
Abstract
This study examined the elevated risk of intimate partner violence (IPV) among persons with mental health-related disabilities (MH-RD) and the extent to which known risk factors accounted for this phenomenon. Data were drawn from a nationally representative sample of 33,127 Canadians collected in 2014 as part of Statistics Canada’s General Social Survey. Results showed that respondents with MH-RD had more than three-fold increased odds of both overall and severe IPV victimization. Although females were more likely to possess a MH-RD, males and females with MH-RD reported similarly elevated odds of IPV victimization. Risk factors that contributed to a significant reduction in elevated odds of IPV for respondents with MH-RD were child maltreatment (CM), respondents’ nonprescription drug abuse, and perpetrators’ jealous, monitoring, and socially isolating behaviors. The inability to test additional risk factors and bidirectionality in the relationship between MH-RD and IPV may have contributed to the failure to fully account for these respondents’ elevated odds of IPV. Future research is needed to understand the complex mechanisms contributing to the elevated risk of IPV and enhance prevention and intervention strategies for this underresearched and underserved vulnerable population.
Approximately 15% of the world’s population, representing more than a billion people, live with a disability (World Health Organization and The World Bank, 2011). Disabilities include physical (mobility, flexibility, dexterity, pain), sensory (seeing, hearing), cognitive (learning, developmental, memory), and mental health-related impairments (Grondin, 2016). Disability is a well-established risk factor for violent victimization, with persons having mental health-related disabilities (MH-RD; for example, anxiety, depression, bipolar disorder) facing a particularly high risk (Gearon & Bellack, 1999; Goodman et al., 2001; Khalifeh & Dean, 2010; Mikton et al., 2014). Although a variety of perpetrators, such as personal care assistants, health care providers, and strangers may commit violence against persons with disabilities, there are indications that intimate partners are the most common perpetrators (Ballan et al., 2014; Martin et al., 2006; Milberger et al., 2003; Ridington, 1989; Young et al., 1997). Indeed, in addition to the aforementioned high risk of violent victimization in general, persons with MH-RD also represent a highly vulnerable population for intimate partner violence (IPV) victimization (Du Mont & Forte, 2014; Friedman & Loue, 2007; Hughes et al., 2012; Machisa et al., 2017; Nathanson et al., 2012; Trevillion et al., 2012).
Despite evidence for an elevated risk of IPV against persons with MH-RD, our review uncovered only two studies that examined the operation of risk factors that may underlie this association. Using nationally representative data from Statistics Canada’s 2009 General Social Survey (GSS), Du Mont and Forte (2014) analyzed social capital risk factors for women’s IPV victimization by current or former partners. 1 They found social capital factors (weaker sense of belonging to their community, lower levels of trust toward others, less likely to report living in a welcoming community, and discrimination) to be associated with women having a MH-RD. They then ran a regression with these factors along with sociodemographic risk factors (age, marital status, and annual household income) and found all of them to be significant predictors of IPV. Interestingly, based on our comparison of their regression analysis to the prevalence rates reported in their article, the elevated odds of IPV for those with MH-RD appeared to be unaffected by adjusting for these risk factors, 2 thereby suggesting that they were not implicated in these women’s elevated odds of IPV.
The second study of risk factors examined the role of a personal history of child maltreatment (CM) in IPV risk among women with MH-RD (Machisa et al., 2017). There are indications in the literature that persons with disabilities are more likely to have experienced maltreatment in childhood (Ballan et al., 2014; Friedman & Loue, 2007; Goodman et al., 2001; Lightfoot & Slayter, 2014; Schröttle & Glammeier, 2013). Machisa et al. (2017) analyzed data from a representative sample of 501 women in Gauteng Province of South Africa. They found that mental health problems (measured by PTSD, depression, and binge drinking) mediated the relationship between CM and past-year IPV, thereby demonstrating CM to be a potentially important risk factor for understanding the elevated risk of IPV among persons with MH-RD. Machisa et al. (2017) noted, however, that their study was limited by the exclusion of a number of other well-established risk factors for IPV in an integrated ecological framework.
Research on disabilities and IPV using an ecological approach, which directs attention to risk factors including victim-related characteristics, perpetrator-related characteristics, and relationship factors (Brownridge, 2006a; Sobsey & Calder, 1999), has repeatedly shown that perpetrator-related characteristics (partner’s domineering, jealous, possessive, and substance abusing behaviors) are crucial for understanding the elevated risk for persons with disabilities in general. Using nationally representative Canadian data, Brownridge (2009) identified an apparent widening of the gap in risk of IPV for women with disabilities relative to women without disabilities between 1993 and 2004. By 2004, the gap in risk had increased to the point that these perpetrator-related variables could no longer fully account for these women’s elevated odds of IPV (although they appeared to be reduced with these adjustments; odds ratio (OR) = 1.85, p < .01; adjusted odds ratio (AOR) = 1.67, p < .05). A subsequent analysis of data from the 2009 Canadian GSS (cf. Brownridge et al., 2016) showed that adjustments for these perpetrator-related characteristics significantly reduced, but did not fully account for, the elevated odds of IPV for persons with physical disabilities (OR = 1.71 vs. AOR = 1.24, t = 8.86, p < .001), nonphysical disabilities (OR = 2.20 vs. AOR = 1.55, t = 9.71, p < .001), and multiple disabilities (OR = 2.86 vs. AOR = 1.88, t = 10.60, p < .001).
