
Abstract
Adolescents’ involvement in bullying is associated with both sleep and mental health problems, but the nature of this association remains unclear; further, its association with academic outcomes has received little attention. Thus, the aims of the current study were to (a) determine whether involvement in bullying as a victim, bully, or bully-victim was associated with greater sleep and mental health problems and (b) explore the potential mediating effect of sleep and mental health problems on the association between bullying and academic outcomes. A large 2012 population-based study in Hordaland County, Norway, surveyed 10,220 adolescents (16-19 years; 54% girls) about bullying involvement using the revised version of the Olweus Bully/Victim Questionnaire, detailed sleep assessment, and mental health questionnaires. Academic outcomes were obtained from official administrative registries. 1.7% of the adolescents (n = 156) reported being victims of bullying, 1.0% (n = 92) reported being a bully, and 0.5% (n = 50) reported being a bully-victim. All categories of bullying involvement had higher rates of mental health problems compared with adolescents not involved in bullying. Victims reported more symptoms of anxiety and depression, whereas bullies reported higher rates of conduct problems. Adolescents in all bullying categories also reported significantly shorter sleep duration and higher prevalence of insomnia as well as lower grade point average (GPA) compared with adolescents not involved; however, school absence was not associated with bullying involvement. Bullying involvement and GPA showed complete mediation for bullies and bully-victims and partial mediation for victims through sleep duration, conduct problems, and symptoms of depression and attention deficit hyperactivity disorder (ADHD). Bullying is strongly associated with mental health and sleep problems, in addition to lower academic performance. Findings support the importance of addressing bullying involvement during this important developmental period.
Introduction
Experiencing bullying is prevalent during the school years, with a declining rate from early childhood to late adolescence (Kretschmer, Veenstra, Dekovic, & Oldehinkel, 2017; Tochigi et al., 2012). Still, a survey of adolescents from 40 countries found that a sizable number of adolescents experience bullying (Craig et al., 2009), but the prevalence rates vary according to methodology and across countries (Cook, Williams, Guerra, & Kim, 2009).
Bullying is related to a range of negative health outcomes, (Moore et al., 2017) and this holds true both for those who experience bullying (the victims), for those who perform bullying behavior (the bully), and for those who have a double role; the bully-victim (Herge, La Greca, & Chan, 2016; Moore et al., 2017; Veenstra et al., 2005). Specifically, sleep problems and short sleep duration are prevalent in adolescence (Clarke & Harvey, 2012). A recent meta-analysis concluded that there was a strong link between peer victimization and sleep problems (van Geel, Goemans, & Vedder, 2016). However, most studies have focused on victims of bullying, whereas less is known about sleep in the other bullying roles. There are some notable exceptions, including a Scottish study of 5,420 adolescents with a high rate of insomnia symptoms among victims, bullies, and bully-victims between 11 to 17 years of age (Hunter, Durkin, Boyle, Booth, & Rasmussen, 2014). A higher rate of insomnia as well as bedtime fears were also found among victims and bully-victims in comparison with those not involved in bullying among eight hundred eighty seven 14 to 17-year-old high school students (Donoghue & Meltzer, 2017). Similarly, all the groups of bullying involvement were at higher risk of sleep problems compared with noninvolved adolescents in a study of high school students in China (Zhou et al., 2015). In contrast, a Greek study that included children and adolescents aged 10 to 18 years demonstrated that some sleep problems were specific for different bullying roles; irregular sleep patterns and short sleep duration were more frequent among bullies, while insomnia symptoms were more often reported by bully-victims (Kubiszewski, Fontaine, Potard, & Gimenes, 2014).
The association between bullying involvement and sleep may be specific to certain developmental levels, as indicated in a recent meta-analysis in which the association between peer victimization and sleep was stronger for the younger age groups (van Geel et al., 2016). Some studies have not found this association in the high school years, (Tochigi et al., 2012) and this may be related to the higher rate of bullying in younger years. In contrast, sleep patterns undergo major changes from early childhood through late adolescence, with the rate of sleep problems increasing, (Sivertsen, Harvey, Pallesen, & Hysing, 2017) and sleep duration becoming shorter (Hysing, Pallesen, Stormark, Lundervold, & Sivertsen, 2013). Thus, the association between bullying and sleep needs to be addressed specifically in late adolescent samples. Another concern with previous studies is that they have often assessed sleep problems using a single item and crude measures (Biebl, DiLalla, Davis, Lynch, & Shinn, 2011). Few have assessed insomnia according to diagnostic criteria, and a good measure of sleep duration is rarely included. A further concern is that both victims and bullies are more likely to be from a low socioeconomic status (SES) background (Tippett & Wolke, 2014) and a social gradient is also demonstrated in adolescents’ sleep (Hysing, Petrie, Boe, Lallukka, & Sivertsen, 2016), thus, adjusting for SES is important.
