
Abstract
Intimate partner violence (IPV) is a worldwide social issue perpetrated by intimate male partners against their wives. Studies on IPV have generated accurate comparative information since the 1993 World Conference on Human Rights and the Declaration on the Elimination of Violence Against Women to guide strategy and track progress in attempts to comprehend the IPV issues. In many attempts to understand violence against women, the social construction of IPV was not well documented in the literature. This article aims to explore IPV survivors’ social construction of IPV by analyzing the experiential narratives of IPV survivors. To address the objective, this article used the phenomenological approach by examining the lived experiences of 15 IPV survivors. Our study finds that IPV made IPV survivors empowered, and with this social construction, survivors were able to overcome violence perpetrated by their intimate partners. The findings further proved that giving preferential attention to the needs of IPV victims could lead to victim empowerment, a factor needed in the elimination of violence against women and children in all forms. It is suggested for any intervention activities to (a) ultimately address the empowerment of individuals and (b) respond to the needs of individuals because what may work for one victim may not work for another.
Keywords
Introduction
Intimate partner violence (IPV) is a global social problem mostly perpetrated by intimate male partners against their wives (United Nations University—International Institute for Global Health, 2018). Issues range from the physical and mental health of women, economic productivity, and cultural traditions to human rights (James-Hawkins, Salazar, Hennink, Ha, & Yount, 2019; Sarkar, 2008; Shay-Zapien & Bullock, 2010). Since the 1993 World Conference on Human Rights and the Declaration on the Elimination of Violence Against Women (Devries et al., 2013), studies on IPV have produced reliable comparative data to guide policy and monitor progress in efforts to understand the problem of IPV, eliminate violence, and treat IPV victims. For example, Alzoubi and Ali (2021) and Fulu and Miedema (2015) reported that (a) IPV was perpetrated mainly by male partners against their female counterparts, (b) IPV was found in societies where gender roles were unequal and among families with low socioeconomic status living in disadvantaged neighborhoods, and (c) male intimate partners were usually unemployed. Some of the reasons cited were household mismanagement, infidelity, child neglect, nonsubmission to husbands (Boy & Kulczycki, 2008), religious convictions, and traditions (Kposowa & Aly Ezzat, 2019; Takyi & Lamptey, 2020). Other researchers have reported on the phenomenon of victim blaming, the social construct in which women choose to remain in the abusive relationship, internalizing victimization, refusal to accept social and professional support (Gracia & Lila, 2015), and the influence of sociocultural norms and traditions in the perpetration of IPV (James-Hawkins et al., 2019; Jesmin, 2015a, 2015b; Yount et al., 2016).
Studies using the social construction theory of violence have placed the discussions between the two poles of a dyad, that is, the perpetrator and the victim dyad. On the perpetrator side, researchers have focused on the justification for and circumstances of violence by perpetrators and the impact of violence on victims’ well-being (Bosco, Schneider, Coleston-Shields, Higgs, & Orrell, 2019; Cannon & Buttell, 2016; Dalton, Jung, & Willis, 2017; Kaye, Mirembe, Ekstrom, Bantebya, & Johansson, 2005; Mehrotra, 1999; Muehlenhard & Kimes, 1999; Salter, 2016). On this side of the dyad, studies have examined perpetrators’ construction of violence, which is founded on hegemonic masculinity, and concluded that manliness is associated with assertiveness, aggressiveness, independence, dominance, and violence (Bhana & Mayeza, 2016; Bozkurt, Tartanoglu, & Dawes, 2015; Taylor, das Nair, & Braham, 2013). Anwary (2015) detailed how hegemonic masculinity is sanctioned in Bangladesh to protect the masculine image, and punish anyone who attempts to emasculate men. In a study in South Africa, researchers debunked the idea that the school playground is a free space for students to play; rather, the school playground articulates the dominant ideal of hegemonic masculinity rooted in violence (Bhana & Mayeza, 2016). However, some researchers warn that there is no universal model of masculinity, but rather a “heterogeneous diversity of male identities and ways of being men in human societies” (Fernández-Álvarez, 2014, p. 48). A similar argument was posited in the classic work by Badinter (1992).
Studies on the victim’s side of the dyad have focused on attitudinal factors and the role of the community in the perpetration of violence against women. In a study by Jesmin (2015), the results revealed that women living in communities with permissive attitudes toward wife beating were more likely to justify the acts of husbands beating their wives. According to this study, women who married at an early age, had a low level of education, belonged to poor households, and had no access to information appeared to be at higher risk of justifying wife beating. A much earlier work reported that if wife abuse is deemed necessary, it should happen under legitimate circumstances, with legitimate causes and legitimate reasons, and within the tolerable limits of the community (Rao, 1997).
