
Abstract
While the literature examining physical intimate partner violence (IPV) is extensive, the impact of psychological IPV on mental health during high-risk times such as the period following childbirth is not well understood. The current study examined associations between psychological IPV and the course and severity of women’s postnatal mental health symptoms (depression, anxiety, and trauma symptoms). Both main effects of psychological IPV exposure and possible exacerbation by broader social victimization (i.e., gender discrimination) were considered. Participants were 76 mothers from a larger longitudinal study, who completed self-report measures of IPV, gender discrimination, and affective symptoms at 3, 6, 12, and 18 months postnatal. Hierarchical linear modeling revealed a main effect of psychological IPV on the course of trauma symptoms only. As hypothesized, gender discrimination moderated the effect of psychological IPV on all symptom trajectories in a synergistic manner. At moderate to high levels of gender discrimination only, psychological IPV predicted higher affective symptom severity and an escalating course of postnatal anxiety symptoms. These findings underscore the importance of expanding current conceptualizations of IPV impacts to incorporate relevant aspects of individuals’ social-ecological context. Future directions and implications for prevention and intervention are discussed.
According to the Centers for Disease Control, approximately 37% of women in the United States report experiencing incidents of intimate partner violence (IPV)—acts of physical aggression, sexual coercion, psychological aggression, emotional abuse, and manipulative or controlling behaviors within an intimate relationship—at least once during their lifetimes (Smith et al., 2018). Negative outcomes from exposure to IPV include damage both to mental health (Blasco-Ros, Sánchez-Lorente, & Martinez, 2010; Breiding, Black, & Ryan, 2008; Coker, Smith, Bethea, King, & McKeown, 2000; Dutton, Bermudez, Matás, Majid, & Myers, 2013; Flanagan, Gordon, Moore, & Stuart, 2015; Jaquier, Flanagan, & Sullivan, 2015; Pico-Alfonso et al., 2006; Tiwari et al., 2008) and to physical health (Breiding et al., 2008; Campbell, 2002; Coker et al., 2000; Dillon, Hussain, Loxton, & Rahman, 2013; Sanchez-Lorente, Blasco-Ros, & Martínez, 2012; Stewart et al., 2017; Tiwari et al., 2008). Although IPV is detrimental at any time, women’s perinatal exposure to IPV is particularly concerning and has been reported in 3%-30% of pregnancies (Bhandari et al., 2008; Campbell, 2002). Given the deleterious lasting impacts of perinatal IPV on both maternal and child well-being (Campbell, 2002), these prevalence rates signify a global mental health concern.
While much of the perinatal IPV literature has focused on the impact of physical abuse/aggression, understanding the distinct contributions of psychological IPV to negative mental health outcomes across the life span has received increasing interest in recent years (Guyon, Sarah, Dunn, & Huth, 2017; Huth-Bocks, Krause, Ahlfs-Dunn, Gallagher, & Scott, 2013). Psychological IPV—that is, psychological aggression or emotional abuse—is more prevalent than physical violence (reported rates as high as 72%; see Dillon et al., 2013; Tiwari et al., 2008) and, as both an antecedent and correlate of physical aggression, it may create a context of risk for poly-victimization (Dillon et al., 2013). Experiences of psychological IPV have further shown similar or even greater negative effects on affective symptomatology (depression, anxiety, and trauma symptoms) compared with physical IPV (Blasco-Ros et al., 2010; Coker et al., 2000; Karakurt, Smith, & Whiting, 2014; Lawrence, Yoon, Langer, & Ro, 2009; Pico-Alfonso et al., 2006). However, the role that perinatal exposure to psychological IPV may play in mental health trajectories is not well understood. Furthermore, despite evidence of a relationship between affective symptomatology and psychological IPV, findings have been inconsistent on the strength of these relationships and the prevalence of negative outcomes (Howard, Oram, Galley, Trevillion, & Feder, 2013; Stewart et al., 2017). For example, a meta-analysis of the association between women’s postnatal depression and perinatal IPV exposure yielded widely varying effect sizes (Howard et al., 2013).
Inconsistent findings regarding the degree to which psychological IPV shapes perinatal mental health suggest that it will be important to broaden the investigative lens to consider factors that may work in tandem with IPV. A social-ecological framework that acknowledges combined impacts of stressors across multiple levels of a person’s experience within a larger social context could help shed light on sources of such variability. It is important to recognize individuals as part of a larger societal context, moving past the focus on individual-level factors and considering macro-level influences on mental health trajectories. Thus far, social-ecological models of IPV have largely focused on explaining risk of victimization or perpetration; however, it is equally important to extend this framework to better understand the impact of IPV. It may be necessary to broaden conceptualizations of factors that contribute to perinatal mental health outcomes after psychological IPV victimization to include the role of societal-level forms of victimization. One contextual factor requiring further study is gender discrimination; although reported by almost two thirds of women in the United States (Carliner, Sarvet, Gordon, & Hasin, 2017), limited attention has been paid to the effect of gender discrimination on mental health—especially perinatal mental health. According to this traumatology perspective, gender discrimination may be experienced as an ongoing social identity trauma perpetuated by family and social systems, continuously traumatizing and sensitizing women to other sources of stress or trauma (Kira, Hanaa, & Bujold-Bugeaud, 2015). Given the perinatal period may bring increased exposure to discrimination (Rosenthal et al., 2014), it may be important to examine this risk deriving from women’s larger social-ecological context. The current investigation aims to address these gaps by examining the joint contributions of psychological IPV exposure and gender discrimination to women’s mental health trajectories during the postnatal period.