Overall, there are strong indications that persons with MH-RD are at elevated risk for IPV and research is needed to determine the extent to which a history of CM, perpetrator-related characteristics, as well as additional risk factors from an ecological framework contribute to understanding this phenomenon. This study, then, analyzed a large-scale nationally representative sample of noninstitutionalized Canadians to meet the following objectives: (a) establish the extent to which persons with MH-RD in Canada have an elevated risk of IPV compared with those who do not have MH-RD; (b) compare those with and without MH-RD in terms of CM, perpetrator-related, and other risk factors for IPV; and (c) identify the extent to which differences in these risk factors explain the elevated risk of IPV against persons with MH-RD.
Materials and Methods
The Data Set
We used data from Cycle 28 of Statistics Canada’s GSS, which was conducted in 2014. 3 The 2014 GSS surveyed a random sample of 33,127 noninstitutionalized persons aged 15 years and older living in the 10 Canadian provinces, with a response rate of 52.9% (Statistics Canada, 2016a). Respondents completed in-depth telephone interviews concerning the nature and extent of their criminal victimization, including experiences of IPV. Because this study concerned IPV by current partners, we selected a subsample of 17,643 respondents who were married/living common-law at the time of the survey. A MH-RD was indicated if a respondent reported having an emotional, psychological, or mental health condition (e.g., anxiety, depression, bipolar disorder) that had been, or was expected to be, present for at least 6 months and which sometimes, often, or always limited their daily activities (Burczycka, 2018). Four percent of respondents in this study reported having a MH-RD (n = 774).4,5
Measurement
CM
CM was assessed using items derived from a modified version of the Childhood Experiences of Violence Questionnaire (cf. Walsh et al., 2008) and that have been used in other epidemiological surveys conducted by Statistics Canada (2013, 2014). Respondents were asked questions on the frequency with which CM occurred before age 15. Similar to other research (e.g., Afifi et al., 2014, 2016; Brownridge et al., 2017), in this study the childhood exposure to violence (EV) and physical child abuse (PCA) variables were coded dichotomously (yes/no) as follows: exposure to violence (EV) was determined by whether the respondent saw or heard any of their parents, step-parents, or guardians hit each other or another adult 3 or more times. Respondents were coded as having experienced PCA if: (a) an adult had slapped them on the face, head, or ears, or hit them with something hard to hurt them 3 or more times; (b) an adult pushed, grabbed, shoved, or threw something at them to hurt them 3 or more times; and/or (c) an adult kicked, bit, punched, burned, or physically attacked them in some way at least once. Child sexual abuse (CSA) was coded as having occurred if the respondent reported that an adult forced or attempted to force them into any unwanted sexual activity, by threatening them, holding them down, or hurting them in some way, and/or whether an adult touched them against their will in any sexual way.
Sociodemographic variables
Interviewers recorded respondents’ gender and, if necessary, asked them to self-report their gender as either male or female. Age in years was self-reported. Education was measured by asking respondents about the highest level of education that they had attained. Marital status was based on respondents’ self-report of whether they were living in a marital or common-law relationship at the time of the survey. The presence of children referred to whether one or more children aged 0 to 14 years were reported by respondents to be residing in the household.
Respondent’s substance abuse
Respondent’s heavy drinking was measured with items that asked about the frequency with which the respondent consumed five or more drinks on a single occasion in the month prior to the survey (1 or more times/never). Respondent’s drug use was based on items asking about the frequency with which the respondent used nonprescription drugs (marijuana, hashish, hash oil or other cannabis derivatives, magic mushrooms, cocaine, speed, methamphetamine, ecstasy, phencyclidine, mescaline, or heroin) in the month prior to the survey (1 or more times/never).
Perpetrator-related characteristics
Respondents reported on their partner’s characteristics, including the same item identified above regarding heavy drinking. Partner’s jealousy referred to the respondent’s partner being jealous and not wanting her or him to talk to other men/women. Monitoring the respondent was measured with an item that asked the respondent if their partner demanded to know who they were with and where they were at all times. Finally, the partner’s socially isolating behaviors were indicated by the respondent’s report of whether or not their partner attempted to limit their contact with family or friends.
Violence
Eleven behavioral items from a modified version of the Conflict Tactics Scales (CTSs; Straus, 1979) were used to measure violence (α = .779). The CTS has been demonstrated to be a valid and reliable measure of IPV (Archer, 1999; Straus et al., 1996). IPV was defined as acts of physical assault (having something thrown at you that could hurt; being pushed, grabbed, or shoved in a way that could hurt; being slapped; being hit with something that could hurt; being kicked, bit, or hit with a fist; being beaten; being choked; being threatened with or having a knife or gun used against the respondent), physical threat (being threatened to be hit with a fist or anything else that could hurt), and sexual assault (being forced into any sexual activity by being threatened, held down, or hurt in some way; being subjected to nonconsensual sexual activity by means of drugs, intoxication, manipulation, or nonphysical force) perpetrated by the respondent’s current marital/common-law partner within the 5 years preceding the interview. Hence, if respondents reported having experienced any of the aforementioned forms of violence within the 5 years preceding the interview by a current partner, they were coded as having experienced IPV. For the descriptive analyses, an additional IPV variable was derived from the aforementioned IPV variables to assess the prevalence of severe IPV (being hit; kicked, bit/hit with a fist; beaten; choked; threatened with a knife/gun; sexually assaulted).
