
Abstract
Childhood adversities have significantly negative consequences on physical and mental health. The Childhood Experience of Care and Abuse Questionnaire, Version 3 (CECA.Q3) interview, as an extended version of the CECA.Q, is widely used in the assessment of childhood adversities. Although its reliability and validity have been demonstrated, the application of CECA.Q3 is limited due to its intensive and lengthy interview. This article aimed to develop and validate a brief form of the CECA.Q3 (CECA.Q3-BF) among a population of mood disorders. Data analyzed were from a clinical sample of 210 patients with mood disorders. Data were randomly split into training and testing datasets. The training data set was used for scale reduction by applying principal component factor analysis, while the testing one was used for cross-validation to examine whether the CECA.Q3-BF could have a good yield of accuracy. The optimal cutoff points of the CECA.Q3 were also tested. Overall, four out of eight subscales had items reduction without compromising their accuracy of measurements for childhood adversities. They are Antipathy (reduced by four items), Neglect (reduced by five items), Psychological Abuse (reduced by 15 items), and Role Reversal (reduced by 11 items). The CECA.Q3-BF removed 35 items (35/100, 35%) from the full CECA.Q3. The accuracy of CECA.Q3-BF was validated in the testing dataset. The CECA.Q3-BF offers a brief but good accuracy of measure for childhood adversities. Future studies are warranted to further validate this brief form. The CECA.Q3-BF is expected to improve the application of CECA.Q3 in clinical and epidemiological surveys, as it significantly reduces the length of the interview and therefore has better compliance.
Introduction
Childhood adversities are defined as “exposures during childhood or adolescence to environmental circumstances that are likely to require significant psychological, social, or neurobiological adaptation by an average child and that represent a deviation from the expectable environment” (McLaughlin, 2016). The expectable environment refers to a variety of environmental inputs that the human brain requires to develop normally, such as sensory inputs, exposure to language, and the presence of a sensitive and responsive caregiver (Fox et al., 2010).
Exposure to childhood adversities, for example, child abuse and neglect, exposure to violence, and family economic hardship, is common across the world. It was estimated that about 50% of participants in the United States had adverse childhood experiences (ACEs) across various epidemiological surveys (Green et al., 2010; Kessler et al., 1997; McLaughlin et al., 2010, 2012). Nearly 85% of young people reported experiencing at least one adversity during their childhood in the Russian Federation (Kachaeva et al., 2014). The WHO World Mental Health Surveys documented a prevalence of childhood adversities in high-income (38%), high-middle-income (39%), and low- and lower-middle-income countries (39%) (Kessler et al., 2010).
Childhood adversities in the form of childhood maltreatment and household dysfunction have been investigated as a significant risk for both physically and psychologically negative consequences. ACEs have been linked to numerous health behaviors and conditions, including smoking, obesity, diabetes, HIV-risk related behaviours (e.g., substance misuse, unprotected sex), and cardiovascular disease (Centre on the Developing Child, 2007; Champbell et al., 2016; Pedersen, 2018). Exposure to early life adversities increases the risk of having a wide variety of subsequent psychiatric disorders, such as mood disorders, anxiety, substance use, psychotic experiences, personality disorders, disruptive behavior disorders, and even antisocial behaviors (Afifi, 2012; Afifi et al., 2011; Braga et al., 2017; Green et al., 2010; Li et al., 2016; McGrath et al., 2017; McLaughlin et al., 2012). A dose–response relationship between childhood adversities and these negative health outcomes has also been detected in both children and adults (Atkinson et al., 2015; Bright et al., 2016; Dong et al., 2004). Notably, the impact of childhood adversities can pass onto the next generation (Galler & Rabinowitz, 2014; Pedersen, 2018). Epigenetic changes can be triggered by environmental factors including early life adversities, which alters gene expression and its impacts could last through the life span and even pass on to the next generations (Gudsnuk & Champagne, 2012; Kundakovic & Champagne, 2015). Research has shown an increased risk of posttraumatic stress disorder (PTSD), mood disorders, substance abuse, asthma, and excessive television watching among the offspring whose parent(s) were exposed to childhood adversities (Le-Scherban et al., 2018; Yehuda et al., 2008).