Psychological IPV and Mental Health
When examining the role of experiencing psychological IPV in mental health, it is useful to note that there is not a widely accepted definition of psychological aggression or emotional abuse (terms often used interchangeably in literature), nor is there consensus on what level of aggression surpasses that threshold of “psychological abuse” (Jordan, Campbell, & Follingstad, 2010). However, there is general agreement that psychological IPV or psychological aggression consists of a wide range of intimate relationship behaviors or coercive actions intended to produce emotional harm or threat of physical harm. Furthermore, psychologically, aggressive acts can span from mildly coercive actions that occur occasionally in well-adjusted relationships to more comprehensive patterns of coercive domination and manipulation (e.g., ridiculing, berating, verbal threats, attempts to isolate, or control one’s partner; Jordan et al., 2010). There is evidence to support a distinct contribution of psychological IPV to mental health. Changes in psychological IPV have been associated with changes in depression and anxiety symptoms, even after controlling for the effects of physical IPV (Lawrence et al., 2009). Another study found that women exposed to psychological IPV alone had a higher probability of continued exposure to psychological IPV and lower possibility of recovery from depression symptoms over time, compared with women who experienced both physical and psychological IPV (Blasco-Ros et al., 2010). These studies highlight the gravity of psychological IPV as a problem, one that may carry particular weight during pregnancy and early parenthood due to the scope of potential impacts on mother and child. Physical IPV exposure has been related to adverse pregnancy outcomes (i.e., miscarriage, placental abruption, preterm birth, low birth weight, fetal death) and maternal mental health outcomes that include depression, anxiety disorders, posttraumatic stress disorder (PTSD), and substance use (Campbell, 2002; Coker et al., 2000; Howard et al., 2013; Stewart et al., 2017). Perinatal exposure to psychological IPV has been less thoroughly examined. Despite increased focus on the relationship between affective symptomatology and psychological IPV (Ahlfs-Dunn & Huth-bocks, 2014; Guyon et al., 2017; Huth-Bocks et al., 2013; Parrish, Lanier, Newby-Kew, Arvidson, & Shanahan, 2016), findings have been inconsistent on the strength of these relationships and the prevalence of negative outcomes (Howard et al., 2013; Stewart et al., 2017). Furthermore, while it is well established that perinatal exposure to IPV is associated with maternal depression (Flanagan et al., 2015; Martin et al., 2006; Tiwari et al., 2008), studies examining associations with other forms of perinatal affective symptomatology (i.e., perinatal anxiety and trauma symptoms) have been limited (Jaquier et al., 2015).
The majority of the perinatal IPV research reviewed above has focused mainly on symptom severity, yet longitudinal examination of symptom course may be crucial for understanding processes contributing to the well-being of both mothers and their children. Cross-sectional studies do not provide a complete picture of the impact of IPV, given that mental health problems associated with psychological IPV may persist long after cessation of abuse (Blasco-Ros et al., 2010). Prior research further suggests that it is not simply the severity of maternal affective symptoms but also their chronicity and timing that predict child developmental outcomes (Laurent et al., 2013; Deave, Heron, Evans, & Emond, 2008; Dunkel Schetter & Tanner, 2012). Thus, a longitudinal lens is needed to identify and ultimately intervene on perinatal IPV–related mental health risk.
Psychological IPV in a Social-Ecological Context—Gender Discrimination
In addition to taking a broader temporal perspective, it may be important to consider how experiences of victimization within intimate relationships are compounded by victimization at a larger social level. Drawing from Bronfenbrenner’s (1979) ecological system’s theory, social-ecological models of IPV incorporate attention to “the interconnectedness between risk factors on four levels: individual (e.g., history of violence); relationship (e.g., influence of one’s peers); community (e.g., social capital); and societal (e.g., sociocultural norms)” (Willie, Khondkaryan, Callands, & Kershaw, 2018, p. 241). Thus far, social-ecological models of IPV have largely focused on explaining a person’s risk of becoming a victim or perpetrator of IPV. In the current study, we extend this framework to better understand differential impacts of IPV exposure. In particular, we propose that we may learn more about forces driving perinatal mental health trajectories by examining the individual-level risk factor psychological IPV exposure in concert with risk deriving from women’s larger social-ecological context.
While there are various aspects of an individual’s social-ecological context that may help to understand differential impacts of IPV victimization (e.g., household income, social support), we propose that it may be beneficial to examine aspects that speak to women’s experiences of victimization at a larger societal level. A key risk spanning these social-ecological levels that has been shown to exacerbate mental health vulnerabilities is gender discrimination (Kira, Hanaa, et al., 2015; Klonoff, Landrine, & Campbell, 2000; Schmitt, Branscombe, Kobrynowicz, & Owen, 2002). Krieger (2014) defined discrimination as a “socially structured and sanctioned phenomenon, justified by ideology and expressed in interactions among and between individuals and institutions, that maintains privileges for members of dominant groups at the cost of deprivation for others” (p. 650). Within a context such as the United States, where women are considered the nondominant gender group, women may experience individual, institutional, or structural gender discrimination, comprising a range of micro-level insults (e.g., implicit and explicit insults to identity status and exclusions that constitute identity threats) and macro aggressions (e.g., vicarious knowledge of gender-based violence, rape, hate crimes, policies and social structures, and norms that perpetuate discriminatory attitudes and behaviors) across the life span (Kira, Hanaa, et al., 2015; Krieger, 2014). The perinatal period may bring increased exposure to gender discrimination through inequalities in the workplace (i.e., family leave policies, workplace discrimination, and conditions for breastfeeding women), societal and cultural norms (i.e., body policing, awareness of parenting gender norms), and shifts in interpersonal relationships (i.e., sexist overtures, individual experiences of gendered microaggressions related to pregnant or postpartum status). Thus, the perinatal period may represent a time in which victimization deriving from women’s larger social-ecological context (e.g., gender discrimination) is particularly salient. However, there is no research to our knowledge addressing possible synergistic effects of gender discrimination and psychological IPV in relation to perinatal mental health.
Gender discrimination has been associated with elevated psychological distress, depressive and anxious symptoms, and poorer physical health in nonperinatal women (Carliner et al., 2017; Kira, Omidy, et al., 2015; Klonoff et al., 2000). In addition, developmentally based trauma frameworks classify ongoing identity threats that emerge early in life without a foreseeable end, such as gender discrimination, as Type III continuous identity traumas (Kira, Hanaa, et al., 2015). According to this traumatology perspective, gender discrimination may be experienced as an ongoing social identity trauma perpetuated by family and social systems, continuously traumatizing and sensitizing women to other sources of stress or trauma (Kira, Hanaa, et al., 2015).