Method of Analysis
To examine the prevalence of IPV and investigate independent variables by MH-RD status, we conducted descriptive analyses using cross-tabulations and unadjusted ORs. Logistic regression was used for the multivariable analyses because it is an appropriate technique for predicting a dichotomous dependent variable from a set of independent variables.6,7
Results
Descriptive Analyses
Prevalence of IPV by MH-RD
Among respondents with MH-RD, 6.8% reported having experienced IPV in the 5 years prior to the survey compared with 2.2% of those without MH-RD. That difference translated to those with MH-RD having an elevated odds of IPV that was more than 3 times that of their counterparts without MH-RD (OR = 3.33; p < .001). A similar pattern was evident when examining severe IPV, with those having MH-RD reporting 3.5 times the odds of severe IPV victimization relative to those without MH-RD (MH-RD = 4.3% vs. without MH-RD = 1.3%; OR = 3.49; p < .001).
Independent variables by MH-RD
Table 1 contains the distribution of independent variables for those with and without MH-RD. Results showed that respondents with MH-RD were more likely than those without MH-RD to report having experienced CM. Nearly 40% of respondents with MH-RD had experienced PCA compared with 17% of those without MH-RD (OR = 2.95; p < .001). The gap between the two groups was even wider with respect to CSA. Nearly one-quarter of respondents with MH-RD had experienced CSA compared with about 8% of those without MH-RD (OR = 3.50; p < .001). EV was the least common form of CM within each group. Nevertheless, respondents with MH-RD had 2.5 times the odds of reporting EV (OR = 2.50; p < .001).
Distribution of Independent Variables by MH-RD Status.
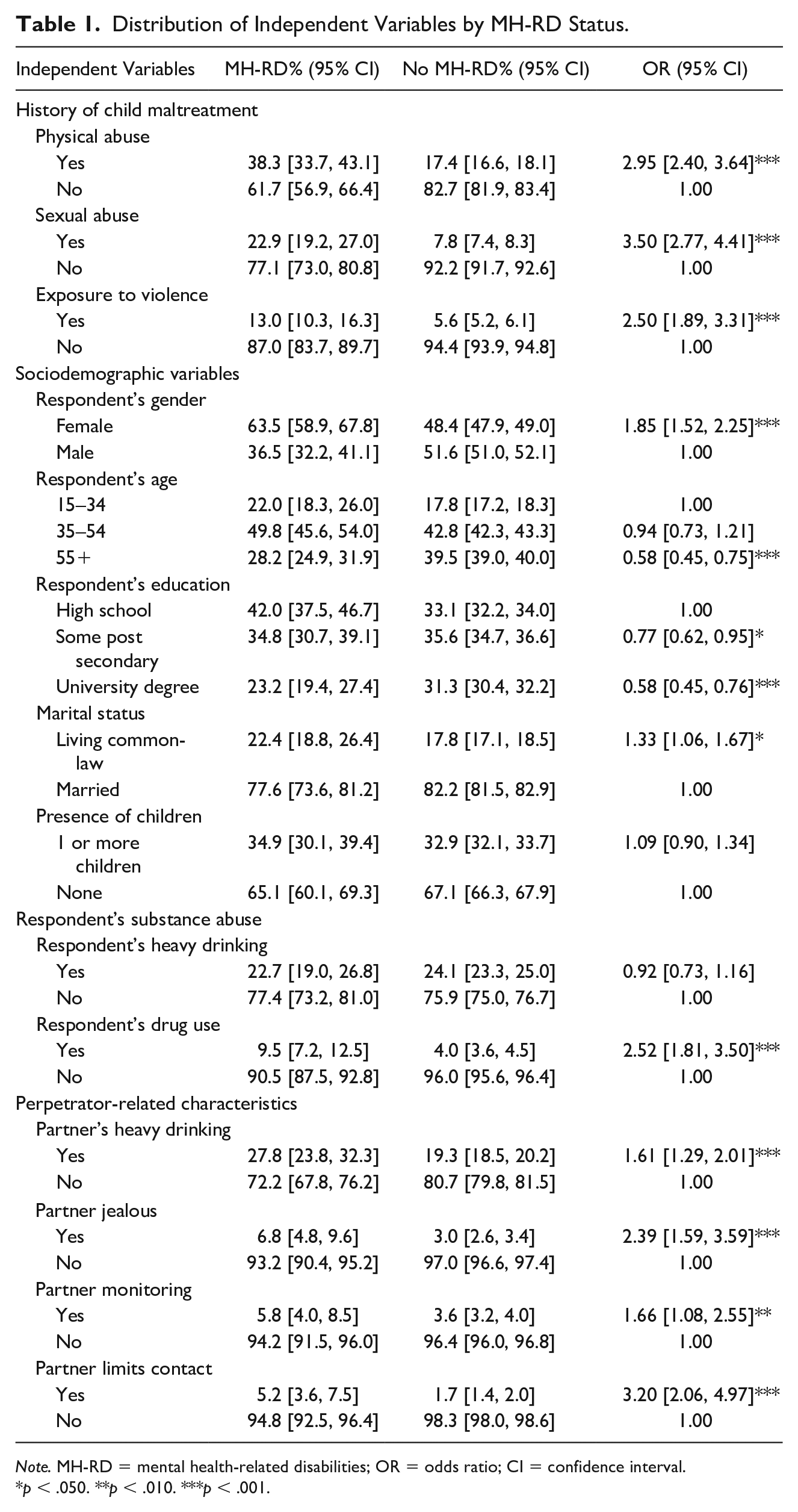
Note. MH-RD = mental health-related disabilities; OR = odds ratio; CI = confidence interval.
p < .050. **p < .010. ***p < .001.
