
Abstract
Sexual revictimization refers to exposure to more than one incident of rape and is a known risk factor for poor mental health among civilians. This construct has been understudied among veterans. In addition, although individuals who have experienced revictimization generally have greater symptom severity than those who have experienced one rape, it is unclear whether these differences persist following treatment. This study examined differences between veterans who reported histories of revictimization (n =111) or a single rape (n = 45), over the course of a 3-week intensive cognitive processing therapy (CPT)-based treatment program for veterans with posttraumatic stress disorder (PTSD). The sample consisted of predominately female (70.5%) post–9/11 veterans (82.7%). Self-reported PTSD and depression symptom severity were assessed regularly throughout the course of treatment. Controlling for non-interpersonal trauma exposure and whether veterans were seeking treatment for combat or military sexual trauma, sexual revictimization was generally associated with greater pretreatment distress and impairment. However, sexual revictimization did not impact rates of PTSD or depression symptom change over the course of intensive treatment, or overall improvement in these symptoms posttreatment. Our findings suggest that the rates of sexual revictimization are high among treatment-seeking veterans with PTSD. Although veteran survivors of sexual revictimization tend to enter treatment with higher levels of distress and impairment than their singly victimized peers, they are equally as likely to benefit from treatment.
The term sexual revictimization refers to the experience of more than one incident of nonconsensual sexual activity. Some have used the term to refer specifically to individuals who have experienced nonconsensual sexual activity both in childhood and adulthood (Charak, DiLillo, Messman-Moore, & Gratz, 2018; Ullman & Peter-Hagene, 2016), childhood and adolescence (Hannan, Orcutt, Miron, & Thompson, 2017), or repeated incidents during adolescence and adulthood (Najdowski & Ullman, 2011). Other studies use a restrictive definition of the nonconsensual sexual activity encompassed by revictimization, such as rape (i.e., oral, vaginal, or anal penetration obtained by force or incapacitation; Walsh, Danielson, McCauley, Saunders, & Kilpatrick et al., 2012), while even other studies have included a more broad range of coercive tactics (Asoved, Long, & Voller, 2011; Brousseau, Hébert, & Bergeron, 2012) or type of contact obtained (Hannan et al., 2017; Najdowski & Ullman, 2011; Ullman & Peter-Hagene, 2016).
Sexual revictimization is alarmingly common among individuals who have experienced sexual assault and has a significant negative impact on mental health. For example, among women who have been raped, over half experience more than one rape (Bostock & Daley, 2007; Walsh et al., 2012). Individuals who have experienced sexual revictimization are at increased risk for developing symptoms of posttraumatic stress disorder (PTSD; Walsh et al., 2012), report greater general mental health symptom severity (Asoved et al., 2011; Creech & Orchowski, 2016; Hannan et al., 2017; Najdowski & Ullman, 2011; Ullman & Peter-Hagene, 2016), and report experiencing increased difficulty with emotion regulation (Charak et al., 2018). Notably, only one study on the impact of revictimization on mental health to date has included veterans (Creech & Orchowski, 2016), who were all female. The one study to date among men (Asoved et al., 2011) was in a civilian sample. In addition, although revictimization is clearly linked to the development of distress and impairment, less is known about whether differences between singly and revictimized individuals persist following treatment.
Despite the relative dearth of studies examining the impact of revictimization on treatment outcomes, insights might be gathered from studies that evaluate sexual assault characteristics more broadly. One study of veterans with a history of military sexual trauma (MST) who received outpatient (i.e., weekly) cognitive processing therapy (CPT) found no differences between those with and without a history of childhood sexual abuse in baseline PTSD severity or rate of change in PTSD symptoms over the course of the therapy (Holder, Holliday, & Surís, 2019). One notable caveat is that it is unclear whether individuals without a history of childhood sexual abuse in this study may have experienced revictimization during other developmental time periods. In a comparative treatment study examining prolonged exposure, stress inoculation training, and a combination therapy for adulthood sexual assault survivors, childhood abuse (i.e., physical or sexual abuse or witnessing extreme violence within the family) was associated with greater posttreatment PTSD severity while controlling for baseline symptoms (Hembree, Street, Riggs, & Foa, 2004). In the same study, adulthood sexual assault prior to the index trauma was not significantly related to posttreatment PTSD severity. Thus, although these results indicated that repeat adulthood sexual assaults may not impact posttreatment symptoms, it is unclear whether the posttreatment differences associated with child abuse reflected cases where the child abuse had been sexual in nature.
