
Abstract
Lesbian and bisexual women experience significantly higher rates of sexual assault and rape compared with heterosexual women. Despite this, researchers have yet to distinguish whether sexual orientation itself or some other related social characteristics explain these higher rates. The objective of this study was to analyze women’s rates of sexual assault and rape across sexual orientation status while accounting for other social characteristics (e.g., race, education, income, outness). Women (N = 1,366), who identified as lesbian (31%), bisexual (32%), and heterosexual (31%), completed a nationally distributed, cross-sectional online survey in 2016. Victimization and repeat victimization were assessed using a modified version of Sexual Experience Survey–Short Form Victimization. Overall, 63% of bisexual, 49% of lesbian, and 35% of heterosexual women reported experiencing rape in their lifetime. When holding all other social characteristics constant, sexual orientation remained a significant predictor in the model. Compared with the odds of heterosexual women experiencing sexual assault or rape, bisexual women (3.7 odds of victimization; 7.3 odds of repeat victimization) and lesbian women (3.2 odds of repeat victimization) were disproportionately victimized. Sexual orientation clearly plays a role in sexual victimization risk, independent of other measured sociodemographic indicators. Continued research is needed to explore possible mechanisms behind sexual assault and rape prevalence, as well as the influence of contextual factors of victimization risk among sexual minority men.
According to current estimates, nearly 7% of women in the United States identify as lesbian (1%) or bisexual (6%), with 17% of women below the age of 44 reporting same-sex sexual experiences (Copen, Chandra, Febo-Vazquez, 2016). This population is becoming increasingly recognized in the field of health disparities as a community of interest (Pérez-Stable, 2016), especially regarding experiences of sexual assault and rape. Indeed, sexual assault rates are high among lesbian and bisexual women (Heidt, Marx, & Gold, 2005; Hequembourg, Parks, Collins, & Hughes, 2015; Satinsky & Jozkowski, 2014). In a systematic review of 75 studies, Rothman and colleagues note that the median reported rate of sexual assault for lesbian and bisexual women is 43% (Rothman, Exner, & Baughman, 2011). When compared with heterosexual women, lesbian and bisexual women are more than 2 times more likely to be victims of sexual assault (Cramer, McNiel, Holley, Shumway, & Boccellari, 2012; Rothman & Silverman, 2007).
Research also suggests that some women are at higher risk of repeated sexual assault and rape victimization, and this may be particularly the case among sexual minority women. In a study of college women (Daigle, Fisher, & Cullen, 2008), those who experienced one instance of sexual violence were more likely to experience subsequent instances of sexual violence compared with women who did not have an initial sexual violence experience. In a national study of more than 11,000 women, rates of repeat victimization (experiencing both childhood and adult abuse) were lower among exclusively heterosexual women (10%) compared with either lesbian or bisexual women (23% and 26%, respectively; Drabble, Trocki, Hughes, Korcha, & Lown, 2013). In addition, Morris and Balsam (2003) found that lesbian and bisexual women who were victimized in childhood were 4 times more likely to experience that same type of victimization (physical or sexual) in adulthood. Because sexual violence and repeat victimization are commonly associated with higher rates of anxiety, depression, posttraumatic stress disorder, and social difficulties in heterosexual populations (Messman-Moore & Long, 2000), it is important that these rates be thoroughly assessed in lesbian and bisexual women as well.
Collectively, we know that several sociodemographic characteristics (e.g., income, education, race, “outness”) correlate with differing rates of sexual violence risk for women. For example, several studies find that women of color (Black et al., 2011), women residing in rural areas (Lewis, 2003), transgender women (Langenderfer-Magruder, Walls, Kattari, Whitfield, & Ramos, 2016), women attending college (Daigle et al., 2008), and women in the military (Mattocks et al., 2013) have higher sexual assault rates than their peers. These higher rates are not surprising; minorities and other vulnerable groups are at greater risk of all types of violence in general due to social disadvantage and discrimination (Brown, 2004). Because the identity of “woman” already puts an individual at greater risk of sexual assault, when this identity intersects with other socially disadvantaged characteristics (e.g., person of color, lesbian/bisexual sexual orientation), we find higher rates of sexual assault and rape.