As a continuous identity trauma, the chronic stress associated with gender discrimination may deplete psychosocial reserves needed to cope with subsequent stressors, yielding more severe trauma-related mental health symptoms (Kira, Omidy, et al., 2015). Awareness and direct experiences of gender discrimination could also amplify IPV-related harm by reducing help-seeking behaviors. Gender discrimination has been associated with feelings of powerlessness, stigma internalization, and reduced self-efficacy (Kira, Omidy, et al., 2015), all of which have been found to interfere with help-seeking in women exposed to IPV (Overstreet & Quinn, 2013). Therefore, gender discrimination during the perinatal period may confer risk deriving from women’s larger social-ecological context that further sensitizes women to harmful mental health effects of psychological IPV. Understanding the joint contribution of these risk factors to women’s perinatal mental health trajectories may be important for developing interventions and policies that build resiliency in women exposed to IPV.
Current Study
As outlined above, critical gaps in our understanding of how psychological IPV contributes to perinatal mental health suggest that a broader consideration of both the longitudinal course of symptoms and the social-ecological context in which IPV occurs are necessary. The first objective of the current study was to examine the association between exposure to psychological IPV and the trajectory of women’s mental health (depression, anxiety, and trauma symptoms) following the birth of an infant. Our second objective was to assess whether gender discrimination exacerbates this association. In accordance with past IPV research, we hypothesized that greater exposure to psychological IPV across the perinatal period would predict greater severity and an increasing course of maternal depression, anxiety, and trauma symptoms from 3 to 18 months postnatal. Based on the proposal that gender discrimination may sensitize women to the impact of other forms of victimization, we hypothesized that these relations between psychological IPV exposure and mental health trajectories would be strongest for women experiencing high levels of gender discrimination.
Method
Participants
The data from the current study come from a larger longitudinal study of stress regulation in mother–infant dyads. A sample of 91 women were recruited from the Women, Infants, and Children (WIC) program and from other community agencies serving low-income families in a midsized predominantly European American city in the Pacific Northwest. Women were eligible to participate if they were 18 years or older, English speaking, and had an infant less than 12 weeks old. The majority of the mothers participating in the study were European American (76.9%), with 9.9% Latina American, 3.3% African American, 2.2% Native American, 3.3% Asian American, and 4.4% who indicated “other” as their race/ethnicity.
The majority of the sample (94.5%) reported being in a heterosexual relationship at the beginning of the study, and only a small proportion (7.2%) reported ending their relationship during the study period. A large proportion (74.7%) further reported exposure to mild or severe psychological IPV at some point in the study. Thus, the current sample largely represented women who were in a stable romantic relationship with a male partner that included at least some IPV exposure. A semistructured clinical interview (the NetSCID) administered at the first assessment further revealed substantial rates of psychological disorder for a community sample: 18.5% of mothers met criteria for current anxiety disorders (4.3% for a past anxiety disorder), 3.3% met criteria for a current major depressive episode (17.4% for a past major depressive episode), and 12% met criteria for PTSD. Of the 91 participants, 54 women (59.3% of the baseline sample) completed the final assessment. In comparison with completers, noncompleters were more likely to represent a higher risk group (i.e., younger, lower socioeconomic status, African American, more depression symptoms). An overview of participant demographics is in Table 1. For a more detailed description of study demographics and analyses of attrition characteristics, see Laurent (2017). Current analyses are based on the 76 participants who completed measures of both IPV and gender discrimination.
Sample Demographics (N = 91).

Procedure
Prior to study participation, mothers provided written informed consent for all study procedures, which were approved by the University of Oregon Institutional Review Board. When their infant was approximately 3 months old, mothers completed a set of online questionnaires that included sociodemographic questions and the self-report measures listed below. At this time, they also completed a home visit that involved a semistructured, computer-assisted diagnostic interview administered in person by a trained female graduate student. Mothers returned for laboratory visits when their child was 6, 12, and 18 months postnatal; at each time, they repeated the self-report questionnaire measures listed below.
Measures
Psychological IPV
At each study time, psychological IPV exposure was measured using the short form of the Revised Conflict Tactics Scale (CTS2S; Straus & Douglas, 2004). The CTS2S is a 20-item version of one of the most widely used tools in IPV research that has been validated against the full CTS2 scale and includes 10 subscales that assess both the participants’ and their partner’s perpetration of physical, sexual, and psychological aggression, as well as injury and use of negotiation tactics. Each subscale contains items measuring a severe and a mild form of aggression. At the initial visit (3 months postnatal), participants rated how many times in the past year their partner engaged in acts of physical, sexual, and psychological aggression. At each subsequent visit (6, 12, and 18 months postnatal), participants rated how many times since their last visit their partner engaged in acts of physical, sexual, and psychological aggression. Example items include the following: “My partner pushed, shoved, or slapped me” (physical, severe); and “My partner insulted or swore or shouted or yelled at me” (psychological, mild).
Responses are coded to create a binary variable for “prevalence” (0 = no instance of the behavior, 1 = one or more instances) as instructed in Straus and Douglas (2004). These prevalence variables are then used to create “severity” levels for each type of aggression: 0 = none, 1 = minor only, and 2 = severe. Example items include the following: “My partner pushed, shoved, or slapped me” (physical, severe); and “My partner insulted or swore or shouted or yelled at me” (psychological, mild). In the current study sample, 74.7% of women reported being a victim of psychological aggression at one or more time points during the study (49.0%-61.5% mild, 2.6%-8.7% severe across assessments). Despite lower prevalence of severe psychological abuse, the prevalence of mild psychological victimization in the current sample is of note, given increasing focus on cumulative effects of mild forms of victimization. Reported rates of other forms of victimization across assessments were lower (physical aggression/injury = 1.9%-9.0% mild, 0%-3.8% severe; sexual aggression = 3.8%-10.9% mild, 0% severe). Mean partner psychological aggression severity scores across the four times were used to assess women’s total psychological IPV exposure.