Limiting revictimization studies to only those who have experienced an assault specifically in childhood and adulthood could hamper our understanding of repeated victimization. Research has demonstrated that both adolescent and adulthood sexual assaults significantly impact risk for later victimization and subsequent psychopathology (Miron & Orcutt, 2014; Rich, Gidycz, Warkentin, Loh, & Weiland, 2005; Ullman & Peter-Hagene, 2016). Consequently, this study defined revictimization to include more than one experience of attempted rape or rape at any point in an individual’s life. We also focus on experiences of attempted rape or rape, considering that assault perpetrated with more violent and forceful tactics is more strongly associated with mental health symptom severity in general (Brown, Testa, & Messman-Moore, 2009; Peter-Hagene & Ullman, 2015) and worse treatment outcomes compared to other forms of nonconsensual sex (Hembree et al., 2004).
To address presently unanswered questions about the impact of sexual revictimization on pretreatment mental health and treatment outcomes, this study examined the impact of sexual revictimization on distress and impairment among male and female veterans with PTSD who underwent a 3-week intensive CPT-based treatment program. Based on prior research, we expected that revictimized veterans would report greater distress and impairment prior to the initiation of the treatment, as indicated by greater depression, posttraumatic stress, and negative posttraumatic cognitions as well as less satisfaction with their participation in social roles compared to singly victimized veterans. To examine potential treatment differences, the rates of posttraumatic stress and depressive symptom change over the course of therapy, and overall symptom improvement were also compared between the two groups. These analyses were approached in exploratory fashion given the lack of existent research on revictimization on treatment outcomes.
Method
Participants
The sample for this study consisted of 156 veterans and service members (92.3% discharged/retired, 7.7% on active duty, reserves, or National Guard; hereafter collectively referred to as veterans) who were enrolled in a 3-week intensive treatment program (ITP) for PTSD at The Road Home Program, a non-VA mental health clinic, between May 2016 and March 2019. All veterans in this sample endorsed having experienced attempted rape or rape at some point in their lives. Veterans attended either a MST (n = 120) or combat trauma cohort (n = 36). When veterans reported both MST and combat exposure, the decision of which cohort to attend was made jointly between the veteran and intake clinician. In some cases, veterans do not disclose or minimize the impact of their history of MST during the intake process, despite being screened for MST exposure. Data from individuals who had attended both cohorts were collapsed for this study due to the prevalence of sexual trauma in both groups.
The sample comprised 110 female (70.5%) and 46 male (29.5%) veterans. Gender was not significantly associated with revictimization status, χ2 (1, N = 156) = 3.36, p = .067. The average age of participants was 42.0 years (SD = 10.4, range = 24–70 years), and the majority of participants screened positive for MST (95.5%) on intake questionnaires. The mean number of non-interpersonal trauma types experienced was 7.21 (SD = 3.32, range = 0–13). Among the sexual trauma survivors in the MST cohorts, 85% identified a sexual trauma as their index trauma, compared to 8% in combat trauma cohorts. Additional demographic and clinical characteristics are displayed in Table 1. Portions of this sample have previously been published on (Carroll, Lofgreen, Weaver, Held, & Klassen et al., 2018; Held, Klassen, Boley, Wiltsey Stirman, & Smith et al., 2019; Horwitz, Held, Klassen, Karnik, Pollack et al., 2018; Zalta, Held, Smith, Klassen, & Lofgreen et al., 2018)
Demographics and Clinical Characteristics.
