
Abstract
Reproductive coercion (RC) is a form of violence perpetuated against women. It occurs when male partners adopt behaviors meant to control a woman’s birth control or pregnancy despite her wishes. This amounts to interference with a woman’s autonomy in reproductive decisions. The three main forms of RC are birth control sabotage (including nonconsensual condom removal), pregnancy coercion, and controlling the outcome of a pregnancy. This qualitative exploratory study examines issues in the acknowledgment of RC. Participants were 21 young women in Québec (Canada), who had experienced this form of violence. Results of individual semi-directed interviews reveal that RC can be difficult to acknowledge. A thematic analysis demonstrates that awareness is modulated by the manifestations of RC and by the emotional bond with the perpetrator. Acknowledgment of RC behavior varies according to the form that is experienced: Nonconsensual condom removal is the most readily identified, whereas acknowledgment of pregnancy pressure and pregnancy coercion takes longer, requiring repeated incidents before it is identified as a form of violence. In addition, acknowledgment is facilitated when relationships are casual and uncommitted compared with romantic and committed. Moreover, reading about the issue, confiding in a friend or acquaintance, and finding a new partner who respects one’s reproductive rights facilitate RC acknowledgment. In contrast, not self-identifying as a victim, assuming responsibility for the incident, having a limited understanding of sexual violence, and experiencing other forms of violence with an intimate partner contribute to impede RC acknowledgment. Results are discussed in terms of practical implications for young adults and health care professionals.
Keywords
Violence against women constitutes a major social and public health issue (World Health Organization, 2002). The United Nations defines it as follows: any act of gender-based violence that results in, or is likely to result in, physical, sexual or psychological harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life. (United Nations General Assembly, 1993)
Globally, an estimated 35% of women worldwide are victims of violence, with serious consequences for their physical, psychological, sexual, and reproductive health (World Health Organization, 2013). Reproductive coercion (RC) is a form of violence perpetrated against women that occur “when women’s partners demand or enforce their own reproductive intentions” (Moore, Frohwirth, & Miller, 2010, p. 1738).
Various conceptualizations and typologies of the forms of violence have been proposed in the literature (Institut national de santé publique du Québec, 2018; Kelly & Johnson, 2008; Lessard et al., 2015; Nicolaidis & Vanya, 2009). Due to its high prevalence, we consider intimate partner violence (IPV) as one of the predominant forms of violence against women (World Health Organization, 2013). For instance, about one in five women in North America has experienced physical or sexual violence (SV) by an intimate partner (World Health Organization, 2013). More alarming still is the serious and widespread scope of this behavior. Because IPV encompasses psychological, verbal, and sexual aggression as well as economic domination, it cannot be conceptualized as the outcome of loss of control, but instead as a strategy for dominating another person (Gouvernement du Québec, 1995). SV is understood as “any sexual act, attempt to obtain a sexual act, unwanted sexual comments or advances, or acts to traffic, or otherwise directed against a person’s sexuality using coercion, by any person regardless of their relationship to the victim [ . . . ]” (World Health Organization, 2013, p. 149). More specifically, intimate partner sexual violence (IPSV) refers to sexual aggression perpetrated by an intimate partner (e.g., nonconsensual fondling or penetration or sexual aggression) (Bagwell-Gray, Messing, & Baldwin-White, 2015). RC is closely linked to IPSV, as victims of male partner contraceptive interference more frequently report partner sexual assault (Katz & Sutherland, 2020), sexual persistence from their partner, defined as continued sexual pursuit despite a partner’s refusal, and more frequent compliance with unwanted sex (Katz & LaRose, 2019).
RC: An Emerging Form of Violence at the Intersection of IPV and SV
RC is an emerging category in the terminology of violence. Indeed, few data document the chronology and crystallization of RC in the context of IPV. Thus, data on dynamics of IPV and its intersection with RC is limited, as well as data examining the relational context of RC (Katz & LaRose, 2019). It has been studied mainly by health researchers (American College of Obstetricians and Gynecologists, 2013; Silverman & Raj, 2014). It can be defined as “behavior that interferes with contraception use and pregnancy in ways that reduce female control over reproductive decisions” (Silverman & Raj, 2014, p. 2). In an RC situation, it is more difficult for women to exercise their reproductive rights because the partner overrules them using intimidation, threats, or violence (Moore et al., 2010). Although RC is most often conceptualized as occurring within an intimate partner relationship, it can also occur in other contexts. For example, institutions have been known to sterilize women with intellectual disabilities (Tilley, Walmsley, Earle, & Atkinson, 2012). RC may also occur within a family, for example, when parents wield their legal authority to prevent their daughter from having a voluntary abortion. That said, in this article, we focus on RC in intimate partner heterosexual relationships, whether casual or committed. We have chosen to focus on heterosexual relationships as this is the most documented type of relationship in the literature, and issues related to reproductive and sexual health can be addressed simultaneously when RC is perpetrated by a male to a woman.