The association between bullying and mental health problems is more established. Mental health problems are higher among those involved in bullying compared with noninvolved peers across a range of mental health indicators (Cook, Williams, Guerra, Kim, & Sadek, 2010; Lereya, Copeland, Zammit, & Wolke, 2015; Olweus & Breivik, 2014). Still, there are differential patterns of mental health problems between bullies, victims, and bully-victims. Victims have been shown to have more internalizing problems (especially anxiety and depression) than their peers (Copeland, Wolke, Angold, & Costello, 2013; La Greca & Harrison, 2005; Landoll, La Greca, Lai, Chan, & Herge, 2015; Siegel, La Greca, & Harrison, 2009). In contrast, bullies are more often characterized by externalizing problems (such as conduct problems and antisocial behavior; Copeland et al., 2013; Fanti & Kimonis, 2012), and bully-victims are likely to have both internalizing and externalizing problems (Cook et al., 2010).
With respect to academic outcomes, experiencing bullying as a victim, bully, or bully-victim is associated with poor school achievement (Cook et al., 2010; Juvonen, Wang, & Espinoza, 2011; Kowalski & Limber, 2013). Bullying involvement may be directly related to school performance or potentially mediated by known risk factors for reduced school performance, such as mental health problems (McLeod, Uemura, & Rohrman, 2012). Short sleep duration may be another likely mediating mechanism, given that sleep deprivation is associated with learning and memory difficulties, and confirmed by the association between sleep and grade point average (GPA) in the adolescent years (Hysing, Harvey, Linton, Askeland, & Sivertsen, 2016). To our knowledge, factors that may mediate the association between bullying involvement and academic outcomes among adolescents have not been previously examined.
Based on the above considerations, the aims of the current study were to further investigate the association between bullying involvement, sleep and mental health problems, and school performance during late adolescence. Specifically, the study addressed conceptual and methodological gaps in previous studies by including all aspects of bullying involvement (i.e., bully, victims, and bully-victims), obtaining adolescents’ GPA from registers as an objective academic outcome, and using a comprehensive sleep measure that assessed both sleep duration and symptoms of insomnia. Furthermore, the current study extended prior research by evaluating the potential mediating effect of sleep and mental health problems on the association between bullying involvement and academic outcomes.
Method
Procedure
This population-based study used data from the youth@hordaland-survey of adolescents in Hordaland County in Western Norway. All adolescents born between 1993 and 1995 were invited in 2012 to reach all adolescents in late adolescent and high school age. The main aim of the survey was to assess the prevalence of mental health problems and service use in adolescents. Adolescents in upper secondary education received study information via e-mail, and one classroom school hour was allocated for completing the questionnaire. Those not in school received information by postal mail to their home address. The questionnaire was web-based and covered a broad range of mental health issues, daily life functioning, use of health care and social services, and demographic characteristics, as well as a request for permission to obtain school data and to link the information with national health registries and parental reports on a corresponding questionnaire. Uni Research Health collaborated with Hordaland County Council to conduct the study.
Sample
All adolescents born between 1993 and 1995 were invited (N = 19,430) to participate during the first months of 2012, of which 10,220 agreed, yielding a participation rate of 53%. All sleep variables were manually checked for validity with subjects providing obvious invalid responses being omitted from further analyses. Invalid responses included (a) sleep onset latency (SOL) or wake after sleep onset (WASO) more than 12 hours, (b) SOL + WASO longer than time in bed (TIB), and (c) negative values of sleep duration and sleep efficiency. This resulted in 374 adolescents (3.7%) being omitted. Among the 9,846 remaining adolescents, 1,499 (15.2%) did not give consent to link their data to the official register on school absence, thus yielding a sample size of 8,347 for the linked data set.
Instruments
Sociodemographics
Gender and date of birth was identified through personal identity number in the Norwegian National Population Register. Exact age was estimated by calculating the interval of time between date of birth and date of participation. SES was assessed by both maternal and paternal education, reported separately with three response options: “primary school,” “secondary school,” and “college or university.”
Bullying
Bullying was measured by two global questions from the revised version of the Olweus Bully/Victim Questionnaire (OBVQ); one question on being bullied by peers (bullying victimization) and one question on bullying peers (bullying perpetration) (Solberg & Olweus, 2003). The revised version of the OBVQ contains a definition or explanation of bullying which precedes the two global questions. The explanation is designed to capture all three main elements of the definition of bullying: the intention to harm the victim, the repetitive nature of bullying, and the imbalance in power between the victim and the perpetrator(s). A shorter version of the explanation of bullying was used in the present study. The question on being bullied (“How often have you been bullied at school in the past couple of months?”) and bullying peers (“How often have you taken part in bullying another pupil(s) at school the past couple of months?”) had five response alternatives: “I haven’t been bullied/bullied other students at school in the past couple of months,” “only once or twice,” “‘2 or 3 times a month,”’ “about once a week,” and “several times a week.” By combining the two global questions, adolescents were divided into four groups: bullies, victims, bully-victims, and noninvolved (Solberg & Olweus, 2003; Boulton & Smith, 1994). OBVQ is one of the most widely used bully questionnaires in the world and has shown generally favorable psychometric properties (Solberg & Olweus, 2003; Olweus, 2013).