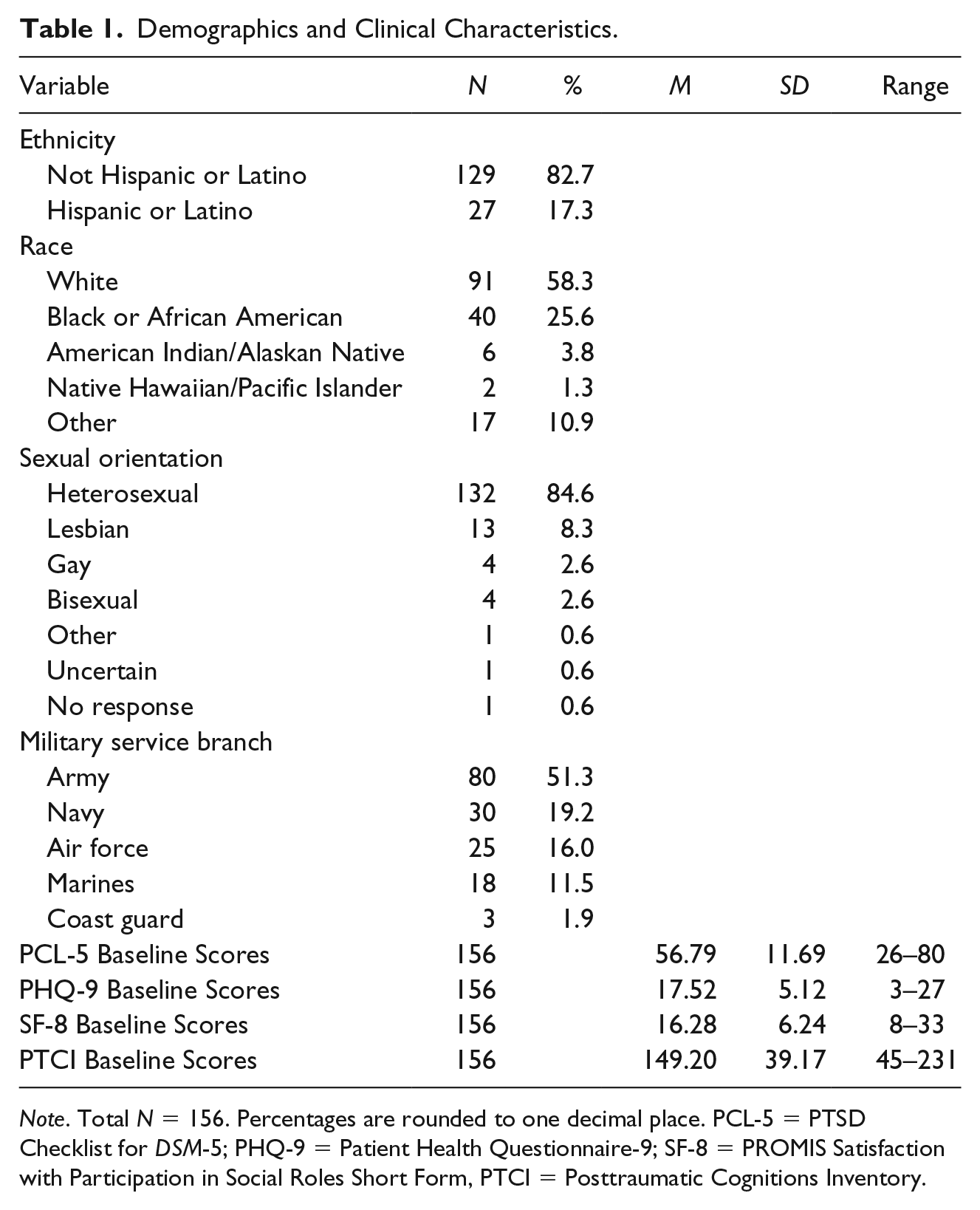
Note. Total N = 156. Percentages are rounded to one decimal place. PCL-5 = PTSD Checklist for DSM-5; PHQ-9 = Patient Health Questionnaire-9; SF-8 = PROMIS Satisfaction with Participation in Social Roles Short Form, PTCI = Posttraumatic Cognitions Inventory.
Procedures
The ITP program attended by participants lasted 3 weeks, consisting of 15 days of treatment in an outpatient clinic, delivered over 19 days. Veterans attended individual and group CPT sessions daily. Consistent with the CPT protocol, veterans are encouraged to identify an index trauma (Resick, Monson, & Chard, 2016, p. 94); however, in cases of multiple traumas, clinicians attempt to address major assimilated stuck-points related to various traumas. Veterans also participated in secondary intervention components including mindfulness, yoga, fitness, nutrition, psychoeducation, art therapy, and case management, with the option to receive medication management, acupuncture, spiritual care, or massage therapy as needed. Programming is nearly identical across cohorts; however, MST cohort participants are more routinely exposed to fellow cohort members challenging negative sexual victimization-related beliefs in CPT group, compared to combat cohort participants. A full description of the ITP and its components can be found in (Held et al., 2019; Zalta et al., 2018).
