
Abstract
There is limited evidence on the prevalence and determinants of violence against pregnant women in India. Previous studies were entirely restricted to the violence against women in the reproductive age group. There is lack of evidence about the factors affecting violence against women during pregnancy. Understanding such factors, women’s perception regarding violence during pregnancy and their justification of such violence could manifest an important aspect of violence. Women living in slum communities particularly are victims of violence. In this context, this study intended to examine women’s perception, prevalence of, and factors affecting the violence against women during pregnancy in the slum communities of Pune. A community-based cross-sectional study of 1-year duration was undertaken in urban slums of Pune city, Maharashtra, India. The study participants were women who have delivered 2 years preceding the survey. Using simple random sampling, 500 women were selected from 10 purposively selected slums. House-to-house visits were made and face-to-face interviews conducted using a pretested structured questionnaire. Univariate, bivariate, and logistic regression analyses were applied. The study results show that 15.3% of women have experienced violence during their recent pregnancy. Furthermore, 9.2% of women experienced physical violence, 1.8% sexual violence, and 11.2% psychological violence. Education level of women, husband’s education and alcohol consumption, history of violence in the family, and provision of spurious justification for violence have emerged as some of the leading factors associated with the violence inflicted during pregnancy. Effective interventions at both community and health care settings are needed urgently to reduce the violence inflicted during pregnancy.
Introduction
The United Nations’ Sustainable Developmental Goals (SDGs) was formulated during 2015. SDG5, namely, the “gender goal,” exclusively deals with achieving gender equality and empowering women and girls. It is targeted to eliminate all forms of violence against women and girls (VAWG) including trafficking and sexual and other forms of exploitation. VAWG is a major public health issue and societal concern (Krug et al., 2002; Oram et al., 2017). Women worldwide may face violence in almost all countries and all cultures (García-Moreno et al., 2015). The phrase “violence against women” encompasses many forms of violence, including violence by an intimate partner (intimate partner violence [IPV]) and rape/sexual assault and other forms of sexual violence perpetrated by someone other than a partner (non-partner sexual violence). The Centers for Disease Control and Prevention defines “intimate partner violence” as a serious, preventable public health problem that affects millions of people around the world. The term “intimate partner violence” stands for physical violence, sexual violence, stalking, and psychological aggression (including coercive acts) by a current or former intimate partner (World Health Organization [WHO]).
WHO’s (2013) report “Global and Regional Estimates of Violence against Women” concluded that 30% of women worldwide have experienced physical and/or sexual violence by partners. According to this report, the worst affected region is Southeast Asia, with a prevalence rate of 37.7%. Substantial past literature has shown that higher prevalence rates of violence against women are observed in India (Kalokhe et al., 2017, 2018). Recently, violence inflicted during pregnancy and its health consequences on mother and baby have gained attention. Researchers around the world have been working on this with evidence provided regarding violence during pregnancy. In India, the recent National Family Health Survey–four (NFHS-4) reported 3.3% of women ever experienced violence during pregnancy.
A large number of studies documented the higher prevalence of IPV among the slum residents in India. A study by Silverman et al. (2016) conducted in Mumbai slums found that one in every three women (34.0%) and 48.5% reported gender-based household maltreatment by husbands and in-laws during the prepregnancy period. The study conducted in Kolkata slums found that more than half of the surveyed women had experienced the violence. A study conducted in Pune slums during 2008 found that about 60% women have ever experienced wife beating (Ruikar & Pratinidhi, 2008). Das et al. (2013) held that 35% of the women reported that violence is justifiable if a woman disrespected her in-laws or argued with her husband, failed to provide good food, housework and child care, or went out without permission. A recent study by Kalokhe et al. (2018) conducted in Pune found that the experience of domestic violence was associated with less educational attainment by the participant’s spouse, less satisfaction of the spouse’s family with the maanpaan (wedding-related gifts provided by the bride’s family) that they received at the time of marriage.
People living in slums are deprived of adequate living space, involved mostly in informal work in the unorganized sector, and suffer from poverty, alcoholism, and lack of education. These adverse socioeconomic conditions create low self-esteem and insecurity among men, which find expression in aberrant behaviors, and violence is used as a compensatory behavior (Pandey et al., 2009). Slum 1 communities in India are a result of massive migration from rural to urban areas. This leads to increased number of slum settlements in the urban areas without increase in basic facilities and housing. The cultural difference in the slum settlements creates acutely tense situations, leading further to violence. The basic quality of life among the slum communities has been reported to be essentially poor by many studies.
Substantial studies undertaken in slum communities of India examined the prevalence, risk factors, and consequences of violence against women (Begum et al., 2015; Rocca et al., 2008; Sinha et al., 2012). However, only handful of studies focused on violence during pregnancy in slums in India.