Sleep measures
Adolescents’ self-reported usual bedtime and rise time were indicated in hours and minutes using a scroll down menu; data were reported separately for weekdays and weekends using a consensus sleep diary (Carney et al., 2012). TIB was calculated as the difference between bedtime and rise time. SOL and WASO were indicated in hours and minutes, and sleep duration was defined as TIB minus SOL and WASO. Sleep efficiency was calculated as sleep duration divided by TIB multiplied by 100 (reported as percentage; higher scores reflecting greater sleep efficiency). Subjective sleep need was reported in hours and minutes, and sleep deficit was calculated separately for weekends and weekdays by subtracting total sleep duration from subjective sleep need. This measure has been used in previous studies (Hysing et al., 2013).
Insomnia was operationalized according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) criteria for insomnia. Difficulties initiating and maintaining sleep (DIMS) were rated on a 3-point Likert-type-scale with response options “not true,” “somewhat true,” and “certainly true.” If confirmed (i.e., “somewhat true” or “certainly true”), adolescents were then asked how many days per week they experienced problems either initiating or maintaining sleep. Adolescents also provided information on the duration of DIMS. A joint question on tiredness/sleepiness was rated on a 3-point Likert-type-scale with response options “not true,” “somewhat true,” and “certainly true.” If confirmed, adolescents then reported the number of days per week they experienced sleepiness and tiredness, respectively. To meet the DSM-5 criteria for insomnia, adolescents had to report DIMS at least 3 times a week, with a duration of 3 months or more, as well as tiredness or sleepiness at least 3 days per week.
Mental health problems
Depression symptoms were measured using the short version of the Mood and Feelings Questionnaire (SMFQ) (Angold et al., 1995). The SMFQ consists of 13 items focusing on cognitive and affective symptoms rated on a 3-point Likert-type-scale. The Norwegian translation of the response categories corresponds to the original categories of “not true,” “sometimes true,” and “true.” The SMFQ has been found to have high internal consistency and essential unidimensionality in a population-based study (Sharp, Goodyer, & Croudace, 2006) and a study based on the sample from youth@-hordaland (Lundervold, Breivik, Posserud, Stormark, & Hysing, 2013). Cronbach’s alpha for the SMFQ in the current study was .91.
Anxiety symptoms were measured using the short five-item version of the Screen for Child Anxiety Related Emotional Disorders (SCARED) (Birmaher et al., 1999). This version consists of the five indicators that discriminate best between anxious and non-anxious children, assessed by a comprehensive symptom checklist for all Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) diagnoses. Furthermore, it has shown similar psychometric properties to the 41-item SCARED (Birmaher et al., 1999). Cronbach’s alpha for the five-item SCARED in the current study was .69.
Attention deficit hyperactivity disorder (ADHD) symptoms were measured using the World Health Organization adult ADHD Self-Report Scale (ASRS) (Kessler et al., 2005). ASRS consists of 18 items: nine items measure symptoms of inattention and 9 items measure symptoms of hyperactivity–impulsivity. Symptoms are rated on a 5-point Likert-type scale ranging from “never” to “very often.” The ASRS has shown high internal consistency and construct validity when used with adolescents (Adler et al., 2012). Cronbach’s alpha for the ASRS in the current study was .91.
Conduct problems were measured using the Youth Conduct Disorder (YCD) instrument, consisting of eight items which are part of the Diagnostic Interview Schedule for Children Predictive Scales (DPS) (Lucas et al., 2001). The DPS scale has been shown to accurately identify adolescents who are at high probability of meeting diagnostic criteria for conduct disorder. Cronbach’s alpha for the YCD in this study was .79.
Academic outcomes
GPA
Official registers from Hordaland County provided information on academic grades. In Norway, secondary schools use a scale from 1 to 6, with 6 as the highest grade (outstanding competence), 2 (low level of competence) as the lowest passing grade, and 1 as failure. GPA was calculated as the average of the student’s grades for the last semester.
School attendance
Official register-based data on school nonattendance were provided by Hordaland County Council, and included both days and school hours of absence for the last semester (6 months).
Representativeness
Compared with national and regional statistics provided by the Norwegian Directorate for Education and Training (2014), the mean GPA of all mandatory courses for adolescents in the current study (mean 3.57) was identical to the national GPA in 2012 in this age cohort (mean 3.57) but slightly lower than the GPA in the Hordaland county (mean 3.61) (Hysing et al., 2016).
