
Abstract
Trauma-focused research highlights the reactions of seasoned professionals when engaging with vulnerable clients; however, less is known about the common reactions of novices engaged in trauma research, who may lack the skills to cope and interact with traumatized participants. The purpose of this study is to (a) describe common reactions experienced by novice trauma interviewers; (b) examine whether the issues they face are similar to those of seasoned helping professionals; and (c) discuss ways in which training and supervision can increase the well-being of interviewers in trauma research. A semi-structured assessment was administered to novice interviewers who had previously conducted psychosocial and trauma assessments with diverse community participants. Participation was voluntary. The assessment elicited responses concerning secondary traumatic stress, vicarious trauma, posttraumatic growth, and self-help and resources. Audio files were transcribed; responses were compiled to explore themes and identify illustrative quotes. Eight interviewers (two males, six females) participated. Six reported no prior experience working with populations with histories of trauma. Novice interviewers described experiences of secondary traumatic stress, vicarious trauma, compassion fatigue, posttraumatic growth, and resilience. Novice interviewers described symptoms consistent with those reported by seasoned helping professionals; positive and negative symptoms often coexisted. Interviewers who completed more assessments described reactions of sadness, anger, insomnia, and changes in worldview. Interviewers who shared similar traumatic histories or environments reported more examples of countertransference. All reported similar feelings of posttraumatic growth, such as hope and optimism, for their participants and an increased appreciation of their resilience. Implications for training and supervision are discussed.
Trauma-focused research highlights the reactions of seasoned front-line professionals and the stresses they encounter when engaging with vulnerable clients. A large body of literature indicates that empathetic listening to others’ traumatic experiences often evokes difficult and negative reactions in helping professionals across numerous disciplines (e.g., nurses, social workers, firefighters, emergency room doctors and psychologists; Cieslak et al., 2013; Coles et al., 2014). These reactions are described as conceptually overlapping and the terms used to describe them are frequently used interchangeably (Office of Justice Programs, n.d.). In contrast, little attention has been paid to identifying the common reactions of novices, particularly those engaged in trauma research, despite the fact that they are also on the front lines conducting interviews with traumatized participants.
Seasoned professionals have typically engaged in clinical work over many years and are likely to be better accustomed to dealing with participants with trauma than novice researchers, although we recognize that that trauma-related research can take a toll on seasoned professionals as well (Weill, 2014). Novices who elect to participate in trauma research often engage with clients in distress without the skills or experience that allow them to preserve their own mental health and work effectively with traumatized individuals. Novices may also vary greatly with respect to education, clinical experience, and training, as well as personal resources and previous personal experiences with trauma. These characteristics are likely to affect their ability to cope with hearing the painful experiences of others (Weill, 2014). Despite the fact that many novice interviewers in trauma-focused research describe the disclosure of trauma as both therapeutic and valuable (Griffin et al., 2003; Newman et al., 1999; Seedat, 1998), novice interviewers may fear that asking sensitive questions about trauma and mental health will result in participants feeling uncomfortable or retraumatized. These assumptions may be based on their lack of skills to confidently address participants’ trauma (Seedat et al., 2004).
Reactions Reported by Seasoned Professionals
Common negative reactions include experiences of secondary traumatic stress, vicarious trauma, and compassion fatigue. Secondary traumatic stress reactions stem from the processing of other people’s traumatic experiences. These reactions mirror those of the trauma victims with whom they work and include symptoms commonly associated with posttraumatic stress disorder (PTSD), ranging from including depressed mood to intrusive images and thoughts regarding patients’ trauma (Coles et al., 2014; O’Reilly & Kiyimba, 2015). Vicarious trauma involves a negative transformation in worldview, with helping professionals typically experiencing skewed cognition, often becoming more fearful, vulnerable, and/or cynical, in addition to the symptoms presented in secondary traumatic stress (Figley Institute, 2012; National Child Traumatic Stress Network, Secondary Traumatic Stress Committee, 2011; Office of Justice Program, n.d). Individuals may report a loss of personal sense of meaning in life and/or feel hopeless about the future. Compassion fatigue, similar to symptoms of depression and a precursor to burnout, is another common reaction experienced by helping professionals and is experienced as the feeling of “not feeling” anymore and potentially losing compassion for others. It can be experienced through signs of frustration, exhaustion, helplessness, detachment, and avoidance (Figley Institute, 2012; Richard, 2013; Silveira & Boyer, 2015).