The IPV literature is mostly filled with results from the Americas, the Middle East, Europe, Africa, and Asia (Boonzaier, 2008; Fujiwara, Yamaoka, & Kawachi, 2016; Gage & Thomas, 2017; Gracia & Lila, 2015; Mehrotra, 1999; Perova & Reynolds, 2017). These studies have examined hegemonic masculinity and IPV, the role of social capital in the prevention of abuse, socioeconomic factors of abuse, and attitudinal factors toward abuse, including attitudes of police authorities. There have been very few or quite limited reports on IPV in the South Asian region, particularly in the Philippines. In addition to reports by the Philippine Statistics Authority (PSA), developments in IPV have been reported by Tsai, Cappa, & Petrowski (2016), Fehringer and Hindin (2014), and Mandal and Hindin (2014). Tsai investigated the relationship between IPV and contraception use, concluding that the use of contraception is significantly higher for women who have experienced physical and/or sexual violence. Fehringer and Hindin described the context of and motivations for female- and male-perpetrated IPV in Cebu, Philippines, arguing that motivations on the perpetration of violence differed by gender, with women using force for self-defense whereas men acting out of dominance and control. Mandal and Hindin posited that IPV is passed intergenerationally by presenting evidence that children who witnessed IPV in childhood would subsequently use IPV in later life.
However, no studies exploring the social construction of IPV have been conducted in the Philippines. This is a gap in the research that this article aims to pursue. To bridge this gap, this article aims to explore IPV survivors’ social construction of IPV by analyzing the experiential narratives of IPV survivors. This aim is undertaken by analyzing research participants’ (RPs) lived experiences as IPV victims, police blotter reports of IPV incidents, and other documents pertaining to IPV in the Philippines. This article aims to examine this issue in the following sections: an explanation of social construction theory and its application to IPV, the methodology adopted in this study, the findings and discussion of the results, and finally, the conclusion and insights.
Do Social Constructs on IPV Influence the Victims’ Perceptions of Their Social Processes?
Hörl’s theory of the social construction of violence is founded on “selective perceptions that grow out of . . . special positions in society” (Hörl, 2007 p. 37). These selective perceptions can be placed at two different perception levels: individual and community. For the former, the perceived constructs for spousal violence were the following: victims’ perceptions of masculinity and femininity and victims’ attitudes toward violence, the economic activities of wives and spousal duties, infidelity, and the mismanagement of households (Alzoubi & Ali, 2021; Barnett, Maticka-Tyndale, & Kenya, 2016; Hatcher et al., 2013). These constructs underscored that men should rule and subjugate women, and these constructs were maintained because of men’s dominant position in society. For the latter, the fulfillment of social expectations by women was the major construct for IPV, including negligence in performing domestic duties, nonsubmission to male authority, nonfulfillment of spousal duties, and inappropriate public display of behavior (Barnett et al., 2016; Laisser, Nyström, Lugina, & Emmelin, 2011). Subjugating women, submission to male authority, and the imposition of masculine rule are major component concepts of masculinity in which the achievement of masculinity is founded on violence (Demetriou, 2001). Feminist researchers posited that in societies where the patriarchal system is imposed, there is the protection of the masculine image, women are demeaned, and anyone who attempts to emasculate men is sanctioned (Anwary, 2015). Within this scope, abuse becomes legitimate and within legitimate bounds (Rao, 1997). Because this theory is based on “selective perceptions,” different perceptions may exist. It is, therefore, important to explore the dyad in the social construction of IPV between perpetrators and victims as well as the reciprocal relations involved (Hörl, 2007).
Studies investigating the perpetrator side of the dyad have considered IPV a serious public health problem and a violation of women’s human rights (Devries et al., 2013) that should be prevented. These studies have examined the deleterious effects of IPV on women’s reproductive health and outcomes for pregnancy (Sarkar, 2008), the fetus and the victims’ extended family (Shay-Zapien & Bullock, 2010), the mental health of victims, and the sexual transmission of infectious diseases (Dillon, Hussain, Loxton, & Rahman, 2013). Clinical studies have associated detrimental emotional, psychological, and social well-being (Ali, Mogren, & Krantz, 2013); aggressive behavior of children (Holmes, 2013; Levendosky, Bogat, & Martinez-Torteya, 2013); abortion; and unintended pregnancies with IPV (Pallitto et al., 2013). Researchers have reported that male intimate partners refused to acknowledge the perpetration of violence because they perceived violent acts as men’s prerogative because men either acted in self-defense against a threat posed by their wives (Catlett, Toews, & Walilko, 2010; Dworkin, Colvin, Hatcher, & Peacock, 2012) or performed a duty as protectors of their wives and families (Boonzaier, 2015). However, some studies report that some cultures do not share these findings (Salter, 2016).