Three Manifestations of RC in Intimate Partner Relationships
Studies of RC have identified three types of situations in which it manifests: birth control sabotage, pregnancy coercion, and controlling the outcome of a pregnancy (Grace & Fleming, 2016; Grace & Anderson, 2018; Lévesque & Rousseau, 2016). Birth control sabotage refers to behavior that interferes with the partner’s contraception method using one or more tactics such as hiding, damaging, or removing birth control pills; damaging or piercing condoms; or nonconsensual removal of a vaginal ring, contraceptive patch, or intrauterine device (IUD) (Chamberlain & Levenson, 2012; Nikolajski et al., 2015). Brodsky (2017) adds the practice of “stealthing,” defined as “nonconsensual condom removal during sexual intercourse.” We should recall that since 2014, the Supreme Court of Canada has considered condom sabotage as sexual assault (“R. c. Hutchinson, 2014 CSC 19,” 2014). This ruling reminds us that the partners must consent to the types of sexual activity that they will perform as well as the conditions for them to take place. When fraud is involved, such as lying about wearing a condom, the notion of consent is vitiated and the behavior qualifies as SV.
Pregnancy pressure refers to behaviors that seek to pressure a female partner to become pregnant despite her wishes or intentions (Chamberlain & Levenson, 2012; Miller & Silverman, 2010). This form of RC may involve physical violence or threats of same, forced sexual relations, or threats to withhold financial support or to end the relationship and have a baby with another woman (Nikolajski et al., 2015).
Pregnancy coercion refers to controlling and dominating behaviors such as threats or acts of violence if the woman does not comply with her partner’s wishes concerning the outcome of a pregnancy (Chamberlain & Levenson, 2012). For instance, some women are pressured to continue a pregnancy that they want to terminate, whereas others are pressured to terminate a pregnancy that they want to continue (Chamberlain & Levenson, 2012; Nikolajski et al., 2015). Other women have reported that their partner tried to physically injure them to provoke a miscarriage (Chamberlain & Levenson, 2012; de Sousa, Burgess, & Fanslow, 2014).
Prevalence of RC
According to the few available data, the estimated RC prevalence varies from 5% to 13% for women aged 16 to 29 years who consult a family planning clinic (Grace & Anderson, 2018), with 9% for women in the United States (Black et al., 2011). RC may be manifested by various behaviors. In a literature review, Grace and Anderson (2018) report U.S. prevalences ranging from 7% to 11% for birth control sabotage, 1% to 2% for stealthing, and 1% to 19% for pregnancy pressure. For pregnancy coercion, the prevalence ranges from 0.1% to 4% for coercion or pressure in the decision to terminate, with 8% for pressure by the male partner not to terminate. However, RC rates appear to be considerably higher when women are questioned at health care facilities (Grace & Anderson, 2018) or when younger members of the population are questioned. In a recent survey for which undergraduate female students were recruited, 21% of them reported contraceptive interference (Katz & LaRose, 2019). In addition, there is a very strong association between women who experience IPV and reports of RC. Indeed, almost half of women who reported experiencing RC said that they had also been a victim of IPV (Katz, Poleshuck, Beach, & Olin, 2017; Sutherland, Fantasia, & Fontenot, 2015). In Canada and Québec, the scope of this problem remains unknown.
Acknowledgment of SV and RC Violence Victimization: Issues and Challenges
The difficulty in acknowledging the presence of violent behavior in intimate relationships is not limited to cases of RC. Although recognition of victimization has been addressed in many studies of domestic violence and sexual assault (Fisher, Daigle, Cullen, & Turner, 2003; Koss, 1985), clearly delineated definitions of the various forms of sexual victimization have not been proposed (Harned, 2005). That said, in the 1980s, Koss documented acknowledgment issues based on the experience of women that she identified as “hidden rape” victims, meaning that they reported experiences that complied with the legal definition of rape but did not identify them as such (Koss, 1985). Since then, several studies on this topic have indicated that non-acknowledgment is a widespread problem for women (Cleere & Lynn, 2013; Harned, 2005; Johnstone, 2016; Littleton, Grills, Layh, & Rudolph, 2017; Wilson & Miller, 2016). The majority of these studies used various versions of the Sexual Experiences Survey, a questionnaire that measures sexual aggression toward women with items concerning coercive, threatening, and forceful behavior, as well as explicit questions addressing acknowledgment of sexual victimization. When respondents identify a set of behaviors as representative of their intimate experience and that these behaviors are considered sexual assault by the law, but that they do not feel victimized, the researchers may decide it is a case of non-acknowledgment. For example, the meta-analysis by Wilson and Miller (2016), which covers 28 articles and data on 5,917 rape survivors in the United States, indicates that more than half of the female victims (60.4%) did not acknowledge that they were victims of sexual aggression, although their experiences may qualify as assault. It is noteworthy that the prevalence of non-recognition was significantly higher (62.7%) in female college students aged 16 to 24 years compared with older noncollege participants.
Other studies have identified barriers and factors that impede acknowledgment of SV by victimized women. Littleton et al. (2017) found that a closer relationship with the assailant strongly influenced the failure to acknowledge sexual aggression. For example, when the perpetrator was a romantic partner, there was much less acknowledgment of sexual aggression compared with casual or non-romantic partners. Furthermore, unacknowledged victims were more likely to continue the relationship with their assailant than women who acknowledged the behavior as violent (Littleton et al., 2017). Drug or alcohol use at the time of the sexual aggression is another influential factor in the nonrecognition of violence (Fisher et al., 2003; Harned, 2005). In a qualitative study, Harned (2005) found that many women who reported having unwanted sexual experiences under the effect of alcohol or drugs tended to feel responsible for what happened, so they absolved the partner of blame. They did not seem to consider how being intoxicated could affect their capacity to consent. In other cases, unacknowledged victims excused the aggressor’s behavior because he was drunk or drugged, and therefore out of control (Harned, 2005).