Specifically, considerable studies support the relationship between childhood adversities and mood disorders, including major depressive disorder (MDD), bipolar disorder (BD) (type I—BDI and type II—BDII) (Angst et al., 2011; Li et al., 2016; Liu, 2017; Palmier-Claus et al., 2016; Shanahan et al., 2011). It was found that childhood adversities, including child abuse and parental loss, were 2.63 times more likely to have occurred in patients with BD compared with nonclinical controls (Palmier-Claus et al., 2016). Meta-analyses of epidemiological studies also found a two- to three-fold increased odds of recurrent and chronic depression in adulthood (Li et al., 2016; Nanni et al., 2012). Moreover, two longitudinal studies showed that adverse childhood experiences predicted more severe depressive symptoms and longer time to remission in adults (Fuller-Thomson et al., 2014; Rhebergen et al., 2012). Furthermore, a study examining the relationship between childhood psychological abuse and depressive symptoms in adults showed that psychological abuse was positively related to automatic negative thoughts and negatively related to automatic positive thoughts, and these automatic thoughts both mediated the relationship between childhood maltreatment and symptoms of depression in adulthood (Gibb et al., 2007).
Although childhood adversities are associated with many serious negative consequences, the good news is that early detection and intervention can prevent, or at least attenuate, the impact on the later-on health issues (Centre on the Developing Child, 2007; Pedersen, 2018). As a result, screening for exposure to child adversities is a critical step to identifying and preventing children at risk from developing later onset of psychiatric disorders. In addition, given that childhood adversities have long-term and detrimental effects on mental health, it is also important for mental health professionals to detect early life adversities in their patients, which will help in secondary prevention of mental illnesses, such as remission and/or relapse of depression.
The Childhood Experience of Care and Abuse Questionnaire, Version 3 (CECA.Q3) is one of the most widely used measurement tools for assessing the exposure to childhood adversities (see Supplemental Appendix 1 for the full questionnaire). It is an extended version of the original CECA.Q which is a retrospective self-report assessment used to complete collect information on adverse events experienced before the age of 17 years. Because of its good psychometric properties, careful, detailed, and behaviorally-based questioning, and wide range of experiences covered, the CECA.Q is to be the considered the gold standard for the assessment of childhood adversities (Schimmenti & Bifulco, 2015). This tool has been developed for over 20 years and is being used in clinical, forensic, and social work practice (CATS Middlesex University, 2019). It has been translated into numerous languages and is used in Europe, the United States, Canada, South America, and Asia (CATS Middlesex University, 2019). The CECA.Q3 examines relationships with parents and any abusive experiences in childhood and adolescence. These negative experiences include parental loss/separation, parental care (antipathy, neglect, and psychological abuse), role reversal, support, physical abuse, and sexual abuse (Bifulco et al., 2005). Research has demonstrated its reliability (Cronbach’s α = .80–.87) and validity (correlation coefficient r = .35–.74, p < .01) both in community and clinical samples (Bifulco et al., 2005; Fisher et al., 2011; Li et al., 2006).
Why Is a Brief Form of the CECA.Q3 Necessary?
The application of current the CECA.Q3 is limited by a large number of items and length of time it takes to complete in clinical populations. According to a review study on measurement instruments of childhood adversities, the CECA.Q required a relatively longer time (15–20 min) to complete and score compared with other instruments, such as Child Maltreatment Interview Schedule (CMIS, 5–10 min), Child Abuse and Trauma Scale (CATS, 5–10 min), and Child Trauma Questionnaire (CTQ, 10–15 min) (Burgermeister, 2007). This may affect participants’ cooperation and adherence and may result in high missing data and loss of follow-up. In addition, some items on the childhood adversities measures of CECA.Q3 have been developed based on the investigators’ clinical experience and sense (Bifulco et al., 1994), rather than empirically data-driven methods, to yield specific childhood adversity dimensions or constructs.
Why Is the Brief Form of the CECA.Q3 More Beneficial in a Clinical Setting?
First, the prevalence of childhood adversities in patients with mental disorders, especially mood disorders, is higher than that in the general population. Research has compared the prevalence of ACEs among adults with mood disorders with the U.S. general population (Lu et al., 2008). Approximately 89% of participants with mood disorders reported at least one adverse experience in childhood. In comparison, this rate was 64% and 74%, respectively, from two population surveys (Lu et al., 2008). An extremely high prevalence of child adversities (93%) was also recently found in Kenyan patients with substance use disorders (Kiburi et al., 2018).
Second, given the well-established relationship between childhood adversities and mood disorders, it is necessary to screen for the exposure to early life adversities for this clinical population to better understand their situation. A more practical instrument could shorten the length of the interview, improve patients’ compliances, reduce the psychiatric and psychological burden from the recall of negative experiences, and assist in the investigation of underlying mechanisms between maltreatment and mood disorders.
This project is targeted at the above-mentioned issues in the measurement of childhood adversities. We aim to (a) develop and validate a brief form of the CECA.Q3 (CECA.Q3-BF) in a clinical population with mood disorders to improve its application; and (b) determine optimal cutoff points of the CECA.Q3-BF for participants with mood disorders.