Review of Literature
Women Perception and Justification of Violence Against Women
Women’s own perception and attitude toward violence against women affects the extent of violence against women. Their justification and acceptance of violence also affect women in many ways. The available evidence shows women who have justified violence under certain conditions were more likely to experience further violence than those who do not justify (Donta et al., 2016; Jejeebhoy, 1998; Krause et al., 2017; Rani & Bonu, 2009; Waltermaurer, 2012). The patriarchal societies reinforced by strict gender norms and values that put women in a subordinate position to men have higher odds of violence against women. Patriarchal societies where a defined gender role attitude prevails to put women under pressure to accept the violence under different circumstances leads to more violence against women. Hence, women’s tolerance of violence in absence of proper help seeking became justification of violence. However, previous research found that increased education level of women decreased the justification of violence (Dalal et al., 2012; Rani & Bonu, 2009).
Recent studies have argued that women empowerment, particularly economic empowerment, can be considered as a protective factor for violence against women in South Asian countries and especially in India (Dalal, 2011; Donta et al., 2016; Krishnan et al., 2012). Furthermore, women with greater social and economic autonomy are able to seek health care when faced with violence (Rowan et al., 2018). However, women’s working status alone cannot protect them from being victims of violence (Krishnan et al., 2010). Many other factors, individually or in combination, were found to be protective for women encountering violence.
Risk Factors of Violence During Pregnancy
IPV during pregnancy has recently received global attention. Prevalence of IPV against pregnant women differs across populations globally with rates reported to range from 0.9% to 30% (Gazmararian et al., 1996; Taillieu & Brownridge, 2010). The said prevalence range from 2% to 20% in India (Das et al., 2013; Khosla et al., 2005; Raj et al., 2011). Risk of domestic violence was twice for women who justified wife beating than women who did not justify wife beating (Begum et al., 2015). Recent literature shows that the risk of IPV increased due to the low level of female education, lower socioeconomic situation, and harrowing poverty (Raj et al., 2018). Studies have also demonstrated a higher prevalence of violence among women belonging to the Scheduled Caste (an oppressed caste in the Indian caste system where Scheduled Castes (SCs) and Scheduled Tribes (STs) were considered to be lower caste), thereby stressing the role of caste in the oppression and violence experienced by women (International Institute for Population Sciences & ICF, 2016; Mahapatro et al., 2012).
Numerous studies reported that having an alcoholic partner increases the likelihood of violence against women in general and during pregnancy in particular (Varma et al., 2007; Wagman et al., 2018). Men who believe in the traditional gender role attitudes are more likely to perpetuate the violence than men who believes in the gender egalitarian approach (Pulerwitz & Barker, 2008). Several interventions targeted at men to educate and engage them to reduce IPV perpetuated by them have yielded positive outcomes around the world (Miller et al., 2012; Pulerwitz et al., 2015; Verma et al., 2006). The risk factors of violence against women during pregnancy vary from socio-demographics to behavioral factors. However, research exploring such factors were scanty in India. The risk factors of such violence vary from community, culture, tradition, and caste to religion. Some factors were observed to be common across the all communities in India.
Consequences of Violence During Pregnancy
Available studies clearly showed the significant association of IPV against pregnant women and negative maternal and child health outcomes such as miscarriages, premature labor, low birth-weight babies, and postpartum depression (Ludermir et al., 2010; Mahapatro et al., 2011; Muthal-Rathore et al., 2002; Sarkar, 2013; Silverman et al., 2016). Violence during pregnancy has also been linked to reduced and early cessation breastfeeding (Shroff et al., 2011; Miller-Graff, et al., 2018), higher prevalence of antenatal and postpartum depression (Halim et al., 2018; Nayak et al., 2010), less utilization of maternal health services (Singh et al., 2018), higher use of tobacco and smoking (Ackerson et al., 2007), higher chances of suicide (Devries et al., 2011), burns, and injuries (Spiwak et al., 2015), and increased fear of childbirth (Hossieni et al., 2017). The study by Das et al. (2013) shows that women who experienced IPV were more likely to report pregnancy-related illness and longer hospitalization.
Studies across the globe reported that physical violence against pregnant women may lead to rupture of membranes and placental abruption (Audi et al., 2012; Shah & Shah, 2010). Women who face partner violence may be less likely to adopt contraception and more likely to experience a subsequent unwanted pregnancy (Begum et al., 2010; Stephenson et al., 2008). Study by Tavoli et al. (2016) reported that domestic violence against women during pregnancy had significant adverse association with their quality of life. A recent study conducted in Bangladesh found that women who face violence during pregnancy were less likely to prepare for childbirth (Pun et al., 2018). These negative health consequences of violence during pregnancy necessitate the formulation of effective strategies to reduce the burden of violence against pregnant women.
Method
Study Design and Setting
This study is a community-based cross-sectional study conducted during January 2018 to February 2019. This study was conducted in the slum communities of Pune city, Maharashtra, which is one of the largest metropolitan cities in India. Pune is the second largest urban agglomerate in the state of Maharashtra, following Mumbai, and is the seventh-most populous city in the country. Pune Metropolitan Region consists of Pune city and suburbs of Pimpri-Chinchwad. The Pune Municipal Corporation (PMC), well known as Pune Mahanagar Palika, is the civic body that governs Pune. PMC has a total of 154 administrative wards. The administrative wards are divided for the decentralized planning and program functioning in the city.
