population. Finally, while the sample was diverse across multiple domains, the majority of participants were White and female, which may limit the generalizability of the results in terms of both race/ethnicity and gender, although it is unclear whether the sample differs significantly from the larger population of IPV prevention professionals in the United States. Future studies may consider targeted recruitment efforts to ensure more representation from men and non-White racial and ethnic groups.
In conclusion, the IMPACT intervention, a set of interactive, online, science-based training modules self-administered by a diverse sample of IPV prevention professionals, was successful in increasing general IPV prevention knowledge and self-efficacy to utilize best practice strategies in real-world IPV prevention work. Given the scope and severity of IPV in the United States (Smith et al., 2018), highly scalable interventions like IMPACT can play a crucial role in disseminating science-based, best practice prevention knowledge and skills to front-line professionals, thereby helping to prevent and stop IPV.
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance that state-level domestic and sexual violence coalitions provided in recruiting participants for the IMPACT study. The authors also thank these participants for the substantial time, effort, and commitment they contributed to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant R44 HD072725).