Method
Study Sample
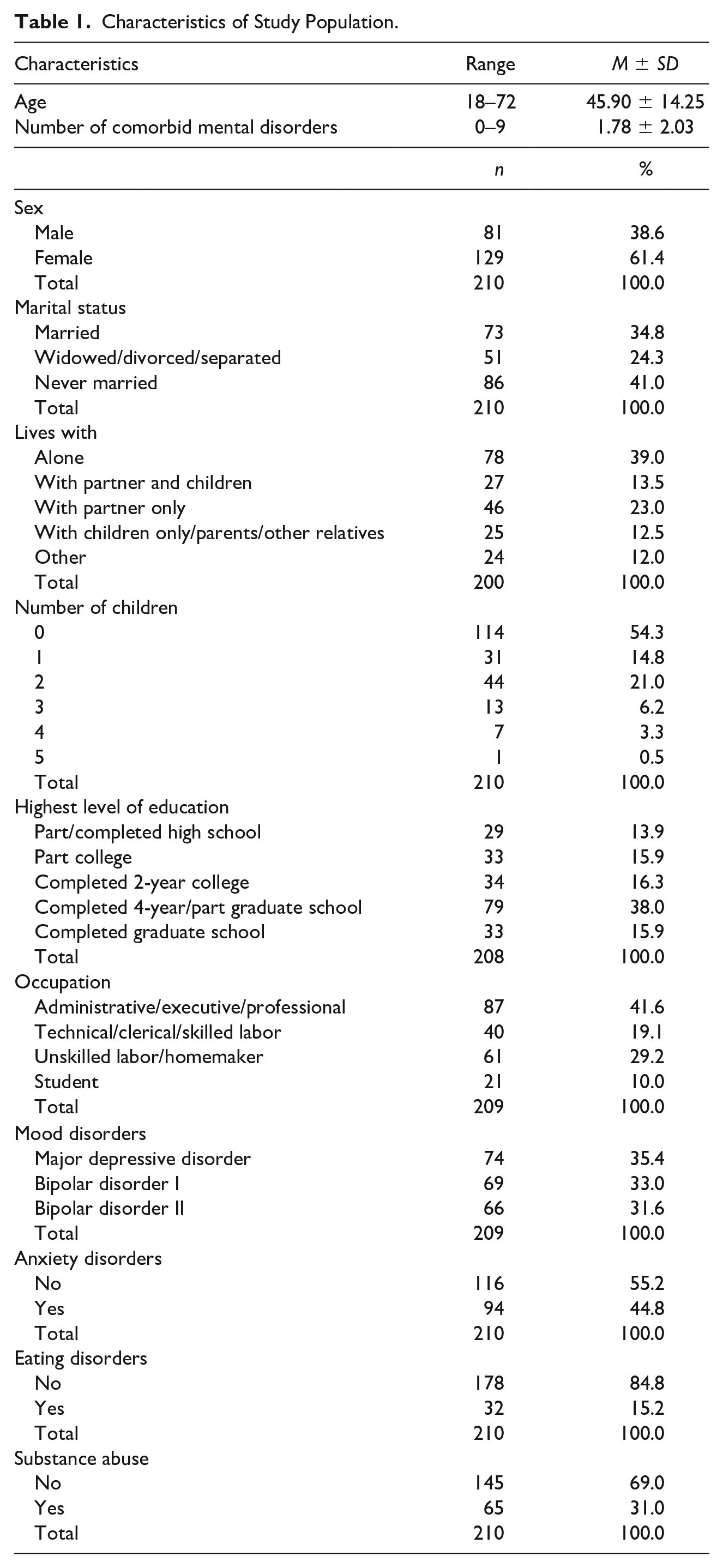
A total of 241 outpatients with a clinical diagnosis of mood disorder were recruited from the Mood Disorders Program (MDP) of the McGill University Health Centre, a large, university-based teaching hospital in Montreal, Canada. The hospital provides services for the general population representing all socioeconomic levels and a wide range of ethnic groups. Only those who were aged 18 years or more at the time of study screening and had a diagnosis of current or lifetime MDD and/or BDI or BDII) according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; Bell, 1994) and participated in the CECA.Q3 interview were included in this study. Those who cannot understand or communicate either in English or French were excluded. All participants were clinically euthymic, therefore, not suffering from a current mood episode. A total number of 210 participants were included in this study (Table 1). The ethical approval was obtained from the Research Institute of the McGill University Health Center (11-520-PSY), with informed consent completed by all the study participants.
Characteristics of Study Population.