Ethical Consent
Savitribai Phule Pune University granted the institutional ethical review permission. The study objective was explained to the respondents before starting the interview. Written consent was obtained before the survey. Respondents were assured that they could leave the survey anytime without giving any explanation.
Sampling
The study conducted among the slum communities in Pune city which has around 22% of its population living in slums (Census 2011, 2011). Slum communities are situated in all the corners of the city. Pune city divided into 154 administrative wards, for this study 10 wards was purposively selected. The estimated sample for this study was 550. We have decided to cover 550 respondents from 10 slums considering 60 respondents per slum. Randomly selected one slum from one administrative ward to have representation of the city. With 10% refusal, we have completed 500 interviews across all the selected 10 slums. The door-to-door survey helped to identify the potential respondent’s availability and willingness to participate in the study.
Selection of Respondents
Two trained female investigators conducted house-to-house survey to find the potential respondents in selected slum settlements. The criteria to be included in the study were (a) women had given birth in the last 2 years, (b) they did not have any major illness, and (c) those who completed 18 years.
Data Collection
House-to-house visits were made and women were interviewed face to face using a pretested semi-structured questionnaire. Study followed WHO’s (2001) ethical and safety recommendations. Participants were told that the study was related to maternal and child health, and women who had given birth in the last 2 years approached. Before interview, participants were informed of the nature and potential sensitivity of the violence-related questions. Eligible women who agreed to participate in the study were asked to give written consent to participate in the study. The trained female investigators conducted the interviews. Female investigators were undergone extensive training on how to conduct interviews on sensitive issues such as violence. They were also equipped with skills to handle any emotional issues aroused during interview. The interviews were conducted in the respondent’s house or near an Anganwadi center (government approved center for providing supplementary food to children and lactating women), where respondents had opportunity to share their experiences without fear. The interviews were conducted if the privacy during interview was assured. The interviews were conducted in Marathi or Hindi language based on respondent’s choice. Interviews were lasted for around 30- to 60-min duration. Information on socio-demographics and maternal history was collected. Furthermore, information on the experiences of violence, justification provided for violence, and history of violence was also collected. The study participants were not paid any honorarium for participation in study.
Measurement of Violence
Violence was measured using a modified version of WHO’s (2005) multicountry study of violence against women instrument. This instrument contains 13 items on physical, sexual, and psychological violence which a woman might have experienced with her current partner and has been validated in Indian studies (Vachher & Sharma, 2010). Physical violence was measured through five items (viz., pushed/scrambled, slapped/thrown something to harm, kicked/pulled/beaten, shoved/burned, and harmed using knife or gun. Psychological violence was measured through four items (viz., insulted/treated you the way which agonized, humiliated you before someone, scared you, and threatened to harm you or anything that is important to you). Sexual violence was measured through three items (viz., have had sex without your consent/forceful sex, had to have sex with your husband because you scared of him, and made to do something indecent).
Binary variables were created to estimate the prevalence of physical, psychological, and sexual violence during pregnancy. Furthermore, to estimate the prevalence of physical violence in pregnancy, a woman’s responses across the corresponding six items were summed. A woman received a 0 if she had not experienced any physical violence during pregnancy and a 1 if she had experienced one or more acts of physical violence during pregnancy. Psychological violence and sexual violence were estimated in the same fashion using the relevant violence items from the instrument. Binary variables were also created to estimate the proportion of women who had experienced any form of violence. To assure internal consistence and reliability of outcomes measures, we used the Cronbach’s alphas for physical, sexual, and psychological IPV scales used in this study. The alpha scores for physical violence 0.781, psychological violence 0.828, and for sexual violence 0.708.
Independent Variables
Age (less than 24, 25–30, and above 30), education (illiterate, primary, secondary, and higher secondary and high), occupation (working, not working), religion (Hindu, Muslim, and others), caste (Scheduled Caste, Scheduled Tribes, and Other Backward Classes [OBCs]), 2 type of family (joint family, nuclear family), number of children (one or more than one), husband’s age (less than 24, 25–30, and above 30) and husband’s education (illiterate, primary, secondary and higher and above), women justifying violence (yes = 1 or no = 0), husband’s alcohol consumption (yes = 1 or no = 0), and previous experience of violence (yes = 1 or no = 0).
Dependent Variables
Any violence (physical, sexual, and psychological) experienced by women during pregnancy (yes = 1, no = 0).
Statistical Analysis
Data were cleaned and entered into the SPSS version 21 for the analysis. Descriptive analysis and binary logistic regression were applied to find the association of predictors of violence during pregnancy. These results are expressed as odds ratio (OR) and 95% confidence interval (CI).