As is the case for conjugal and sexual violence, women who experience RC may find it difficult to acknowledge that their partner’s behavior is violent (Brodsky, 2017; Nikolajski et al., 2015). For example, in her article on stealthing, Brodsky (2017) noted that some women considered nonconsensual condom removal as a form of violation of their dignity and autonomy. Nikolajski et al. (2015) argue that women may not necessarily recognize RC as unhealthy behavior when the relationship is not physically violent or when they believe that it is normal behavior for a couple. Similarly, Fisher et al. (2003) showed that women were more likely to count incidents as sexual aggression when the aggressor used physical force, threatened to use physical force, or stopped just short of nonconsensual penetration. Johnstone (2016) explains that nonrecognition of sexual assault is due mainly to the fact that women often assume they, and not the aggressor, are to blame. This normalizes or diminishes the seriousness of the act. Some women simply avoid talking about it so as not to be labeled as a victim. The confusion surrounding consent has also been identified as a significant barrier to acknowledgment of victimization. Harned (2005) observed that some interviewed women did not label unwanted sexual experiences as sexual abuse or assault because they felt that they had failed to send a “no” message or to clearly explain that they did not want sexual relations. Others said that they did not label the experience as sexual abuse or assault because they ended up saying “yes” under their partner’s insistent advances and pressure (Harned, 2005).
Objectives
Acknowledgment is an essential process that enables the victim to name that she has been violated, and, if she wants, to get the support and services that can help her. This exploratory qualitative study was conducted to more deeply explore young women’s acknowledgment of RC and the associated issues. We addressed the following questions: (a) How does the RC acknowledgment process take place according to its different forms? (b) How does the relational context influence RC acknowledgment? (c) Which factors facilitate RC acknowledgment, and which contexts and factors impede it? This reflection is part of a larger study based on a theoretical framework of intersectional feminism conducted to examine RC and the help-seeking and service use trajectories of young women aged 18 to 29 years.
Method
Participants
Twenty-one young women aged 18 to 29 years (M = 24.85; median: 26; SD = 2.81) participated in this study. Most were Canadian citizens (95.2%). The majority were Caucasian (71%), with 10% Caribbean origins, 10% North African origins, and one Asian origins (5%). Most participants identified as heterosexual (n = 15; 71%), with some bisexual (14%), queer (10%), or asexual (5%). The majority were students at the time of the interview (62%), with 24% working full-time and 13% receiving welfare. Most had completed post-secondary education (81%).
Procedure
The study protocol was approved by the ethics committees of the main researcher’s university and of the CEGEPs (the college equivalent in Québec) that agreed to participate (n = 6). The participants were selected by purposive sampling (Patton, 2002) using the following criteria: age 18 to 29 years, has experienced reproductive 1 coercion in the last 2 years in the context of an intimate relationship involving or not an emotional attachment to a male partner, and French-speaking. Participants were recruited in Montreal (Canada) via flyers placed in colleges and universities and via recruitment ads and business cards posted in abortion clinics, on social media, and in various community organizations that work with female victims of violence. Twenty-one participants completed an individual in-depth interview between March 2017 and May 2018. An additional 11 women initially contacted the team to participate in the study, but of these, two lost interest, six failed to confirm the interview appointment, one was younger than 18 years, and two did not meet the inclusion criteria. Most of the interviews were held in a private office space at the university and all were audio-recorded. The interviews lasted from 30 to 90 min. Each participant received a monetary compensation of CAD$30. Verbal and written informed consent was obtained before the interviews began.
Measures
Individual interview
The research team developed a guide for conducting the in-depth interview used in this study. The interview covered various themes: the participant’s representation of her intimate relationship; RC manifestations, chronicity, and summation over time; acknowledgment of RC; coping skills; and contacts with health professionals and/or community counselors. The interviews were semi-structured and based on open-ended, non-leading questions. Follow-up questions were asked depending on the participants’ responses to lead-off questions. The guide was revised slightly after the first interviews to include points that emerged from the participants’ statements, such as the impact of disclosure movements (e.g., #BeenRapedNeverReported; #MeToo) on their resilience paths.
Questionnaire
At the end of the individual interview, participants were asked to complete a short questionnaire to gather data on sociodemographic characteristics, RC experiences (translated into French) (Clark et al., 2014; Miller, Jordan, Levenson, & Silverman, 2010), and reproductive health. Seven items addressed manifestations of RC, the presence of physical or emotional violence, and the intensity of conflicts with the partner. Seven items addressed the partner’s interest in the participant becoming pregnant (e.g., “Did he tell you not to use contraception?”; “Did he force you to have unprotected sex so you would become pregnant?”). Four items addressed the negotiation (or not) of decisions concerning reproductive health (e.g., “Did you ever fear discussing contraceptives with your former partner?”).
Data Analysis
The interviews were transcribed verbatim. Data management and analysis were performed by thematic analysis (Braun & Clarke, 2012) using NVivo 11 (QSR International Pty Ltd.). Thematic analysis is a method for identifying, analyzing, and reporting patterns (themes) within data (Braun & Clarke, 2012). Accordingly, we (the research team, comprised of both authors and a doctoral student) first performed an active reading of all the transcripts. We then individually generated an initial coding on the first two interviews that was later subject to a group discussion where its discrepancies were resolved. The final coding was then applied to all remaining interviews by two members of the research team, following an appreciation of intercoder agreement (90% baseline as measured by kappa coefficient with NVivo). We created matrices to more clearly identify the divergences, similarities, and central points associated with the acknowledgment process as a function of the relational context (Miles, Huberman, & Saldana, 2014). Initial themes were identified, discussed in group meetings and reviewed. We then assigned appropriate names for the themes and chose the extracts that best illustrated the analysis.
