
Abstract
Subthreshold psychotic experiences (PEs) are known to confer a risk for suicidality. Yet, despite evidence of a strong etiological trauma–psychosis pathway, the coalesced effect of such concurrences on suicide risk is largely discounted. Our aims were to examine the impact of different manifestations of life span trauma and PEs on the risk of suicidal thoughts and attempts, using an exploratory person-centered approach. Data from the Adult Psychiatric Morbidity Survey (N = 7,403) were analyzed. PEs were assessed using the Psychosis Screening Questionnaire (PSQ) alongside items probing childhood and adult trauma, in addition to 12-month suicide thoughts and attempt. A manual three-step latent class analysis elicited four distinct profiles, namely, a socially disconnected/high PE, a sexual victimization/moderate PE, a life span trauma/low PE, and a baseline class. The socially disconnected class, characterized by a moderate likelihood of social disconnection, a high probability of various PE endorsements, yet a low likelihood of other significant trauma, showed the greatest risk of 12-month suicide ideation (odds ratio [OR] = 13.0, 95% confidence interval [CI] = [8.539, 19.021) and attempt (OR = 24.2, 95% CI = [10.349, 56.860). Neither multiple nor recurrent traumatic experiences invariably result in the emergence of PEs. Instead, a sense of social disconnection may be either resultant of PEs or alone sufficient to cultivate such symptom presentations, even in the absence of prior traumas. Moreover, just as traumatic encounters increase the risk of suicidality, so too might seemingly more innocuous adversities, such as poor-quality social relationships, further elevate the risk, particularly when proximal and coupled with the simultaneity of PEs.
Introduction
Suicide is a leading cause of preventable death, accounting for more than 800,000 fatalities each year (World Health Organization, 2014). Early global estimates indicate the presence of a schizophrenia diagnosis in around 14% of suicide deaths (Bertolote et al., 2004), whereas the combined lifetime risk of death by suicide is estimated to be 6% among schizophrenic populations (Hor & Taylor, 2010; Nordentoft et al., 2013). Research also shows that approximately 30% to 40% of individuals with psychotic spectrum disorders have thoughts of ending their lives, 20% to 30% attempt to end their life, and a further 5% to 10% die by suicide (Fialko et al., 2006; Palmer et al., 2005; Radomsky et al., 1999). Moreover, a history of suicide attempt, which predates first episode psychosis, significantly increases the risk of future suicidality (Sanchez-Gistau et al., 2013). Incidentally, mortality rates are also likely to be underestimated due to the current inability to capture suicides that occur prior to initial contact with mental health services (Nordentoft et al., 2015). That being said, despite recent studies evidencing a downward trend in suicide-specific mortality among this population (Gatov et al., 2017; Laursen et al., 2019; Tanskanen et al., 2018), contemporary meta-analyses and reviews continue to illustrate a considerable and pervasive disproportion in the number of suicide-related deaths relative to the general population (Hjorthøj et al., 2017; Nordentoft et al., 2013; Piotrowski et al., 2017; Walker et al., 2015). By extension, in lieu of formal diagnosis, subthreshold psychotic experiences (PEs) have been consistently associated with an elevated risk of suicidal thoughts, behaviors, and even death by suicide across both cross-sectional and prospective studies (Yates et al., 2019).
Existing studies in the psychosis and suicide domain have focused predominately on the role of comorbid psychological conditions (e.g., anxiety or depressive disorders) in intensifying suicide risk (Björkenstam et al., 2014; Honings et al., 2016; Kelleher, Devlin, et al., 2014; Kelleher et al., 2012, 2013), particularly in relation to subthreshold psychotic symptoms that are believed to be transdiagnostic in nature (van Os & Reininghaus, 2016). Yet, PEs have been shown to be a robust predictor of the subsequent development of suicidal thoughts and behaviors in a series of longitudinal studies (Kelleher, Cederlöf, & Lichtenstein, 2014; Kelleher et al., 2013; Sullivan et al., 2015). Moreover, the risk of suicidal behavior has been found to increase in line with the number of psychotic symptoms endorsed (Dutta et al., 2010; Nishida et al., 2010; Saha et al., 2011), irrespective of accompanying mental disorders (Honings et al., 2016). Nonetheless, a limitation of this existing research surrounding PEs and suicide has been the failure to fully account for different combinations of putative factors (e.g., interpersonal trauma) that may interact with PEs to influence suicide outcomes.
Likewise, a growing number of prospective studies examining the role of social and environment factors within the developmental trajectory of psychosis have found that early childhood trauma is a common precursor to the onset of PEs (Croft et al., 2019; Varese et al., 2012). Research also suggests that traumatic experiences during childhood are often highly interrelated, rarely occurring in isolation (Finkelhor et al., 2007), and are frequently associated with revictimization and comorbid psychopathologies in adulthood (Burns et al., 2016). In addition, the relationship between trauma and psychosis symptomology has been shown to be mediated by various intervening environmental factors such as loneliness and perceived social disconnection (Boyda et al., 2014; Boyda & McFeeters, 2015). Indeed, literature shows that social disconnection and loneliness have an analogous risk for mortality as other well-established mortality factors (physical activity, obesity, substance abuse, responsible sexual behavior, mental health, environmental quality, immunization, and access to health care; Holt-Lunstad et al., 2010).