In terms of sociodemographic variables, nearly two-thirds of respondents with MH-RD were female (63.5%; OR = 1.85; p < .001). 8 A significant difference was present in only one age category. Those having MH-RD were less likely to be aged 55 and older (OR = .58; p < .001). Respondents with MH-RD were less likely than those without MH-RD to have some postsecondary education (OR = .77; p < .05) or a university degree (OR = .58; p < .001). In terms of marital status, respondents with MH-RD were slightly more likely to be living in a common-law union (OR = 1.33; p < .05). No difference was found in the proportion of those with and without MH-RD that had children under age 15 living in their home.
With respect to respondents’ rates of heavy alcohol consumption, no difference was evident between the two groups. However, those with MH-RD had 2.5 times the odds of using nonprescription drugs in the month prior to the survey (OR = 2.52; 95% confidence interval (CI) = 1.81, 3.50; p < .001).
All of the perpetrator-related characteristics showed significant differences across the two groups. Compared with those without MH-RD, respondents with MH-RD had over one and a half times the odds of having a partner that abused alcohol in the month prior to the survey (OR = 1.61; 95% CI = 1.29, 2.01; p < .001) and who monitored their whereabouts at all times (OR = 1.66; 95% CI = 1.08, 2.55; p < .01), more than twice the odds of having a jealous partner (OR = 2.39; 95% CI = 1.59, 3.59; p < .001), and more than 3 times the odds of having a partner that limited their contact with family or friends (OR = 3.20; 95% CI = 2.06, 4.97; p < .001).
Multiple Logistic Regression Analyses
Separate logistic regressions for respondents with and without MH-RD
Results of the direct logistic regressions on IPV for respondents with and without MH-RD are presented in Table 2. Given the small subsample of respondents with MH-RD relative to those without MH-RD, most of the odds ratios for the MH-RD subsample were not statistically significant. However, a comparison of the odds ratios across the two groups using pseudo t-tests suggested that the effects of the independent variables tended to be similar for both groups. Controlling for all other variables in the model, child physical abuse (CPA) was associated with 8% and 53% (p < .05) increased odds of IPV victimization for those with and without MH-RD, respectively (pseudo t = −.72). Neither CSA nor EV was associated with IPV for either group.
Results of Direct Logistic Regressions on IPV for Persons With and Without MH-RD.
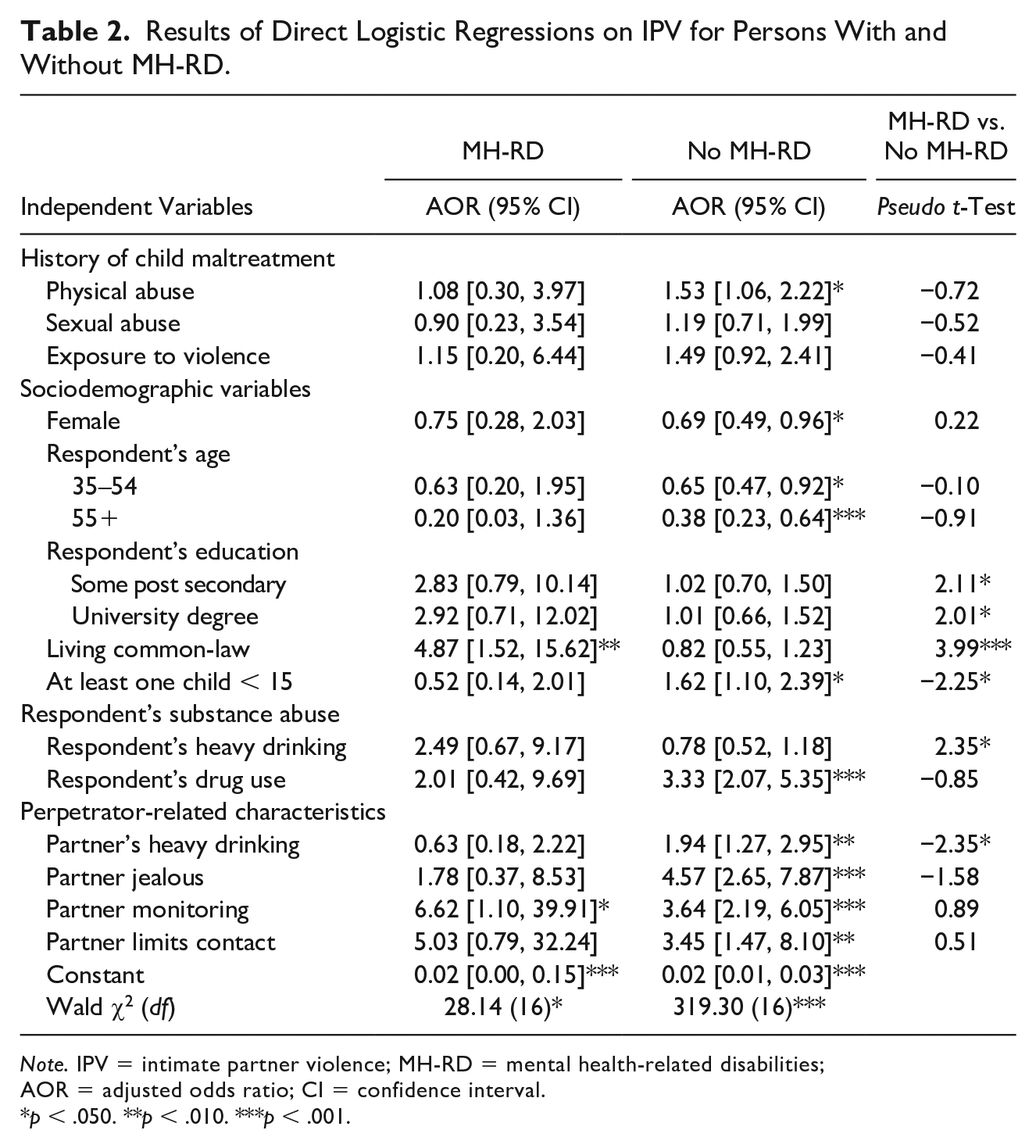
Note. IPV = intimate partner violence; MH-RD = mental health-related disabilities; AOR = adjusted odds ratio; CI = confidence interval.
p < .050. **p < .010. ***p < .001.
For both groups, females had lower odds of IPV victimization (MH-RD AOR = .75; without MH-RD AOR = .69, p < .05; pseudo t = 0.22). The odds of IPV victimization similarly declined with age for both groups, such that those under age 35 had the highest odds of IPV victimization. Although education did not affect the odds of IPV for respondents without MH-RD, the pseudo t-tests indicated that the odds ratios across the two groups were different. The magnitude of the odds ratios on the education variable