Ethics
The study was approved by the Regional Committee for Medical and Health Research Ethics (REC) in Western Norway. In accordance with the regulations from the REC and Norwegian health authorities, adolescents aged 16 years and older can make decisions regarding their own health (including participation in health studies), and thus gave consent themselves to participate in the current study. Parents/guardians have the right to be informed, and in the current study, all parents/guardians received written information about the study in advance. School attendance were the official reports from the registers of Hordaland County. The registry data were linked to the youth@hordaland-survey for participants who consented to participate in the study as a whole (including school registry information) or specifically consented to the use of their registry information.
Statistical Analyses
Independent samples t tests and chi-square tests were used to examine differences in demographic variables and school absence and school performance. For comparison of mental health problems (SMFQ, ASRS, YCD, and SCARED) and sleep duration (on weekdays and weekends) across the four groups of bullying involvement we used Analysis of covariance (ANCOVA), estimated marginal means (EMM) adjusting for age, gender, and parental education. The mental health scales were standardized and Cohen’s d effect sizes were calculated.
The association between bullying involvement (i.e., being a bully, a victim, or a bully-victim vs. no involvement) and GPA was further examined by estimating a structural equation model, allowing for mediation by sleep duration; conduct problems; and symptoms of anxiety, depression, and ADHD. Analyses controlled for age and sex. Separate analyses were conducted for each of the bullying involvement groups, comparing them with the noninvolved participants. The variance inflation factor (VIF) for the mediators ranged from 1.05 to 1.60, well below the recommended cut-off VIF > 10 for structural equation modeling (SEM) analyses (Kline, 2016). All analyses were conducted using the robust maximum likelihood estimator and missing data were handled by full information maximum likelihood (FIML). Indirect effects were investigated using the built-in function IND in Mplus. A significant mediation effect was determined using 95% bias-corrected bootstrap confidence interval (Mackinnon, Lockwood, & Williams, 2004). The standardized effect sizes are reported.
The t tests, chi-square tests, ANCOVA, and multiple regression analysis (to obtain VIF) were conducted using of IBM SPSS statistics version x. Mplus (Version 8) was used for the mediation analyses (Muthén & Muthén, 2017).
Results
Bullying Involvement
In all, 1.7% of the adolescents (n = 156) reported being victims of bullying, while 1.0% (n = 92) reported being a bully, and 0.5% (n = 50) reported being a bully-victim. The large majority (96.8%, n = 8,940) of the adolescents had not been involved in bullying behavior or been the target of bullying the last months. As detailed in Table 1, all three categories of bullying involvement were more prevalent among boys than girls (p < .001). The adolescents’ age and parental education were not significantly associated with bullying status.
Demographic Characteristics by Bullying Involvement in the youth@hordaland Survey.
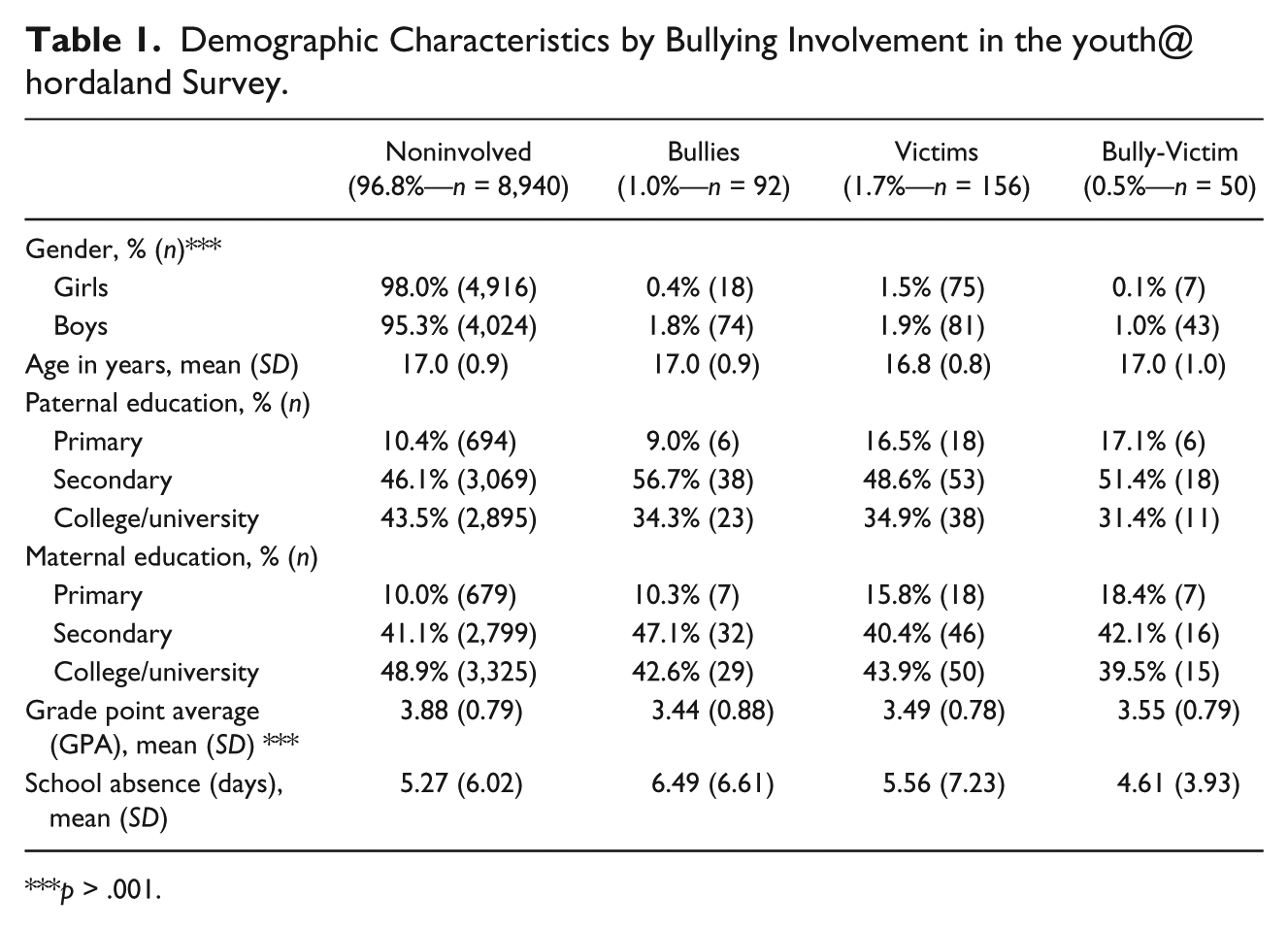