Furthermore, a recent meta-analysis found that loneliness was more strongly associated with PEs in nonclinical samples compared with clinical samples (Chau et al., 2019), indicating that irrespective of the methods of assessment, a sense of social disconnection is considered a significant aversive experience that is linked to a wide array of accompanying negative public health consequences (Cacioppo & Cacioppo, 2014; Hakulinen et al., 2018; Leigh-Hunt et al., 2017).
Yet, as with the aforementioned literature in psychosis and suicide literature, important co-occurring relationships are largely overlooked within studies examining the trauma–psychosis pathway. As a result, there is a disconnect between evidence of a (a) potential etiological pathway in psychosis–suicide studies and (b) psychopathological co-occurrences in trauma–psychosis studies. Given the abundance of research linking (a) trauma and psychosis and (b) psychosis and suicide, the next logical step is to implement statistical models that seek to adjoin these intersecting research areas.
Traditional variable-centered approaches are likely to lead to an underestimation of risk as they are limited in the ability to capture the influence of co-occurring relationships within groups (Darby, 2007). To depict the possible interrelatedness of such experiences, corresponding analytic procedures must be employed so that research can refine the heterogeneity between those who experience diverse variations of trauma and psychosis. Thus, Latent Class Analysis (LCA) is useful to identify inherent subgroups of individuals within a larger heterogeneous population based on shared endorsements. It addresses several of the methodological challenges that can arise in traditional subgroup analyses, including low statistical power, high Type I error, and limitations in examining higher order interactions. In this way, it is well suited to capture the multidimensional nature of trauma and its relationships with co-occurring factors (Logan et al., 2011).
With this in mind, we adopted an exploratory person-centered approach to investigate the interrelationships between a range of traumas and PEs on the risk of suicidal thoughts and attempt. The aim was to uncover distinct typologies reflecting varying degrees of childhood and/or adult trauma with or without PE and ascertain whether any of these had a discernibly greater risk of suicidal thoughts and attempts.
Method
Participants and Procedure
The Adult Psychiatric Morbidity Survey 2007 (APMS 2007) was carried out between October 2006 and December 2007 by the National Centre for Social Research (NatCen) in conjunction with the University of Leicester. The survey was commissioned by the NHS Information Centre for Health and Social Care and employed a multistage stratified probability sampling design. The survey consisted of a Phase 1 and a Phase 2 (clinical) interview. Individuals aged 16 years and older living in private households were identified for interview, using the small user postcode address file (PAF). In instances where there were more than one person aged 16 years or older, one adult was chosen randomly to ensure that all eligible members of any household had the same chance of being selected. From 13,171 eligible households, 7,403 individuals undertook Phase 1 interviews, which consisted of a series of demographic questions and the assessment of a range of common mental disorders, alcohol and drug use, and general health, using standardized instruments. Of this group, 849 respondents were found to be eligible for a Phase 2 clinical interview, based on disorder-specific probability calculations, of which 74% (N = 630) took part in the clinical interviews. To ensure that the results were representative of the population living in private households in England, the data were weighted to account for nonresponse, gender, age, and region.
Measures
The analytic model adjusted for a variety of sociodemographic and clinical correlates of suicidality and PEs.
Demographic factors
Demographic factors included respondent sex, age band, marital status, educational attainment (0 = no qualifications, 1 = any qualification) and ethnic origin (Caucasian, Black, South Asian, mixed, or other). A proxy measure of socioeconomic status (SES) was formed from responses to two items, specifically the receipt of job seekers allowance and/or housing benefit, with a positive endorsement of one or both items used to signify low SES.
Clinical variables included general practitioner (GP) contact relating to a mental, nervous, or emotional complaint within the past year (0 = no, 1 = yes), in addition to the presence or absence of a drug dependency within their lifetime (0 = no, 1 = yes).
Adverse childhood experiences
Items were extracted which were indicative of physical and sexual abuse, neglect, and household dysfunction in childhood.
Childhood physical abuse was assessed by the item, “Severely beaten by parent/step-parent/carer before the age of 16?” (0 = no, 1 = yes).
Experiences of childhood sexual abuse (0 = no, 1 = yes) were derived from responses to two items, specifically “touched in a sexual way without consent before the age of 16” and “sexual intercourse without consent before the age of 16,” with an endorsement of either item denoting a positive occurrence.
Verification of one or both of the following experiences, namely, “Spent any time in any kind of institution up to the age of 16” or “Ever taken into Local Authority Care as a child up to the age of 16” was used to constitute incidents of childhood neglect (0 = no, 1 = yes).
Exposure to household violence in childhood was captured by a positive response to the item, ever experienced “violence in the home?” (0 = no, 1 = yes) in conjunction with an endorsement of the “more than months and before 16” response option for the subsidiary item, “When violence in the home last occurred?”
A measure of parental separation in childhood was formed from a negative endorsement of the item, “Lived with both natural parents until the age of 16?” together with a positive endorsement of the “Parental separation or divorce” response option for the subsidiary question, “Reason you did not live continuously with both natural parents at home until the age of 16.”