While trauma research studies have focused primarily on the negative effects of listening to the experiences of traumatized clients, research also suggests that many mental health professionals are resilient or experience posttraumatic growth (Yilmaz, 2017). Research suggests that post traumatic growth can transition from vicarious trauma, and that individuals need to feel pain first (Barrington & Shakespeare-Finch, 2013; Silveira & Boyer, 2015; Sui & Padmanabhanunni, 2016). Definitions of resilience usually focus on personal and professional factors that enable individuals to cope successfully, bounce back, or even thrive when confronted by stress and adversity (McCann et al., 2013; Sexual Violence Research Initiative, 2015; Yilmaz, 2017). Although much of the literature equates resilience with posttraumatic growth, the latter term refers more specifically to positive change that follows trauma (Westphal & Bonanno, 2007). These changes include a new appreciation for one’s personal strength and life in general and a focus on helping others (Westphal & Bonanno, 2007). While both constructs are focused on well-being, research suggests that they are inversely related. Many individuals are resilient in the face of trauma and may not experience posttraumatic growth (Westphal & Bonanno, 2007).
Self-Help and Support
To combat negative reactions, researchers have adopted measures such as focusing on initial and ongoing training and conducting regular interviewer team meetings and supervision (Urquiza et al., 1997) to help novice trauma interviewers engage in self-help, receive support, and debrief distressing experiences. However, even with training and supervision, novices may be unprepared to effectively interact with participants who are overwhelmed and lack basic resources, and hear about severe trauma experiences, some of which may not have previously been disclosed. It is important to identify the common reactions that novice interviewers experience when engaged in trauma research and determine whether they differ from those who have years of professional experience so that training and supervision can be tailored to meet their needs.
The purpose of this study is to describe the initial reactions experienced by novice interviewers regarding their experiences conducting trauma research with marginalized communities in Los Angeles. We will also examine whether the issues novice trauma interviewers face are similar to those described in the literature on seasoned helping professionals. Finally, we will discuss ways in which training and supervision can address the experiences of novice trauma interviewers to increase the well-being of both interviewers and participants in trauma research.
Method
Sample
The University of California, Los Angeles (UCLA) Centers of Excellence (COE) study (Liu, Loeb, Chin & Wyatt, 2019) included 15 novice interviewers (five men, 10 women) who received training in the mental and physical health correlates of trauma, interviewing skills, role-playing interview techniques, Mental Health First Aid, and the Collaborative Institutional Training Initiative. They interviewed a total of 200 multiethnic participants recruited from community fairs, organizations, and clinics in marginalized and underserved communities. Participants were eligible to participate in the study if they were between the ages of 18 and 65 years and spoke English or Spanish. The interview was titled “Life Experiences Assessment” and included sociodemographic questions as well as measures of somatic and depressive symptoms, health care utilization, having a life-threatening illness, serious or traumatic events, and 21 items assessing five dimensions of trauma (sexual abuse, interpersonal violence, community violence, family adversity, and perceived discrimination; see Liu et al., 2014 for additional information). This standard core battery was administered to all participants through face-to-face interview sessions. All participants were compensated for their time and received referrals provided by the Los Angeles County Department of Mental Health services. Participants were able to refuse to answer questions or withdraw from the study at any time without any consequences. Any participant who expressed suicidal ideation was immediately connected to a senior investigator, who assessed for suicide risk and referred those deemed at risk to a Los Angeles County social worker who facilitated linkage with mental health services and resources. No participants required hospitalization. The research was approved by the institutional review board at the UCLA. All study participants provided written informed consent.
Novice interviewers were able to contact seasoned clinicians and/or researchers at any time to ask questions and receive guidance and support. The interviewers reported either being a community stakeholder (n = 4) or health professionals, including premed postbaccalaureate students (n = 5), an undergraduate (n = 1), a medical student (n = 1), or master’s level students (n = 3). To be eligible for participation, novice interviewers had to have conducted more than one interview, which excluded two interviewers. The remaining 13 interviewers were invited to participate in the study by email. Five interviewers did not respond to the email. Those who did not respond may not have participated for a variety of reasons, including the fact that their formal participation in the COE study had ended, participation was optional, there was no financial remuneration, and many were full-time students.