p > .001.
Bullying Involvement and Mental Health Problems
Figure 1 displays the EMM of mental health problems in standardized t scores by bullying involvement status, as well as Cohen’s d effect sizes (compared with noninvolved). Both victims, bullies and bully-victims, reported more symptoms of depression compared with adolescents not involved in bullying. The highest level of depression was found for victims (d = 1.1) and bully-victims (d = 1.0). The same pattern was observed for symptoms of anxiety, but with smaller effect sizes (see Figure 1 for details). In contrast, bullies had significantly higher levels of conduct problems (d = 1.4), followed by bully-victims (d = 0.8). Victims of bullying did not score higher on conduct problems than the noninvolved group. In terms of symptoms of ADHD, all three categories of bullying involvement scored higher in the ASRS scale (ds from 0.5 to 0.7) than noninvolved adolescents, but the bullying involvement groups did not differ significantly from each other.

EMM of mental health problems in standardized t scores by bullying involvement.
Bullying Involvement and Sleep Problems
Figure 2 displays the sleep duration by bullying involvement. Both victims (5:44 hours), bullies (5:31 hours) and bully-victims (5:26 hours), reported significantly shorter sleep duration on weekdays compared with adolescents not involved in bullying (6:26 hours). A similar pattern was observed for weekend sleep duration (see Figure 2). The prevalence of DSM-5 insomnia was highest in victims of bullying (36.5%), but also elevated in bullies (27.2%) and bully-victims (26%) compared with adolescents not involved in bullying (18.2%; p < .001).

EMM of sleep duration on weekdays and weekends by bullying involvement.
Bullying Involvement and Academic Outcomes
Victims, bullies, and bully-victims had lower GPAs compared with adolescents not involved in bullying, with medium effect sizes (d = 0.49, d = 0.56, and d = 0.42, respectively). However, the three bullying categories did not differ significantly from each other (see Table 1). Days of school absence were not significantly associated with bullying involvement.
Mediation Analyses
The possible mediating effects of sleep duration and symptoms of mental health problems on the association between bullying involvement status and GPA were investigated. For all three groups, the mediation analysis showed significant indirect effects through sleep duration, symptoms of depression, and symptoms of ADHD, but not through symptoms of anxiety (see Figures 3, 4, and 5). For victims, there was no significant indirect effect through conduct problems (see Figure 3). Furthermore, the direct effect from victim to GPA was significant, suggesting partial mediation for the victims. In contrast, there were significant indirect effects on GPA also through conduct problems for bullies and bully-victims (see Figures 4 and 5, respectively). However, for these two groups, the direct effect was not significant, suggesting complete mediation by sleep and mental health on the association between being a bully or a bully-victim and GPA. The correlations between the mediator variables for the mediation analysis involving victims are shown in Table 2. Very similar correlations (not shown) were found in the mediation analyses involving bullies and bully-victims (see Figure 3b and 3c, respectively).