for those with MH-RD suggested that IPV victimization may be associated with higher levels of education for this group (e.g., university degree MH-RD AOR = 2.92). Although nonsignificant for those without MH-RD, living in a common-law union was associated with nearly 5 times the odds of IPV for those with MH-RD (AOR = 4.87, p < .01; pseudo t = 3.99, p < .001). The presence of children in the home was not associated with the odds of IPV for respondents with MH-RD, but it was associated with 62% increased odds of IPV for those without MH-RD (AOR = 1.62, p < .05; pseudo t = −2.25, p <.05).
Respondent’s alcohol abuse was not associated with the odds of IPV for those without MH-RD, but it may be associated with increased odds of IPV for the respondents with MH-RD (AOR = 2.49; pseudo t = 2.35, p < .05). On the contrary, use of nonprescription drugs was associated with more than 3 times greater odds of IPV for those without MH-RD (AOR = 3.33, p < .001) and the pseudo t-test suggested that this variable was also associated with increased odds of IPV for those with MH-RD (AOR = 2.01; pseudo t = −.85).
Partner’s alcohol abuse was associated with increased odds of IPV for respondents without MH-RD (AOR = 1.94, p <.01), but not for those with MH-RD (AOR = .63; pseudo t = −2.35, p < .05). Having a jealous partner was associated with more than 4 times the odds of IPV victimization for those without MH-RD (AOR = 4.57, p < .001), and the pseudo t-test indicated that the odds for those with MH-RD were similar (AOR = 1.78; pseudo t = −1.58). Monitoring behaviors by partners was associated with increased odds of IPV for both groups (MH-RD AOR = 6.62, p < .05; without MH-RD AOR = 3.64, p < .001; pseudo t = 0.89). Finally, having a partner that limits the respondent’s contact with family and friends was associated with increased odds of IPV victimization for those without MH-RD (AOR = 3.45, p < .01), and the pseudo t-test suggested a similar effect for those with MH-RD (AOR = 5.03; pseudo t = .51).
Sequential logistic regressions
Results for the sequential logistic regressions are presented in Table 3. The first model showed that, without any controls, respondents with MH-RD had 233% greater odds of IPV victimization compared with those without MH-RD (p < .001). The second model controlled for a history of CM. With these controls, the elevated odds of IPV for respondents with MH-RD were 153% greater than their counterparts without MH-RD (p < .001). Controlling for sociodemographic variables in the third model left the relative odds of IPV on the disability variable unchanged (AOR = 3.34; p < .001). The fourth model, which controlled for the respondent’s substance abuse, resulted in an adjusted odds that was 191% greater for those with MH-RD (p < .001). With controls for perpetrator-related characteristics in Model 5, respondents with MH-RD disabilities had 139% elevated odds of IPV victimization (p < .001). Model 6 controlled for all of the variables in the study. Doing so reduced the elevated odds by 143% such that respondents with MH-RD had 90% greater odds of IPV compared with respondents without MH-RD (p <.05; pseudo t = 2.49, p < .05).
Results of Sequential Logistic Regressions on IPV for Persons with MH-RD Relative to Persons without MH-RD.