Despite this, research has yet to disentangle sexual orientation from other social factors. Due to the discrimination and stigmatization lesbian and bisexual women face (e.g., employment discrimination), other characteristics (e.g., income) may be intertwined with and/or account for part of the elevated risk found in this population. Unfortunately, most studies of lesbian and bisexual women categorize women by their sexual orientation alone, without considering other social markers in the analyses. Because people hold multiple characteristics (e.g., sexual orientation, race, education, income) simultaneously, each may affect their experience uniquely or in combination (Crenshaw, 1991). In the current study, we parsed out some of the impact of these characteristics. Thus, the purpose of this study was to examine the prevalence rates of sexual assault and rape experienced by lesbian, bisexual, and heterosexual women while controlling for some of the other characteristics that may also influence their victimization risk.
Study Aim
The current study assessed national U.S. prevalence estimates of sexual assault and rape victimization and repeat victimization among lesbian, bisexual, and heterosexual women while accounting for other social characteristics (outness, income, education, and race) of these women. This is important because previous research indicates sexual assault and repeat victimization affect lesbian and bisexual women at higher rates compared with heterosexual women. But previous studies comparing these groups have yet to control for how other characteristics could confound the relationship that sexual orientation has with sexual assault risk.
Method
Participants and Procedures
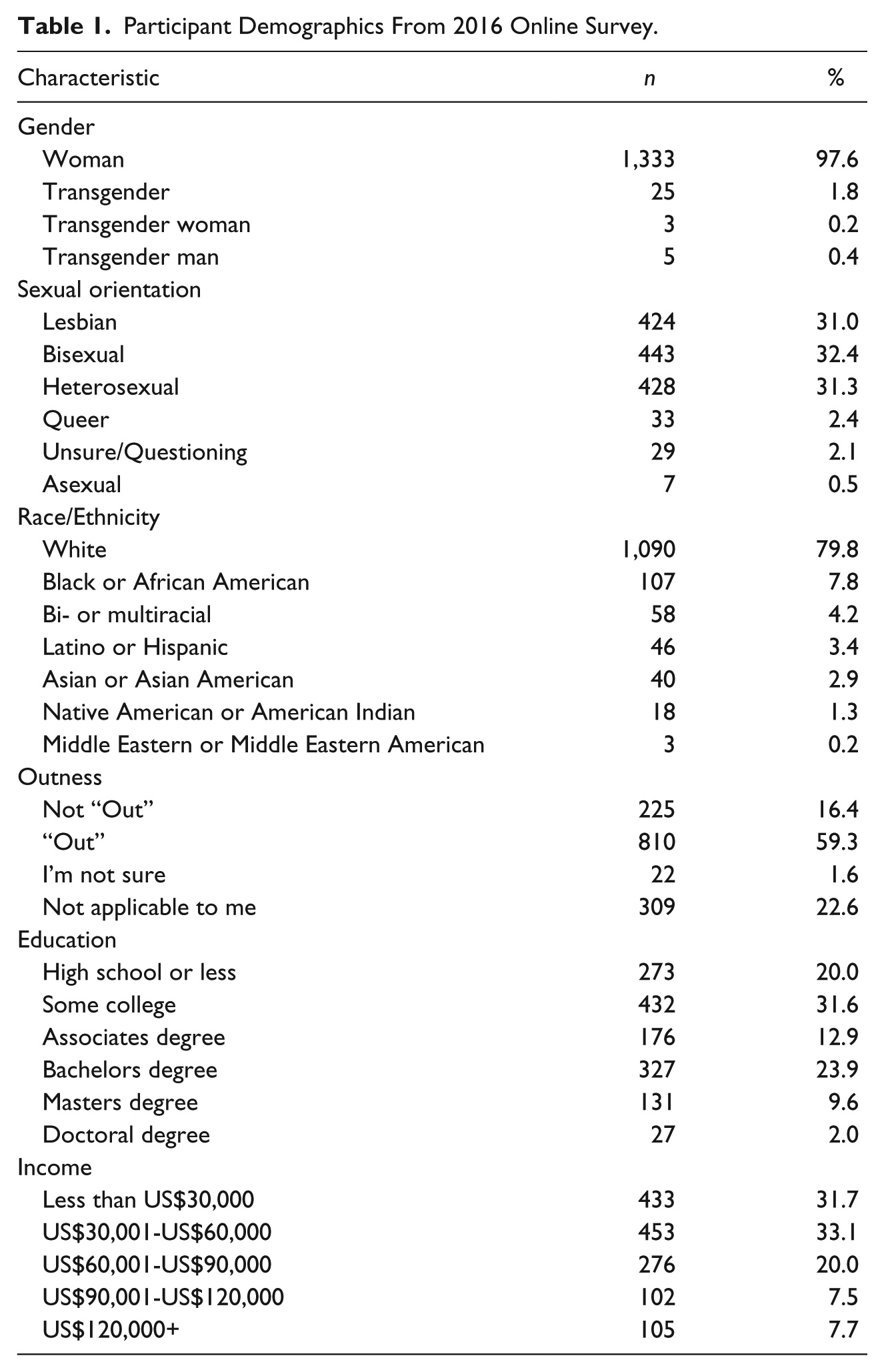
Participants (N = 1,366) completed an online survey in the summer of 2016. Most identified as women (97.6%, n = 1,333), with 2.4% identifying as transgender (n = 33). Due to preset quotas, the sample comprised of participants who identified as lesbian (31.0%, n = 424), bisexual (32.4%, n = 443), and heterosexual (31.3%, n = 428) in fairly equal frequency, with about 5% identifying as another sexual orientation—these smaller sexual orientation groups were not included in analyses in the current study. The mean age of participants was 41.9 years (SD = 17.4). The majority of the participants were White (80%) with no college degree (51%). See Table 1 for full demographic information.