Results
Sample Characteristics
Table 1 presents the socio-demographic characteristics of the sample (500). A total of 46.6% respondents are less than 24 years of age, and 44.4% respondents are in between 25 and 30 years of age. The mean of the ages of the sample is 25.17 ± 4.10 and the median age is 25. A total of 5.8% of respondents were illiterate, 3.4% had primary education and majority of respondents (85%) had secondary or higher education, 84.6% of women were not working. About 67.6% of the respondents lived in nuclear family while the rest 32.4% lived in joint families. As far as religion is concerned, the Hindu women were 74.8%. In terms of caste, 35.6% were SCs, 8% STs, 18.4% OBCs, and 38% other castes. Around 41% women had one child, and 44% had two children.
Socio-Demographic Characteristics of Study Respondents.

Perception on Justification of Violence Against Women During Pregnancy
Table 2 summarizes the responses to the question, “Do you think that wife beating is common in pregnancy?” In response, 68% of respondents said yes, violence in any form could be possible during pregnancy. When asked about the reasons for violence in particular, 63.6% of respondents said that negligence toward home could be a reason, 60.2% agreed upon negligence to child/children, 59.4% agreed about inappropriate cooking, 58.8% about not respecting in-laws, 50% about going out without permission. Also, 57.8% respondents agreed on not obeying in-laws and 50.4% for denying sex as possible reasons.
Perceived Opinion on Causes of Wife Beating During Pregnancy.
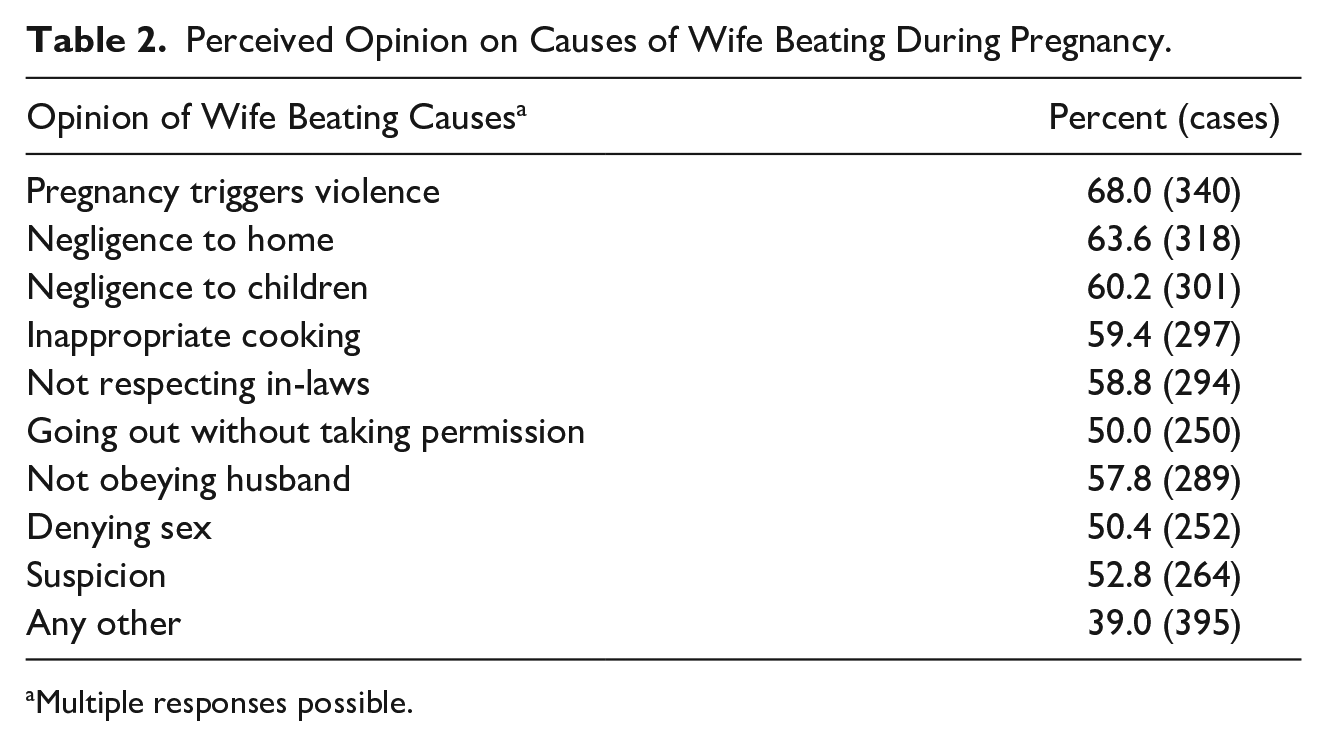
Multiple responses possible.
After taking note of their perceived opinion on reasons for violence during pregnancy, we asked about the actions to be taken after experiences of such violence. Table 3 shows that 17.4% of respondents said that one should tolerate violence, 73.4% said it should be discussed with family members, 10% held that one should leave home, and 51.6% of women stated that one should file a police complaint against husband. Around 16.8% of respondents stated that there was need of some other steps to be taken. When asked “Is violence under influence of alcohol acceptable?” 12.2% of respondents affirmed for acceptance.