Information collected during the intake evaluation within 2 weeks prior to the start of the ITP included demographic information, trauma history, satisfaction with social role participation, posttraumatic stress symptoms, and depression symptoms. Posttraumatic stress symptom severity was also assessed approximately every other day for a total of 10 times throughout the ITP, including a posttreatment assessment collected on the final day. Depression severity was assessed every other day, for a total of eight times over the same period. This study was approved by the Institutional Review Board at Rush University Medical Center. As all assessments were collected as part of routine clinical care, a waiver of consent was obtained.
Measures
Demographics
Demographic information, such as age, sex, race, ethnicity, education level, branch, service era, and last or current military pay grade, was assessed when participants first made contact with the program and during the intake evaluation. History of MST is also reported, to help describe trauma exposure in the sample. It was assessed using a two-item MST screen (McIntyre, Butterfield, Nanda, Parsey, & Stechuchak et al., 1999): (a) Did you receive uninvited and unwanted sexual attention, such as touching, cornering, pressure for sexual favors, or verbal remarks? (b) Did someone ever use force or threat of force to have sexual contact with you against your will? These items are standard in the Veterans Health Administration universal screening for sexual harassment and assault and have demonstrated high sensitivity among women (Kimerling, Gima, Smith, Street, & Frayne, 2007; McIntyre et al., 1999). Participants were coded as reporting MST if they endorsed either item.
Trauma History Questionnaire
The Trauma History Questionnaire (THQ) is a 21-item self-report measure that was adapted from the Traumatic Events Questionnaire (Vrana & Lauterbach, 1994) and the Life Events Checklist (Blake, Weathers, Nagy, Kaloupek, & Gusman et al., 1995) to assess lifetime exposure to Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5; American Psychiatric Association, 2013) traumatic events. For each endorsed event, respondents choose from the following options regarding the stage of life when the event occurred and the frequency: once during childhood (age 0–16), multiple times during childhood, once in adulthood (age 17 and older), multiple times in adulthood, and multiple times in childhood and adulthood. Participants were considered singly victimized if they endorsed one occurrence in response to the question, “Have you ever been sexually assaulted (e.g., attempted rape, made to have intercourse, oral or anal sex against your will)?” They were categorized as revictimized if they reported that this occurred more than once during any developmental time period(s). A non-interpersonal trauma control variable was also created, based on categorization of trauma types in prior research (Iverson et al., 2013), using items 1 to 5, 8 to 9, 11 and 12, 15 to 17, and 21 of the THQ. Items from this pool (e.g., fire or explosion, transportation accident, and seeing dead bodies), for which participants reported having an exposure, were summed such that the total score indicates the number of non-interpersonal trauma types experienced. This variable did not include traumas such as physical assault or assault with a weapon due to the possibility that these traumas could include experiences such as childhood physical abuse or intimate partner violence. Internal consistency is not reported because checklists for low-frequency events violate the assumptions of this statistics (Turner & Wheaton, 1995).
PTSD checklist for DSM-5 (Weathers, Litz, Keane, Palmieri, & Marx et al., 2013)
The PTSD checklist for DSM-5 (PCL-5) is a 20-item self-report measure of PTSD symptom severity over the past month on a scale from 0 (not at all) to 4 (extremely), with higher scores reflecting more severe PTSD symptoms. Every other day during the ITP, veterans reported their PTSD symptom severity over the past week. When completing the measure, veterans rated their symptoms in relation to a self-reported index trauma. Veterans’ written descriptions of their index traumas on their posttreatment survey were coded as either likely related to sexual victimization or to other trauma. In the 22 cases where veterans’ description was ambiguous (e.g., “the first time it happened”) or missing for that time point, the index trauma from the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5; Weathers et al., 2018), was used to code this variable. The PCL-5 has been shown to be a reliable and valid measure of PTSD symptom severity in veteran and military populations (Bovin, Marx, Weathers, Gallagher, & Rodriguez et al., 2016; Wortmann, Jordan, Weather, Resick, & Dodanville et al., 2016). Internal consistency in the present sample at baseline was good (α = .89).