Procedures
The novice interviewers were recruited from an email listserv 3 weeks after the completion of data collection for the COE study. Participation was voluntary. An initial email to all of the eligible interviewers (n = 13) involved in the study was sent to gauge participation interest. Up to two follow-up emails were sent, resulting in responses from eight of the 13 eligible interviewers. All eight interviewers completed an informed consent through email before participating in the research. Telephone interviews were conducted between June and August 2017. The semi-structured interview was guided by previously published measures of secondary traumatic stress and posttraumatic growth (see the appendix). Interviews lasted from 60 to 90 min. To explore secondary traumatic stress, sample questions included the following: “Have you experienced any persistent negative emotions such as sadness, anger, frustration, etc.?” and “Have you had any recurrent intrusive thoughts or nightmares about the participant’s trauma?” To explore posttraumatic growth, sample questions included the following: “Have you experienced any positive transformations such as sense of optimism?” and “Have you experienced any changes in your beliefs or worldview or your self-perception?” Regarding self-help, resources, and support, we asked questions such as “How did you try to protect and to take care of yourself during your time interviewing participants? Please tell us about your experiences. What worked well for you?” and “What, if any, were the resources and supports made available to you to enable you to continue this work?” Additional questions focused on the interview experience in general and the overall impact it had on the novice interviewer. Audio files were transcribed by the authors.
Data Analysis
Each transcript was reviewed by the research team, and responses pertaining to each theme from the literature (secondary traumatic stress, vicarious trauma, compassion fatigue, posttraumatic growth, resilience, and self-care and resources) were compiled into documents to explore the themes and identify illustrative quotes. The themes were also analyzed by number of interviews conducted by each novice interviewer, to explore whether those with more interviewing experience differed in any key ways from those with less experience. The data pertaining to each theme were reviewed as well as the illustrative segments, and the team discussed came to consensus about the main findings.
Results
Interviewer Characteristics
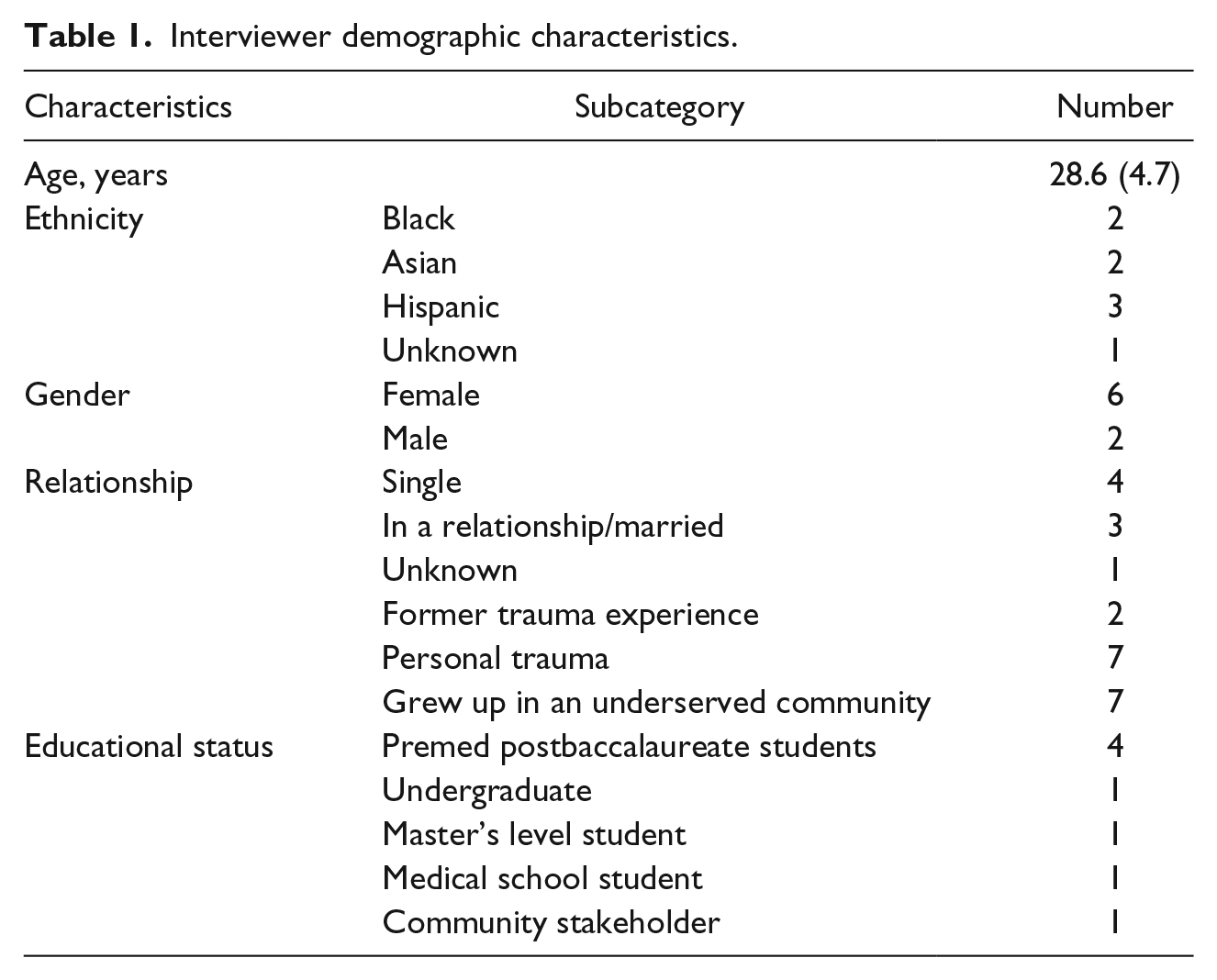
Eight interviewers (two males, six females) participated in the interview, with an age range of 21 to 38 (M = 28) years. Interviewers were ethnically diverse: three were Hispanic, two were African American, two were Asian, and one declined to state her race/ethnicity. Six had no prior experience working with populations with histories of trauma; two had little to some experience. Seven interviewers were raised in underserved communities. Four interviewers reported that they were enrolled in premed postbaccalaureate program (n = 4), while the other interviewers reported they were a community stakeholder/advocate (n = 1), undergraduate student (n = 1), medical student (n = 1), or a master’s level social welfare student (n = 1). Interviewers included in this analysis conducted a total of 3 to 57 interviews each (see Table 1).