Opinion on Whether to Take an Action Against of Wife Beating During Pregnancy.
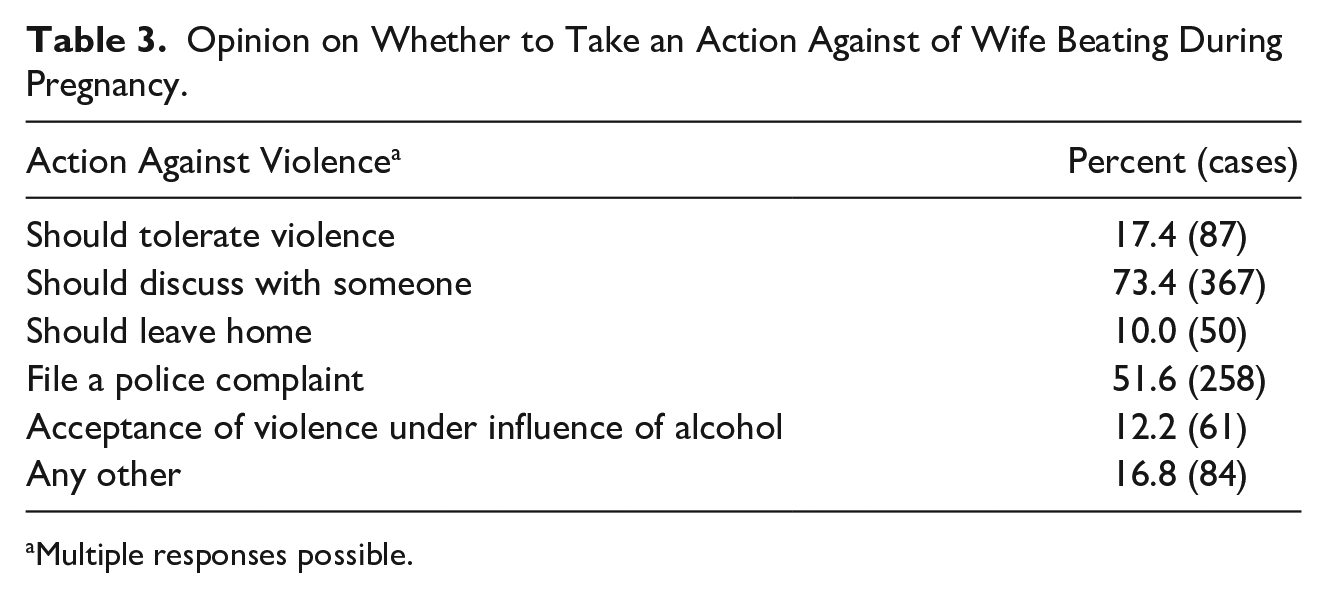
Multiple responses possible.
Prevalence of Violence Against Women During Pregnancy
Table 4 indicates the socioeconomic variables and occurrence of violence faced by women during their last pregnancy. Out of 500 women interviewed, 78 women reported of violence during last pregnancy which is 15.6%. The incidences of cases of violence during pregnancy was found to be higher in the age group less than 24 years, standing at 16.3% (38 women), whereas in age group 25 to 30, 16.2% (36) cases of violence were reported. The risk of incidences of violence were found to be decreasing with the growing age, where we found comparatively less cases of incidences which is 8.9% in the age group of 31 and above.
Prevalence of Any Violence During Pregnancy With Socio-Demographic Variables.

Educational status of women is also a matter of concern; 13.8% of illiterate women had faced violence in their last pregnancy followed by 10.8% of women with higher secondary level of education and above. Again, 29.4% of women with primary education and 17.1% women with secondary education reported to face any form of violence during their last pregnancy. As far as family type is concerned, nearly 18.6% of women residing in nuclear families and 13.6% of women in joint families recorded the occurrence of any form of violence. Furthermore, linking the number of children and prevalence of violence, we found that 14.6% of women having one child, 13.6% women having two children, and 24% women having three or more than three children reported having suffered any form of violence.
Type of Violence During Pregnancy
Table 5 shows almost 15.6% (cases 78/500) of respondents admitted that they have faced violence in any form during their last pregnancy. Although 9.2% said it was physical violence, 1.8% reported sexual violence, 11.2% psychological violence, and 5% reported violence in any other form than these. Furthermore, the study also explored the types of violent act faced by women. Table 6 indicates the types of violence and acts of violent behavior women faced during their last pregnancy. Under the behavior of psychological violence by husband, 8.6% of women reported insult or agonized actions, 5.6% of women said their husband humiliated them, 2.6% said their husband made them feel scared, 1.8% reported getting threatened, and about 7.4% reported psychological violence in other ways. With regard to physical violence, 4.6% of respondents experienced physical violence in the form of pushing or scrambling. Around 7.8% experienced slapping or that something was thrown at them with the intention to be harmed by their husband; 3.8% of women got kicked, pulled, or beaten; 1.6% cases of shoving or burning; 0.2% reported of being harmed using knife or gun; and about 2.2% respondents said they faced physical violence in some way other than those listed above. In sexual violence, 1% of respondents reported being subjected to sexual intercourse by their husband without consent or forceful sex, 0.8% of respondents had to do sex with husband under intimidation from husband, and 0.2% said their husband asked them to do something indecent. A total of 0.8% of women were reported to have had faced sexual violence in other forms in addition.