Participant Demographics From 2016 Online Survey.
We created the survey using a systematic, iterative process. The preliminary survey was first reviewed by an expert panel (n = 6) of researchers with expertise in sexual health, gender, and sexual orientation. The survey was then pilot tested using a small focus group (n = 5) of lesbian, gay, bisexual, and transgender (LGBT) college students representing different majors who identified as women, transgender, and genderqueer. After additional revisions, the survey was pilot tested again using a convenience sample from the general population (n = 20). People in this group represented a range of ages (23-68 years), differing racial identities, several sexual orientation categories, politically liberal and conservative ideologies, and a range of education and income levels. Finally, the survey was reviewed again by the expert panel of sexual health researchers (n = 6).
The survey was then launched by Qualtrics Online Survey Company—an online research sample aggregator that collaborates with more than 20 online panel providers, reaching more than 1 million people. Qualtrics Online Survey Company advertises that their participant pools are representative of U.S. Census demographics (Qualtrics, personal communication, August 15, 2014), though it is not a probability-based sample. This company identified individuals from their national participant pool who met the study’s eligibility requirements (women above the age of 18) and sent out incentivized invitations, which included cash, airline miles, gift cards, redeemable points, and sweepstakes entrances. Invitations were sent to the participant pool until sexual orientation sample quotas were met (Qualtrics, personal communication, August 15, 2014). The study protocol was approved by the institutional review board prior to survey distribution.
Measures
Demographics
In the demographics section, participants were asked about their gender (“What is your gender?”), race (“How would you describe your race?”), sexual orientation (“How would you describe your sexual orientation?”), household income (“What is your household income before taxes?”), and level of education (“What is the highest level of education you have completed?”). Answer options for each of these items are presented in Table 1. Questions about how “. . . ‘out’ or ‘open’ you are about your sexual orientation” were also included in this section. Answer options for outness included a 4-point continuum from “hardly anybody knows” to “I am very ‘out’, I make sure almost everyone I interact with knows.” This continuum was later dichotomized into “Out” and “Not Out” options. Two additional choices of “I am not sure” and “I don’t think this applies to me” could also be selected for the outness question.
Modified Sexual Experience Survey–Short Form Victimization (SES-SFV)
We used a modified version of the SES-SFV (Koss et al., 2007), which assesses prevalence rates of sexual assault and rape. For the purpose of this study, we define sexual assault as sexual contact or behavior that occurs without the consent of the recipient (Department of Justice, 2016). Rape is conceptualized as a type of sexual assault that involves penetration of a body (oral, vaginal, and/or anal) without consent.