Adverse adult experiences
Adult sexual abuse (0 = no, 1 = yes) was assessed from response to two items, specifically “touched in a sexual way without consent after the age of 16” and “sexual intercourse without consent after the age of 16,” with a confirmation of either item indicating the presence of adult sexual abuse experiences.
Intimate partner violence (IPV; 0 = no, 1 = yes) was measured through responses to 10 domestic violence items. Initially, the items were grouped into three categories, specifically exclusion (two items), threats of violence (three items), and physical assault (five items). Endorsement of a minimum of one item in each category was used to indicate a positive response to that category. Next, a binary measure of IPV experiences was computed whereby endorsement of all three categories of IPV was taken to indicate prior experiences of domestic abuse.
Social disconnectedness was generated from seven items taken from the social support section. Responses to each item ranged from 1 = not true to 3 = certainly true. Example items include “Family & friends make me feel loved” and “Family & friends would see that I am taken care of if I needed to be.” A composite total score was created and then dichotomized into a binary social disconnectedness variable (0 = no, 1 = yes), whereby the bottom 10% of scores were taken to indicate a positive endorsement of lower quality and availability of social support.
PEs
The PSQ (Bebbington & Nayani, 1995) was used to capture four types of PEs (0 = not endorsed, 1 = endorsed) in the year preceding the survey. The PSQ screens for the presence of mania, thought insertion, paranoia, strange experiences, and hallucinations through a core item and two supplementary items for each group of PEs. For the current study, items pertaining to mania were excluded. The core hallucination question, “Over the past year, have there been times when you heard or saw things that other people could not?” was utilized as this encompassed both auditory and visual experiences. For the remaining three groups of PEs, subsidiary items were analyzed as these have been found to more accurately reflect true PEs. The three core and selected subsidiary questions were as follows (analysis questions in italics):
Thought insertion: “Over the past year, have you ever felt that your thoughts were directly interfered with or controlled by some outside force or person? Did it come about in a way that many people would find hard to believe?”
Paranoia: “Over the past year, have there been times when you felt that people were against you? Have you felt that a group of people was plotting to cause you serious harm?”
Strange experiences: “Over the past year, have there been times when you felt that something strange was going on? Was it so strange that other people would find it very hard to believe?”
Suicidality
Suicidality was captured using items from the revised clinical interview schedule (CIS-R) covering recent thoughts of suicide “Have you seriously thought about suicide within the last year?” and suicide attempts in the past 12 months, for example, “Have you attempted suicide in the last year?” (0 = no, 1 = yes).
Analytic Plan
A manual three-step LCA (Asparouhov & Muthén, 2014) was conducted to identify homogeneous groupings of individuals who endorsed similar patterns of interpersonal trauma and PEs. The estimation procedure also examined each of the subgroups in relation to a range of predictors and distal outcomes. The manual three-step approach is advantageous over the more commonly used “Classify-analyze” approach as it takes account of classification uncertainty rate (Asparouhov & Muthén, 2014). In addition, the manual three-step approach does not derive classes from the “Most Likely Class Membership” variable, which is commonly used in post hoc multinomial logistic regressions. Recent research shows that this practice produces substantially biased parameter estimates and standard errors and therefore should be avoided (Heron et al., 2015; Lanza et al., 2013). A series of 2 to 6 class models were estimated and several fit indices were used to determine the optimal model fit. In addition to parsimony consideration, the Akaike information criterion (AIC; Akaike, 1987), the Bayesian information criterion (BIC; Schwarz, 1978), and the sample size–adjusted BIC (SSABIC; Sclove, 1987) were used to ascertain model fit. Better fitting models are indicated by lower values of the AIC, BIC, and the SSABIC. The Lo–Mendell–Rubin adjusted likelihood ratio test (LMR-LRT; Lo, 2001) was applied to compare models. When a nonsignificant value (p = >.05) is reached, this indicates that the model with one less class should be accepted. Predictors of class membership were assessed using the auxiliary command (R3STEP) and included a range of sociodemographic variables (Table 3). Categorical distal outcomes were assessed using the DCAT auxiliary command, which examines the relationship between the latent predictor (i.e., the classes) and the manifest outcomes, that is, suicide thoughts and attempts (Table 4; Asparouhov & Muthén, 2014; Lanza et al., 2013). All analyses were conducted using Mplus Version 8.3 (Muthén & Muthén, 2017), using sample weights and robust maximum likelihood (Yuan & Bentler, 2008).
Results
The sample was majority White British (85.3%) with a mean age of 46 years. Females were in the majority (51.4%). Almost 13% reported attending a family doctor (GP) for mental, nervous, or emotional problems in the past 12 months; 12% were dependent on a Government welfare program; 3.4% of the sample endorsed dependency on one or more forms of illegal drugs use; and 24% reported having attained a degree-level qualification. Table 1 shows all variables of interest.
Descriptive Statistics for All Variables of Interest.