Prevalence of Type of Violence During Pregnancy.
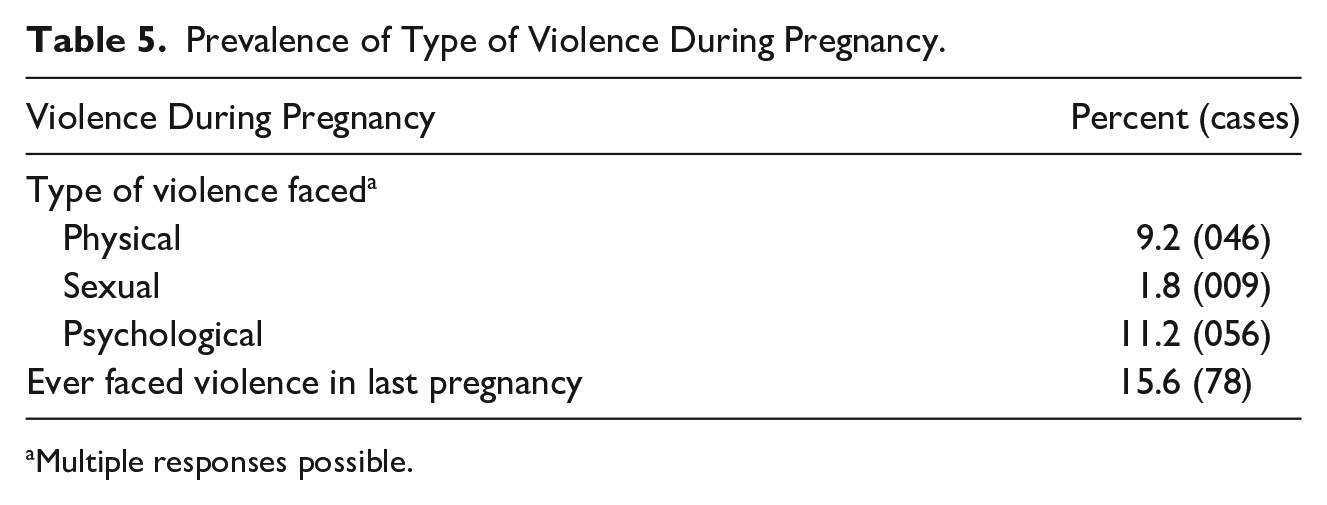
Multiple responses possible.
Experienced of Type of Violence and Violent in Specific.

Multiple responses possible.
Determinants of Violence Against Women During Pregnancy
The logistic regression has been applied to examine the factors contributing to the violence during pregnancy. Table 7 shows the ratio of adjusted and unadjusted odds of violence during pregnancy. In the adjusted model, women belonging to OBC group were found to have experienced higher levels of violence than the SC category women (adjusted odds ratio [AOR] = 3.611; 95% CI = [1.321, 9.872]). Women with three or more children faced higher odds of violence (AOR = 2.418; 95% CI = [0.899, 6.507]) compared with women with one child. A strong association has been found with women’s previous experience of violence, that is, women who reported to have experienced violence earlier were more likely to experience violence during pregnancy (AOR=39.107; CI=[17.425, 87.769]). The husband’s behavior also has strong association with the violence during pregnancy; husbands who consume alcohol are more likely to perpetrate violence during pregnancy than those who do not have any addiction (AOR=1.107; CI= [0.593, 3.498]).
Logistic Regression of Adjusted and Unadjusted Determinates of Violence During Pregnancy.