Results
The participants had experienced various forms of RC, and in different relational contexts, as presented in Table 1. All participants who said they had been in an intermittent uncommitted relationship reported nonconsensual condom removal. This manifestation of RC also occurred in repetitive uncommitted relationships and in couple relationships in which violence was present. Pregnancy pressure (encouragement or discouragement) and pregnancy coercion (forced continuation or termination) were present only in couple or repetitive uncommitted relationships. Only one participant reported incidents of control or constraint over the use of her contraceptive method when she was in a couple relationship without violence. Participants may have experienced RC in more than one relationship during the surveyed period. As a result, the number of reported situations exceeds the number of participants.
Manifestations of Reproductive Coercion According to Relational Context.
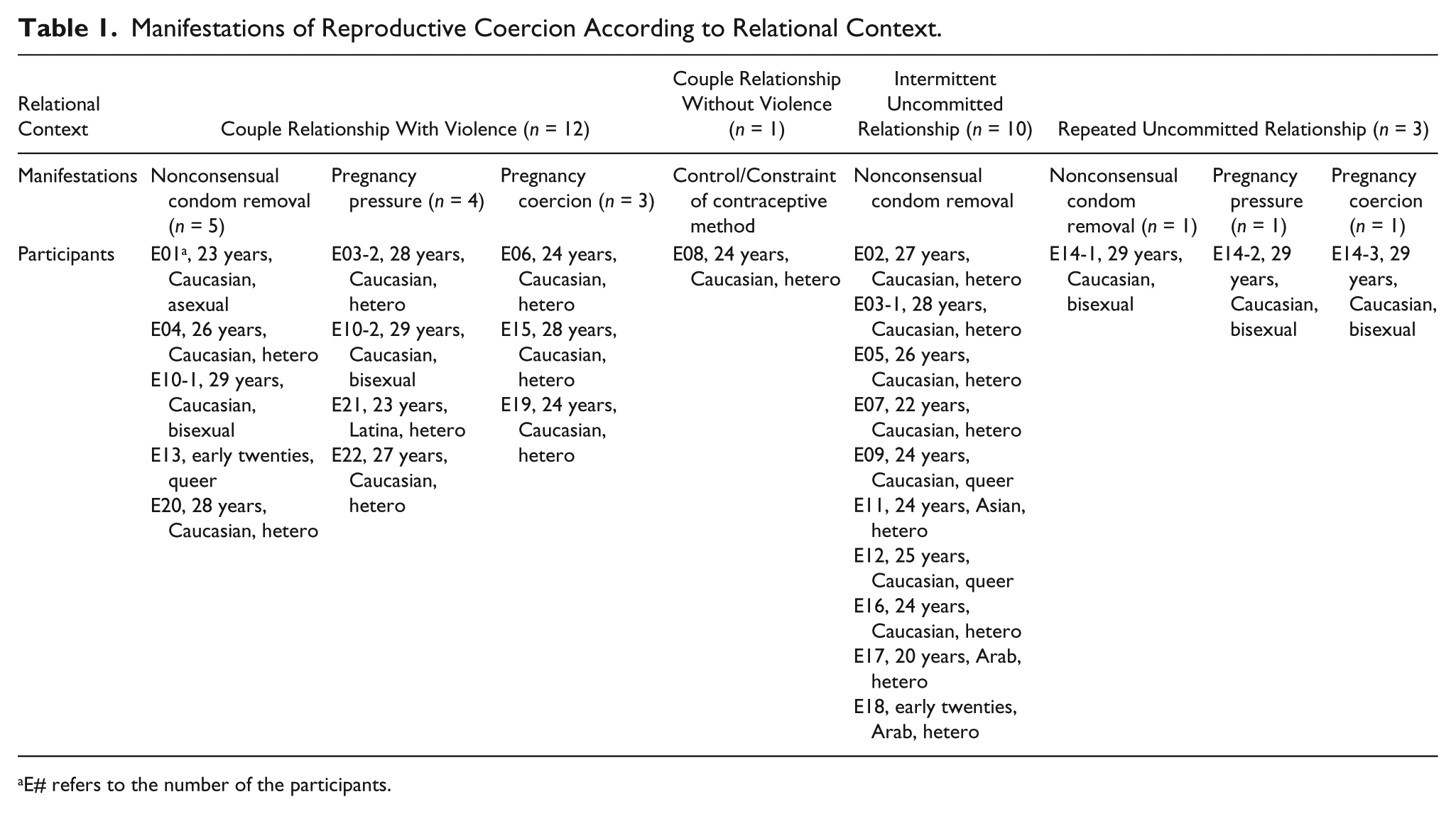
E# refers to the number of the participants.
Acknowledgment of RC: Influence of the Type of Violence Perpetrated, Awareness of the Associated Consequences, and the Relational Context
The analysis of the interviews revealed that RC acknowledgment followed a process that was modulated by the type of violence perpetrated. Thus, nonconsensual condom removal, pregnancy pressure, and pregnancy coercion contributed differently to the RC acknowledgment process, either facilitating or impeding it. The relational contexts also made distinct contributions. In a committed relationship, the acknowledgment process was more challenging due to romantic feelings that blurred judgment. Moreover, women who were not in a committed relationship appeared to assume more responsibility for RC incidents, which impeded their acknowledgment of RC as perpetrated violence.