The original SES-SFV asks participants about their experiences with various tactics perpetrators can use (e.g., Taking advantage of me when I was too drunk or out of it to stop what was happening) to facilitate four distinct nonconsensual behaviors: (a) non-penetrative sexual behaviors (fondling, kissing, rubbing up against private areas of body, or removing clothing), (b) oral sex, (c) vaginal penetration, and (d) anal penetration. Modifications included adding two additional tactics that participants could indicate a perpetrator used to facilitate nonconsensual sexual behavior: (a) making me feel as though refusing was useless and (b) just doing the behavior without giving me a chance to say “no” (e.g., surprising me with the behavior). The former tactic (making me feel refusing was useless) has been shown to relate to sexual assault victimization (Canan, Jozkowski, & Crawford, 2016; Jozkowski & Peterson, 2013). Importantly, the latter tactic (surprising me with the behavior) was added by request of participants during the survey pilot testing phase and is consistent with deceptive tactics found in the sexual consent literature (Jozkowski & Peterson, 2013). Participants could select if any of the tactics occurred prior to 14 years of age (0, 1, 2, 3-9, or 10+ times) or from 14 years of age to present (0, 1, 2, 3-9, or 10+ times). We also added an “Unsure” answer choice to the SES-SFV’s original standalone question of “Have you ever been raped?” This option was added in case participants may not have previously labeled their experience as rape, but after taking the survey, they had begun to question this label.
Participants who reported experiencing any tactics greater than “0” on either of the two periods (birth to 13 years of age, 14 years of age to present) for any of the nonconsensual sexual behaviors were guided into a specific victim branch of the survey. Participants who selected “0” times for all tactics over both time periods for all behaviors and also selected “Yes” or “Unsure” to the “Have you ever been raped?” question were also triaged into the victim branch of the survey. All other participants who selected “0” times for all tactics over both time periods for all behaviors and answered “No” to being raped then completed a different set of questions, which are not reported here.
Data Analysis
We categorized participants’ experiences of lifetime sexual assault (LSA) into four categories based on their SES-SFV responses: non-victim, victim of non-penetrative behavior only (hereafter referred to as “sexual assault”), victim of attempted penetrative behavior only (hereafter referred to as “attempted rape”), and victim of penetrative behavior (hereafter referred to as “rape”). A 3 × 4 chi-square analysis with a Cramer’s V effect size was conducted with sexual orientation and the SES-SFV categorizations.
Due to limitations of the SES-SFV measure, people who had multiple experiences of victimization within one time frame (e.g., oral penetration at 18 years old and then vaginal penetration at 20 years old) are indistinguishable from people who had multiple experiences in the same day (e.g., one instance involving both oral and vaginal penetration). Therefore, we used at least one instance of childhood sexual assault (CSA; occurring before 14 years of age) and at least one instance of adulthood sexual assault (ASA; occurring on or after 14 years of age) to create a measure of repeat victimization, which is similar to other researcher’s operational definitions (e.g., Drabble et al., 2013). This way, we can be sure that there were multiple occurrences because they happened at different ages. Separate chi-square analyses, with Cramer’s V effect sizes, assessed differences in CSA, ASA, and repeat victimization by sexual orientation categories (see Table 2).
LSA, CSA, ASA, and Repeat Victimization Rates Between Lesbian (L, n = 424), Bisexual (B, n = 443), and Heterosexual (H, n = 428) Participants.

Note. All comparisons within the same question utilized a Holm’s sequential Bonferroni correction. LSA = lifetime sexual assault; CSA = childhood sexual assault; ASA = adulthood sexual assault.
When a group is statistically similar to another group that shares the same letter and is significantly different than another group that has a different letter.
Between-group differences were not tested post hoc. If group-level chi-square was not significant or cell counts were too small, further comparisons were not conducted.
To test whether differences in victimization experiences were predicted by sexual orientation, independent of other demographic characteristics (race, income, education, and outness), we used multinomial logistic regression analyses. The dependent variable, victimization, included three categories: single victim (either birth to 13 years or 14 years to present) = 1; repeat victim (victimization during both time periods) = 2; and non-victim = reference. Independent variables included sexual orientation, race, income, education, and outness. For specific response options, see Table 3. In an effort to build a concise model, we first performed individual univariate tests with each dependent variable separately. If the likelihood-ratio chi-square of these univariate tests met a liberal threshold of p < .25 (Bursac, Gauss, Williams, & Hosmer, 2008), then the independent variable was retained in the multivariate model.
Odds of Experiencing Lifetime Sexual Assault Victimization and Repeat Victimization.