Per Straus and Douglas (2004), the subscales are not intended to be summed to obtain a total score; therefore, calculating internal consistency reliability is not appropriate. However, evidence for the concurrent and construct validity of the CTS2S, as measured by the correlation between the short form and full scales, has been established, ranging from .65 to .94 for being victimized by a partner who engaged in the behaviors assessed by the subscales (Straus and Douglas, 2004). Previous research shows support for the reliability and validity of the CTS long form across ethnic groups and gender (Cronbach’s alpha: physical = .86, psychological = .79; Stith et al., 2000; Straus and Douglas, 2004). While there is debate on the use of the CTS, Straus and Mickey (2012) found that the full-scale CTS has high sensitivity and construct validity supporting continued use of the CTS to investigate IPV in the lives of women. Given that evidence for the construct validity of the CTS2S, as measured by the correlation between the short form and full scale has been established, the CTS2S was used in the current sample to limit participant burden.
Gender discrimination
Starting at the second (6-month) assessment, gender discrimination was measured using a six-item scale that assessed participants’ perceptions of both micro- and macro-level experiences of gender discrimination (Schmitt et al., 2002). Representative items included “I have personally been a victim of sexual discrimination,” and “Prejudice against my gender group has affected me personally.” At each time point, participants were asked to rate their level of agreement with statements about exposure to gender discrimination and their experience as a woman, on an 8-point Likert-type scale (1 = strongly disagree to 8 = strongly agree). Ratings were averaged to yield total scores ranging from 1 to 7.83 (M = 2.48, SD = 1.60). Internal consistency reliability was adequate for this measure (α = .86-.93). Women’s mean gender discrimination scores across the four times were used to assess total gender discrimination exposure.
Anxiety
Anxiety symptoms were assessed at each time using the Beck Anxiety Inventory (BAI; Beck & Steer, 1993). The 21 items include affective (e.g., “unable to relax,” “fear of losing control”) and physiological (e.g., “numbness or tingling,” “feeling hot”) symptoms of anxiety. At each time point, participants rated how much they were bothered by each symptom in the past month on a 4-point scale (0 = not at all to 3 = severely) to yield total summed scores ranging from 0 to 28 (M = 8.17, SD = 6.83). Across assessments, 37.9% of participants scored at or above the clinical threshold for mild anxiety (8 or above), and 16.3% of the sample fell in the moderate to severe anxiety range (20 or above). Internal consistency reliability was adequate for this measure (α = .85-.93).
Depression
Participants reported depression symptoms at each time, using the Center for Epidemiologic Studies Depression Scale (CESD; Radloff, 1977). At each time point, participants rated the frequency of 20 symptoms of depression in the past week on a 4-point scale (1 = rarely or none of the time to 4 = most or all of the time). Total summed scores ranged from 0 to 44 (M = 9.51, SD = 8.34), with 19.9% of the sample scoring above the clinical threshold of 16 across assessments. Internal consistency reliability was adequate for this measure (α = .86-.89).
Trauma symptoms
At each time, trauma symptoms were measured by the Trauma Symptom Checklist–40 (TSC-40; Elliot & Briere, 1992). At each time point, participants rated the frequency of 40 symptoms in the past 2 months on a 4-point scale (0 = never to 4 = often). Symptoms tap multiple domains found to be affected by trauma exposure: anxiety, depression, sexual difficulties, and dissociation. Total summed scores ranged from 3 to 97 (M = 23.33, SD = 17.48). Internal consistency reliability was adequate for this measure (α = .92-.94).
Analytic Strategy
Hierarchical linear modeling (HLM) was selected to analyze effects of exposure to psychological IPV and gender discrimination on mothers’ mental health trajectories. This approach divides variability in the outcome into within-person and between-person components to obtain more accurate standard errors for testing regression coefficients. Furthermore, this approach allows for analysis of smaller sample sizes (N > 50) as levels of analysis within this approach are defined by the repeated measurement occasions nested within individuals. Anxiety, depression, and trauma symptoms were examined as unique outcomes in separate models. At Level 1, women’s symptoms were modeled with an intercept (β0, representing symptom severity level) and, if found to improve model fit, a temporal component (β1, representing the linear slope or course of symptoms). At Level 2, between-person differences in these trajectory components could be explained by adding hypothesized predictors. For illustration, the two-level equations testing (a) main effects of exposure to psychological IPV and gender discrimination, and (b) interaction effects of exposure to psychological IPV and gender discrimination on mothers’ anxiety symptoms are shown:
Level 1 model:

Level 2 model:
a)
b)
Results
Data Screening and Preliminary Descriptive Analyses
Table 2 presents descriptive statistics and correlations of study variables. Significant positive correlations between mean levels of gender discrimination, psychological IPV, and symptoms suggested preliminary support for hypothesized associations. However, correlations do not allow examination of symptom trajectories, which we examine below. Prior to model testing, variables that might need to be controlled to assess influences on symptom trajectories were examined; these included women’s psychiatric diagnoses and socioeconomic status (self-reported education and income levels) at the first study time. The only significant association was between PTSD and trauma symptom severity. The models for trauma symptoms therefore included PTSD diagnosis as a covariate.
Correlations Between Study Variables (Means Across Assessments).