Nonconsensual condom removal: Rapid and clear acknowledgment
The participants acknowledged nonconsensual condom removal as RC via two central processes: (a) non-respect of a prior agreement about contraception, with consequences for the consent to have sexual relations and (b) immediate and short term-term reactions to the incident. This manifestation of RC was more readily and rapidly acknowledged because it was concrete and visible during sexual relations (i.e., the condom was absent).
Most participants perceived nonconsensual condom removal as problematic primarily because it was a violation of a prior agreement with the partner about condom use during sex. The analysis of the contraceptive negotiation process clearly shows that condom use was discussed and agreed upon before sexual relations could take place (Lévesque, Rousseau & Dumerchat, Forthcoming). The discovery that the partner did not respect the agreement led to rapid acknowledgment of the situation as inacceptable, as these extracts testify: There was penetration, without a condom. Oh man! I was in a rage. Really. I pushed him off me and I said, “What did you just do?” Me, I say, “It was clear as black and white: I told you no way.” He says, “Oh, I was so excited, I thought it would be OK.” So I say, “No, we talked about it. It was very clear.” (E04) I was really mad, that time! Me, I took precautions to make sure there was no contact with [ . . . ] oh [ . . . ] whatever! So I wouldn’t catch heaven knows what! And then, that guy, he took off the condom and it was like he had the right to decide for me. Was I ever mad, that time. (E18)
For another participant, sexual consent applies repeatedly in a sexual relationship, and nonconsensual condom removal invalidates this consent: “You know, I agreed to have protected sex with you. If it’s not protected, then I haven’t agreed” (E05).
The immediate reactions following RC strengthened the feeling that the incident was problematic: “Then a minute later, I was crying, and I was like, ‘OK, so why do I feel bad?’” (E12). In this case, the sadness and anger that were felt and identified so rapidly prompted the participant to think about what had happened and to identify what had provoked the distress and tears. The participants also reported several consequences of nonconsensual condom removal, including fear of catching a sexually transmitted infections (STI; n = 10) or getting pregnant (n = 5) as well as psychological repercussions such as shame (n = 8), anxiety (n = 7), anger (n = 6), insecurity (n = 6), and confusion (n = 5). The impact of these consequences on their physical or psychological well-being enabled the participants to acknowledge the behavior as RC. Thus, their emotional reactions sent a signal that the situation was problematic, whereas in a sexual relationship that is desired, consensual, and respectful, these consequences would not arise. Furthermore, all participants whose sexual partner had removed a condom without consent ended the relationship with the partner.
Nevertheless, despite the fact that the participants reported immediate negative reactions, some of them doubted their right to confront their partner about the incident, particularly when he was indifferent. In other situations, the partner played the incident down so as to soften the women’s reaction (e.g., claiming that she’s exaggerating, that it’s not serious). This manipulation made the women doubt the seriousness of the experience and the validity of their feelings about it. According to one participant, “OK, maybe I’m freaking out for nothing, basically. I’m freaking out for no reason. I have to calm down” (E12). Moreover, following the participant’s negative reactions, some partners proposed alternate versions of the situation, making it more confusing and difficult to interpret: Then after, this is what happened. He was like, “Well, excuse me! I didn’t know. How was I supposed to know! You learn something new every day!” Blah, blah, blah [ . . . ] [playing] the innocence card. I’m like, “Whoa! He’s deciding to be all humble! Oh boy. Now what do I do?” So, that’s how it went. It turned into grayer and grayer areas on top of gray areas, until [ . . . ] everything got totally confused. (E12)
Pregnancy pressure: Difficult to acknowledge and accept
Five participants had experienced this type of RC in a couple relationship where violence was present or in a repetitive uncommitted relationship. They report the main problem was recognizing the presence of violence in their intimate relationship: “I never stopped to think that it was manipulation, or that he [ . . . ] Like, he was treating me super badly! And that it was unacceptable. I didn’t take the time to think about it” (E21). Thus, at the time when they were being subjected to the behavior, the young women did not necessarily recognize it as violent. Some felt that although they did not recognize the violence during the relationship, later they were able to, after separating from the partner, as this participant explains the following: A month after separating and even during the relationship, I don’t think I can say that I experienced reproductive coercion. It’s really a lot of little things that accumulate, and then I become aware in hindsight, because I have to accept it, because [ . . . ] You know, I’m starting to be able to use the words that I feel apply. (E10)
The awareness of the various consequences involved also helped the participants recognize, in time, that their partner had behaved violently toward them during the relationship: I didn’t see the violence. I saw it after, especially in the aftereffects, and by thinking about them, by kind of analyzing these aftereffects. Well, I thought it over and it was actually [ . . . ] I was traumatized by the violence. It’s as if it took these symptoms and problems to get me started, to mull it over and realize. (E10)
In addition, because it was easier to identify problems in someone else’s relationship, learning that the former partner was repeating the same violent behavior in a new relationship could facilitate awareness of the violence that occurred in the participant’s own relationship. In short, pregnancy pressure, having the added element of IPV, appears to have taken more time to acknowledge than nonconsensual condom removal.