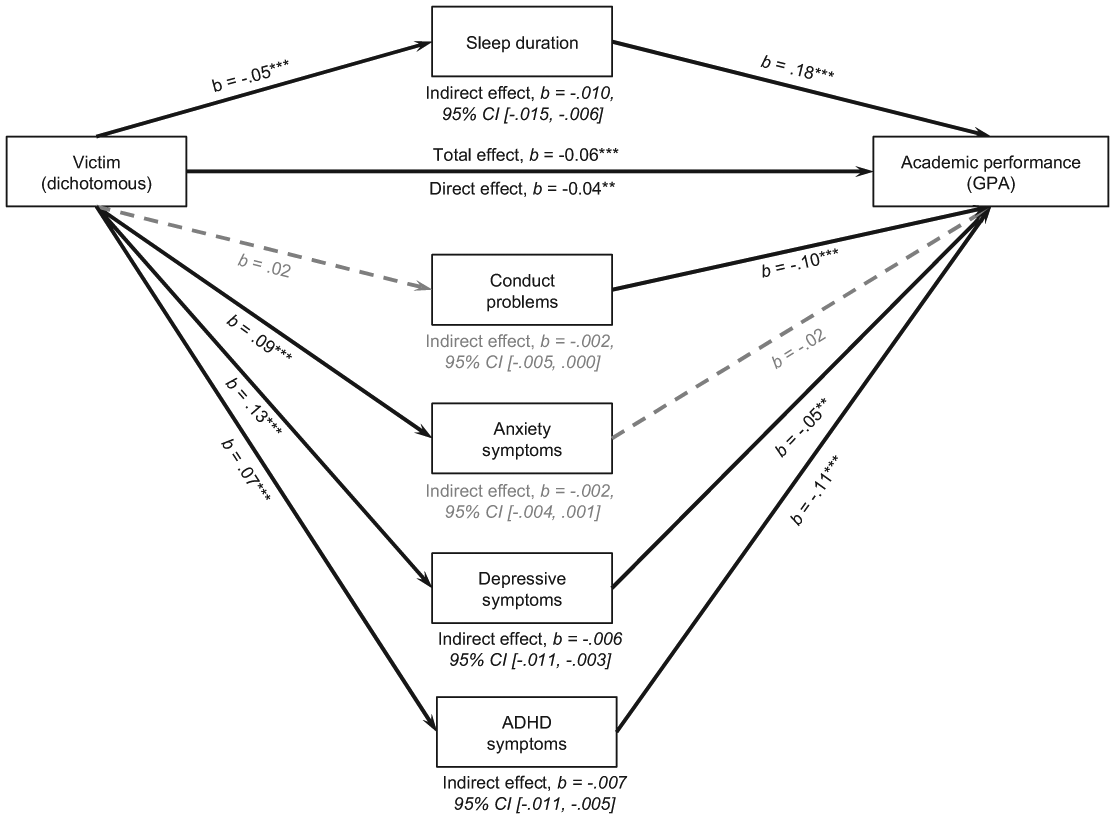
Model of victim as a predictor of GPA, mediated by sleep duration, conduct problems, symptom of anxiety, depression and ADHD, adjusted for age and sex.

Model of bully as a predictor of GPA, mediated by sleep duration, conduct problems, symptoms of anxiety, depression and ADHD, adjusted for age and sex.

Model of bully-victim as a predictor of GPA, mediated by sleep duration, conduct problems, symptoms of anxiety, depression and ADHD, adjusted for age and sex.
Correlations Between the Mediator Variables for Victims.
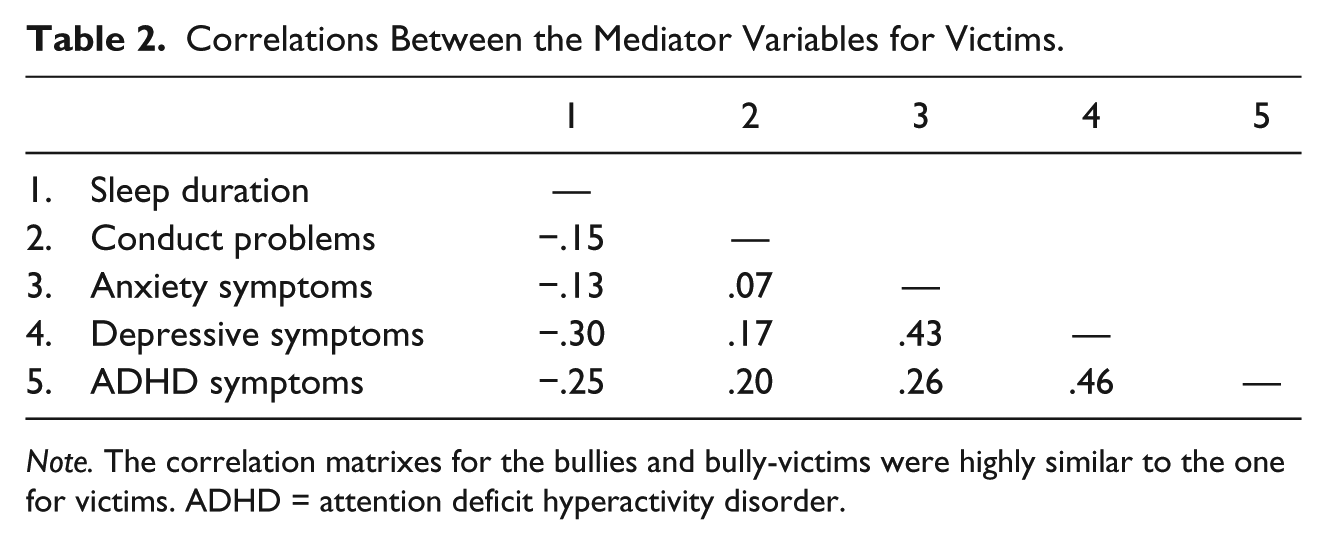
Note. The correlation matrixes for the bullies and bully-victims were highly similar to the one for victims. ADHD = attention deficit hyperactivity disorder.