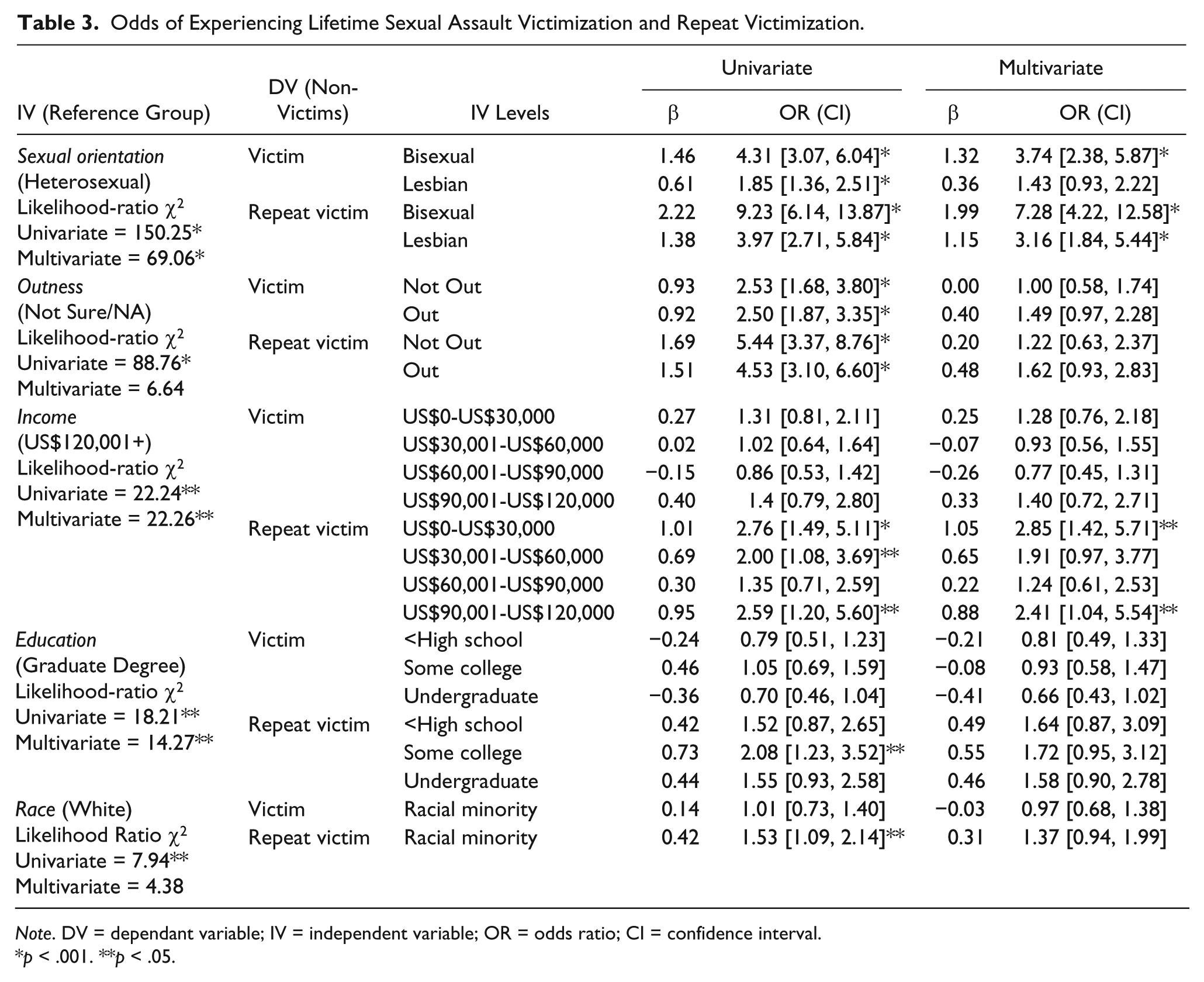
Note. DV = dependant variable; IV = independent variable; OR = odds ratio; CI = confidence interval.
p < .001. **p < .05.
Results
Overall, 67% (n = 921) of the sample experienced one or more types of sexual assault and/or rape. Most (50%, n = 678) experienced rape alone or rape in addition to other victimizing behaviors. Some experienced sexual assault only (10%, n = 137) and 8% (n = 106) experienced attempted rape only. Fewer participants (31%, n = 399) experienced CSA than experienced ASA (63%, n = 811). In addition, 26% (n = 342) experienced repeat victimization (at least one CSA instance and one ASA instance). See Table 2.