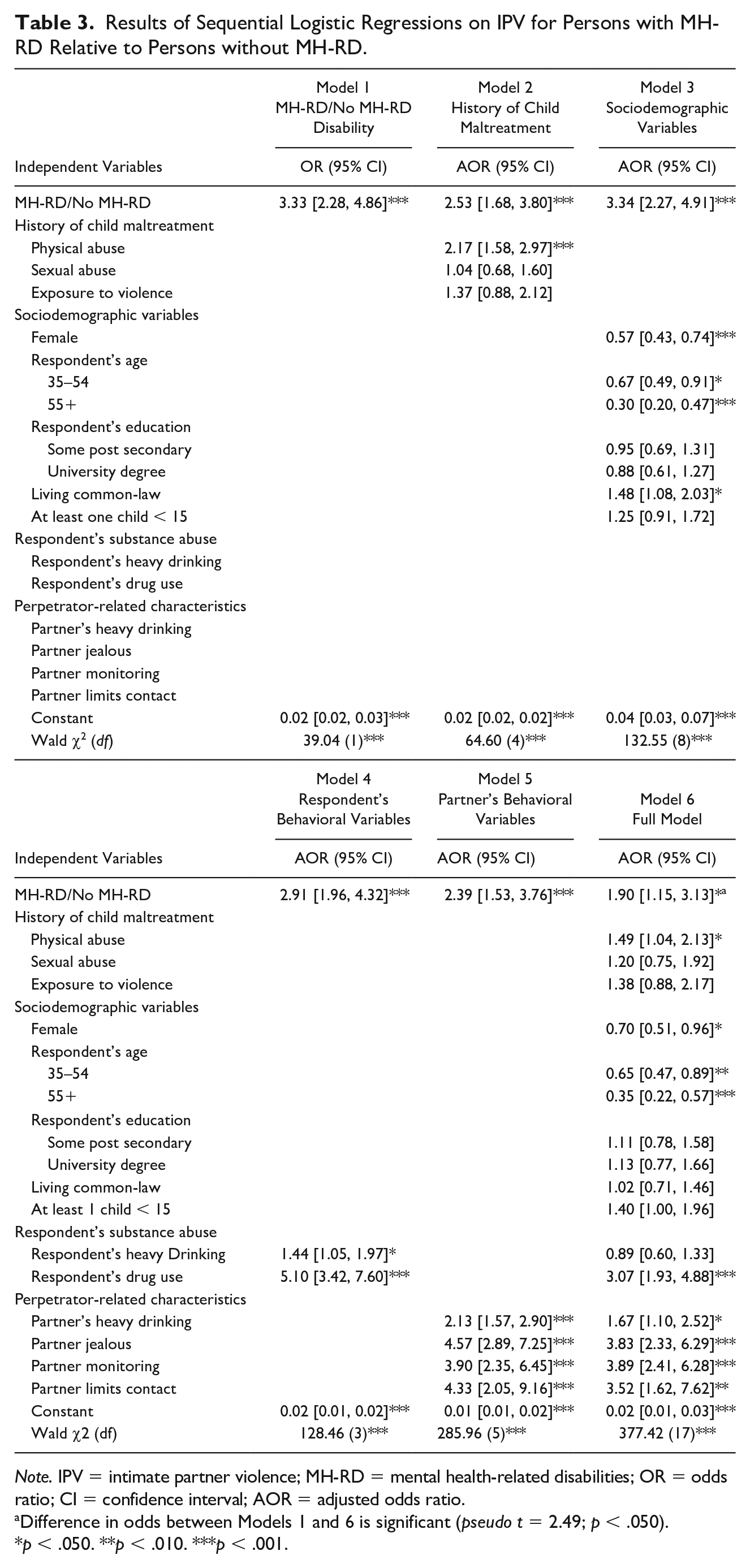
Note. IPV = intimate partner violence; MH-RD = mental health-related disabilities; OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio.
Difference in odds between Models 1 and 6 is significant (pseudo t = 2.49; p < .050).
p < .050. **p < .010. ***p < .001.
Discussion
Consistent with past research (Gearon & Bellack, 1999; Goodman et al., 2001; Khalifeh & Dean, 2010; Mikton et al., 2014), respondents with MH-RD reported experiencing IPV, both overall and severe, at a rate more than 3 times that of their counterparts without MH-RD. Clearly, Canadians with MH-RD are at elevated risk of IPV victimization. This study was one of only a few empirical investigations into risk factors for IPV victimization among persons with MH-RD, and it was the first to examine the extent to which risk factors accounted for their elevated odds of IPV. The sequential logistic regressions showed that no single grouping of variables from the ecological framework accounted for the elevated odds of IPV among respondents with MH-RD. Indeed, a significant reduction in this vulnerable population’s relative odds of IPV only occurred when simultaneously controlling for variables from all levels of the ecological framework. It follows that a consideration of Model 6 in the sequential logistic regressions in the context of findings from the descriptive and direct logistic regression analyses may provide some insights into the underlying dynamics contributing to this elevated risk.