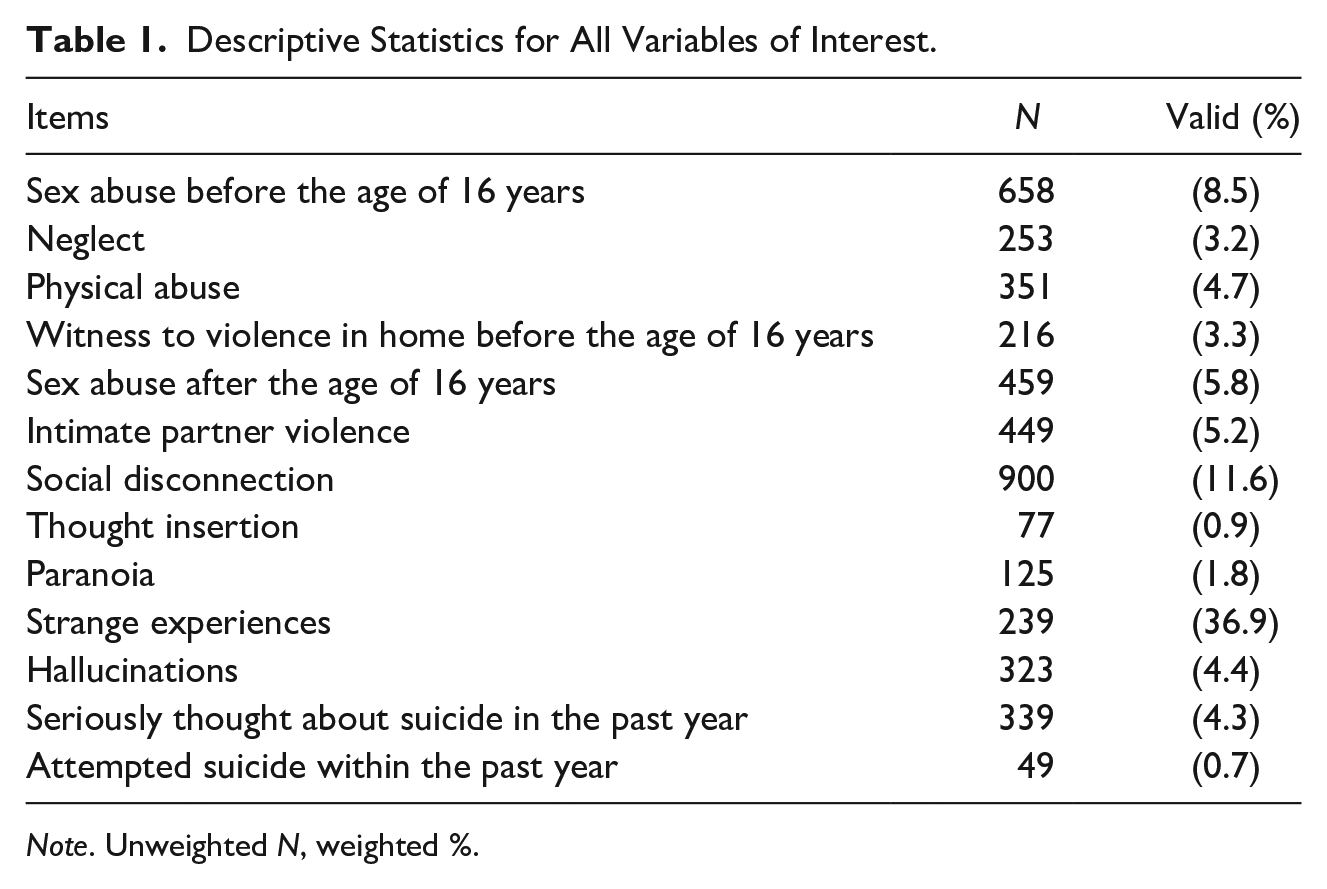
Note. Unweighted N, weighted %.
Table 2 shows the fit statistics for the LCA. Although the LMR-LRT was nonsignificant, the four-class solution was determined to be the optimal solution due to the lower BIC values in comparison with Class 3. Classes 5 and 6 were rejected due to higher BIC and nonsignificant LMR-LRT. Entropy for this model was 0.86. Within each class, the average probability of belonging to that class ranged from 0.70 to 0.95, indicating adequate classification accuracy (values of 1.00 indicate certainty with respect to classification).
Fit Indices for Latent Class Models 2 to 6.

Note. Most optimal model is shaded. AIC = Akaike information criterion; BIC = Bayesian information criterion; SSABIC = sample size–adjusted BIC; LMR-LRT = Lo–Mendell–Rubin adjusted Likelihood Ratio Test value and associated significance level.
p < .001, Weights applied.
The profile plot and endorsement probabilities for the four-class solution are shown in Figure 1. The y-axis refers to the probability of having endorsed yes to the category of events. Probabilities were classified as follows: low (<.20), moderate (0.21–0.50), and high (>0.51–1.0). Interpretation of the four-class solution was as follows: Class 1 (Socially disconnected—high PEs; n = 213, 2.9%) was the smallest class who endorsed low levels of life span trauma, but the moderate probability of social disconnection combined with the highest endorsement of PEs. Class 2 (Sexual victimization; n = 312, 4.2%) reflected individuals with a high probability of sexual abuse in both childhood and adulthood, coupled with the moderate endorsement of IPV experiences and low endorsement of PEs, with the exception of strange experiences. Class 3 (Life span adversity; n = 338, 4.6%) reflected individuals who endorsed the moderate to high levels of both childhood and adult adversity coupled with low levels of PEs. Class 4 (Baseline class; n = 6,538, 88.3%) reflected individuals with low probabilities of all life span adversity and moderate endorsement of strange experiences (PEs).