Bivariate Comparisons
Overall, 63% (n = 281) of bisexual women, 49% (n = 206) of lesbian women, and 35% (n = 149) of heterosexual women reported experiencing rape in their lifetime. There were significant differences between lesbian, bisexual, and heterosexual women in experiencing rape, χ2(2, n = 1,295) = 71.4, p < .001; small–medium effect size, Cramer’s V = .235, p < .001. After using a Holm’s sequential Bonferroni correction, bisexual women were more likely to experience rape than lesbian, χ2(1, n = 867) = 19.4, p < .001; small effect size, Cramer’s V = .15, p < .001, and heterosexual women, χ2(1, n = 871) = 71.3, p < .001; medium effect size, Cramer’s V = .29, p < .001. In addition, lesbian women were more likely to experience rape than heterosexual women, χ2(1, n = 852) = 16.6, p < .001; small effect size, Cramer’s V = .14, p < .001.
Eleven percent (n = 48) of bisexual women, 8% (n = 35) of lesbian women, and 4% (n = 18) of heterosexual women reported experiencing attempted rape only. There was a significant difference between lesbian, bisexual, and heterosexual women experiencing attempted rape only, χ2(2, n = 1,295) = 13.5, p = .001; small effect size, Cramer’s V = .10, p = .001. After a Holm’s sequential Bonferroni correction, only two comparisons remained significant. Bisexual women were more likely to experience attempted rape than heterosexual women, χ2(1, n = 871) = 13.7, p < .001; small effect size, Cramer’s V = .13, p < .001. Lesbian women were also more likely to experience attempted rape than heterosexual women, χ2(1, n = 852) = 5.9, p = .014; small effect size, Cramer’s V = .08, p = .014. Comparisons between lesbian, bisexual, and heterosexual women for sexual assault–only experiences were not significant, χ2(2, n = 1,295) = 2.6 (p = .27), Cramer’s V = .05 (p = .27). See Table 2 for further prevalence information.
Multinomial Logistic Regression
In the multinomial models (Table 3), participants were classified based on victimization outcome. Specifically, the log odds of each victim outcome (single victimization = 1; repeat victimization = 2; non-victim = reference) were modeled as a linear combination of the predictors. All demographic variables significantly (p < .05) predicted victimization at the univariate level—sexual orientation, χ2(4, n = 1,295) = 150.3; outness, χ2(4, n = 1,366) = 88.8; income, χ2(8, n = 1,366) = 22.2; education, χ2(6, n = 1,366) = 18.2; race, χ2(2, n = 1,366) = 7.9. Because of this, all were retained in the multivariate model. At the multivariate level, only sexual orientation (χ2 = 69.06) and income (χ2 = 22.26) remained significant predictors of victimization while holding all other variables constant.
With non-victimization as the dependent variable reference category, bisexual women (odds ratio [OR] = 3.7, 95% confidence interval [CI] = [2.38, 5.87]) had increased odds for single victimization compared with heterosexual women. Bisexual (OR = 7.3, 95% CI = [4.22, 12.58]) and lesbian women (OR = 3.2, 95% CI = [1.84, 5.44]) had increased odds of repeat victimization compared with heterosexual women. In addition, none of the income levels significantly differed for single victimization as compared with non-victimization; the only differences occurred when comparing income levels for repeat victimization versus non-victimization. Individuals who earned US$0 to US$30,000 per year (OR = 2.9, 95% CI = [1.42, 5.71]) as well as individuals who earned US$90,000 to US$120,000 per year (OR = 2.4, 95% CI = [1.04, 5.54]) had increased odds of repeat victimization compared with individuals who earned over US$120,000 a year. Mid-range incomes were not significantly different from incomes of more than US$120,000 for repeat victimization.
Discussion
Approximately half of the sample had experienced rape (i.e., nonconsensual completed oral, vaginal, and/or anal penetration). This is notably higher than a number of studies which indicate between 18% and 22% of women in the general U.S. population have experienced rape in their lives (Black et al., 2011; Tjaden & Thoennes, 2006). These high prevalence rates are likely influenced by our oversampling of lesbian and bisexual women, who experience increased rates of sexual assault and rape (Hughes et al., 2010; Rothman et al., 2011; Satinsky & Jozkowski, 2014).