Discussion
In the present large-scale population-based study of Norwegian adolescents, bullying involvement was relatively infrequent, with 1.7% of the adolescents reported being victims, 1% reported bullying others, and 0.5% reported both categories. Adolescents involved in bullying across the different roles had, in general, higher rates of mental health problems compared with adolescents not involved in bullying. While victims reported more symptoms of anxiety and depression, bullies had higher rates of conduct problems. All three categories had significantly shorter sleep duration and higher prevalence of insomnia as well as lower GPA compared with adolescents not involved in bullying. The bully-GPA link and bully-victim GPA link were fully mediated by sleep and mental health problems (except anxiety), while the victim-GPA link was partially mediated by the same variables.
The overall results suggest that even if the rate of bullying involvement in this age cohort is low in Norway, which is in accordance with the prevalence for the national pupil survey, (Kretschmer et al., 2017) the consequences for those involved are substantial. This point was demonstrated by the strong associations between bullying involvement and both sleep and mental health problems, as well as reduced academic achievements. While the rate of bullying was similar to other Norwegian data, it is still lower than many international estimates (Cook et al., 2009; Craig et al., 2009). The Health Behaviour in School-aged Children (HBSC) study comprising pupils from 40 countries study using a similar definition of bullying as the presents showed that the prevalence rates of bullying and victimization in Norway was lower than in many other countries (Craig et al., 2009). The lower prevalence in Norway and other Nordic countries may be a result of the high awareness of school bullying at the societal level as well as differences in national policy and implementation of interventions programs against bullying. The governmental response to bullying in Norway includes, compulsory annual pupil surveys in in three grade levels as well as increasing the responsibility of schools using the national Education Act.
The reliance on school registry data precludes us from conclusions regarding rates of bullying of adolescents who are not in school, and this may have impacted the relatively low level of bullying. The present study focused on the rate of bullying involvement in the general school population and did not specifically focus on high-risk groups, due to limited statistical power. The participants in the youth@hordaland-survey are a diverse group with regard to for instance gender, SES, and ethnicity (Hysing et al., 2016; Skogen, Boe, Sivertsen, & Hysing, 2018). We acknowledge that there might be some groups such as adolescents from minority groups (Hansen, Melhus, Hogmo, & Lund, 2008) others may be more at risk of for instance or homophobic bullying (Poteat, Mereish, DiGiovanni, & Koenig, 2011). Thus, the rate and the possible associations between bullying and school outcomes should be specifically addressed in such groups in future studies.
The expected differential patterns of mental health problems across bullying involvement was partly confirmed with higher externalizing problems for bullies and internalizing problems being more frequent for victims. While conduct problems were more frequent among adolescents that had bullied others, depressive symptoms and anxiety were higher among all groups compared with their noninvolved peers, with the highest rates among the victims. The ADHD symptoms were higher across all types of bullying involvement in comparison with peers. Although ADHD may be expected to be related to conduct problems, and thus be more frequent among those who bully others, ADHD symptoms in this age group are closely related to depressive symptoms and internalizing problems as well, and thus may explain the lack of differences across the bullying involvement groups (Lundervold, Hinshaw, Sorensen, & Posserud, 2016). Interestingly, bully-victims did not report more symptoms of mental health problems compared with the bullies and victims, which are in contrast to previous studies describing bully-victims as a particular risk group (Copeland et al., 2013). This discrepancy could be due to the age of the present sample, as it is possible that the most troubled bully-victims are no longer present in school by late adolescence.