Sociocultural studies have drawn their conclusions from the many preexisting harmful local practices and traditions that contribute to the social construction of IPV. For example, Draper (1992) and Boonzaier (2015) claimed that IPV has its roots in sociocultural conventions for example, gender inequality, male supremacy and dominance, and power relations. In a study by Helman and Ratele (2016), IPV begins in the family where male domination is encouraged, including behavioral control (Lelaurain et al., 2018). Controlling women in almost every aspect leads to their marginalization, making them less empowered by offering them few opportunities to participate in decision making (Barchi, Winter, Dougherty, & Ramaphane, 2018). Women are made to bear the heavy burden of production and reproduction, and limited access to education and livelihoods is afforded to them. This marginalization is the outcome of discrimination, patriarchal attitudes, economic inequality, gender inequality, and violence tolerance.
The underlying theme of the many studies on the perpetrator side of the dyad shows evidence of hegemonic masculinity. These studies indicate that superiority and authority are anchored in dominance, aggression, and violence (Anwary, 2015). In some studies, abuse is even legitimized or legitimated by societies that welcome this form of masculinity (Bhana & Mayeza, 2016).
Studies of the victim side of the dyad have directly addressed victims’ perceptions of violence (Hörl, 2007) to define the context and perceptions of abuse (Mehrotra, 1999), to find ways of improving empowerment (Bosco et al., 2019), and to design empowerment programs for both batterers and victims (Catlett et al., 2010). Some contexts of IPV situate abuse as “fighting” that occurs normally within the conjugal abode as a means to settle disputes and differences (e.g., infidelity and disrespect to husbands; Kaye et al., 2005). Another context views IPV as a normal phenomenon that occurs in every family and requires no intervention from any parties (Odero et al., 2014). Some contexts construe women as passive and helpless and as needing to be dominated and protected by men (Boonzaier, 2008). The context that construes women as helpless and passive involves the acceptance of male supremacy, with which feminist researchers disagree. For feminist researchers, abuse of women is an outcome of permissive societies where abuse is considered legitimate and encouraged in some circumstances (Bhana & Mayeza, 2016). Therefore, attempts to implement strategies to prevent any form of abuse require comprehension of the context of abuse (Li, Levick, Eichman, & Chang, 2015). Some studies have reported that responses aimed at preventing abuse have created confusion among victims (Dichter, 2013) because victims perceive their actions as self-defense, expressions of anger, and ultimate acts to end violence (Stuart et al., 2006). Finally, in studies recommending programs for empowering IPV victims, the theory of social construction suggests that to reduce IPV, interventions should (a) ultimately address the empowerment of individuals to allow them to make informed choices and (b) respond to the victim’s needs because what may work for one victim may not work for another (Lanier & Maume, 2009).
In the Philippines, violence against women has been reported to be present in all regions of the country (PSA, 2013) and has affected the lives of many women. In a report by the PSA (2017), the percentage of women who experience physical, sexual, and/or emotional violence decreases slightly with age. In this report, women who were divorced, separated, or widowed were more likely to have experienced all forms of violence by their recent partner compared with married or cohabiting partners. Factors of these abusive acts were identified, and researchers have reported findings consistent with studies on male-perpetrated IPV in other developing countries, suggesting similar dynamics of male IPV perpetration (Fehringer & Hindin, 2014). The outcome of abusive treatment results in absolute surrender to the husband’s authority (Tsai, Cappa, & Petrowski, 2016). However, no studies exploring the social construction of IPV have previously been conducted in the Philippines.
Method
The data used in this article were taken from the project “Social Capital and Resilience of Intimate Partner Violence (IPV) Victims in Cebu City, Philippines.” The project was conducted from 2016 to 2017 using a phenomenological approach with 15 female RPs who were all IPV survivors selected through snowball sampling. The project sought to classify and examine the victims’ personal experiences as IPV victims to support different stakeholders who were embarking on projects for the welfare of IPV victims and its social support structure on the different levels of their disclosure. Specifically, the project dealt with the experiences of the RPs on the following contexts: their perception on themselves before and after the abuse and their informal support structure, their perceptions on intimate violent acts, and cohabitation history and relational experiences with their intimate partners.