Pregnancy coercion: Abortion, a turning point in the acknowledgment of RC
Three participants reported experiencing pregnancy coercion. Two of these had gone through an abortion even though they had not yet decided whether or not to continue the pregnancy. Instead, the decision to terminate resulted from the partner’s pressure or threats. One participant had talked with the father about having a child, and both seemed to be in favor. Then there was an incident of unprotected sex, encouraged by the partner, who said, “It’s a new year. We can start off on a good foot, and whatever happens, happens!” The result was pregnancy. This provoked a strong reaction by the partner, who forced her to have an abortion. The abortion was a watershed moment for the participant. The serious distress that she felt triggered her awareness of the RC: “I fell into a deep depression, with suicidal thoughts and all that” (E06). One participant mentioned that after an unplanned pregnancy attributed to contraceptive failure, her partner refused to discuss it and forced her to have an abortion. She said she had wanted to talk it over with him, at least to feel that they had made the decision together. For her, the RC was manifested by her partner’s close-mindedness and refusal to listen, as well as his lack of responsibility on the day of the abortion: He was at his place [ . . . ] He was having fun while me, I was having an abortion, you know [ . . . ] So, you could say that I, like, realized what our relationship was, that it wasn’t all that great]. I, like, had to admit that [ . . . ] he didn’t really love me. (E15)
The third participant spoke more about her problems finding an appropriate contraceptive method, which led to some unplanned pregnancies. With the same intimate partner, she had had two pregnancies that were terminated after her partner threatened to leave her. She remembered that when she had the abortions, she had felt that it was her decision: “At first, I thought that I was the one who made the decision, but in the end, as time went on, I realized that he was the one who pushed me to do it” (E19). Only with the passage of time was she able to realize that her partner had imposed his will on her, and by the time of the interview she had come to regret it. In these three cases, the partner’s coercion to terminate the pregnancy enabled the participant to identify the non-egalitarian and controlling nature of the relationship and therefore end it.
Acknowledgment of RC Impeded by Individual Perceptions or Facilitated by External Factors
The analysis results revealed factors and contexts that either impeded or facilitated RC acknowledgment. When the participants talked about factors that impeded RC identification, they referred to their individual perceptions of the situation, whereas when talking about factors that facilitated RC identification, they referred to external influences.
Non-acknowledgment due to self-responsibilization, downplaying, IPV, and rejection of sexual victimization
Four main factors appear to have impeded RC acknowledgment in the young women we interviewed: (a) assuming full or partial responsibility, (b) downplaying the incident, (c) being in an intimate relationship marked by violence, and (d) having difficulty self-identifying as a victim. These factors were often intermingled in their statements.
Generally, participants who had experienced nonconsensual condom removal in an intermittent uncommitted relationship (n = 10) assumed more responsibility for the incident compared with those in a committed relationship. Some felt responsible for what had occurred, particularly when they felt that they should have made it clearer that they had not consented, even though they had repeatedly said that they wanted to use a condom: “I know that if I had talked about it more, if I had been surer of myself [ . . . ] We would have used a condom” (E17). Others reported that they had been drinking at the time, which clouded their recollection of what happened: “Hard to remember about that, speaking for myself [ . . . ] Because for me, you know, it was all a bit of a blur. We were drunk. Did I tell him it was OK to take off the condom?” (E11).
Many attempted to downplay the experience, especially when they had limited knowledge of the meaning of sexual aggression, or because they found it hard to view themselves as a victim. Being a victim would mean that they had been disrespected and under the control of another person during the incident. For example, one participant suggested that if she identified an experience as a form of SV, she would have to do something about it. They also said they would feel a responsibility to reproach the partner for his behavior so that it would not happen again: Would it, like, get more complicated if I told him that I had been sexually aggressed? Because it’s a battle. As soon as you say that, it’s like you’re in a kind of [ . . . ] And it’s a kind of battle where you say, “Well, this is wrong! I don’t want this to happen again! I don’t want this to happen to other girls!” And you get involved in a kind of fight, for me anyway, that’s what happens. By playing it down, well then, that’s the end of it. It’s like a weight off your shoulders, instantly. (E12)
One participant said that she did not know that the behavior was RC while it was happening. This contributed to her failure to acknowledge the situation as problematic, instead considering nonconsensual condom removal as “pathetic” or trivial: I really didn’t know that it was sexual aggression at the time. Me, I thought it [nonconsensual condom removal] was something funny, a totally “loser” move that you joke about, you know, but [ . . . ] in the end, not really. That was, like, hard for me. (E16)
The participants who had been in an intimate relationship marked by violence tended to downplay manifestations of RC (n = 7), because compared with other manifestations of violence that occurred in the relationship, they seemed insignificant. For example, the participants talked about their partner’s controlling, manipulative, and/or violent (psychological, sexual, and physical) behaviors. One participant who was involved in a violent relationship talked about the following: “[ . . . ] some really serious things, so that in the end, even condom removal, that kind of thing, for me it was [ . . . ] It seemed kind of insignificant” (E13). Two participants also said that the feelings they had for their partner led to a kind of tolerance of the RC behavior. They explained that their love for their partner effectively eclipsed the violent behavior: “Because I was blind, it was just him, so [ . . . ] He was [ . . . ] He was like an angel, then! I couldn’t see past that” (E19); “I felt like I’m saying too much about the positive side. But even if the relationship was only 20% positive, you could say that I loved him so much at the time, that it was strong!” (E15).