Interviewer demographic characteristics.
Themes
Interviews were coded for novice interviewers’ experiences of secondary traumatic stress, vicarious trauma, posttraumatic growth, and training/resources/self-care. Two additional themes, compassion fatigue and resilience, emerged from the data and were subsequently included in the analysis. Key symptoms of each phenomenon (defined above) were used for coding purposes.
Secondary traumatic stress
Interviewers described experiencing more symptoms of secondary traumatic stress as a result of conducting more number of interviews. All but one interviewer described having at least one symptom of secondary traumatic stress. Those who conducted fewer interviews reported only symptoms of sadness. For instance, Interviewer (I) 2 (eight interviews) and I8 (two interviews) expressed feeling “very sad” and “some sadness,” respectively. Those who conducted more interviews described more symptoms of secondary traumatic stress, including intrusive thoughts and images, and other symptoms of posttraumatic stress. For instance, I3 (16 interviews) expressed feeling “terrified, extremely sad.” Those who conducted more interviews described experiencing a range of negative emotions, for example, an “emotional roller coaster” (I4), “different mood” (I6), or “uncomfortable, uneasy” (I1). One interviewer who conducted 17 interviews shared that he had intrusive thoughts: “In general, when I would have interviews like that, I would think about it for weeks and weeks . . . I’ve thought about it like a couple days ago” (I6). Another interviewer (I4) who had conducted 23 interviews described, “Going home sometimes as much as you try to disconnect, you don’t want to become too invested in their struggles.” She reported that she went home crying after a participant had shared their suicide plan; she stated, “It was very unreal, I have never experienced that . . . I was caught off guard how much it would affect me.” I7 (57 interviews) described having trouble sleeping, as well as experiencing “a sense of sadness mixed with anger, and then a sense of ‘do I even have a right to be angry’?” She said her “emotions were just all over the place.”
Vicarious trauma
Novice interviewers reported beginning stages of vicarious trauma such as “Walking a thin line made me feel I was taking things for granted” (I4), “eye opening” (I4, I5, I7), and a sense of “reality” (I1, I2, I6). For instance, I2 stated, “When you read about things in a book, it’s more of an abstract, but when you see it and it is actually really happening, then it’s reality.” Another described feeling “shattered” and “astounded” by the circumstances of the participants she interviewed. When asked, “What was the most emotionally disruptive thing to hear from a participant while interviewing? How did that make you feel as you heard it? What about afterwards?” she responded, I think that it would be hearing from the participants who slept with the lights on for the past few years because of the trauma that they have experienced and not feeling safe. This participant was employed full-time but sleeping less than 5 hours a night. I believe that was my second interview and I had to pause because it kind of shattered my perception of what mental health looked like. Here was someone who looked like they were functioning but clearly there was this aspect that no one knew about. I think I was astounded at that point. I took a 30-minute break because I had to process everything and take a step back. This is someone who tried to get assistance, but couldn’t get through the whole story. (I7; 57 interviews)
Those who conducted more interviews seemed to experience greater vicarious trauma and discussed examples of how it altered their perception of life in a negative manner. One interviewer (I6; 17 interviews) expressed, After I would interview people, you know, if you think, especially right after, I would go home and kind of think about everything that I was lucky to have. But, sometimes it wasn’t all positive things. There was that end too.