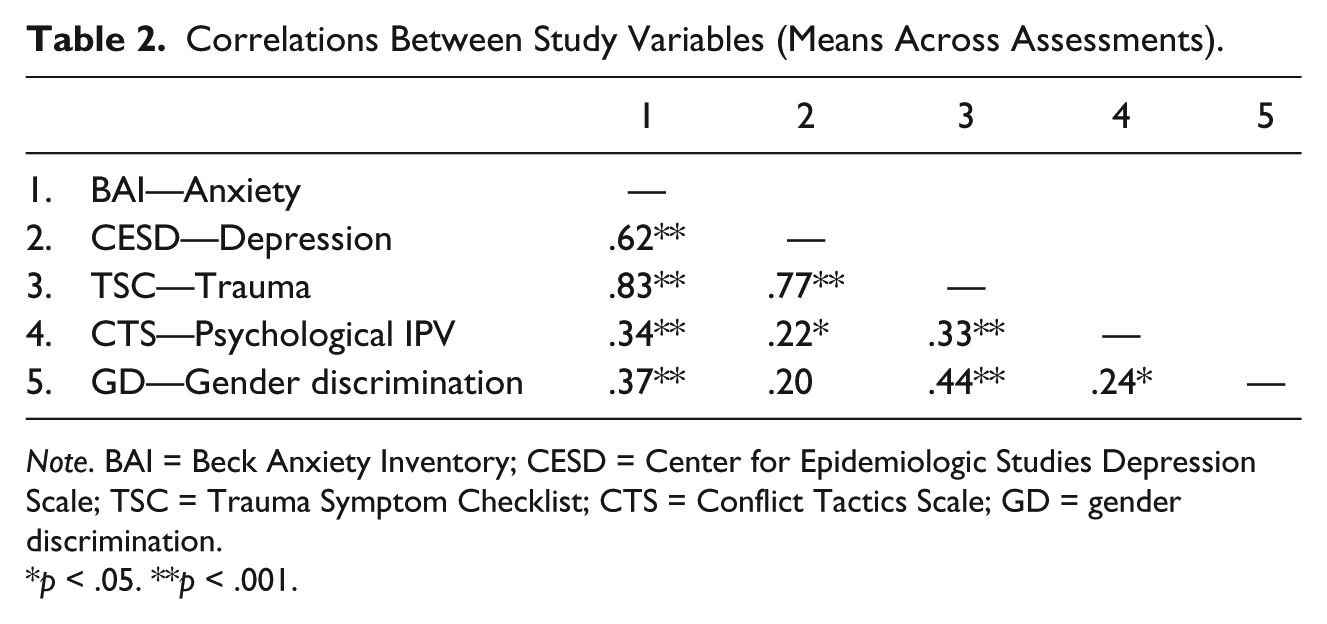
Note. BAI = Beck Anxiety Inventory; CESD = Center for Epidemiologic Studies Depression Scale; TSC = Trauma Symptom Checklist; CTS = Conflict Tactics Scale; GD = gender discrimination.
p < .05. **p < .001.
Baseline Models of Mental Health Trajectories
First, HLM models were fit without any explanatory predictors to describe participant anxiety, depression, and trauma symptom trajectories. For each outcome variable, the addition of a linear slope (representing the course of symptoms from 3 to 18 months) to a model that only included an intercept (representing symptom severity—levels at 18 months) resulted in improved fit to the data as evidenced by significant change in the deviance statistic: anxiety, χ2(3) = 9.44, p = .02; depression, χ2(3) = 17.98, p < .001; trauma, χ2(3) = 24.35, p < .001. For each outcome variable, there was nonsignificant improvement from linear to quadratic model. Nonsignificant average trajectory slopes indicated that symptoms did not change from 3 to 18 months postnatal in the sample as a whole. However, tau statistics demonstrated significant between-person variability in all model terms, χ2(75) = 244.74 to 366.65, p < .001, indicating heterogeneity in both symptom course and severity across participants. Predictor variables (mean levels of gender discrimination and psychological IPV exposure) were added at Level 2 to explain this variability. We tested (a) main effect models with exposure to psychological IPV and gender discrimination predicting symptom trajectories and then (b) moderation models with the interaction of exposure to psychological IPV and gender discrimination predicting symptom trajectories.
Explanatory Models: Main Effects of Psychological IPV Exposure and Gender Discrimination on Women’s Postnatal Mental Health Trajectories
To test the first study hypothesis, women’s mean levels of exposure to psychological IPV and gender discrimination were entered as predictors of their symptom trajectories. Psychological IPV exposure predicted a more negative slope term in the trauma symptom model, indicating that women reporting greater IPV showed a declining course of symptoms from 3 to 18 months postnatal (see Table 3, Part A). No other main effects of psychological IPV exposure were found. Gender discrimination was a significant predictor of the intercept term in the anxiety symptom model, indicating that women reporting greater gender discrimination showed greater symptom severity at 18 months postnatal. No other main effects of gender discrimination were found.
Associations Between Psychological IPV, Gender Discrimination, and Mental Health Trajectories.
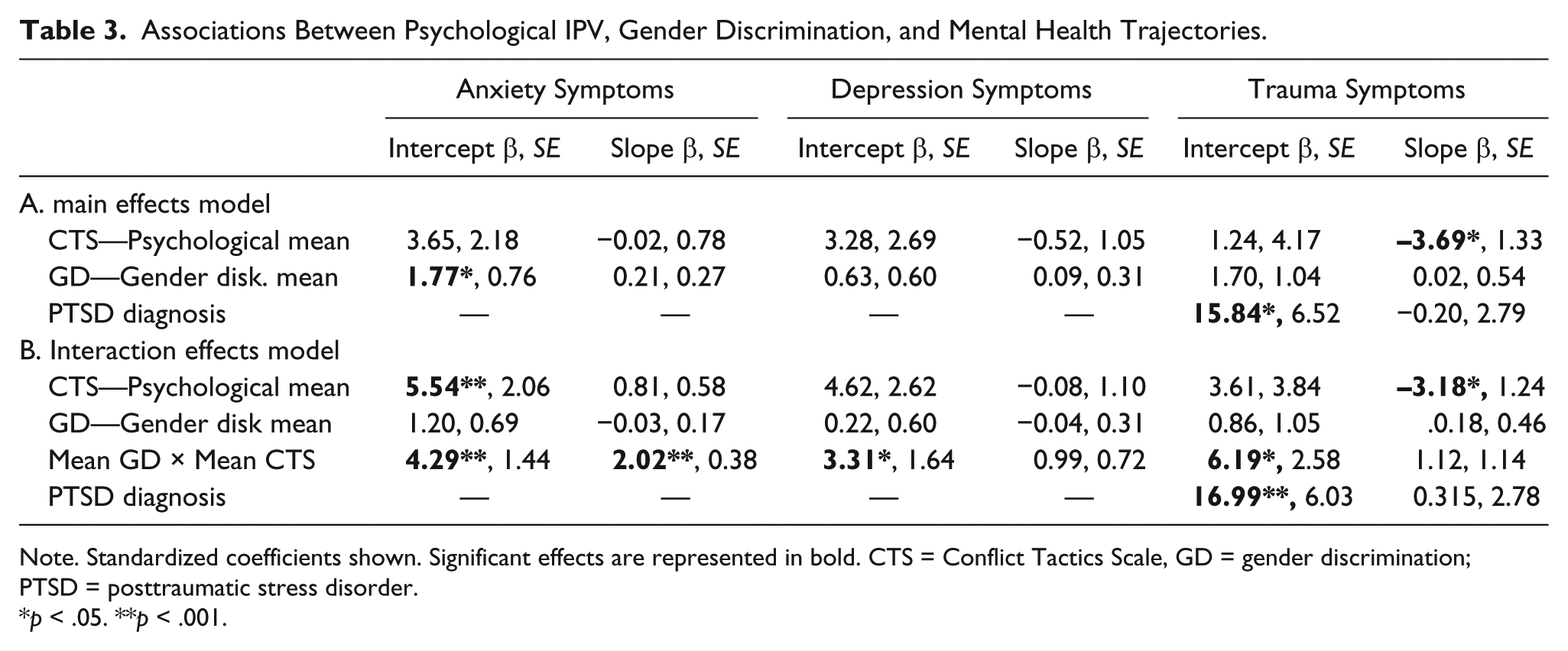
Note. Standardized coefficients shown. Significant effects are represented in bold. CTS = Conflict Tactics Scale, GD = gender discrimination; PTSD = posttraumatic stress disorder.