Study Procedure
Eligible subjects with a primary mood diagnosis of MDD, BDI, or BDII were identified and informed about the study by a member of their treating team at the MDP, usually either a psychiatrist, psychiatry resident, or nurse. In addition to having a primary mood disorder, subjects had to be currently euthymic (i.e., not actively experiencing a major depressive, manic, or hypomanic episode) and able to provide informed consent before being approached by a member of the research team for recruitment. The subjects were then met by either a graduate student or trained research volunteer (e.g., medical school student) who would describe the purpose of the study and its procedures. Upon agreeing to participate and signing the consent form, subjects were given a package of questionnaires to take home and complete. They then underwent a single 3-hr session which included a psychiatric diagnostic interview and a family history interview administered by a trained graduate student or research assistant. Following their participation, subjects were provided with $20 compensation to cover their travel expenses. Accuracy about the participants’ psychiatric history, treatment, and the diagnosis was verified by a review of their medical charts and confirmation from their treating physician when necessary.
Measures
Clinical diagnoses of psychiatric diseases
The research version of the Structured Clinical Interview for the Diagnosis of DSM-IV Disorders (SCID) was used to assess participants’ sociodemographic characteristics and to verify the diagnoses of MDD and BD. This structured interview was administered by trained master’s-level graduate students who underwent a 4-month SCID-training conducted by a SCID-certified trainer. The interviews took between 45 minutes and 2 hours to complete. In addition, we also collected information on a variety of mental disorders via SCID, including mood disorders (MDD, BD type I and type II, dysthymic disorder, and schizoaffective disorder), substance use disorders (alcohol abuse, alcohol dependence, substance abuse, and substance dependence), anxiety disorders (panic disorder, agoraphobia disorder, social phobia, specific phobia, obsessive-compulsive disorder [OCD], PTSD, and generalized anxiety disorder [GAD]), and eating disorders (anorexia, bulimia, and binge eating disorder).
Childhood adversities
Participants were invited to complete the CECA.Q3, which was used to measure various types of childhood adversities, including subscales Parental Loss, Parental Care (Antipathy, Neglect, and Psychological Abuse), Role Reversal, Support, and Physical and Sexual Abuse.
Parental loss
Parental loss during childhood is assessed in the CECA.Q3 through two screening questions: (1) “Did either parent die before you were age 17,” and (2) “Have you ever been separated from your parent for 1 year or more before age 17.” These items offer binary options (1 = Yes and 0 = No for mother and father, respectively), and detailed questions are then asked subsequently about the events, such as age, duration, and reason for separation. This section yields a score ranging from 0 to 4 with higher scores indicating more loss risk factors.
Antipathy
Parental antipathy refers to “hostile or cold parenting” and is assessed by eight statements like “She/He was very difficult to please” (Bifulco et al., 2005). These antipathy items are scored for mother and father, respectively, on a 5-point Likert-type scale ranging from 1 (no, not at all) to 5 (yes, definitely) (Bifulco et al., 2005). This section yields a score ranging from 8 to 40, with higher scores indicating more maternal/paternal antipathy during childhood. Cutoff scores for adults with major depression are used to indicate “marked or moderate” level of severity for antipathy: 28 points for mother, 30 for father (CATS Middlesex University, 2014).
Neglect
Neglect refers to parent’s disinterest in material needs, health, schoolwork, and friendships; it is evaluated by eight statements like “She/He was concerned about my worries” and “She/He neglected my basic needs (e.g., food and clothes).” These neglect items are scored for mother and father, respectively, on a 5-point Likert-type scale ranging from 1 (no, not at all) to 5 (yes, definitely) (Bifulco et al., 2005). This section yields a score ranging from 8 to 40, with higher scores indicating more maternal/paternal neglect during childhood. Cutoff scores for adults with major depression are used to indicate “marked or moderate” level of severity for neglect: 25 points for mother, 26 for father (CATS Middlesex University, 2014).
Psychological abuse
There are 17 items for mother and father, respectively, to assess the amount and frequency of psychological abuse during childhood for statements like “She/He would tease me.” Each item is scored as 0 (no), 1 (unsure), and 2 (yes). This section yields a score ranging from 0 to 34 for mother and father, respectively, with higher scores indicating more maternal/paternal psychological abuse. The corresponding frequency for each item is scored for mother and father, respectively, from 0 (never) to 3 (often). Thus, it yields a total frequency score ranging from 0 to 51 for mother and father, respectively, with higher scores indicating more frequent maternal/paternal psychological abuse during childhood. The cutoff score for the “marked or moderate” psychological abuse is not officially defined (CATS Middlesex University, 2014). In this study, the cutoff of the mean plus one standard deviation was used. This yielded a cutoff score of 12.6 and 12.3 for maternal and paternal psychological abuse, respectively.