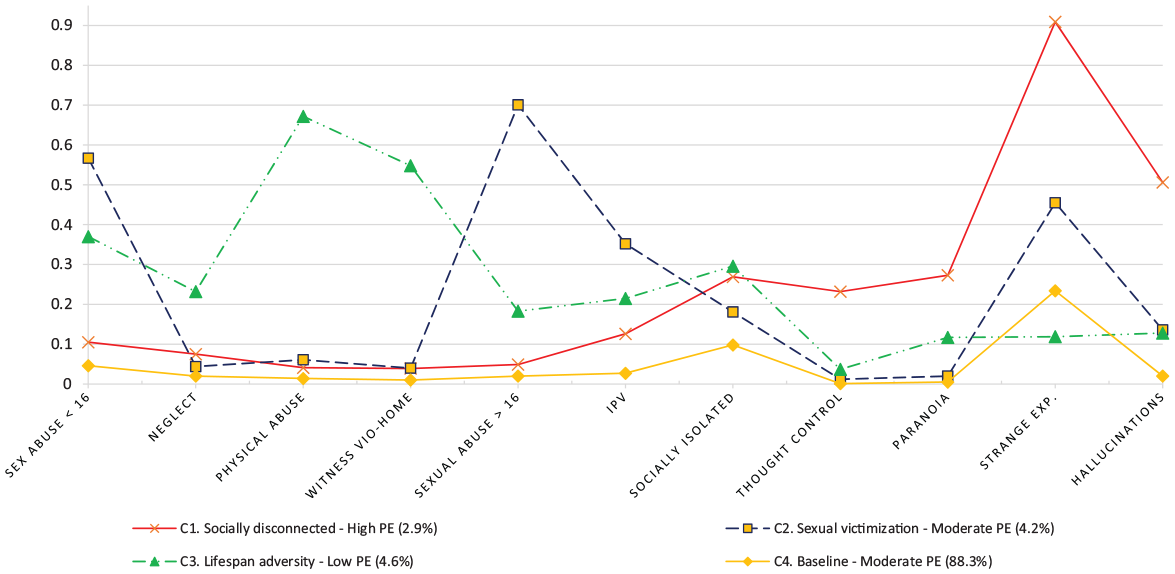
Profile plot of life span trauma and PEs.
The observed results of demographic predictors of class membership indicated that there was a positive and significant relationship between drug dependency (β = 1.12, p < .001), being separated (β = 0.87, p < .001), and the socially isolated class. However, a significant but negative relationship was observed between 12-month help-seeking and this class (β = − 0.67, p < .001). There was a significant but negative relationship observed between the 16 to 24 year band and the sexual victimization class (β = − 0.78, p < .05). However, a positive and significant relationship between being female (β = 1.51, p < .001), being drug dependent (β = 1.51, p < .001), no qualifications (β = − 0.75, p < .001), and being separated (β = 1.18, p < .001) was also observed with this class. Finally, the observed results showed significant but negative relationships in the 35 to 44, 45 to 54 year bands and the life span adversity class (β = −0.21, p < .01, β = − 0.23, p < .001), and drug dependency (β = 2.13, p < .001). There was also a significant but negative relationship with being widowed (β = − 0.85, p < .001) and the life span adversity class. Results are shown in Table 3.