p < .05. **p < .001.
Explanatory Models: Gender Discrimination × Psychological IPV Exposure Effects on Women’s Postnatal Mental Health Trajectories
To test the second study hypothesis, interactions between women’s mean levels of exposure to psychological IPV and gender discrimination were added as predictors of their symptom trajectories. Gender discrimination was found to moderate the effect of psychological IPV on anxiety symptom trajectories, with the interaction significantly predicting both the intercept and slope (see Table 3, Part B). This model explained 23.4% of the variance in participants’ intercepts and 60.0% of the variance in slopes. The interaction was also a significant predictor of the intercept in both the depression and trauma symptom models (see Table 3, Part B), explaining 16.8% and 39.9% of the variance in depression and trauma symptom severity, respectively. In each case, a positive interaction coefficient was consistent with a synergistic effect of psychological IPV and gender discrimination on women’s final symptom severity and/or the course of symptoms from 3 to 18 months postnatal. Figure 1 illustrates effects on each symptom outcome, with predicted symptom trajectories plotted at high (+1 SD) and low (−1 SD) values of psychological IPV and gender discrimination exposure.
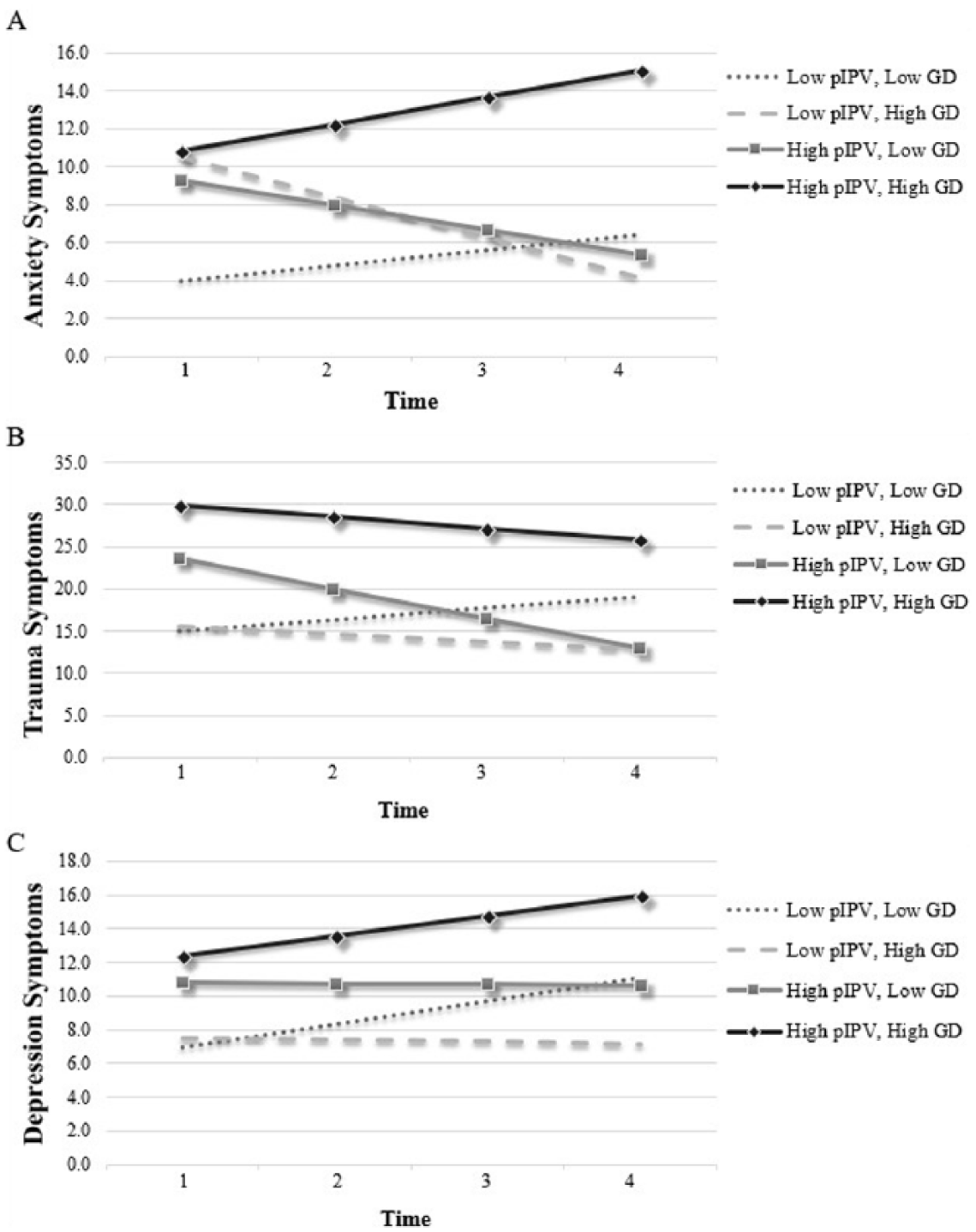
Women’s predicted affective symptom trajectories from 3 to 18 months postnatal at high and low levels of reported psychological IPV and gender discrimination.