However, rates of rape among heterosexual women in our sample are still notably higher (35%) than previous studies (Muehlenhard, Peterson, Humphreys, & Jozkowski, 2017; Tjaden & Thoennes, 2006). These higher rates may be partially explained by the two additional prompts that were added to the original SES-SFV (“Making me feel as though refusing was useless” and “Just doing the behavior without giving me a chance to say ‘no’ [e.g., surprising me with the behavior]”). These two prompts uniquely captured 103 additional participants who would not have otherwise been detected by the original SES-SFV items (Canan, 2017). Previous research finds that the more prompts for victimization experiences participants are given, the more likely a memory of sexual assault will be recalled, resulting in increased opportunities for participants to answer affirmatively to the victimization experience (Bachman, 2012). We argue that this methodology is more comprehensive than previous measurements, and therefore, our rates may more accurately represent U.S. women’s experiences.
Our findings are consistent with previous studies (Andersen, Hughes, Zou, & Wilsnack, 2014; Drabble et al., 2013; Hughes et al., 2010) in that bisexual women reported the highest rates of sexual assault and rape, followed by lesbian women. Sadly, it seems as though sexual violence is the status quo for lesbian and bisexual women with 63% and 49% experiencing rape, 11% and 8% experiencing attempted rape only, and 10% and 12% experiencing sexual assault only, respectively. In other words, only 16% of bisexual and 32% of lesbian women never experienced sexual assault in their lifetime. For comparison, one in five women on college campuses report experiences of sexual assault before they graduate (Muehlenhard et al., 2017). These college rates have warranted government attention (The White House, 2014) and news coverage (Bogdanich, 2014) discussing the issue as one of “seriousness and urgency” (White House Task Force to Protect Students from Sexual Assault, 2017). Our study finds that sexual assault and rape experiences of lesbian and bisexual women alarmingly exceed these estimates. Our findings strongly suggest that lesbian and bisexual women are at particular risk and should be included in the national discussion on sexual violence education, prevention, and intervention efforts (Campbell, 2009; Girshick, 2002).
Our finding that sexual orientation was the most significant predictor of victimization status, even when holding all other variables constant, further warrants heightened attention for this population. Bisexual women were 3.74 times as likely as heterosexual women to be victimized and 7.28 times as likely as heterosexual women to experience repeat victimization. Although this study cannot fully answer why this occurs, one explanation may be the sexualization of bisexual women. That is, stereotypes about bisexual women often characterize them as more sexually promiscuous than other women (Klesse, 2005). Some argue that the sexualization of bisexual women is a result of biphobia and leads to sexual objectification of this group (Eisner, 2013). Others contend that the sexual objectification of women in general is a contributing factor to high sexual assault rates in women (Friedman & Valenti, 2008; Loughnan, Pina, Vasquez, & Puvia, 2013). Therefore, if bisexual women are sexually objectified at equal or increased rates compared with heterosexual women, not only because of their gender but also because of their sexual orientation, these overlaid identities may increase their risk of sexual assault and rape. These higher rates are not surprising because vulnerable groups, including groups that are objectified, are at greater risk of all types of violence due to social disadvantage and discrimination (Brown, 2004).
Both low (US$0-US$30,000; OR = 2.9) and middle–high incomes (US$90,000-US$120,000; OR = 2.4) were also significant predictors of repeat victimization compared with the highest incomes (US$120,000+). The former finding is not surprising, yet the latter finding was unexpected. Previous research has indicated that poverty is a risk factor for sexual assault victimization (Grecco & Dawgert, 2007). However, there is little, if any, research that might suggest why women with middle-high incomes are 2.4 times more likely to experience repeat victimization compared with women with the highest incomes. Future research exploring the role socioeconomic status and income may play in sexual assault risk may be helpful to more specifically parse out these income categories, which would allow for continued monitoring of this novel association.
Limitations
To obtain a sufficient sample inclusive of our target population of interest (e.g., lesbian and bisexual identified women), we used an online survey company to distribute the survey link to a national sample of adults in the United States. Therefore, these findings are restricted to people who have access to the internet, are signed up to be part of Qualtrics panels, and who are responsive to survey requests. In addition, the survey was provided in English, thus excluding non-English readers. Furthermore, although our sample was a national sample, our participant demographics had slightly lower proportions of racial/ethnic minority groups than 2015 U.S. Census estimates; participant demographic quotas were consistent across other variables (Ryan & Bauman, 2016; U.S. Census Bureau, 2016). Importantly, we control for some of the possible challenges these limitations may pose by including our sociodemographic indicators (such as race/ethnicity, income) in our analyses.