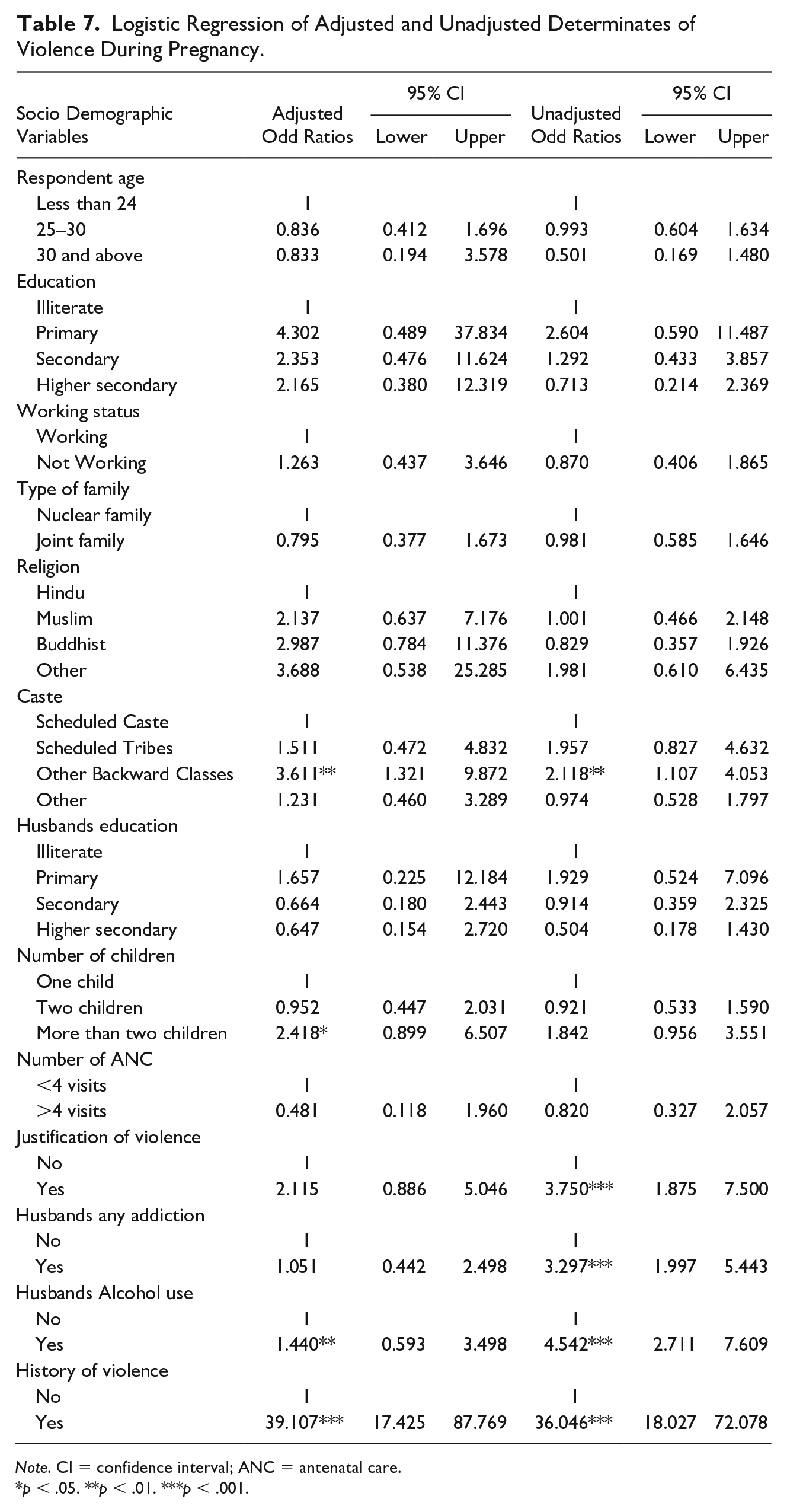
Note. CI = confidence interval; ANC = antenatal care.
p < .05. **p < .01. ***p < .001.
In the unadjusted model, women who justified violence under certain conditions were more likely to experience violence during pregnancy (unadjusted odds ratio (UOR) = 3.750; 95% CI = [1.875, 7.500]). Husbands with any type of addiction (UOR = 3.297; 95% CI = [1.997, 5.443]), especially alcohol addiction (UOR = 4.542; 95% CI = [2.711, 7.609]), increased the odds of violence against women during pregnancy.
Discussion
The study provided evidence that acceptance or justification of violence is very high among women and women who justified violence are at greater risk of becoming victims of violence during pregnancy. More than half of the surveyed women agreed that in certain conditions, husbands have right to beat wife even when she is pregnant. Earlier studies particularly in South Asia reported similar results of higher acceptance of wife beating (Jejeebhoy, 1998; Krause et al., 2017; Rani & Bonu, 2009; Waltermaurer, 2012). This may be attributed to the patriarchal norms inculcated in the women folk since childhood, which prescribed that women are obligated to perform certain duties in the household and if not appropriately executed in any situation, the partner has the authority to punish. A study by Kimuna et al. (2013) found that women who believed that wife beating was justified under certain circumstances were more likely to experience domestic violence. The gendered norms of society have considerable influence on women who are conditioned to believe in patriarchal authority and accept the violence inflicted by the husband. Effective intervention to forge gender equitable norms among men and women is necessary to overcome the menace of domestic violence. Furthermore, interventions to educate women about their rights, particularly right to protect from any form of violence, will reduce the justification of violence against women.
In this study, 15.6% women reported prevalence of violence against pregnant women in the study area. Further 9% reported of physical violence, 10% of psychological violence, and 2% of sexual violence have been reported. The study results bring to light important aspects of violence during pregnancy in India, particularly in urban slums. The recent NFHS-4 reported only 5% of violence against women in Maharashtra. This study results showed considerable higher percentages of prevalence than large population-based estimation in India. This higher prevalence of violence against pregnant women is a concern for many reasons. The earlier limited available studies in India reported similar or higher prevalence in India (Huria et al., 2005; Koski et al., 2011). Whereas some studies reported higher levels, a few others reported lower prevalence of violence against pregnant women than our current study (Das et al., 2013; Peedicayil et al., 2004). This may be attributed to methodological differences, definitional differences, and reporting patterns of violence (Babu & Kar, 2009; Ruiz-Pérez et al., 2007).