Patient Health Questionnaire-9 (Kroenke, Spitzer, & Williams, 2001)
The Patient Health Questionnaire-9 (PHQ-9) is a 9-item self-report measure of depression symptoms occurring in the past 2 weeks. Respondents rate items from 0 (not at all) to 3 (nearly every day). Higher scores reflect greater depression symptom severity. This measure has demonstrated good reliability and validity in a variety of populations, including veterans (Corson, Gerrity, & Dobscha, 2004). Internal consistency in the present sample at baseline was good (α = .82).
Posttraumatic Cognitions Inventory (Foa, Ehlers, Clark, Tolin, & Orsillo, 1999)
The Posttraumatic Cognitions Inventory (PTCI) is a 33-item self-report scale that measures thoughts and beliefs that have developed after exposure to a traumatic event, including self-blame, negative cognitions about the self, and negative cognitions about others and the world. Veterans completed this measure at intake. Items are rated from 1 (totally disagree) to 7 (totally agree), with higher scores indicating stronger negative posttrauma cognitions. The PTCI has demonstrated strong reliability and validity (Foa et al., 1999) and is frequently used in military populations with PTSD (Sexton, Davis, Bennett, Morris, & Rauch, 2018). Internal consistency in the present sample at baseline was excellent (α = .96).
PROMIS satisfaction with participation in social roles short form (Cella, Riley, Stone, Rothrock, & Reeve et al., 2010)
The PROMIS Satisfaction with Participation in Social Roles Short Form (SF-8) is an 8-item self-report measure assessing subjective satisfaction with participation in various social roles in different domains of daily life. Veterans completed this measure at intake. Items are rated from 1 (not at all) to 5 (very much), with higher scores indicating greater satisfaction. The PROMIS Social Function measures have demonstrated reliability and validity in a range of clinical populations (Hahn, Beaumont, Pilkonis, Garcia, & Magasi et al., 2016). Internal consistency in the present sample was excellent (α = .91).
Statistical Analysis
Initial examination of baseline differences in PCL-5, PHQ-9, PTCI, and SF8, as well as post-ITP differences in PCL-5 and PHQ-9 were explored via multiple linear regression analyses adjusting for non-interpersonal trauma exposure and cohort type. Adjustment for multiple comparisons was made using Hochberg’s step-up procedure (Hochberg, 1988). Standardized coefficients were reported to illustrate effect sizes for comparisons while adjusting for covariates. Longitudinal analysis of change in PCL-5 and PHQ-9 over time was conducted using mixed-effects regression models. This approach allows for some missing-at-random data across time points, models individual change, and has less restrictive assumptions regarding variances and covariances over time. Victimization status (single vs. repeated victimization) was examined as a predictor of both outcomes over time, and the interaction between victimization status and time was examined to assess whether changes across time differed between victimization groups. Due to our specific interest in potential similarity of change over time and the inability of traditional significance testing to establish similarity of group change, nonsignificant interaction terms were followed by tests of noninferiority of pre–post change scores between the two groups using the two one-sided tests (TOST; Schuirmann, 1987) method. This procedure establishes non-inferiority if the 90% confidence interval for the difference between comparison groups falls fully within a pre-established equivalence margin. The margin utilized here was 10 points for the PCL-5 and 5 points for the PHQ-9 (McMillan, Gilbody, & Richards, 2010; Wortmann et al., 2016). All models were adjusted for the presence of total of non-interpersonal trauma types, to account for the possibility that greater distress and impairment among revictimized individuals is due to greater trauma exposure more generally. Models were also adjusted for cohort type (i.e., combat trauma or MST).
Results
Seventy-one percent of the sample reported experiencing more than one rape during their lifetime. Baseline differences between victimization groups were statistically significant following correction for multiple comparisons for posttraumatic stress symptom severity (b = –.33, p < .001), depression symptom severity (b = –.25, p = .002), negative posttraumatic cognitions (b = –.28, p = .001), and satisfaction with participation in social roles (b = .22, p = .007). Post-ITP differences were not significant for posttraumatic stress (b = –.14, p = .104) or depression (b = –.16, p = .067). Effect sizes for both preprogram and postprogram comparisons in these measures were all small, though they were slightly smaller at postprogram comparisons.