Role reversal
The CECA.Q3 assesses the experience of role reversal or parentification during childhood, which refers to the degree to which a child has to take over the responsibilities of a parent at a very young age, or the degree to which a child was expected to provide emotional support by parents which is more appropriate from an adult (Brown et al., 2007). A total of 17 questions, such as “Did you have a lot of responsibility in the home as a child, more than other children your age?” are used in this subscale and scored on a 5-point Likert-type scale ranging from 1 (no, not at all) to 5 (yes, definitely). The total role reversal scores could range from 17 to 85, with higher scores indicating more role reversal during childhood. Similarly, we used the mean plus one standard deviation of the total score to indicate the severity of role reversal. This yielded a cutoff score of 54.0.
Support
Close relationships in childhood are assessed in the CECA.Q3 through three screening questions regarding supportive adult, supportive peer, and closest people. These items offer binary options (1 = Yes, 0 = No), and questions on the relationship are then asked subsequently. Total support scores could range from 0 to 3, with higher scores indicating better support during childhood.
Physical abuse
Physical abuse during childhood is screened by a single question “When you were a child or teenager were you ever hit repeatedly with an implement (such as a belt or stick) or punched, kicked or burnt by someone in the household” (1 = Yes, 0 = No). A series of severity questions are then followed to collect information about the abusive experience from mother and father, respectively. These questions are (a) “Did the hitting happen on more than one occasion?” (yes = 1, no = 0), (b) “How were you hit?” (belt or stick or punched = 1, kicked = 1, hit with hand = 0, other = 0), (c) “Were you ever injured, for example, bruises, black eyes, broken limbs?” (yes = 1, no = 0), and (d) “Was this person so angry they seemed out of control?” (yes = 1, no = 0). The severity of physical abuse for each parent could range from 0 to 4, with higher scores indicating more severe physical abuse from that parent during childhood. The cutoff score for “marked” physical abuse is a score of at least 1 for one or both parent(s) (Bifulco et al., 2005).
Sexual abuse
Three screening questions are used to screen sexual abuse during childhood. One example of these three questions is “When you were a child or teenager, did you ever have any unwanted sexual experiences” which is scored as 0 (no), 1 (unsure), and 2 (yes). The total score could range from 0 to 3, with higher scores indicating more sexual abuse during childhood. Seven subsequent questions are then followed to evaluate the severity of sexual abuse, such as “Was the other person someone you knew” (1 = Yes, 0 = No). The severity of sexual abuse yielded scores ranging from 0 to 7, with higher scores indicating more severe sexual abuse. The cutoff for “marked or moderate” sexual abuse is at least one “yes” answer for these three screening questions (Bifulco et al., 2005).
Statistical Analyses
The total analytic sample of 210 subjects was randomly split into two groups: a training group and a testing group for cross-validation purposes (Arlot & Celisse, 2010). The training group was used for item deduction, whereas the testing group was used to verify the reliability and classification of the shortened questionnaire compared with the full version.
For the subscales of CECA.Q3 with Likert-type scale or ordinal format (Antipathy, Neglect, Psychological Abuse, and Role Reversal), principal component analyses were applied because the primary purpose was to identify and compute composite scores for the factors underlying the short version of the CECA.Q3. Principal component analysis has been commonly used to “test whether an existing measurement scale (e.g., a questionnaire) can be shortened to include fewer items (e.g., questions/statements)” (Laerd Statistics, 2018), and has been applied in many studies on the development of shortened questionnaires (Barke et al., 2016; Foerster et al., 2015; Goodwin et al., 2015; Wang et al., 2018). For those subscales with binary answers (Parental Loss, Support, Physical Abuse, and Sexual Abuse), categorical principal component analyses were used (Linting et al., 2007).
Prior to the factor analysis, Bartlett’s test of sphericity (Snedecor & Cochran, 1989) was conducted to ensure sufficient correlations exist among the items to proceed (p < .05). Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy (>0.60) (Kaiser & Rice, 1974) was also examined. Principal component analysis with varimax rotation was used to remove potentially redundant items for each studied subscale. Given the missing values in the dataset, maximum likelihood with the expectation-maximization (EM) algorithm was used to estimate the covariance matrix (Graham, 2009; Truxillo, 2005; Weaver & Maxwell, 2014). The number of factors was determined by the scree test with the eigenvalues greater than 1. Items with lower than cutoff score of factor loading were then removed. The cutoff score of factor loading was defined according to sample size (Hair et al., 2014). As different sample sizes will offer different power to the analysis, Hair et al. believed that when it comes to determining the cutoff score of factor loadings, the sample size should also be taken into account. The cutoff score of factor loading should be smaller when the sample size is large; conversely, the cutoff score could be larger when the sample size is small (Hair et al., 2014). In this analysis, the cutoff score of factor loading was varied by subscale. The Cronbach’s alpha was checked before and after to see if the exclusion of the items significantly decreased the reliability. Items significantly associated with the changes of the Cronbach’s alpha were retained in the subsequent analyses. All these above analyses were done with the training dataset and by subscales.