Another reported experiencing changes in worldview: . . . It was sort of just a reality check that everyone goes through trauma throughout their life and they just accumulate these experiences throughout time. I kind of like talked through it with my friends because that was something that was affecting me, and just very sad about how everyone’s going to go through something and it’s just a matter of time. In the moment, I think it was the same thoughts going through my head: “Oh you’re so young and you still have so much to experience and just see how the world works.” (I1; 36 interviews)
Compassion fatigue
Interviewers described compassion fatigue (e.g., feelings of helplessness, exhaustion, and frustration). Participants who conducted fewer than 17 interviews did not express symptoms of compassion fatigue. Interviewers expressed early signs of compassion fatigue by stating they felt helpless: “I wish I could do more to help them” (I6; 17 interviews). Another shared their “frustration that people have to deal with this and there is not anything I can do about it” (I4; 23 interviews). One participant expressed feeling “mentally exhausted” from interviewing participants (I7; 57 interviews). Interviewers also described experiencing conflicting emotions because they felt helpless and wanted to be able to do more for their participants. They mentioned feeling guilty: I felt I had responsibility. [I felt] very uncomfortable when people would talk about monetary questions. I felt guilty for having them come in and desperate for the money, it was a weird trade off in my head. They would talk about how much the money meant to them. I wanted them to feel some sense of control and they were telling me how little money they had. . .I can’t do anything for them beyond giving them the 40 dollars. (I4, how many interviews)
Similarly, another interviewer reported that the most difficult part was knowing that the participants needed so much more than what was currently available and not having the adequate resources to point them to. We had a list of resources, but some of the participants needed so much more than was currently available or known. (I7)
This same interviewer described having a suicidal participant whom she tried to help by calling someone; she wished she “could’ve done more.” Another interviewer mentioned the challenge of seeing participants “leaving the office crying” and not being able to do anything for them: “They asked if I was a therapist and hoped I might be, but were sad when I was not. And at the end of the day, all I was going to do was give them a piece of paper” (I4). An interviewer described this inability to help the participants as “the hardest thing”: “It didn’t feel that there were specific things I could do to help them, which was hard” (I6).
Posttraumatic growth
While interviewers described many instances of secondary traumatic stress and vicarious trauma, they all provided examples of how the experience helped them in a positive way. Several gave examples of posttraumatic growth and shared that conducting these interviews made them feel more optimistic and, for some, inspired activism: “[I have] a lot more hope . . . I want to say I feel more optimistic to speak up about certain issues, especially mental health issues . . . It has made me feel more vocal” (I4) and “This reinforced for me the need to provide greater access to care for this population” (I5). Another interviewer said, “Hearing these people’s experiences solidified my resolve to advocate for those who do not have a voice at all times” (I7) and later commented on her increase for empathy for the participants and individuals in general.
Interviewers also noted a sense of satisfaction from interviewing patients: I feel a satisfaction from interviewing these patients. Mostly because many of the patients thanked me for their experience. . .I felt that gratification almost every time I left. I transformed how I approach patients, I approach them with more care and empathize with their social problems. I became more sensitive and more careful with how I ask these type of questions, and how I interact with patients again with my tone, timing and my diction. (I3)
They noted feeling more appreciative and grateful as a result of conducting the interviews. For example, one interviewer (I4) said that she is now “more mature” and feels “more humble.” She said she did not realize that the experience “would be as impactful as it has been, almost life changing,” and that doing the interviews made her appreciate “the basic needs of life a lot more: housing, clothes, and food.” An interviewer (I2) said she felt “a greater understanding,” a “sense of bless, a very humble experience,” and another reported that hearing people’s stories put things in perspective for her: I would definitely try to think about the stories that were more inspiring than depressing. And would kind of use it to get through things that I was finding difficult at that time. Because I have my own problems, and it helped me that way to think about someone who I interviewed, and they’re still more challenged. So, I think that as a way it helped me a lot. (I6)
Resilience
All but one interviewer commented on participants’ resilience, despite “what was going on in South Central [Los Angeles]” (I2). Interviewers expressed surprise at the resilience they observed among participants they interviewed, despite extensive histories of adversity and trauma. For instance, I5 reported, “For the people I talked to though, it did not seem like they were suffering from mental illness, at least not diagnostically speaking. It really showed me how resilient this group was (and people in general).” Some expressed feelings of awe and inspiration stemming from participants’ stories of resilience: “It was a powerful thing to see them get up and try despite. The fighting spirit and that was amazing” (I4).