Mixed-effects longitudinal modeling results suggested that both random intercept and slope components were associated with better model fit for longitudinal modeling of posttraumatic stress and depression (p < .001). A quadratic time component was significant for posttraumatic stress change over time (p < .001) but not for PHQ (p = .563). Overall differences across time between victimization groups were significant for both posttraumatic stress (b = −6.07, p = .004) and depression (b = −2.55. p = .007). The interaction between victimization status and time was not significant for posttraumatic stress (b = 0.25, p = .373) or depression (b = 0.05, p = .600) suggesting the lack of evidence for differential change in either outcome during the program. Follow-up noninferiority tests comparing pre–post posttraumatic stress and depression symptoms change scores between the two groups supported the equivalence of the programmatic change in the two groups, with 90% CIs for PCL-5 (90% CI: −8.70 to 2.41) and PHQ-9 (90% CI: −2.54 to 1.42) falling within the established equivalence margins.
Although not the primary outcome for this study, further data are provided on treatment outcomes for illustrative purposes. Across victimization groups, 63% of participants experienced significant reductions in PCL-5 scores, with 41% falling below the likely diagnostic cutoff for this measure (Bovin et al., 2016). Fewer veterans (39%) experienced improvements in depression, with 35% falling below the cutoff for moderate depression posttreatment (Kroenke et al., 2001). Finally, post hoc analyses were conducted to examine whether the lack of posttreatment differences could be explained by revictimized individuals, who started the program with greater distress, being more likely to drop out of treatment. Only 10 individuals failed to complete the program and these veterans did not differ from completers in victimization status χ2 (1, N = 156) = .65, p = .48.
Discussion
This study was one of the first to examine the associations between revictimization and mental health symptoms among veterans, as well as one of only a few studies to examine this phenomenon in a mixed-gender sample. Rates of revictimization were high in our treatment seeking sample of individuals who reported at least one experience of sexual victimization. Consistent with expectations, results indicated that revictimization was associated with greater PTSD and depression symptom severity, negative posttraumatic cognitions, and lower satisfaction with participation in social roles at the initiation of the 3-week CPT-based ITP. These findings were consistent, even controlling for individuals’ exposure to non-interpersonal trauma. Thus, our study suggests that experiencing multiple rapes may confer unique risk for poor mental health, more so than experiencing a single rape or numerous noninterpersonal traumas more broadly. This is not surprising, given that being raped, even as a single event, has been shown to be associated with a higher risk for PTSD than other types of traumas (Iverson et al., 2013). Although the magnitude of the association between victimization and pretreatment distress and impairment was small, it is also robust, given that analyses controlled for exposure to other types of trauma.
Revictimization status did not impact the rate of symptom change across the course of 3-week CPT-based ITP (Figures 1 and 2). In other words, individuals who reported a single or more than one rape experienced similar PTSD and depression symptom improvements. By the conclusion of treatment, there were no statistically significant or clinically meaningful differences. These findings suggest that although revictimized individuals enter treatment with higher levels of distress and impairment, they are equally as likely to benefit from the 3-week CPT-based ITP as their peers who have experienced a single rape. However, it is also notable that although the majority of patients in this sample experienced reductions in PTSD symptoms over the ITP, a majority also continued to report symptom severity consistent with a likely PTSD diagnosis. Thus, PTSD treatment for veteran sexual assault survivors can still be improved.

Veterans’ depression symptom severity over the course of the 3-week CPT-based ITP, according to sexual victimization status.

Veterans’ posttraumatic stress symptom severity over the course of the 3-week CPT-based ITP, according to sexual victimization status.
The findings from this study hold implications for treatment planning with sexual trauma survivors. It is a common assumption that, particularly in cases of repeated interpersonal trauma exposure, patients need a period of stabilization prior to directly processing traumatic experiences (Herman, 2015). The stabilization period would typically involve forming a trusting relationship with the therapist, learning adaptive coping skills, and ensuring the patient’s access to basic resources. Only after patients have reached stabilization would the therapist initiate trauma-focused treatment. Such stage-based models of trauma treatment have been incorporated into MST treatment programs (e.g., Johnson, Robinett, Smith, & Cardin, 2015). Although stabilization treatment components may be beneficial to some patients, their delivery during a preliminary treatment stage may delay patients’ access to trauma processing components that are most likely to drive significant symptom reductions. Our results suggest that, at least in cases of sexual revictimization specifically, revictimized individuals are just as likely as singly victimized individuals to experience significant treatment gains when trauma-focused treatment is delivered from the onset of the ITP without an initial stabilization phase. Post hoc analyses also suggested that revictimized individuals are not more likely to drop out of this type of treatment.