The RPs and the Recruitment Procedure
Initially, the recruitment of RPs was facilitated by a police station’s women’s desk officer on duty. RPs met the following criteria: the victim’s residential address was available to facilitate personal interviews, the type of violence was reported, surviving abuse, the victim’s personal background, and the extent of victim disclosure recorded in the police blotter journal. Successive RPs were recruited through the snowball approach (Ellard-Gray, Jeffrey, Choubak, & Crann, 2015). Prior informed consent (PIC) was given to all RPs prior to the actual interview sessions. Majority of the RPs were legally married females (93%), with the remaining 7% in cohabiting arrangement, underwent counseling from local nongovernmental organizations (NGOs; 67%), and did not sever the marital union (73%). The average age of RPs was 39.87 years. They had lived in an abusive relationship for an average of 13.67 years and had an average of four children. All the RPs belonged to the lower income bracket, and were IPV survivors.
Data and Collection Procedure
The primary data collected were interview transcripts of survivors of IPV. These data were the narrated personal experiences of survivors, including the processes and strategies used in victimization. Face-to-face interviews lasted approximately 45 to 60 min each and were nonstructured and free form. A total of 20 interview transcripts were collected from these interview sessions. At the RPs’ request, interview sessions were held in private and in the local language, Cebuano. According to the RPs, the subject of intimate violence was considered a personal matter and could not be disclosed to persons outside their trust circles. Therefore, the interviews began when trust was established and full cooperation was guaranteed. Interview sessions were conducted with an individual trusted by the RP, labeled the referrer. Although referrers had knowledge of the topic, they were not consulted during the actual interview or allowed to provide input on the topic, except when consulted by the researchers to avoid data or information cleansing or setting the precedent for proxy interviews. The topics discussed were provided in advance for approval by the RPs, and the topics that were rejected were not discussed. Topics discussed revolved around cohabitation history and relational experiences with their intimate partner, perceptions on the quality of cohabitation before and after the abuse, history of disclosure and help-seeking strategies, and strategies used to survive the crises. The topics not discussed revolved around the type of IPV specifically on the sexual abuse and relational assessment with the intimate partner. Secondary data were the publicly communicated official reports, NGO performance reports on IPV cases, technical reports, and policy papers.
Data Analysis Procedure
In the data analysis, the thematic approach was used. All personal information from the interview transcripts was removed to maintain confidentiality. The final approved version was then loaded to Atlas.ti8 software for qualitative data analysis (QDAS). Documents loaded to QDAS were referred to as primary documents (PDs). A total of 10 PDs were loaded to QDAS. The researchers followed a three-phase procedure in the analysis: The first phase was the reading of the entire transcripts to identify the overarching theme; the second phase was the coding and memoing of the narratives using the QDAS with respect to the categories identified; and the final phase was the drawing of interactions between codes and memos. As an outcome of this three-phase procedure, researchers were able to draw two categories: (a) perceptions of violence, victimization, and its impact on the victims; and (b) help-seeking strategies and the means employed to survive IPV.
Ethics and Consent
The study received research clearance from the Research and Development Council of the Cebu Technological University, Cebu City, Philippines. PIC forms were individually given to RPs prior to the actual interview.
Results
RPs claimed that IPV made them empowered individuals. This construct was substantiated with the self-perception of being tough and the perception of indifferent assistance. The former was the outcome of silence from neighbors and isolation; the latter category came from the perception that health care givers and duty providers were indifferent to their situations, and initiatives were rendered useless. These subjective claims are presented in Table 1.
The Survivors’ Social Construction of IPV With Sample Narratives.