Regions of significance—that is, the range of gender discrimination at which the effect of psychological IPV was significant—were calculated using Preacher et al.’s (2006) online utility to further probe the meaning of these interaction effects. These calculations indicated that for mothers experiencing moderate to high levels of gender discrimination (53rd percentile and above), psychological IPV exposure significantly predicted more severe anxiety symptoms by the end of the study (with nonsignificant IPV effects at lower ranges of gender discrimination). The effect on anxiety symptom slopes similarly revealed that for mothers with moderate to high gender discrimination scores (65th percentile and above), psychological IPV exposure significantly predicted a more steeply increasing symptom course. At the lower end of gender discrimination (38th percentile and lower), the opposite was true. Analyses for the depression symptom outcome showed that for mothers with moderate to high gender discrimination scores (39th percentile and above), psychological IPV exposure significantly predicted more severe symptoms (with nonsignificant IPV effects at lower ranges of gender discrimination). Finally, we found that for mothers with high gender discrimination scores (80th percentile and above), psychological IPV exposure significantly predicted more severe trauma symptoms (with nonsignificant IPV effects at lower ranges of gender discrimination). Supplemental material is available online for further illustration of the regions of significance findings.
Summary
Results are consistent with the proposal that exposure to psychological IPV can have a negative impact on women’s postnatal mental health, at least under certain conditions. In the context of moderate to high levels of gender discrimination only, increasing psychological IPV predicted poorer mental health—elevated anxiety, depression, and trauma symptom severity at 18 months postnatal, as well as an increasing course of anxiety symptoms from 3 to 18 months. Several effects in the opposite direction for symptom slopes—main effect of psychological IPV for trauma, effect in the context of low gender discrimination for anxiety—appeared to reflect a capacity for victimized women to at least partially recover from initially high levels of postnatal symptoms.
Discussion
The current study aimed to extend what is known about the effects of IPV by incorporating a social-ecological framework that accounts for the possible moderating influence of gender discrimination on the role that exposure to psychological IPV plays in women’s postnatal mental health trajectories. The present findings provide partial support for our hypotheses; although perinatal exposure to psychological IPV did not independently predict mental health difficulties, it did so in the context of women’s experiences of gender discrimination. Below, we consider specific findings and their implications.
Support for the hypothesized main effect of psychological IPV on women’s mental health during the postnatal period was limited; on its own, exposure to psychological IPV was only a significant predictor of the course of trauma symptoms. Contrary to hypotheses, women who were exposed to psychological IPV experienced relative improvement of symptoms in comparison with those with lower exposure. To interpret this finding, we must take into account the fact that there were no IPV-related differences in symptom severity by the end of the study period, which means that exposed women appeared to be recovering from higher initial trauma symptoms. The period surrounding the birth of a child is thought to be a particularly high-risk time for IPV victimization (Bhandari et al., 2008) due to increased stress, unintended pregnancy, and/or relationship dissatisfaction (Parrish et al., 2016). It is possible that women in more abusive relationships experienced an exacerbation of abuse during pregnancy/early postpartum that caused a spike in trauma-related symptoms around the birth of the baby, followed by some alleviation as the immediate stresses of childbirth receded. The current study design—which only began monitoring IPV and symptoms at 3 months postnatal—does not allow an investigation of such possibilities, and future research should employ a wider longitudinal lens to further illuminate perinatal IPV risk pathways.
Hypotheses regarding synergistic effects of psychological IPV and gender discrimination on women’s postnatal mental health were more fully supported, underlining the importance of a social-ecological lens that considers multiple layers of women’s social context. The present findings indicate that the experience of gender discrimination in tandem with IPV places women at greater risk of experiencing mental health difficulties during the postnatal period. These results are consistent with the conceptualization of gender discrimination as a form of continuous identity trauma that exacerbates other mental health vulnerabilities (Kira, Hanaa, et al., 2015). Specifically, we found that women exposed to high levels of both gender discrimination and psychological IPV experienced greater anxiety, depression, and trauma symptom severity. In addition, anxiety symptoms for these women worsened across the postnatal period. Women reporting high levels of exposure to either psychological IPV or gender discrimination alone, on the contrary, tended to experience greater anxiety symptom severity at baseline followed by some symptom improvement. It may be that the experience of either of these two chronic stressors in isolation offers more room for recovery as women adjust to the new stresses of raising an infant, whereas the combination of the two prevents recovery and fuels a vicious cycle of escalating symptoms.
To understand the root of such difficulties, it is useful to acknowledge the perinatal period as a time in which women must adapt to increased demands on their emotional, social, and economic resources. This means that reductions in social support and increases in stress—both of which may be signified by reports of IPV and gender discrimination—should be especially consequential for women’s well-being during this time. As introduced earlier, these combined risks could cumulatively deplete women’s psychosocial reserves and/or reduce help-seeking behaviors to fuel a range of affective symptoms. In line with this explanation, Bhandari et al. (2008) found that families with multiple stressors were at greatest risk of negative outcomes after exposure to IPV. Having greater access to reliable social support systems beyond the immediate family (as in the case of women reporting lower levels of gender discrimination), however, may serve as a protective factor against the deleterious effects of psychological IPV.