Four out of the seven interviewers who were raised in an underserved community themselves expressed feeling resilient as a result of hearing about individuals’ resilience in the community; however, they described experiencing more countertransference and symptoms of secondary traumatic stress stemming from participants with whom they shared similar trauma histories. One interviewer who came from an underserved community and experienced sexual abuse as a child felt “anguished” to hear about participants’ sexual abuse experiences, and “I couldn’t believe how common it was” but also felt “grounded afterwards and at ease because I felt like the patient had been able to overcome and battle those issues.” The interviewer stated that it seemed as if everyone who was interviewed, experienced sexual abuse, and that, “it really struck a chord,” however still was able to recognize the participant’s resilience and strength, and that brought “ease” (I3).
Similarly, I8, who was also raised in an underserved community, “struggled a lot from poverty,” and also experienced trauma from grief and loss, talked about interviewing a participant who was a single dad who had just lost his wife and was faced with poverty. He described feeling “very sad for them but at the same time . . . [They] showed a great deal of resilience and optimism and that gave me hope.” In addition to sharing his identification with the widowed father and recognition of his resilience, he also provided stories of other participants’ struggles with poverty. In response to noticing changes in self-perception, I4 stated, I relate with a lot of these issues that the participants have dealt with. Low SES growing up in the community and a lot of gang violence and drugs growing up and you almost feel insecure or inferior because you have these experiences or . . . I thought my life was bad—they have it worse and I gave myself permission to feel resilient.
Other interviewers minimized their own history of trauma compared with individuals who they identified with. For instance, I6 shared the following story: People would elaborate on things that happened in their life, and it’s similar, like I’ve also been homeless, but I don’t know if we specifically asked about being homeless. We just started talking about it. And you know, well it’s kind of hard going to school. Like I’d hate to compare myself to them. Like there were some similarities, but they didn’t have as many resources as I did.
Similar to other interviewers, I6 also commented on the participant’s resilience: Because some bad things that you’ve gone through, you kind of are reminded when you hear it from other people . . . and I had never gone through so many horrible things, and continued to go on through life. And that was really inspiring.
I1 reported on identifying with participants with depression and PTSD and having secondary traumatic stress from the countertransference: Individuals whom I’ve had a harder time with are those who were kind of telling me about how they were feeling and they were very similar feelings to what I’ve had in the past, participants who were reporting say a lot of symptoms of depression, PTSD, or those emotions . . . those emotions are a lot of what I’ve felt. Only because I’ve struggled with depressive symptoms and just having these heavy emotions, but again like I said, the specific experiences of the participants are different from my own.
However, just like the others, she also commented on the resilience of the participants: “People I’ve found inspiring are people who’ve gone through these experiences and been able to overcome that and be able to get help with these various emotions and process their health or get mental health treatment.”
Self-help and support
Interviewers explained the importance of having the training, skills, and support to be effective at communicating with those who were sharing experiences of trauma. One interviewer noted the difficulty of “being confident in my ability to have these conversations with someone in-person” (I1), while another said that she relied on her “belief in a higher power and making good out of a bad situation” (I2). Interviewers sought support from their peers and research team (I4, I5, and I6); for example, one said that she “talked it through” with her friends and fellow interviewers. Another interviewer appreciated “the sense of teamwork that the whole team had and being supported by peers and staff” (I4). I1, I7, and I8 commented on the need for senior project researchers to be accessible and the importance of training and debriefing: “Having [senior project personnel] accessible made things run much more smoothly. The initial training and debriefing was very beneficial and added to my overall success” (I7), “Having the investigators there made it very helpful” (I8), and “Throughout the course of the study, we always had, or we always tried to have weekly check-ins that [senior project personnel] scheduled with us. And they would ask us how it had been interviewing, if we were taking any of this home with us, and what we kind of did for self-care . . . And then, I had the other resources outside of the study staff, like I mentioned. I journal and I go to see a psychologist” (I1).
Discussion
Novice interviewers, who interviewed community participants about experiences of trauma, described initial symptoms of secondary traumatic stress (i.e., sadness, trouble sleeping, intrusive thoughts, anger, and tearful), vicarious trauma, (i.e., worldview negatively changed and negative outlook on life), compassion fatigue (i.e., frustration, exhaustion, and helplessness), posttraumatic growth (i.e., new appreciation for life, hopeful, inspired, activism, and advocacy), and resilience (i.e., ability to bounce back and recover quickly). They also described the importance of training, debriefing, and self-care. Interviewers who identified with the participants and reported personal circumstances that mirrored those of the participants (e.g., that they grew up in underserved communities or experienced similar forms of abuse) described simultaneous feelings of resilience and secondary traumatic stress from countertransference. The majority of interviewers (seven out of eight) described facing challenges in interviewing, regardless of the number of interviews that they conducted. Interviewers who completed more interviews expressed numerous symptoms including sadness, anger, insomnia, helplessness, and changes in worldview. The two interviewers with previous experience working with trauma expressed fewer symptoms. All interviewers reported feelings of hope and optimism for their participants and an increased appreciation of their resilience. Interviewers noted the importance of training, debriefing, and support in being able to successfully conduct this type of interviewing and were appreciative of the investigators for the time devoted weekly to ensure their well-being.