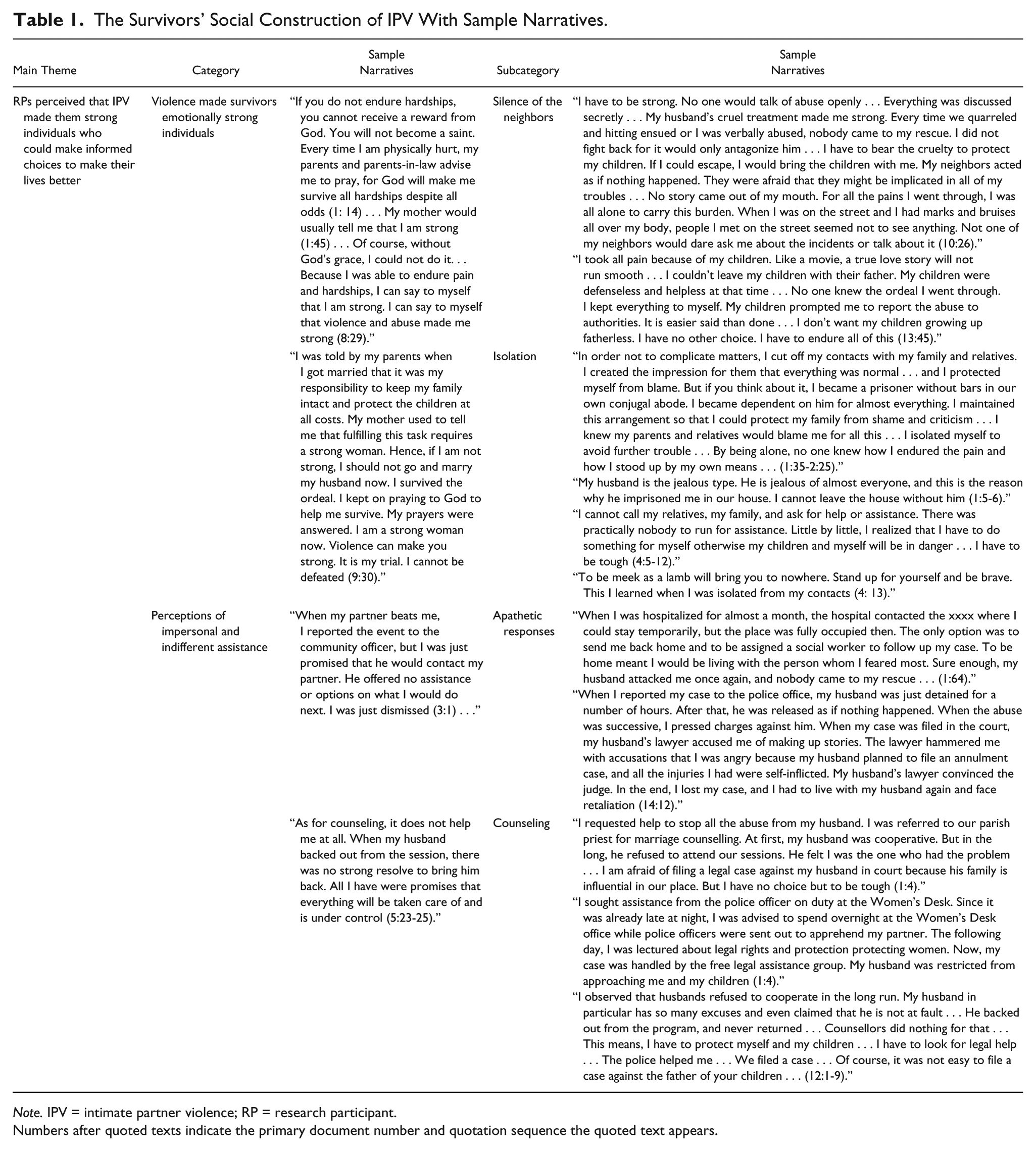
Note. IPV = intimate partner violence; RP = research participant.
Numbers after quoted texts indicate the primary document number and quotation sequence the quoted text appears.
Violence Made Survivors Emotionally Strong Individuals
The RPs claimed that IPV had made them tenacious because they were able to endure hardships to promote their own ends, such as keeping their marriage intact, keeping their children safe, and protecting the family from shame. They believed that their struggle was a worthy cause. The narrative begins with the experience of beating and humiliation and the process of enduring hardship and humiliation. As told by a survivor, If you do not endure hardships, you cannot receive a reward from God. You will not become a saint. Every time I am physically hurt, my parents and parents-in-law advise me to pray, for God will make me survive all hardships despite all odds (1: 14) . . . My mother would usually tell me that I am strong (1:45) . . . Of course, without God’s grace, I could not do it . . . Because I was able to endure pain and hardships, I can say to myself that I am strong. I can say to myself that violence and abuse made me strong (8:29).
Because they were able to endure suffering, the family was intact. According to an RP, I was told by my parents when I got married that it was my responsibility to keep my family intact and protect the children at all costs. My mother used to tell me that fulfilling this task requires a strong woman. Hence, if I am not strong, I should not go and marry my husband now. I survived the ordeal. I kept on praying to God to help me survive. My prayers were answered. I am a strong woman now. Violence can make you strong. It is my trial. I cannot be defeated (9:30).