In the testing dataset, cross-validation was conducted to examine whether the CECA.Q3-BF could have a good yield of accuracy. Cronbach’s alpha was used to examine the reliability of CECA.Q3-BF. Sensitivity, specificity, and area under the receiver operating characteristic curve (AUC) were generated by comparing the test results from the full version (as the gold standard) with the brief version of CECA.Q3. New cutoff points for each subscale were also determined by maximizing the combination of sensitivity, specificity, and correct classification. All the analyses were conducted using Stata, Version 14 (StataCorp., 2015).
Results
Table 1 showed the sociodemographic characteristics of the study sample. The study cohort (N = 210) included more females (61.4%) than males (38.6%). Most of the participants were never married (41.0%), living alone (39.0%), having no child (54.3%), and with a high level of education (graduate school, 53.9%) and occupation (administrative/executive/professional, 41.6%). The study sample was randomly split into training (n = 103) and testing groups (n = 107). There was no significant difference between these two groups in terms of subjects’ sociodemographic characteristics (e.g., age, sex, education, marital status, living arrangement, number of kids, and occupation) and prevalence of psychiatric diagnoses (p > .05).
Subscales Parental Loss, Support, Physical Abuse, and Sexual Abuse
For the subscales with dichotomous answers (Parental Loss, Support, Physical Abuse, and Sexual Abuse), no items were removed from the analyses. The statistical results are available upon request.
Subscales Antipathy, Neglect, Psychological Abuse, and Role Reversal
All the four subscales had items reduction without compromising their accuracy of measurements for childhood adversities. They were Antipathy (mother—removed two items, father—two items), Neglect (mother—three items, father—two items), Psychological Abuse (mother—six items, father—nine items), and Role Reversal (11 items). A summary of studied scales for their remaining and removing items is shown in Supplemental Appendix 2. Detailed statistics for factor analysis of the remaining items, including factor loadings, uniquenesses, and communalities, are shown in Supplemental Appendix 3. Reliability and accuracy indicators, including Cronbach’s alpha, AUC, sensitivity, and specificity, and new cutoff points for “market or moderate” severity in the CECA.Q3-BF are presented in Table 2. To illustrate the process of principal component analysis in each subscale, we present the details as following:
Statistics for CECA.Q3-BF by Subscale.

Note. KMO = Kaiser–Meyer–Olkin measure of sampling adequacy; α = Cronbach’s alpha; AUC = area under the receiver operating characteristic curve.
Antipathy mother
Initially, the factorability of the eight antipathy mother items was examined. Due to the missing values in the data, several well-recognized criteria for the factorability of covariance, instead of correlation, were used. First, it was observed that all the eight items had at least 0.7 of covariance with at least one other item, suggesting reasonable factorability. Second, the maximum likelihood with the expectation-maximization (EM) algorithm was also used to estimate the covariance matrix. The EM covariances were also all over 0.7 (see Supplemental Appendix 4). Third, the KMO was 0.85, indicating that the data are meritorious for factor analysis (Kaiser & Rice, 1974), and Bartlett’s test of sphericity was significant, χ2(28) =429.80, p < .05. Finally, the communalities were at least around 0.5, further confirming that each item shared some common variance with other items. Given these overall indicators, factor analysis was deemed to be suitable for all eight items.
The principal component analysis initially generated four factors, which explained 54.7%, 24.8%, 16.8%, and 3.8% of the variance, respectively. Using an eigenvalue greater than 1, the scree test yielded a 1-factor solution with eigenvalues of 4.4 accounting for 54.7% of the total variance. Varimax rotation was performed, and based on the sample size, a cutoff score of 0.60 for rotated factor loading was used to determine whether an item would be retained or removed for CECA.Q3-BF. Two items were eliminated because they did not contribute to a simple factor structure and failed to meet the minimum criteria of factor loading. Thus, the brief form subscale retains six items and could score from 6 to 30, with higher scores indicating more maternal antipathy during childhood.
Antipathy father
The factorability of the eight antipathy father items was initially examined. First, it was observed that all the eight items had at least 1.7 of covariance with at least one other item, suggesting reasonable factorability. Second, the EM covariances were also all over 1.1 with at least one other item. Third, the KMO was 0.85, indicating that the data are meritorious for factor analysis (Kaiser & Rice, 1974), and Bartlett’s test of sphericity was significant, χ2(28)=318.82, p<.05. Finally, the communalities were all above 0.4, further confirming that each item shared some common variance with other items. Factor analysis was deemed to be suitable for all eight items.