These results are consistent with those noted in research conducted with seasoned interviewers, who report symptoms of secondary traumatic stress, vicarious trauma, compassion fatigue, posttraumatic growth, and resilience (Barrington & Shakespeare-Finch, 2013; Coles et al., 2014; O’Reilly & Kiyimba, 2015; Richard, 2013; Seedat et al., 2004; Silveira & Boyer, 2015; Sui & Padmanabhanunni, 2016). When asked questions that queried for symptoms of secondary traumatic stress, vicarious trauma, and posttraumatic growth, interviewers provided numerous examples of each. Furthermore, several themes, which we did not directly inquire about (compassion fatigue and resilience), emerged from the data. The interviewers reported experiencing the emergence of postgrowth from secondary traumatic stress and vicarious trauma (Barrington & Shakespeare-Finch, 2013; Silveira & Boyer, 2015; Sui & Padmanabhanunni, 2016); however, they also experienced both negative and positive reactions to trauma-focused research simultaneously (Collins, 2007).
Additional contributions not previously mentioned in the literature are noted below and important differences between secondary traumatic stress, vicarious trauma, and compassion fatigue, which are often discussed interchangeably in the literature. We found evidence for each of these themes among novice interviewers, suggesting that it may not require years of experience to report symptoms in these domains. In fact, it took as few as three interviews for some to begin to experience secondary traumatic stress and posttraumatic growth and as few as 17 interviews to experience the beginning stages of compassion fatigue. The majority of interviewers (n = 7) reported on symptoms of secondary traumatic stress, but not all reported on symptoms of vicarious trauma and compassion fatigue. As the number of interviews increased, the number of symptoms and reactions increased. Our results suggest that it is possible for novices to report experiences of compassion fatigue and posttraumatic growth earlier than previous research. In this study, interviewers reported early symptoms of compassion fatigue and burnout, but simultaneously experienced signs of resilience and postgrowth. In addition, interviewers who had similar shared experiences with those whom they interviewed were more likely to report symptoms of secondary traumatic stress, vicarious trauma, and compassion fatigue.
This study also has limitations, including a small sample size and less than 100% participation from interviewers participated in this study. Eight out of 13 interviewers participated, and it is possible that the additional interviewers’ subjective accounts could have elicited different reactions. In addition, we were unable to determine their reasons for nonparticipation. The interviewers lost to attrition conducted relatively few interviews (between three and four interviews each) and may have experienced reactions that differed from those who conducted more interviews. Thus, we are not able to describe their experiences adequately. Future studies should examine the impact of experiential proximity on interview quality. It would be interesting to study the different entry levels per novice interviewer, their motivation for interviewing, and the reactions to trauma interviewing to see whether secondary traumatic stress, vicarious trauma, and compassion fatigue increase or decrease over time.
Training Issues
There is a lack of research emphasizing the importance of informing novices that these are issues that they need to be aware of. It is imperative for research training to address these commonly experienced reactions, both positive and negative, among interviewers. This is particularly important if interviewers did not go to school to become a helping professional or front-line employee, as well as if the interviewer has past unresolved trauma history. Interviewers should be aware that there is no single way to process the interview experience, and that their thoughts, feelings, and behaviors may differ initially from those experienced as more interviews are conducted and allow for the possibility that they may experience contradictory symptoms that may feel disorienting or confusing. It may be helpful to reassure novices that participants typically report having no regrets about participating in research as well as indicating that they benefited personally from their participation (Newman et al., 1999). Our results suggest that these reactions are not limited to seasoned clinicians.
Novice interviewers should receive training about countertransference and the importance of debriefing and seeking support to offset the vicarious trauma, secondary stress, and compassion fatigue (Coles et al., 2014) they are likely to experience over the course of interviewing, as shown in our results as the amount of interviews increased per interviewer. Novices should understand distinctions between the different terms—secondary traumatic stress, vicarious trauma, compassion fatigue, post traumatic growth, and resilience (Figley Institute, 2012)—as the terms are often used interchangeably among researchers and individuals faced with these reactions. Clarity of terms (even when their co-occurrence is acknowledged) is important to be able to recognize the warning signs and address negative symptoms with proper resources, training, and support. It is critical to address these issues among novice clinicians in graduate school and medical school, as paraprofessionals are more likely to conduct this work in the real world. Given differences in training, resources available, length of time associated with a specific research project, and treatment for previous personal experiences with trauma, it is important to highlight the needs of novice trauma interviewers to support their well-being as well as the well-being of those they interview.