Silence of the neighbors
Survivors of IPV believed that the silence of their neighbors contributed to their tenacity, which made them not give up easily. On the part of neighbors, they were silent so that they would be spared from all their troubles. Moreover, survivors believed that to a certain extent, fighting among couples is somewhat normal, but not when life and limbs are at risk. When fighting ensued, no one would come to their rescue, and the only option was to bear everything in silence. The perpetrator–husbands used fear, threats, and intimidation to silence their neighbors, and the neighbors chose silence to avoid being implicated in the situation: I have to be strong. No one would talk of abuse openly . . . Everything was discussed secretly . . . My husband’s cruel treatment made me strong. Every time we quarreled and hitting ensued or I was verbally abused, nobody came to my rescue. I did not fight back for it would only antagonize him . . . I have to bear the cruelty to protect my children. If I could escape, I would bring the children with me. My neighbors acted as if nothing happened. They were afraid that they might be implicated in all of my troubles . . . No story came out of my mouth. For all the pains I went through, I was all alone to carry this burden. When I was on the street and I had marks and bruises all over my body, people I met on the street seemed not to see anything. Not one of my neighbors would dare ask me about the incidents or talk about it (10:26).
The neighbors’ silence meant the family’s protection from shame because the least the neighbors can do is to pretend they do not know anything. The victims bear the burden of pain and struggle to survive because they choose silence. As narrated by an RP, I took all pain because of my children. Like a movie, a true love story will not run smooth . . . I couldn’t leave my children with their father. My children were defenseless and helpless at that time . . . No one knew the ordeal I went through. I kept everything to myself. My children prompted me to report the abuse to authorities. It is easier said than done . . . I don’t want my children growing up fatherless. I have no other choice. I have to endure all of this (13:45).
Isolation
Another component of perceived toughness, isolation is achieved by making victims withdraw contact from their social networks. IPV survivors narrated that by isolation, they were able to create the impression in their maternal families that their relationships were normal, they had a perfect family, and be spared from blame.
My husband kept on hammering me to cut off my contacts with my family, relatives, and friends. He made it sure that I could not get out from the house without his permission. Through this scheme, I was able to create the impression that everything was normal . . . and I protected myself from blame. But if you think about it, I became a prisoner without bars in our own conjugal abode. I became dependent on him for almost everything. I maintained this arrangement so that I could protect my family from shame and criticism . . . I knew my parents and relatives would blame me for all this . . . I isolated myself to avoid further trouble . . . By being alone, no one knew how I endured the pain and how I stood up by my own means . . . (1:35-2:25).
In other cases, isolation is an outcome of the abusive partner’s distrust of his intimate partner. This distrust is manifested in episodes of relational jealousy: My husband is the jealous type. He is jealous of almost everyone, and this is the reason why he imprisoned me in our house. I cannot leave the house without him (1:5-6).
Far more than being able to hide from the maternal family’s scrutiny, RPs narrated that through isolation, they realized that there was nobody to help them and rely on, except themselves. By being isolated from their social network, RPs made the resolve to take action and take responsibility for themselves. As narrated, When I was forbidden to make contacts even with my neighbors, I cannot call my relatives, my family, or anybody and ask for help or assistance. There was practically nobody to run for assistance. Little by little, I realized that I have to do something for myself, otherwise my children and myself will be in danger. I have to be tough . . . (4:5-12).
According to one RP, To be meek as a lamb will bring you to nowhere. Stand up for yourself and be brave. This I learned when I was isolated from my contacts (4: 13).
Perceptions of Impersonal and Indifferent Assistance
When IPV incidents were reported to the appropriate authorities, the RPs claimed that the responses of service providers such as police authorities or health care providers in dealing with IPV incidents were impersonal and indifferent. They perceived a lack of concern and indifference in handling their cases. According to an RP, When my partner beats me, I reported the event to the community officer, but I was just promised that he would contact my partner. He offered no assistance or options on what I would do next. I was just dismissed (3:1) . . . As for counselling, it does not help me at all. When my husband backed out from the session, there was no strong resolve to bring him back. All I have were promises that everything will be taken care of and is under control (5:23-25).
Based on the narratives, two types of impersonal assistance were perceived, apathetic responses and counseling by faith-based ministers.