The principal component analysis initially generated four factors, which explained 48.9%, 21.0%, 16.2%, and 13.9% of the variance, respectively. The scree test yielded a three-factor solution with eigenvalues of 2.2, 1.6, and 1.3, respectively, accounting for 86.1% of the total variance. Varimax rotation was performed, and a cutoff score for rotated factor loading was 0.60. Three items failed to meet the minimum criteria of the factor loading, but one of which significantly affected reliability and thus was retained in the scale. Therefore, two items were eliminated, and the brief form subscale retains six items with total score ranged from 6 to 30, with higher scores indicating more paternal antipathy during childhood.
Neglect mother
The factorability of the eight neglect mother items was initially examined. First, all the eight items had at least 1.1 of covariance with at least one other item, suggesting reasonable factorability. Second, the EM covariances were also all over 0.4 with at least one other item. Third, the KMO measure was 0.74, indicating that the data are middling for factor analysis (Kaiser & Rice, 1974), and Bartlett’s test of sphericity was significant, χ2(28)=250.04, p<.05. Finally, the communalities were all above 0.3, further confirming that each item shared some common variance with other items. Factor analysis was deemed to be suitable for all the items.
The principal component analysis initially generated four factors, which explained 53.3%, 13.3%, 27.1%, and 6.3% of the variance, respectively. The scree test yielded a two-factor solution with eigenvalues of 2.1 and 1.6, respectively, accounting for 81.4% of the total variance. Varimax rotation was performed, and a cutoff score for rotated factor loading was 0.55. Three items failed to meet the minimum criteria of factor loading and thus were eliminated. The brief form subscale retained five items and could score from 5 to 25, with higher scores indicating more maternal neglect during childhood.
Neglect father
The factorability of the eight neglect father items was initially examined. First, all the eight items had at least nearly 1.0 of covariance with at least one other item, suggesting reasonable factorability. Second, the EM covariances were also at least nearly 1.0 with at least one other item. Third, the KMO measure was 0.86, indicating the data are meritorious for factor analysis (Kaiser & Rice, 1974), and Bartlett’s test of sphericity was significant, χ2(28)=454.25, p<.05. Finally, the communalities were all above 0.4, further confirming that each item shared some common variance with other items. Factor analysis was deemed to be suitable for all the items.
The principal component analysis initially generated four factors, which explained 56.6%, 27.2%, 8.5%, and 7.8% of the variance, respectively. The scree test yielded a one-factor solution with eigenvalues of 4.1, accounting for 56.6% of the total variance. Varimax rotation was performed, and a cutoff score for rotated factor loading was 0.54. Two items failed to meet the minimum criteria of factor loading and thus were eliminated. The brief form subscale retained six items and could score from 6 to 30, with higher scores indicating more paternal neglect during childhood.
Psychological abuse mother
The factorability of the 17 psychological abuse mother items was initially examined. First, most items had at least 0.2 of covariance with at least one other item, suggesting some factorability. Second, most EM covariances were also at least nearly 0.2 with at least one other item. Third, the KMO measure was 0.78, indicating that the data are middling for factor analysis (Kaiser & Rice, 1974), and Bartlett’s test of sphericity was significant, χ2(136)=910.38, p<.05. Finally, the communalities were at least nearly 0.4, indicating that each item shared some common variance with other items. Factor analysis was deemed to be suitable for this subscale.
The principal component analysis initially generated 11 factors. The first factor explained 46.4% of the variance. The rest factors explained only 1.8% to 8.8% of the variance. The scree test yielded a four-factor solution with eigenvalues of 5.6, 1.1, 1.5, and 1.1 accounting for 69.8% of the total variance. Varimax rotation was performed, and a cutoff score for rotated factor loading was 0.60. Six items failed to meet the minimum criteria of factor loading and thus were eliminated. The brief form subscale retained 11 items and could score from 0 to 22, with higher scores indicating more maternal psychological abuse during childhood.
Psychological abuse father
The factorability of the 17 psychological abuse father items was examined. First, most items had at least 0.2 of covariance with at least one other item, suggesting some factorability. Second, most EM covariances were over 0.5 with at least one other item. Third, the KMO was 0.85, indicating that the data are meritorious for factor analysis (Kaiser & Rice, 1974), and Bartlett’s test of sphericity was significant, χ2(136)=854.90, p<.05. Finally, the communalities were at least nearly 0.4, confirming that each item shared some common variance with other items. Factor analysis was deemed to be suitable for the subscale.