It is notable that the synergistic effects of gender discrimination and psychological IPV were particularly robust for anxiety symptom trajectories. It is possible that the mental health mechanisms affected by gender discrimination and psychological IPV are most closely aligned with those driving anxiety, as opposed to trauma and depression symptoms. According to the tripartite model of anxiety and depression (Clark & Watson, 1991; Craske et al., 2009), physiological hyperarousal and an elevated sensitivity to distal threat (e.g., hypervigilance) discriminate anxiety from depression. Threats posed by an abusive partner and/or a larger environment of discrimination may contribute to chronic hyperactivation of cognitive and neurophysiological stress response systems implicated in anxiety. Future research should examine whether psychological IPV and/or gender discrimination preferentially disrupt the regulation of such systems.
The current study highlights the importance of examining perinatal mental health longitudinally to capture the nature of risk pathways. Cross-sectional analysis or targeted focus on symptom levels in the earlier postpartum period could have provided a misleading picture of the consequences of IPV—that is, no clear added harm of dual IPV and gender discrimination. The present findings support continued investigation of longer term effects, particularly because more chronic or escalating perinatal symptoms have been shown to carry distinct costs for psychophysiological stress regulation in both mothers (Laurent et al., 2018) and children (Laurent et al., 2011; Laurent et al., 2013). Our findings, which point to harmful effects of perinatal intimate victimization specifically in the context of broader social victimization (i.e., gender discrimination), further underscore the importance of expanding current conceptualizations of IPV impacts to incorporate relevant aspects of the social-ecological context.
Further limitations of the current study should be used to guide future research in this domain. Our ability to fully characterize the perinatal period was restricted by the recruitment of women postpartum, and it will be important to prospectively examine symptoms beginning in or prior to pregnancy to define perinatal risk paths. Given psychological IPV victims are at high risk of poly-victimization (Dillon et al., 2013), it will also be important to examine perinatal poly-victimization patterns (e.g., psychological IPV only, psychological and physical IPV, sexual IPV only) and whether these play unique roles in women’s mental health outcomes. Limitations in sample size and diversity (i.e., predominantly low-income European Americans) suggest caution is warranted in generalizing effects to the broader population. Women who experience both IPV and poverty are at higher risk for depression, PTSD, and other forms of emotional distress (Goodman et al., 2009). Therefore, efforts to examine the costs of IPV should include larger samples of women from diverse socioeconomic backgrounds to determine how these different risks may work together.
While the current study contributes to our understanding of the synergistic effects of gender discrimination and psychological IPV on perinatal mental health, our ability to identify implications based on specific experiences of gender discrimination is limited, given the lack of specificity of the current study measure. Future work may benefit from a more in-depth analysis of gender discrimination that assesses both frequency and nature of experiences. Discrimination should also be measured at multiple levels (e.g., individual, institutional, cultural, vicarious experiences of discrimination) separately, rather than collapsing across these levels of discrimination as in the current study measure. In addition, the current study focuses solely on gender discrimination. Future work should draw upon intersectionality theory, which would suggest that women do not experience gender discrimination in isolation of other social identities (Crenshaw, 1989; Sterzing, Gartner, Woodford, & Fisher, 2017). Next steps in this research should thus also include more women from marginalized backgrounds and measure discrimination experiences across multiple identity levels (e.g., gender, racial, sexual orientation).
Finally, the pervasive effects of psychological IPV and gender discrimination on women’s anxiety outcomes in this study suggest more emphasis should be placed on measuring and predicting perinatal anxiety symptoms. The current study measure of anxiety allowed us to examine physiological symptoms of anxiety, thus providing discriminant validity from depression, but it offered less information about the cognitive components of anxiety symptoms (e.g., worry). Future incorporation of more comprehensive measures of anxiety domains and mechanisms may provide important information about symptom typologies in women exposed to perinatal IPV.
Study Contributions and Implications
Previous research has failed to adequately address the contribution of psychological IPV to perinatal mental health. Our findings highlight the adverse impact of psychological IPV (as opposed to the more commonly studied physical IPV) and the role of gender discrimination as a moderating factor that may help explain some of the heterogeneity of effects observed in the literature. These findings speak not only to the harm exerted by these combined forms of victimization, but also to the potential for healing through micro- and macro-level changes to the social context. The present findings suggest that gender discrimination is a relevant social-ecological risk factor during the perinatal period. Our results further suggest that women who experience one risk factor (e.g., elevated levels of either gender discrimination or psychological IPV) may benefit the most from additional support directly after the birth of an infant, whereas women who are exposed to multiple risk factors may need more ongoing support to build stable psychosocial reserves and alleviate distress. Therefore, efforts by women’s health agencies and providers to identify women who may need extra support may benefit from incorporating screenings not only for psychological IPV exposure, but also for social-ecological stressors such as gender discrimination.
Understanding the joint contribution of these factors to women’s perinatal mental health trajectories can inform interventions and policies that help women exposed to IPV. Such efforts might involve incorporating social justice and/or feminist theory frameworks into IPV intervention programs, establishing connections across service providers who observe different aspects of risk, and advancing policies that advocate empowerment of pregnant women and new mothers. Finally, these results suggest that the scope of IPV-related mental health risks extends beyond more commonly assessed depression symptoms, and primary and secondary prevention efforts should incorporate screenings for perinatal anxiety and trauma symptoms. It is our hope that a better understanding of when and how victimization harms women’s perinatal mental health will help inform solutions that benefit not only the women themselves but also subsequent generations and thereby society as a whole.
Supplemental Material
Supplemental_Figures_2_(1) – Supplemental material for Synergistic Effects of Psychological Intimate Partner Violence Exposure and Gender Discrimination on Postnatal Mental Health Trajectories
Supplemental material, Supplemental_Figures_2_(1) for Synergistic Effects of Psychological Intimate Partner Violence Exposure and Gender Discrimination on Postnatal Mental Health Trajectories by Danyelle N. Dawson, Vanessa V. Volpe, and Heidemarie K. Laurent in Journal of Interpersonal Violence
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Society for Research in Child Development Victoria Levin Award and the University of Oregon College of Arts and Sciences. The funding sources had no role in the study design, data collection and analysis, or submission process.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.