Sociodemographic Predictors of Class Membership.
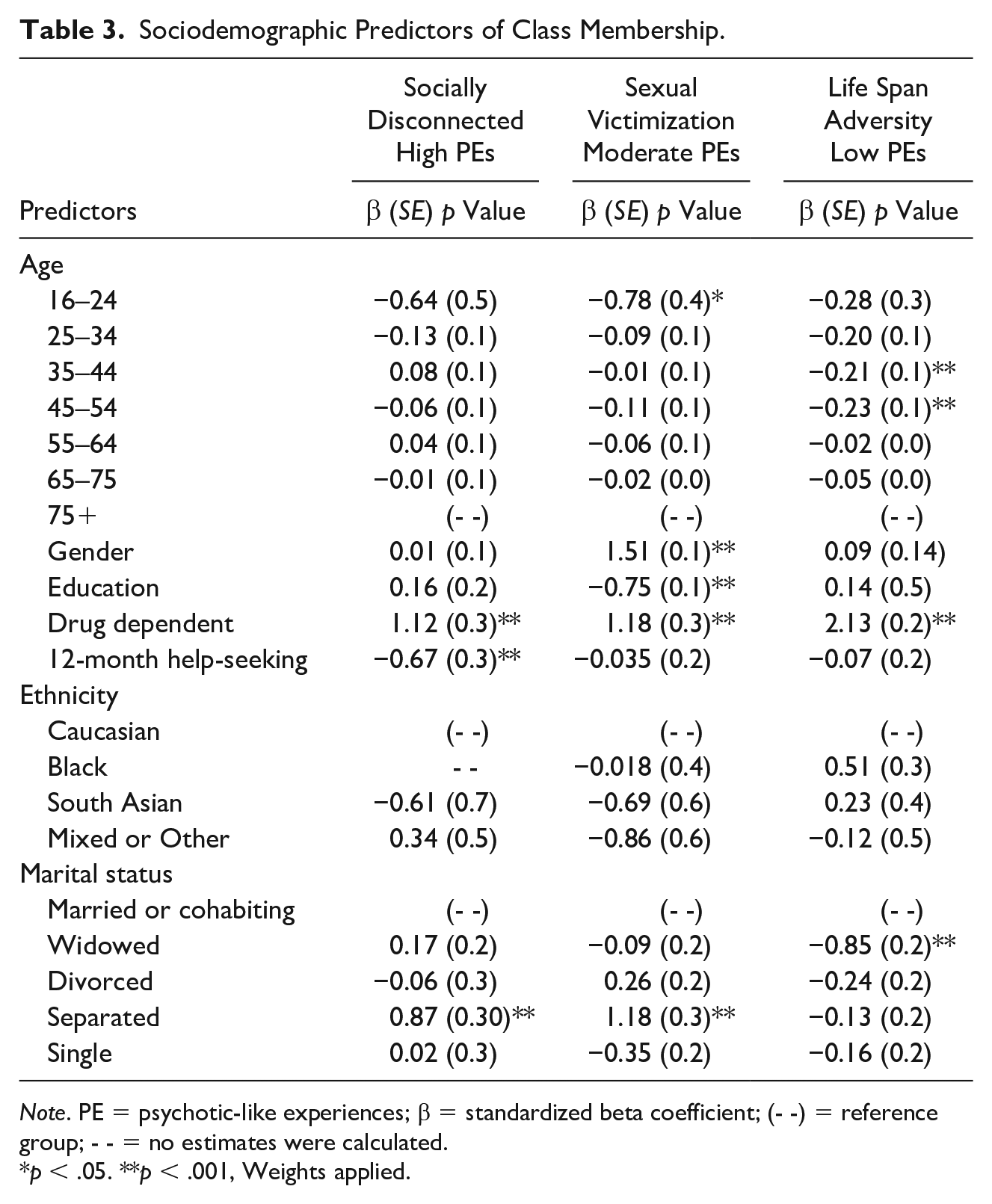
Note. PE = psychotic-like experiences; β = standardized beta coefficient; (- -) = reference group; - - = no estimates were calculated.
p < .05. **p < .001, Weights applied.
Results for each of the distal outcomes are reported in Table 4. The results showed a 13-fold (95% confidence interval [CI] = [8.539, 19.021]), sevenfold (95% CI = [4.730, 10.171]), and ninefold (95% CI = 6.436, 12.542]) increased odds of past 12-month suicidal ideation in the socially disconnected, sexual victimization, and life span adversity classes, respectively, in reference to the baseline class. A 24-fold (95% CI = [10.349, 56.860]), 15-fold (95% CI = [6.792, 33.319]) and tenfold (95% CI = [4.188, 24.011]) increased odds of past 12-month suicide attempt were reported for the socially disconnected, sexual victimization, and life span adversity classes in reference to the baseline.
Estimated Probabilities for Suicide Distal Outcomes Across the Four Classes.
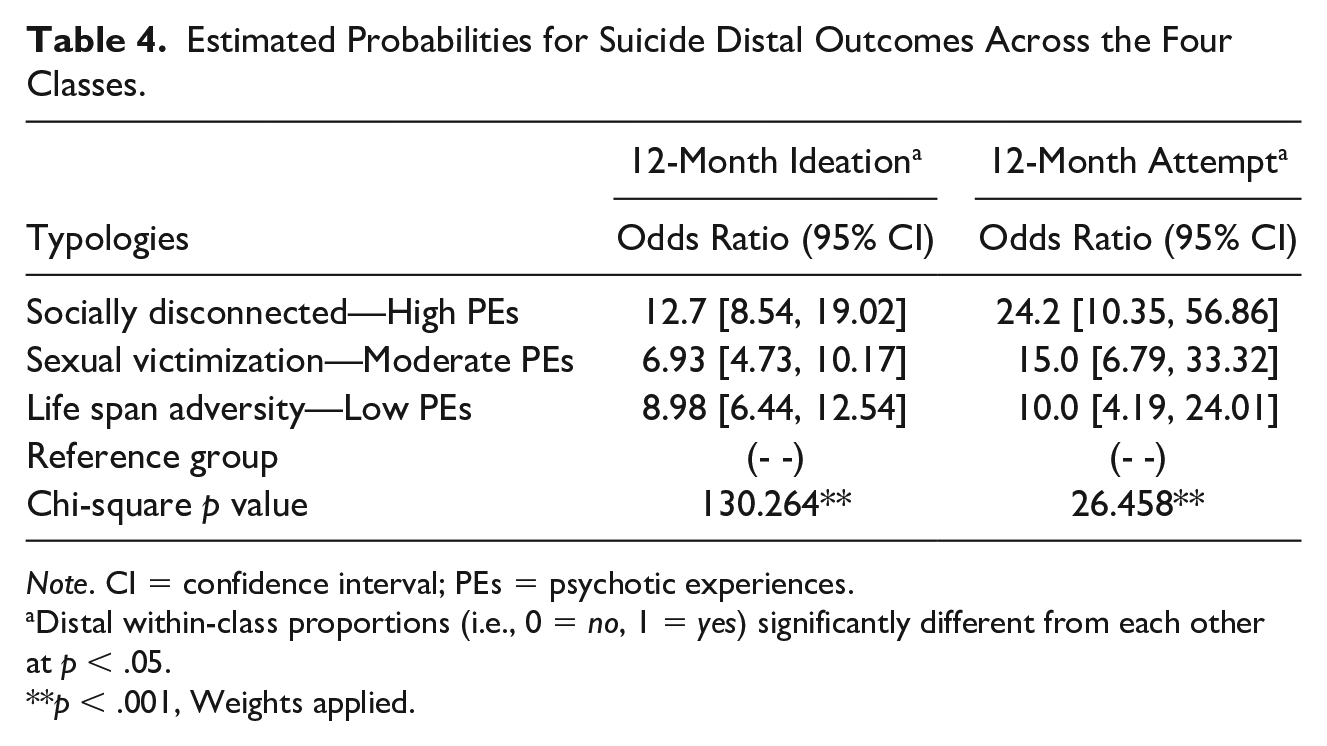
Note. CI = confidence interval; PEs = psychotic experiences.