Apathetic responses
Postabuse interventions, such as obtaining the history of abuse, referring the case to social workers, and medical attention, have placebo effects because these responses fail to address the needs of IPV victims, such as preferential attention to their case or situation. This perception was formed either because of the failure of health care providers to anticipate the consequences of their recommendations or because of apathy toward the conditions suffered by victims. The outcome of this apathetic attitude made the victims tough, and in due time, they learned to fight back. As narrated by one of the RPs, When I was hospitalized for almost a month, the hospital contacted the xxx where I could stay temporarily, but the place was fully occupied then. The only option was to send me back home and to be assigned a social worker to follow up my case. To be home meant I would be living with the person whom I feared most. Sure enough, my husband attacked me once again, and nobody came to my rescue . . . (1:64).
With regard to police arrests, RPs perceived that authorities worked more to restrict the movements of perpetrators than to convict perpetrators during the court litigation of their cases. What they feared most was the retaliation of their husbands: When I reported my case to the police office, my husband was just detained for a number of hours. After that, he was released as if nothing happened. When the abuse was successive, I pressed charges against him. When my case was filed in the court, my husband’s lawyer accused me of making up stories. The lawyer hammered me with accusations that I was angry because my husband planned to file an annulment case, and all the injuries I had were self-inflicted. My husband’s lawyer convinced the judge. In the end, I lost my case, and I had to live with my husband again and face retaliation (14:12).
Counseling
The RPs perceived IPV as destructive to the initiatives of conjugal partners seeking ways to restore relationships. They found counseling sessions useless because their partners refused to cooperate in the long run. “Anyway, it is voluntary” was the common excuse given by counselors for the lack of follow-up of cases. “Hope for change (14:25)” was the reason victims sought and submitted to professional help. However, to their dismay, “the whole process was futile (1:52).” From the perspectives of RPs, IPV destroyed cooperation, thus rendering professional help and all other self-help initiatives meaningless and futile. According to survivors, their husbands claimed that they could not be blamed for the acts committed and saw no need to submit to counseling because they were only imposing what was right at that time. Because of the failure of counselors, survivors claimed that IPV made them tough: I requested help to stop all the abuse from my husband. I was referred to our parish priest for marriage counselling. At first, my husband was cooperative. But in the long, he refused to attend our sessions. He felt I was the one who had the problem . . . I am afraid of filing a legal case against my husband in court because his family is influential in our place. But I have no choice but to be tough (1:4).
In another context, counseling bodies or organizations could not enforce their rules to counselees—usually the male partners—who backed out from counseling sessions. RPs observed that these counselors did nothing if their intimate partners would stop from participating the many sessions required by counseling groups. Thus, RPs assumed that if such cases continued, they perceived it a threat against their security, and has to do something for their own protection. As narrated, I observed that husbands refused to cooperate in the long run. My husband in particular has so many excuses and even claimed that he is not at fault . . . He backed out from the program, and never returned . . . Counsellors did nothing for that . . . This means, I have to protect myself and my children . . . I have to look for legal help . . . The police helped me . . . We filed a case . . . Of course, it was not easy to file a case against the father of your children . . . (12:1-9).
These narrations of the RPs pointed to the reality that they learned to be tough primarily because they perceived that nobody is truly interested to assist them in solving their problems. Thus, RPs thought that IPV transformed them into individuals who could stand before their perpetrators, defend themselves, call for assistance, and who would not just cower in fear and do nothing to survive. In their firmness to help themselves, their persistence in improving their situation gave the victims the determination to report the abusive situations to police authorities. Positive outcomes of their legal cases filed in courts of justice gave victims strength, courage, confidence, and trust in the justice system. In their testimonies, the victims stated that it was not easy for them to file cases against the fathers of their own children. Strength and the will to resolve the situation made them succeed. According to the victims, this will and knowledge of the laws protecting their interests, children, and families from all types of abuse made them empowered. In addition to knowledge of the laws, massive information dissemination and the aggressive pursuit of justice could be strong deterrents to aggressors in the perpetration of violence in all forms. Through the intervention of police authorities, the victims became aware of the legal rights that aimed to protect their interests and welfare: I sought assistance from the police officer on duty at the Women’s Desk. Since it was already late at night, I was advised to spend overnight at the Women’s Desk office while police officers were sent out to apprehend my partner. The following day, I was lectured about legal rights protecting women. Now, my case was handled by the free legal assistance group. My husband was restricted from approaching me and my children (1:4).