Despite the differences among the participants’ statements, they all had one thing in common: They found it difficult to self-identify as a victim. They reported that self-identification as a victim could negatively affect their self-perception. For example, one participant acknowledged that she had been in a situation of nonconsensual condom removal, but still did not self-identify as a victim: “Well, the thing is, me, I don’t identify as that type [ . . . ] It has to do with the fact that I would have [ . . . ] been in a situation where [ . . . ] Uh [ . . . ] I was [ . . . ] There was coercion, yeah” (E17). This tendency to refuse to be labeled as a victim could compromise RC acknowledgment, because these participants felt responsible for what happened to them: I don’t want to say that I’m a victim because I know that if I had taken measures into my own hands, like, spoken up [ . . . ] about what I think and what I feel [ . . . ] It wouldn’t have happened. So, I don’t want to call myself a victim in this case, because [ . . . ] Technically, I’m not, because all I had to do was, like, speak up. (E21)
Acknowledgment of RC following exposure to or awareness of the problem
The participants who reported RC acknowledgment mentioned four main facilitating factors: (a) acquiring knowledge about the issue, (b) hearing a friend describe RC behavior, (c) hearing about acts perpetrated against a friend, and (d) finding a new partner who respects her contraceptive choices.
First, the participants reported that reading about the issue of nonconsensual condom removal or more broadly about RC (n = 3) or hearing a friend describe RC behavior (n = 2) made them aware of the behavior they had been subjected to. Learning about RC also showed them that they were not the only ones to go through this kind of experience. This collectivization of experiences acted to strengthen feelings that these situations were problematic, as one explains, Well, [ . . . ] It was already a problem, but then I saw it as something that that was much more widespread. I saw that it was sort of [ . . . ] It’s super gross, actually! In fact, it’s really a big problem! (E18) Some handouts or [ . . . ] Studies about it, or just info. So in the end, when I read about it, I saw [ . . . ] I went, like, “Wow! That’s really what was happening all those times, and I’m not the only one.” (E20)
Furthermore, two participants said that talking it over with a friend allowed them to put words to their feelings of discomfort. Thus, one participant who reported being pressured by her partner to get pregnant said, “And so, together, by talking to her about it, I realized that [ . . . ] But it was manipulation!” (E21). Similarly, spending time or developing a relationship with a new partner who respected their contraceptive choices promoted acknowledgment of the problematic nature of RC behavior in a previous relationship. These external factors are related mainly to an empathetic response by a friend who listens, or by a new partner who agrees to respect the participant’s contraceptive choice.
In our analysis, we paid particular attention to how oppressions intersect. Thus, we sought to identify whether self-identification with a sexual orientation other than heterosexuality would show greater vulnerability to RC or follow a distinct RC acknowledgment process. We also focused on ethnocultural membership. However, the findings do not reveal distinctions according to these two identity markers, both of which are known risk factors for violence. Thus, in this sample of young women aged 18 to 29 years who have experienced RC in the last 2 years within a relationship with a male partner, self-identification with ethnocultural membership or sexual orientation does not appear to distinguish the experience of RC victimization.
Discussion
This article aimed to explore, based on reports of RC experienced by young female victims, the conditions, and acknowledgment process for this form of violence, as well as the contexts that modulate RC acknowledgment. The results suggest that the RC acknowledgment process varies according to the relational context and with perceptions of the consequences associated with the forms of RC experienced. This concurs with the findings on RC and SV in the broader sense (Boyle & McKinzie, 2015; Cleere & Lynn, 2013; Katz & LaRose, 2019; Littleton et al., 2017). Participants in intermittent uncommitted relationships who reported incidents of nonconsensual condom removal readily recognized the act, because it was visible (physical condom removal) and because it violated the original agreement with the partner concerning condom use. Based on the importance of sexual consent, the participants were able to acknowledge the behavior as violent. These results agree with Harned (2005), who found that some women acknowledged that they had experienced sexual aggression simply because they knew that the sexual activity took place without their consent. The distinction with our results lies in the fact that our participants wanted to have sexual relations. However, they wanted protected sex, which implies contextualized and conditional consent. Acknowledgment of the right to have protected sex and, as a corollary, acknowledgment of the non-respect of consent appear to be significant issues that young women need to be more aware of. However, our results depart from studies of sexual aggression showing that the presence of force or physical violence facilitated acknowledgment (Fisher et al., 2003; Harned, 2005). In another study, women found it harder to recognize RC behavior in the absence of physical violence (Nikolajski et al., 2015).
Our results demonstrate that whereas nonconsensual condom removal in an intermittent uncommitted relationship often spells the end of sexual relations and even contact with the partner, this manifestation of RC does not necessarily result in the end of the relationship for a committed couple. Other manifestations of violence in the couple relationship, as well as romantic feelings for the partner, appear to eclipse this form of RC, and notably due to the partner’s manipulative and controlling behavior. This difficulty in identifying nonconsensual condom removal as RC in a couple relationship—with or without violence—holds true for other manifestations of RC as well. Thus, participants who reported pregnancy pressure also said that they found it harder to recognize this form of RC, given its insidious nature. Instead, these participants reported recognizing RC after the couple broke up, thanks to hindsight and critical reflection. In the case of pregnancy coercion, abortion appears to have been the turning point for RC acknowledgment. These participants said that undergoing a forced abortion under the threat of breakup, their partner’s lack of responsibility on the day of the abortion, and the psychological consequences of the situation enabled them to acknowledge the behavior as violent and therefore unacceptable. They found it harder to acknowledge RC at the time it occurred. These results corroborate studies of SV in intimate relationships: Acknowledgment of such unwanted experiences is clouded by romantic feelings about the partner (Boyle & McKinzie, 2015; Cleere & Lynn, 2013). Similar results were found in studies of women having experienced sexual aggression, who acknowledged the victimization after realizing the extent to which the event had affected them physically and/or emotionally (Harned, 2005). Hence, addressing romantic sentiments and supporting authentic emotions and feelings in order to develop awareness and acknowledgment would be promising intervention avenues in cases of RC in intimate relationships.