Importance of self-care to address secondary traumatic stress, vicarious trauma, and compassion fatigue
To prevent and/or address secondary stress, vicarious trauma, and compassion fatigue that occur among trauma interviewers and to promote resilience and posttraumatic growth, the importance of self-care should be incorporated into training and supervision of trauma interviewers. Various self-care strategies have been identified as effective in helping reduce the heightened anxiety and emotional dysregulation that can result from hearing detailed experiences of trauma (Mathieu, 2012). Many of the self-care strategies that have been utilized by clinicians and other front-line staff can be effectively used by novice interviewers. Such practices include mindfulness, meditation and grounding, deep breathing, and physical exercise (Tang et al., 2007). Peer support, a strategy used by the interviewers in this study, is another effective self-care strategy that can decrease feelings of isolation and provide validation of similar feelings from colleagues (Solomon, 2004). Peer support group models have been used effectively for interpreters working with trauma survivors (Anderson, 2011). Support can take place through informal meetings with peers. A more formal structure of regularly scheduled peer-to-peer individual or group supervision and debriefing meetings are also helpful. With more formal peer supervision and debriefing, it is important to provide training in facilitation and debriefing skills. These opportunities allow peers to share in similar emotional reactions to their work and effective coping strategies (McCann et al., 2013). Such practices can be similarly adapted for use with novice trauma interviewers.
Importance of supervision
Trauma-informed supervision of novices conducting trauma interviews is a fundamental component of the individual’s well-being and depends on their background (whether student or community stakeholder), their support, education, and growth. A trauma-informed supervisor is equipped to assist the trauma interviewer to prepare for a range of potential positive and negative emotional effects of interviewing trauma survivors. Supervision should be focused on minimizing and managing emotional distress experienced by interviewers (Urquiza et al., 1997). Although more research is needed, themes that emerged among this group of novice interviewers suggest that supervision should include psychoeducation regarding traumatic stress, vicarious traumatization, compassion fatigue, resilience, and posttraumatic growth. Addressing these issues is important to prepare interviewers to not only help them understand what to expect but also normalize and manage the emotional impact of co-occurring positive and negative effects as well as anticipating possible changes over time so that they can maximize their effectiveness when interviewing community individuals. Recruitment of research personnel, initial and ongoing training, and structuring regular interviewer team meetings are important components for trauma interviewers. It is proposed that the safety and emotional health of both the respondent and the interviewer should always take priority over data collection. With this in mind, it is particularly important to set up procedures for interviewers to follow before, during, and after an interview to address the emotional impact of the traumatic information that they receive. For example, interviewers are trained on self-regulation and coping techniques to use when emotions are triggered before and after the interview. However, during an interview, it may be more difficult to use such strategies. Therefore, it is important for the interviewer to have specific techniques that can be used if triggered that may be less disruptive, such as deep breathing, and other grounding techniques, such as mental and soothing strategies (Navajitz, 2002). If such techniques are not effectively helping the interviewer during the interview, procedures on taking breaks during interviews and consulting with supervisors during interviews should be put in place.
Although the interviewers experienced negative reactions, each expressed feelings of gratitude and indicated that they had benefited from the experience. The majority of the interviewers in this study came from underserved communities. Their participation in trauma research was a way to give back to the community by being part of an effort to describe the various traumatic experiences experienced by individuals, potentially informing future prevention and/or intervention efforts. These experiences brought out a sense of advocacy in these novices and increased their awareness of the numerous obstacles and traumatic experiences community individuals often face. Conducting the life experience assessments gave the majority of the interviewers much needed clinical experience and allowed them to experience reactions that will help them to become effective helping professionals. Training and supervision that highlights these common reactions can ultimately help novices to monitor and preserve their own well-being as well as those they serve.
Footnotes
Appendix
Acknowledgements
The authors would like to thank all the UCLA Centers of Excellence (COE) interviewers who participated in this research; Whitney Cale and David Patron for assisting with collecting and analyzing data; and Alex Kim for assisting with formatting. In addition, the authors would like to acknowledge the funding by the UCLA COE with funds through the California Department of Mental Health.
Authors’ Note
Jennifer Pemberton is also affiliated with California State University, Northridge, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for this article through the California Department of Mental Health.