Although respondents with MH-RD were more likely to report having experienced a history of all three forms of CM, the direct logistic regressions indicated that only CPA was associated with increased odds of IPV victimization. The descriptive analysis showed that respondents with MH-RD were about 3 times as likely as their counterparts without MH-RD to have experienced CPA. Controlling for all other variables in Model 6 of the sequential logistic regressions, CPA was associated with 49% increased odds of IPV victimization (p < .05). Thus, these analyses suggested that the greater risk of CPA among respondents with MH-RD contributed to their elevated odds of IPV victimization. These results were consistent with observations in the literature linking CM to the development of both MH-RD and increased risk of victimization in adulthood (Friedman & Loue, 2007). In their qualitative study, Schröttle and Glammeier (2013) noted how females with disabilities who were victims of IPV described their victimization “as a kind of continuation of experiences from childhood and adolescence” (p. 242). Their analysis of these women’s accounts indicated that the CM they experienced increased their vulnerability to dominance and violence from partners by negatively affecting these women’s ability to set boundaries, their self-esteem, and rendering them more emotionally needy. CM, and particularly CPA, would appear, then, to be an important consideration for understanding this group’s high risk for IPV.
This study is the first among those investigating risk factors for IPV against persons with MH-RD to include male victimization. Gender was a significant predictor of IPV in Model 6 of the sequential logistic regressions, with women having 30% lower odds of IPV victimization (p < .05). Although the descriptive analysis showed that women were about twice as likely to have MH-RD, the logistic regression indicated that, controlling for all other variables in the model, men in both groups tended to have higher odds of IPV victimization. The higher prevalence of MH-RD among females, and similar prevalence of IPV by gender among respondents with MH-RD (cf. endnote 8), means that in real numbers there will be more female than male victims of IPV with MH-RD in the population. However, these results demonstrate that males with MH-RD also represent a group that is particularly vulnerable to IPV victimization. Saxton et al. (2006) commented on the assumption that men with disabilities are less vulnerable due to their “maleness” and that this assumption denies changes in power dynamics created by disability. Consequently, these men “will continue to be left out of services and resources to challenge abuse, and the abuse will continue” (Saxton et al., 2006, p. 4). A full understanding of the elevated risk of IPV against persons with disabilities requires an examination of both female and male victims. Moreover, effective prevention and intervention necessitates a consideration of women and men with MH-RD who are affected by IPV.
Consistent with research on IPV in general (e.g., Capaldi et al., 2012), age was negatively related to IPV for both groups. Although age was a significant predictor of IPV in Model 6 of the sequential logistic regressions, respondents with MH-RD were roughly equally as likely as those without MH-RD to be in the highest risk age group (15–34), suggesting that differences in age distribution offered little explanation for the elevated odds of IPV for respondents with MH-RD.
Although there were some significant differences between the two groups in terms of education and marital status, Model 6 in the sequential logistic regressions showed that the remaining sociodemographic risk factors (education, marital status, and presence of children) were not significant. This suggested that these sociodemographic variables did not contribute to the reduction of the elevated odds of IPV identified in the Full Model. Indeed, the observation in Model 3 of the sequential logistic regressions, which showed that the elevated odds of IPV for respondents with MH-RD were unchanged with controls for sociodemographic variables, indicated that these variables made no contribution to the reduction observed in Model 6.
In terms of respondent’s substance abuse, drug use by the respondent was associated with 3 times the odds of IPV victimization in Model 6 of the sequential logistic regressions (p < .001). Although the direct logistic regressions suggested that this variable was a significant predictor for both groups, the descriptive analyses showed that respondents with MH-RD were 2.5 times as likely to use nonprescription drugs. Thus, it would appear a greater tendency toward drug use by respondents with MH-RD was an important risk factor contributing to their elevated odds of IPV. Li et al. (2000) also found a significant association between substance abuse and violence for people with disabilities. These researchers suggested that persons with disabilities may abuse substances as a mechanism for coping with their disability or, noting a greater tendency for persons with disabilities to accept social deviance and affiliate with drug using peers, to fit in with their peers.
All of the perpetrator-related characteristics were significant predictors in Model 6 of the sequential logistic regressions. With respect to partner’s alcohol abuse (Full Model AOR = 1.67, p <.05), the descriptive analysis showed that respondents with MH-RD were more likely to have partners that abused alcohol (OR = 1.61, p < .001). However, the direct logistic regressions indicated that, while this variable was a significant predictor of IPV for respondents without MH-RD, partner’s alcohol abuse did not predict IPV for respondents with MH-RD. Thus, it would appear that the observed difference in likelihood of having a partner that abuses alcohol did not contribute to the reduction in elevated odds of IPV observed in Model 6 of the sequential logistic regressions. The remaining perpetrator-related characteristics, involving jealous, monitoring, and socially isolating behaviors, were all strong predictors of IPV in Model 6 of the sequential logistic regressions, and the direct logistic regressions indicated that these variables were important predictors for both groups. The descriptive analysis showed that respondents with MH-RD were more than 1.5 to 3 times as likely to have partners that exhibited these behaviors. Moreover, controlling for these variables in Model 5 of the sequential logistic regressions resulted in the lowest adjusted odds ratio among the models encompassing individual groupings of risk factors (AOR = 2.39, p < 001). Thus, it would appear that the greater tendency of respondents with MH-RD to be partnered with individuals who were jealous, insisted on knowing their whereabouts at all times, and who limited their contact with family and friends contributed to observed reduction in their elevated odds of IPV victimization.