Our results indicate that certain factors facilitate RC acknowledgment. The first is knowledge: reading up on nonconsensual condom removal or talking it over with a friend, acquaintance, or new partner who respects one’s contraceptive choices. These results are similar to those of Harned (2005), who found that some women who received information about sexual aggression were better able to describe their own experience as such. Chamberlain and Levenson (2012) also found that women who learned more about issues of IPV and RC were more inclined to recognize the presence of violence in the relationship and consequently end it. According to Harned (2005), discussing a past incident with others helped some women describe the experience as sexual aggression: Seeking social support was the most common event that triggered women to label their unwanted sexual experiences. More than two thirds of the women (n = 22; 68.8%) said that talking to supportive others after the incident led them to define their experience as sexual abuse or assault. (p. 390)
The participants’ statements also revealed factors that impeded RC acknowledgment: refusal to self-identify as a victim, assuming responsibility for the incident, having limited knowledge about sexual aggression, and being in a violent relationship. Some of these factors have been reported in previous studies on sexual aggression. For instance, some women avoid acknowledging that they experienced sexual aggression so as not to be labeled a victim, which would mean being perceived as vulnerable, controlled, and powerless (Johnstone, 2016). Furthermore, many women do not acknowledge that they were sexually assaulted because they blame themselves, maintaining that they acted recklessly (Harned, 2005; Johnstone, 2016). This can be credited to the social message that says it is up to women to avoid getting into situations that carry a risk for sexual victimization (Kavanaugh, 2013).
Study Strengths and Limitations
This study examines the reports of young women who wanted to share their experiences to help deconstruct the stigma, shame, and guilt associated with violent and RC behavior perpetuated by their partners. The willingness of the participants and the conscientious training and supervision of the research team that interviewed them enabled authentic conversations and meaningful exchanges. Moreover, the theoretical sample for this study presents a diversity of RC experiences, allowing a comparison of the acknowledgment process according to the forms of RC experienced, their frequency, and the relational contexts in which they took place. Nevertheless, this study includes certain methodological limitations, notably the small sample size. First, when the relationship was violent, it was often difficult to acknowledge that RC had occurred. The analysis revealed that these participants could more readily acknowledge that the relationship was unhealthy or harmful but were less able to identify manifestations of RC behavior. In some cases, the intertwined forms of violence within a relationship meant that some behaviors that were perceived as more serious, made some other behaviors look insignificant by comparison. Thus, the participants’ representations of their partners’ behavior according to the manifestation (e.g., physical force) and the relational context in which it occurred created a perceived hierarchy of violence. This acted to normalize or trivialize the RC. Therefore, more participants who were in violent relationships were able to tolerate RC behavior. Moreover, no participant reported forms of contraceptive sabotage other than nonconsensual condom removal. Nor did any participant report forced continuance of an unwanted pregnancy. Presumably, a larger sample would produce more testimonials of diverse forms of RC.
Practical Implications and Avenues for Future Research
These results have several practical implications. The analysis of the participants’ experiences revealed the non-isolated presence of the partner’s indifference to or misunderstanding of nonconsensual condom removal. This demonstrates the importance of the partner’s reactions in the acknowledgment of the problematic nature of RC, as well as appropriate attribution of responsibility to the women who are subjected to it. Therefore, awareness raising campaigns targeting young adults could improve their acknowledgment of RC behavior. These campaigns should include the legal fact that nonconsensual condom removal is considered a form of sexual assault. Health care professionals should also be on the lookout for young women who undergo repeated STI screenings, seek emergency contraceptives (morning-after pills), or consult for an abortion. Many of our participants reported seeking this kind of professional help following an RC incident, although the conditions that create risks for STI exposure or unwanted pregnancy were not discussed during the consultation, thereby limiting access to the appropriate support (Lévesque et al., Forthcoming). Therefore, it is suggested that health care professionals should not only ask whether a reproductive health risk has been taken (e.g., unprotected sex), but also ask how the woman was exposed to the risk. Women reporting CR may be referred to a women’s health center or a community organization specializing in SV.
Future studies could conduct a more detailed investigation of RC acknowledgment in an IPV context. For example, does RC acknowledgment lead to IPV acknowledgment, or is it the inverse? Are these acknowledgment processes concomitant or independent? It would also be useful to gain a deeper understanding of the motivations of the young men who perpetuate the various forms of RC to guide prevention programs. Better documentation of how RC manifests across the human life cycle would also be informative: Do mothers also report these forms of violence? Are they at greater risk for RC and IPV due to the presence of children and shared parenting with the partner? Finally, it is imperative to document the prevalence of this problem in clinical and population samples to develop targeted responses to specific needs.
Footnotes
Acknowledgements
The authors would like to thank the participants who courageously and generously shared their stories. They also thank the various organizations and individuals who collaborated in recruiting them. They are also grateful to Julie Laforest and Carole Boulebsol for their constructive comments on the preliminary manuscript. Further thanks are due to Mélusine Dumerchat and Émilie Blanchette, who improved the quality of this article by transcribing and participating in laboratory discussions of the analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a research grant awarded to the first author S.L. by the Fonds de recherche Société et Culture du Québec (FRQSC).