Several limitations need to be considered. One limitation of this study is the use of a dichotomous variable to assess revictimization status, which limits our ability to examine variability among individuals who have been revictimized. For example, one study of veterans found that women who reported a history of sexual assault reported experiencing an average of seven incidents (Booth, Mengeling, Torner, & Sadler, 2011). This is consistent with our knowledge about sexual assault in the population at large, with research indicating that data tend to be positively skewed and kurtotic (Swartout, Thompson, Koss, & Su, 2015). In other words, a relatively small portion of people experience rape, but a large portion of those individuals experience a high number of assaults. Although dichotomizing sexual victimization exposure is a common practice in the literature, it may be more clinically useful to understand the relative increase in distress and impairment conferred by each additional victimization experience. Similarly, research also suggests that sexual victimization survivors more often than not have experienced emotional and physical abuse (Paranjape & Liebschutz, 2003; Simmel, Postmus, & Lee, 2016). Our study was unable to disentangle the impact of repeated rapes versus cumulative interpersonal trauma more generally due to the way in which the data were captured. Furthermore, as all experiences of rape were assessed retrospectively, we are unable to differentiate whether our findings were related to revictimization specifically, versus other long-term consequences of repeated victimization such as maladaptive coping (Najdowski & Ullman, 2011), poor interpersonal functioning (Rich et al., 2005), or negative beliefs about treatment (Simmel et al., 2016).
Our findings also suggest several avenues for future research. Although this study focused on experiences of rape and attempted rape, other types of nonconsensual sex, such as those compelled by verbal sexual coercion, have also been linked with adverse symptoms (Brown et al., 2009; Testa & Dermen, 1999). Verbal sexual coercion is also more prevalent than physically forced sexual assault (Brown et al., 2009) and can occur frequently within the context of a single relationship (Katz, Kuffel, & Brown, 2006). Future research could compare the impact of frequent exposure to verbal coercion and rape-related revictimization on treatment outcomes. As this study comprised of a treatment-seeking sample, it is unclear whether the degree of sexual victimization influences whether individuals seek treatment in the first place. Even though the proportion of revictimized individuals in this sample was large, it is still possible that survivors who have experienced repeated rapes have greater shame and self-blame such that they are less likely to initiate care. It is also notable that a third of our sample was male, given that revictimization research has almost exclusively focused on women. Future research should include mixed-gender samples to better understand the impact of rape on all survivors and avoid perpetuating the stereotype that men cannot be raped. Greater representation of transgender and sexual minority veterans is also needed in this line of research due to their elevated risk for lifetime sexual victimization (Beckman, Shipherd, Simpson, & Lehavot, 2018; Lehavot & Simpson, 2014; Mattocks, Sadler, Yano, Krebs, & Zephyrin et al., 2013).
In sum, this study demonstrated that a high percentage of treatment-seeking veterans with histories of rape have experienced more than one rape, regardless of their gender. Despite reporting more distress and impairment at the onset of treatment, revictimized veteran’s PTSD and depression symptoms improved as much and as quickly as those of their singly victimized peers, such that differences between groups were nonexistent at posttreatment. Although our study was unable to account for the impact of larger numbers of sexual assault or other types of co-occurring interpersonal trauma, it provides preliminary evidence that survivors of repeated sexual trauma can benefit from rapid initiation of intensive trauma-focused treatment.
Footnotes
Acknowledgments
The authors thank the Wounded Warrior Project for their support of the Warrior Care Network and the resulting research. They also thank the participating veterans and their families, as well as acknowledge the administrators, research assistants, and clinicians at the Road Home Program. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, Wounded Warrior Project, or any other funding agency.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: P.H. receives grant support from the Boeing Company and the Robert R. McCormick Foundation. M.P. receives support from the Wounded Warrior Project and research funding from National Institute of Health and Janssen Pharmaceuticals; he provides consultation to Aptinyx, Clintara, and Palo Alto Health Sciences; he has equity in Argus, Doyen Medical, Mensante Corporation, Mindsite, and Targia Pharmaceuticals; he receives royalties from SIGH-A and SAFER interviews.