The study showed that younger women have experienced more violence than older age women. This is due to the stringent gender norms because of which young married women when entering new households often come groomed with clearly defined gender hierarchies and roles. She tends to belong to the lowest hierarchy in the new family (Kapadia-Kundu et al., 2007). However, some studies reported that increased age of women became a risk factor for violence during pregnancy (Jungari, 2021).
The study results indicated significantly strong association of husband’s alcohol consumption with increased odd of violence during pregnancy. The near universal response that alcohol consumption is a major precipitating factor for violence against women is consistent with many other studies in India and around the world (Begum et al., 2015; Kimuna et al., 2013; Satyanarayana et al., 2015; Wagman et al., 2018). Interventions to reduce alcohol abuse would serve as a practical solution to both the problems of alcohol abuse and violence. Men in slum communities have higher propensity for alcohol consumption and addiction, which gradually increases the chances of their inflicting violence on women in general and during pregnancy in particular.
The study shows important findings that women who were exposed to violence before pregnancy were at higher risk of being subjected to violence during pregnancy. The history of violence has emerged as a strong risk factor for violence during pregnancy. Although a few past studies reported history of violence increase the chances of violence during pregnancy (Castro et al., 2003; Karmaliani et al., 2008; Naved & Persson, 2008 ), there is no conclusive evidence available to compare the current results whether the history of violence is a risk factor or protective factor (Bağcıoğlu et al., 2014; Martin & Garcia, 2011).
Women who belonged to nuclear families were faced with higher chances of violence during pregnancy than women from the joint families. However, in the regression analysis, no significant association was found. This may be due to the burden of financial and household work shared by the husbands belonging to nuclear family. This calls for engaging husbands in the critical discussion on issues related to pregnancy and childbirth. Working women were more likely to experience violence during pregnancy than nonworking women. Evidence from other studies supported this study results (Begum et al., 2015; Krishnan et al., 2010). However, the factors for higher prevalence of violence among working women are not clear. More in-depth research investigations are needed to explore the contextual factors.
Women who belong from the OBC category were reported to suffer more violence than those belonging from the general category. The SC and ST women are vulnerable in multiple ways. They have little power to bargain with their husbands to protect themselves. Furthermore, they are also poor in terms of their economic capacity to face the consequences of violence. The previous studies reported similar findings in India (Kimuna et al., 2013).
Recent evidence gathered from around the world shows that women who have experienced violence during pregnancy are at increased risk of postpartum depression which eventually affects the quality of life of both women and children (Abbaszadeh et al., 2011; Beydoun et al., 2010; Kendall-Tackett, 2007). Hence, there is an urgent need to have more studies to examine the negative effects of violence during pregnancy on both mother and child. The intervention to reduce violence in general and violence inflicted during pregnancy in particular should target intimate male partners. Interventions which exclude husbands may not be effective in reducing the occurrence of violence during pregnancy.
Limitations of the Study
This study has some limitations which are important to note here. The study was conducted in the slum communities of Pune city in Maharashtra; hence the results of this study may not be generalized to other community settings or general population. Also, the sample with which the study was carried out is limited; therefore, while quantifying or assessing the prevalence, one must understand the context. The cross-sectional study design does not allow for establishing a cause-and-effect relationship. Hence, the association observed in regression results could be the function of some factors mentioned earlier or others. Furthermore, the variable justification of violence by women does not reinforce victim-blaming but intended to examine the women attitude and will help in interventions to prevention of violence.
Conclusion
The prevalence of violence during pregnancy in this study results is quite higher than the corresponding national rates. Husband’s education, women’s education, husband’s alcohol abuse, and women’s acceptance of violence have emerged as important determinants for violence during pregnancy. Furthermore, women who have experienced violence before pregnancy were at greater risk of violence during pregnancy. Interventions to reduce the violence during pregnancy must be directed at both husband and wife. Sensitization of men on the consequences of violence during pregnancy may help to reduce the incidences of violence. Involvement of men in maternal health, particularly in antenatal care, will also help to reduce the occurrence of violence against women during pregnancy. The personnel of health care sector should be trained to identify the symptoms of inflicted violence at antenatal care visits. More in-depth research is needed to understand the various consequences of violence perpetrated during pregnancy in India. The immediate efforts are needed from the government to address this issue considering wider consequence of the problem. Reproductive and Child Health (RCH) programs must include the components of screening for the possible violence cases during antenatal care services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was received from the Savitribai Phule Pune University under the scheme of University with Potential of Excellence (UPE) phase-II granted by the University Grants Commission, New Delhi.