Victims, bullies, and bully-victims all reported more sleep problems than peers, with shorter sleep duration and more insomnia. These results are in accordance with a meta-analysis suggesting more sleep problems among victims of bullying (van Geel et al., 2016), and previous studies—that have confirmed an increased rate of sleep problems across bullying involvement (Donoghue & Meltzer, 2017; Kubiszewski et al., 2014; Zhou et al., 2015). The results are particularly important as they further extend previous findings by confirming the bullying/sleep problem association using multiple insomnia criteria (i.e., not limited to a single item assessment of sleep). This finding may be especially relevant for adolescents given the high rate of insomnia in this age group (Hysing et al., 2013). Similarly, the inclusion of short sleep duration, another hallmark of adolescent sleep problems, may also be age appropriate. Thus, the use of developmentally appropriate sleep measures in the present study might be one of the reasons why we found strong associations between bullying involvement and sleep problems, whereas prior literature suggested that this association might be weaker in adolescents than in younger children, (van Geel et al., 2016) or perhaps not present at all (Tochigi et al., 2012).
The present study confirmed the functional impact associated with adolescents’ involvement in bullying, finding lower GPAs among the adolescents involved in bullying compared with peers, in line with previous studies of younger students (Juvonen et al., 2011). For the adolescents that bullied others and the bully-victims, the association between bullying and GPA was mediated fully by sleep duration and mental health problems across all categories except anxiety. In contrast, though a similar pattern was present for victims of bullying concerning sleep duration, depression, and ADHD, there was no mediation effect through conduct problems and a direct association between being bullied and having a lower GPA persisted. This suggests that there might be additional pathways to lower GPA for the victims, for instance through self-esteem (Tsaousis, 2016). Interestingly, the association between bully status as a bully-victim and GPA more closely resembled that of bullies compared with victims. This might be due to the total effect between bully status and GPA being smaller for this group, as the sum of indirect effects was smaller for bully-victims compared with victims, despite the significant indirect effect through conduct problems. Thus, conduct problems seem especially important to understand the association between bullying status and GPA for the bully-victim group. The results underscore the importance of a broad approach in understanding adolescent bullying involvement and school achievement. The interplay between sleep and externalizing (Hysing, Lundervold, Posserud, Sivertsen, 2015) and internalizing problems (Clarke & Harvey, 2012), as well as the interplay between sleep, bullying, and mental health over time (Biebl et al., 2011; Chang et al., 2017) suggest that sleep problems, mental health difficulties, and poor school functioning should be considered and evaluated when adolescents are involved in bullying. It was somewhat surprising that victims of bullying did not have higher absence rates compared with the other groups, as previous studies have identified victimization and being bullied as risk factors for school absence (Juvonen, Nishina, & Graham, 2000). Still, it is possible that these associations are more pronounced in younger age groups, as our findings are in line with a previous study of adolescents (Kowalski & Limber, 2013).
Overall, the strengths of the present study are the broad and detailed assessment of sleep problems and mental health, in addition to the inclusion of victims of bullying, bullies, and bully-victims. Furthermore, the use of administrative registries on academic performance and school attendance reduces the risk of informant bias for these analyses. Nevertheless, there are study limitations that should be noted. All data on sleep and mental health were obtained by self-report, and thus the lack of clinical interviews restricts information on clinical diagnosis. Although self-reported sleep parameters, including SOL and WASO typically differ from those obtained from objective assessments, (Lauderdale, Knutson, Yan, Liu, & Rathouz, 2008) recent studies have showed that such self-report sleep assessments can be recommended for the characterization of sleep parameters in both clinical- and population-based research (Zinkhan et al., 2014). Also, the accuracy of self-reported SOL and WASO are generally better among adolescents than in older adults, (Dillon et al., 2014) and a study of young adolescents in Hong Kong found good agreement between actigraphy measured and questionnaire reported sleep durations (Kong et al., 2011).
The generalizability of the study may be limited to one county in Norway, although the distribution of urban and rural areas in this county reflects that of Norway as a whole. In particular, the mean GPA of study participants was identical to the mean GPA for Norway, suggesting that the sample may be representative of adolescents in Norwegian schools. Due to school records being one of the outcomes in the present study the results are restricted to those who had been in school the last year. The cross-sectional nature of the study precludes conclusions regarding temporal order, and longitudinal studies are needed to increase the understanding of the interplay between sleep, bullying involvement, mental health, and school performance over time.
The present study confirms that bullying involvement is an infrequent but serious condition in late adolescence. For those involved (as victims, bullies, or both), all show more sleep problems, mental health problems, and lower academic performance than their peers. Further studies should investigate whether these associations also are present for young adults. Interventions targeting late adolescent age groups should consider a broad perspective including both mental health and sleep and their school performance.
Footnotes
Acknowledgements
We want to thank the Bergen Child Study group and most importantly we are grateful to all participants that made this study possible
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.