The importance of CM, respondent’s drug use, and the perpetrator’s jealous, monitoring, and socially isolating behaviors for understanding a significant proportion of the elevated odds of IPV for respondents with MH-RD suggests that complex dynamics undergird this phenomenon. Indeed, while these risk factors were able to significantly reduce the elevated odds of IPV for respondents with MH-RD, with controls for these variables in Model 6 of the sequential logistic regressions, respondents with MH-RD still had 90% greater odds of IPV victimization (p < .05). The remaining unexplained odds after full adjustment may be explained by unmeasured factors. CM may have a number of negative sequelae that contribute to the development of a MH-RD. As noted above, it has been suggested that various factors impacting persons with MH-RD may render them more accepting of deviance (Li et al., 2000), as well as vulnerable to domineering partners and possessing a sense that there is no alternative (Schröttle & Glammeier, 2013). Vulnerability to violence is also increased by interpersonal difficulties that are inherent to many mental illnesses (Hughes et al., 2012). Mental illness is associated not only with IPV victimization but also with IPV perpetration (Friedman & Loue, 2007). Unfortunately, it was not possible with the available data in this study to compare rates of perpetration and mutual violence across groups of respondents with and without MH-RD. Similarly, we were not able to study specific sequelae of CM, personality features of the respondents and their partners, as well as more detailed interpersonal and relationship risk factors.
Adding to the complexity of understanding this phenomenon is the issue of bidirectionality in the relationship between MH-RD and IPV. MH-RD can precede, and be a consequence of, IPV. Longitudinal studies have indicated that mental (and physical) health impairments predate IPV (Hahn et al., 2014; Howard et al., 2010; Machisa et al., 2017; Trevillion et al., 2012). Research suggests that disability in general is usually a precursor to IPV (e.g., Copel, 2006), though this may be less the case with respect to MH-RD given the well-established psychological effects of violent trauma. In this context, it is understandable why risk factors would not fully account for the elevated odds of IPV against respondents with MH-RD in a study that was not able to discern temporal ordering of MH-RD and IPV. Future research into understanding the elevated risk for IPV among this group should examine a subsample of respondents for whom their MH-RD preceded their experience with IPV.
Limitations
In addition to the aforementioned limitations regarding bidirectionality as well as the inability to examine perpetration and mutual IPV, there are other limitations of this study which must be borne in mind when extrapolating from the results. First, though the use of a nationally representative sample was a major strength in this study, given the tendency for research in this area to use nonrepresentative clinical samples (Mikton et al., 2014; Nathanson et al., 2012), there are a few considerations that affected the representativeness of the data: (a) individuals without landline or cellular telephones were excluded; (b) as a general population survey, the GSS excluded persons residing in institutions. Consequently, the results of this study are not representative of persons with MH-RD that are at a level of severity that can lead to institutionalization. It is, however, worth noting that having included institutionalized individuals in the GSS would not necessarily have resulted in a representative sample given challenges in obtaining accurate reporting from this population (Howard et al., 2010); (c) the survey was limited to respondents that could speak English or French. Thus, potential respondents that could not speak either of Canada’s official languages were excluded from the sample. However, this was unlikely to have impacted the results of the study given that, according to the 2011 Census, only 1.8% of Canadians speak neither English nor French (Statistics Canada, 2016b).
Second, the GSS possessed measurement limitations. Future research on the relationship between MH-RD and IPV should include more risk factors. For example, measures of neglect and childhood emotional maltreatment, which may be particularly salient with respect to MH-RD, were not assessed in the GSS. As well, the versions of the measures that were used in the GSS have not been validated. Although all of the measures possess face validity, and some measures are modified versions of measures that have been validated (e.g., the CTS), the psychometrics of the specific measures used in the GSS remain unknown. In addition, although this study does not intend to contribute to the literature on gender a/symmetry in IPV, and, in fact, shows that there are more female than male victims of IPV with MH-RD, it is noteworthy that comparisons of risk for IPV across genders using the CTS may be problematic due to limitations of the CTS that may create a false parity in prevalence across genders (cf., for example, Hamby, 2016).
Third, the survey was based on self-reports of victimization. This may lead to underreporting the true prevalence of violence both consciously (socially desirable responding) and unconsciously (recall bias; Chan, 2011; Gelles, 1990). Unfortunately, Statistics Canada did not include in their survey a measure of social desirability, which would have allowed an assessment of the extent to which this may have impacted admissions of IPV victimization. Nevertheless, the use of a 5-year time frame combined with the relative salience of IPV rendered recall bias unlikely to have contributed to underreporting IPV in this study. Finally, it was not possible with the data to group respondents into more specific MH-RD categories. It is reasonable to expect that relationship dynamics, including as they relate to IPV, will differ across disparate MH-RD categories.
Conclusion
More than 1-million Canadians, representing about 4% of the adult population, have a MH-RD (Burczycka, 2018) and these individuals are at elevated risk of IPV victimization. The dynamics that underlie this phenomenon appear to be complex. This study identified differences in risk factors for those with and without MH-RD and showed that these differences (experiences of maltreatment in childhood, victim’s substance abuse, as well as perpetrator’s jealous, monitoring, and socially isolating behaviors) accounted for a significant proportion of this elevated risk of IPV. Future research on the link between MH-RD and IPV is warranted to fully understand the specific mechanisms contributing to the high risk of IPV in this vulnerable population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.