Discussion
RPs’ means to end IPV was attributed to their social construction of IPV. For them, IPV made them emotionally tough to handle all the challenges leading to IPV liberation. Survivors’ social construction of IPV was grounded in their lived experiences, which accounted for the many abuses they received from their intimate partners. Beginning with isolation and the silence of their neighbors and ending with the perception of apathy from duty providers, these experiences created their acquired strength in dealing with all situations of abuse leading to the empowerment of RPs. This construction was affirmed by the perception of religion and the expression of religious faith, convivial prospects for keeping the family intact, keeping children safe, and protecting the family from shame. This construction was exacerbated by parental utilization of biblical texts referring to the dissolubility and sanctity of the spousal union. All these factors to include isolation, apathy, and impersonal attention to the victims’ needs among others were perceived by survivors as instruments that encouraged them to endure their husbands’ cruelty and to bear suffering.
Isolation makes IPV socially invisible, not in the context of bringing private problems to public attention but in the access to support services. In seeking for legal assistance, the fear of retaliation if ever victims would lose their case is a reality that they have to face. Narratives were replete with stories of this fear. The offered assistance such as amicable settlements, reconciliatory moves as the primary solution, securing and granting temporary restraining orders, and marriage counseling gave only temporary solutions, and were mostly perceived by victims as favoring the aggressors. This perception arose when survivors noticed indifference especially from the male police authorities and health care providers. Health care providers did not offer concrete solutions for their concerns aside from medical care. When a health worker was assigned to handle a case, presumably another round of interviews would be conducted, which meant recalling painful experiences. The consequence was that victims would selectively disclose events to health care providers or deemphasize some events.
Survivors’ social construction of IPV reflects hegemonic masculinity and the acquisition of endurance to withstand cruelty. Hegemonic masculinity requires the display of strength in individuals. The strong subduing the weak through physical might and other debasing ploys are attempts to maintain hegemony. This concept corroborates the findings of Anwary (2015), Bozkurt et al. (2015), and Bhana and Mayeza (2016). Furthermore, the survivors referenced the strength they acquired from their faith in a deity and in the perception of impersonal and prejudicial assistance from health care providers and appropriate authorities. Similar findings were reported by Kposowa and Aly Ezzat (2019) regarding the role of religious beliefs as predisposing elements in IPV tolerance and Simmons (2019) on the influence of sociocultural beliefs and norms on domestic violence. It was this issue that made Hörl argue that the social construction grew from selective perceptions that were influenced by victims’ sociocultural milieu (Sigalla, Mushi, & Gammeltoft, 2018), and the existence of the differentials of perceptions. These perceptions may have been the situation prior their empowerment for they showed no courage to end violence but ended up accepting the abusive situation. Hence, it is recommended that in the administration of services to IPV victims, health care providers should be profoundly sensitive and sympathetic, so that by understanding their worldview, victims can be inspired to participate in rehabilitative or empowerment programs (Çalıkoglu et al., 2018; Wadsworth, Kothari, Lubwama, Brown, & Frank Benton, 2018).
Insights and Conclusion
In conclusion, the social construction of IPV—that IPV made women emotionally tough—made victims stand up for their cause to end violence. If this “toughness” that survivors are referring is to be interpreted as “being empowered,” it can be deduced that by empowering women, violence against them can be eliminated together with the full support of both the public and private entities. Many laws have been legislated aimed at protecting women and their children, but with disempowered beneficiaries, these laws will be rendered as counterproductive. Yet, empowerment of victims requires voluntary disclosure from victims, logistics, and other forms of support from surrounding communities and network. Based on the findings of this study, the factor on empowerment freed women from IPV. Along this thought, it is suggested for any intervention activities to (a) ultimately address the empowerment of individuals and (b) respond to the needs of individuals because what may work for one victim may not work for another. It is suggested that studies on IPV in the Philippines need to be aggressively pursued so that the results of such studies can be used in the design of programs for IPV prevention, care, and empowerment of victims.
Limitations
There are some limitations that should be recognized in the current study. Most of the data used in this article were self-reports by the RPs, so it is only possible to draw conclusions for similar situations, and the findings cannot be generalized. Although self-report data are common in the IPV field, this study did not consider the perspective of the RPs’ husbands. Although most of the data in this article were from an urban setting, perceptions of IPV from rural areas need to be considered when comparing and contrasting IPV perceptions in various settings. To obtain a picture of IPV in this part of the country, IPV perceptions from individuals of different social classes need to be considered in future research. Most of the collected data came from the lower social class, giving the impression that IPV involves the poor sector only. In addition, the data relied heavily on the narratives of RPs who requested privacy. The researchers were very limited in their investigation in this regard because they had almost no other means to check their stories with third-party sources.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.