Distal within-class proportions (i.e., 0 = no, 1 = yes) significantly different from each other at p < .05.
p < .001, Weights applied.
Discussion
The present study is the first, to our knowledge, to identify latent classes of interrelationships between life span traumas and PEs on the odds of suicidal ideation and attempts. The generated classes represent underlying subgroups of individuals in the sampled population.
As anticipated, a class emerged (Class 4 labeled the “baseline typology”), constituting the majority of participants (n = 6,538, 88.3%) and consisting of individuals endorsing low life span adversity and a moderate probability of a single PE, “Strange experiences” with a low probability of other PEs. In keeping with this, this class exhibited the lowest risk of all suicide outcomes.
The second-largest class (Class 3: Life span adversity—low PEs) represented 4.6% of the population and was characterized by moderate to high endorsement of most trauma indicators but particularly high probability of physical abuse. This class had a low endorsement of “thought control” and “paranoia” but higher endorsement of strange experiences and hallucinations compared with the baseline class. There were elevated odds of both 12-month suicidal ideation (OR = 9.0) and 12-month suicide attempt (OR = 10.0) in this group compared with baseline. Questionnaire self-reports of hallucinations have previously been shown to have the highest validity compared with clinical interview (vs. questionnaire items on paranoia and strange experiences; Kelleher et al., 2011). The increased probability of clinically relevant PEs and multiple adversities may partially explain the high odds of suicidal behavior among this class.
A further class emerged (Class 2: Sexual victimization—moderate PEs), representing 4.2% of the population and was characterized by individuals who experienced high levels of sexual abuse in both childhood and adulthood coupled with moderate levels of both IPV and PEs. This aligns with prior literature, which found that females with a history of childhood sexual assault are especially vulnerable to future revictimization (Barnes et al., 2009). This class also had increased odds of both 12-month suicidal ideation (OR = 7.0) and 12-month suicide attempt (OR = 15.0).
However, the LCA produced several unexpected outcomes. A socially disconnected and high PEs (Class 1) were generated, representing 2.9% of the population. This was characterized by low endorsement of all life span trauma, yet moderate probabilities of social disconnection, and exhibited the greatest probability of PE endorsement across all emergent classes. Research evidence suggests that there is a trauma–psychosis relationship; however, the disparity in the probability of endorsement of PEs between the life span adversity class versus sexual victimization versus socially disconnected class is difficult to discern. Nevertheless, whether causal or consequential, social disconnection and related appraisals of loneliness is a dominant feature among individuals with psychosis (Lim et al., 2018; Michalska da Rocha et al., 2018).
Finally, we anticipated that a high life span trauma–high PE class would emerge and confer the highest risk of suicidality over and above other typologies; however, this was not supported by the data as no such class materialized from the data. Although unexpected, these findings do serve to substantiate prior assertions that traumatic encounters do not inevitably manifest in the development of PEs and, conversely, that PEs can also emerge in the absence of prior traumas (Murphy et al., 2014).
Instead, a socially disconnected class and high PE class emerged, which was unexpected. Previous research has placed the greatest emphasis on physical and sexual abuse in determining poor psychological outcomes; however, our results suggest that social disconnection is at least as important a factor as this class showed a strong relationship with 12-month suicide thoughts (OR = 13.0) and 12-month attempts (OR = 24.2). The chronology of the encounters is likely to have contributed to these findings, whereby a history of multiple adverse experiences may create an enduring predisposition for suicidal thoughts and behaviors; however, it may be that such distal events (e.g., childhood trauma) may be less influential in determining current suicidality over more proximal factors such as lack of connectedness and poor mental health, which were captured in real time. In addition, the amplified ORs among the only high PE class align with recent research, showing that positive symptoms of psychosis were significant risk factors for suicidal thoughts and behaviors (Huang et al., 2018). Likewise, Kelleher et al. (2012) found that adolescents who reported psychotic symptoms had a nearly 20-fold increased odds of suicide plans and acts compared with adolescents with suicidal ideation who did not report psychotic symptoms. Indeed, DeVylder et al. (2015) also showed that the risk of concurrent suicidal ideation is increased fourfold among individuals with recent PEs, thus alluding to the frequent simultaneity of PEs and suicidal ideation.