Finally, one limitation lies in the SES-SFV scoring of the sexual assault and rape repeat victimization rates. Using the SES-SFV to assess victimization, we can calculate lifetime rates as well as two time-specific rates: birth to 13 years old (CSA) and 14 years old to present (ASA). We also assess repeat victimization rates as at least one experience of CSA and one experience of ASA. But there are many ways to conceptualize repeat victimization, and each has its own set of strengths and limitations. For example, using our method, the format of the SES-SFV does not allow us to confidently assess for multiple events within the same time frame. One victim could experience a singular event at age 18 with three distinct assaultive behaviors in the same night and another victim could experience three different events at ages 18, 25, and 30 with only one behavior occurring at each event. These two individuals would be indistinguishable with current scoring capabilities based on the developer’s guidelines (Koss et al., 2007). Therefore, the prevalence of people experiencing multiple events of sexual assault and rape is likely higher than current reported repeat victimization rates.
Implications
More systemic support is needed to address what we argue is crisis-level prevalence of sexual assault and rape among lesbian and bisexual women. Some possibilities include efforts to increase awareness, sexual assault prevention programming, and rape advocate–assisted services specifically targeted to this population; this list is certainly not exhaustive. Some organizations, including the Human Rights Campaign (2015), are leading some national public discourse on the issue. In addition, a few prominent organizations (e.g., Rape, Abuse, and Incest National Network) include resources for lesbian, gay, bisexual, transgender, and queer (LGBTQ) survivors on their websites (Rape, Abuse & Incest National Network, 2016). Although these activities are promising, our findings call for expanded efforts and resources in light of the magnitude of this problem and its impact on public health.
Specifically, we see a clear need for expanded population-specific services. Other researchers have highlighted gaps and barriers to sexual assault services for the lesbian and bisexual community (Todahl, Linville, Bustin, Wheeler, & Gau, 2009). Some of these barriers include limited staff awareness of lesbian and bisexual sexual violence and low levels of resources. We recommend services should increase diversity in staff recruitment and trainings with the ultimate goals of delivering culturally competent care. In addition, rape crisis centers and general health care centers that offer these services should develop community relations and promote themselves as resources to lesbian and bisexual women. Establishing a supportive presence (attending community events, advertising in community centers and other common lesbian and bisexual spaces) could be an important strategy to increase outreach effectiveness.
Future Research
More victims in our sample had experienced ASA (on or after age 14) than CSA. In our sample, lesbian and bisexual women also experienced more ASA compared with heterosexual women. In their review of lesbian and bisexual sexual literature, Rothman and colleagues recommended increasing research efforts assessing ASA in this population (Rothman et al., 2011). Our findings provide some context around this issue and suggest that investigations including other factors related to sexual orientation may further our understanding of ASA risk. Specifically, research on the situational contexts in which these assaults occur would provide insight into potential lifestyle and routine activity correlates of victimization among lesbian and bisexual women. Further research is also needed to explore sexual assault prevalence and contextual factors among sexual minority men who are far less studied in the sexual assault literature (Peterson, Voller, Polusny, & Murdoch, 2011).
Conclusion
Rates of sexual assault for lesbian and bisexual women are high, with 63% of bisexual women and 49% of lesbian women experiencing rape in their lifetime. Sexual orientation clearly plays a role in sexual violence risk; bisexual women were 3.7 times as likely as heterosexual women to be a victim and 7.3 times as likely as heterosexual women to experience repeat victimization when holding all other variables constant. In fact, sexual orientation had the strongest relationship with victimization status compared with all other demographic characteristics. We argue that the elevated risk linked to sexual orientation may be partially explained through a broad lens of discrimination and social disadvantage (Brown, 2004). Cultural-level attitudes regarding sexuality make it easier to justify sexual violence against lesbian and bisexual women. For example, lesbian and bisexual women may experience hypersexualization and subsequent sexual objectification partially because their identities are tightly tied to their sexuality (Eisner, 2013; Klesse, 2005). Barriers to reporting and minimal structural support may disproportionately burden lesbian and bisexual victims. Therefore, both proactive cultural shifts and reactive support services for lesbian and bisexual victims of sexual assault are needed to address this problem.
Footnotes
Compliance With Ethical Standards
All procedures performed in studies involving human participants were in accordance with the ethical standards approved by Institutional Review Board at the host institution. Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the American Psychological Foundation 2016 Roy Scrivner Memorial Research Grant.