The observed results may also tie in with research by van Os and Reininghaus (2016) who posited a synergistic pathway theory, whereby symptom manifestation may not vary independently but, instead, dynamically interact overtime to recruit more severe additional phenotype symptoms. As a result of increased network activity between psychotic phenomena and environmental stress, in this case, social disconnection, the risk of suicidality may become magnified through feelings of thwarted belongingness. Therefore, the socially disconnected and high PE class is conceivably the highest risk class for suicide, not least because of the presence of PE, but also because they are likely to have a greater propensity for thwarted belongingness (alienation, loneliness, and so on), which is central to contemporary theories of suicide (Joiner, 2007; Van Orden et al., 2008, 2010) and posited as one of the key motivators for suicide (O’Connor & Kirtley, 2018).
Limitations
The results should be interpreted in light of potential limitations. First, as all information was obtained via self-report, there is a possibility of reporting bias. For example, social desirability may have affected the reporting of psychotic symptoms (DeVylder & Hilimire, 2015; Read et al., 2004), suicidal thoughts and behavior (Jenkins et al., 2002), and traumatic experiences (Read et al., 2005). There is also some evidence that individuals may underreport their symptoms due to a misunderstanding of the questions posed or because of a tendency to normalize experience(s) (Wittchen, Knäuper, & Kessler, 1994; Wittchen, Zhao, et al., 1994). Second, the reliability and validity of self-reported trauma histories could not be established. However, several systematic reviews have concluded that adults recall childhood experiences with sufficient accuracy to provide useful information in retrospective studies (Brewin et al., 1993; Hardt & Rutter, 2004; Maughan & Rutter, 1997). Third, several of the measures were derived from either single survey items or a compilation of items that may call into question the reliability and validity of this method of operationalization. While this limitation must be acknowledged, this approach simply reflects the nature of epidemiological data and the efforts by the authors to best capture the observed constructs within the constraints of the available data. Future studies may seek to corroborate the current findings, utilizing more robust and objective assessment methods. Similarly, the suicidal thoughts and behavior items in the APMS were not based on a specific suicide risk assessment scale but were instead measured through a clinical diagnostic instrument (CIS-R). Relatedly, we lacked detailed information about suicidal thoughts and behavior, such as the number and timing of previous suicide attempts, as well as methods used, which would have enabled us to illuminate the association between the emergent latent classes and suicidal thoughts and behavior to a fuller extent. Fourth, some obtained estimates, especially those for a suicide attempt, had wide CIs due to the small number of endorsed cases; at the same time, lower CIs were well in excess of one. Finally, as with all cross-sectional research, the temporal association or causality cannot be established.
Implications
Psychosis significantly increases the risk of suicide ideation, attempt, or death (Huang et al., 2018) and, although evidence suggests that PEs are transitory for the majority of individuals, in a small but significant minority, such experiences can increase the likelihood of transition to a clinically relevant disorder (Reininghaus et al., 2016; van Os & Linscott, 2012; van Os & Reininghaus, 2016). Moreover, recent research suggests that individuals with PEs may be greater consumers of mental health services, including primary care, compared with those without (Bhavsar et al., 2018; DeVylder et al., 2014). Therefore, where individuals present with psychotic phenomena, be that in a primary or secondary health care settings, health professionals should be better trained to recognize the potential need for a more rigorous investigation, which not only includes a comprehensive assessment of (a) distal trauma, but also (b) social connectedness of the presenting client as both factors have been linked to suicidal thoughts and behaviors. For mental health professionals who are tasked with conducting such assessments, there should be clear practice guidelines in place to help guide the process, particularly in light of sustained barriers to abuse enquiries (Hepworth & McGowan, 2013; Read et al., 2007; Sampson & Read, 2017; Young et al., 2001).
Moreover, despite significant progress in mental health provision (Jenkins, 1992) and improvements in recognition and detection of mental health conditions within primary care settings (Pfaff et al., 2001; Taliaferro et al., 2013), there is an ongoing need for training among GPs in relation to issues such as suicide, depression, and abuse (Bajaj et al., 2008; Graham et al., 2011; Leavey et al., 2017; Zuckerbrot & Jensen, 2006).
Conclusion
Our findings tentatively suggest that whereas adverse life events increase the risk of 12-month suicide thoughts and behaviors, further elevated risk of suicide enactment may, in fact, be contingent on more proximal problems such as poor-quality social relationships and current psychological well-being. Indeed, feelings of loneliness can arise from social disconnection and are thought to play a maintenance and/or a causal role in the development of PEs (van der Werf et al., 2010). Conceivably, if PEs worsen, the ability to avail of support, maintain, or create social connections could become strained, thereby antagonizing further psychopathology and perpetuating a pernicious cycle of exclusion, psychopathology, and increased risk of suicide thoughts and behaviors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.