The principal component analysis initially generated 11 factors. The first five factors explained 17.6%, 21.6%, 18.7%, 10.2%, and 8.6% of the variance. The rest factors explained only 2.1% to 5.6% of the variance. The scree test yielded a 2-factor solution with eigenvalues of 6.0 and 2.1 accounting for 40.3% of the total variance. Varimax rotation was performed, and a cutoff score for rotated factor loading was 0.60. Nine items failed to meet the minimum criteria of factor loading and were eliminated. The brief form subscale retained eight items and could score from 0 to 16, with higher scores indicating more paternal psychological abuse during childhood.
Role reversal
One out of 20 items in this subscale was removed from analysis due to high percentage of missing data (55.3%, 57/103). The factorability of the 19 psychological abuse father items was examined. First, most items had at least 1.2 of covariance with at least one other item, suggesting reasonable factorability. Second, most EM covariances were over 1.0 with at least one other item. Third, the KMO measure was 0.72, indicating that the data are middling for factor analysis (Kaiser & Rice, 1974), and Bartlett’s test of sphericity was significant, χ2(171)=552.01, p<.05. Finally, the communalities were all over 0.3, confirming that each item shared some common variance with other items. Factor analysis was deemed to be suitable for the subscale.
The principal component analysis initially generated 13 factors. The first six factors explained 12.4%, 20.0%, 12.5%, 9.5%, 10.7%, and 8.1% of the variance. The rest factors explained only 2.0% to 6.1% of the variance. The scree test yielded a two-factor solution with eigenvalues of 4.4 and 2.4 accounting for 32.5% of the total variance. Varimax rotation was performed, and a cutoff score for rotated factor loading was 0.60. Thirteen items failed to meet the minimum criteria of factor loading. However, two of them were kept in the CECA.Q3-BF because of their significant impacts on reliability. Thus, the brief form subscale retained nine items and could score from 9 to 45, with higher scores indicating more role reversal during childhood.
Discussion
In this study, we developed and validated a brief form of the CECA.Q3 (CECA.Q3-BF) in a clinical sample of patients with mood disorders. Overall, the CECA.Q3-BF removed 35.0% of the original items (35/100 items) from the CECA.Q3. For subscales Antipathy, Neglect, Psychological Abuse, and Role Reversal, it had no substantial deduction of reliability due to the reduction of items compared with the full version. In some subscales (e.g., Neglect Mother, Neglect Father, and Psychological Abuse Father), the CECA.Q3-BF yielded even better reliability than the full version. The cross-validation by subscales in the testing dataset showed acceptable internal reliability and accuracy of CECA.Q3-BF. The AUCs for each subscale were all above 0.90, along with very satisfactory sensitivities and specificities. The CECA.Q3-BF yielded equally or even more reliable and accurate indices for childhood adversities measurement in this clinical population with improved feasibility, which means a shorter questionnaire period, better participants’ cooperation and adherence, and avoiding potential issues related to long self-reporting period, such as missing data and loss of follow-up.
From the analyses, there were no items removed from the subscales with binary answers—Parental Loss, Support, Physical Abuse, and Sexual Abuse. One possible reason is that there are only a few screening questions in such subscales as Parental Loss (two items), Support (three items), and Sexual Abuse (three items). It is not easy to reduce the dimension when it is already small. Another potential reason is that for Physical Abuse and Sexual Abuse, the questions for the severity of abusive experiences are following a progressive logic. Only those participants answered “yes” in the screening questions will have the chance to answer the severity questions. Therefore, the available sample size for these severity questions is too small to detect positive findings.
This study developed and validated a brief form of the CECA.Q3 (CECA.Q3-BF), which significantly reduced the time to complete the questionnaire while maintaining the accuracy of the scale. CECA.Q3 has several advantages in terms of having satisfactory reliability and validity as a self-report measure for ACE, in particular focusing on parental care and abuse and meriting the application for both research and clinical work (Bifulco et al., 2005). Compared with the original CECA.Q3, the CECA.Q3-BF is a more practical assessment tool requiring less time and effort from depressed or hypomanic patients whose attention and concentration are usually compromised. It also saves time for interviewers and makes interviews more cost-effective, which will be beneficial for both clinical and research settings. The brief version not only uses less time to understand what ACEs patients have had but also helps diagnoses and projects prognosis of the diseases. In addition, the brief form was developed and validated in a clinical sample with mood disorders. Based on the wide-accepted association between childhood adversities and mental health issues, this population is more prone to be exposed to and more sensitive to early life adversities compared with the general population. A practical screening instrument with high sensitivity and specificity increases the recognition of childhood adversities and in turn, prevents secondary developments of mental disorders. It will also facilitate further exploration of the underlying mechanisms between childhood adversities and mood disorders. Finally, data-driven methods were used for the dimension deduction, which addresses the gap that the original tool was generated based on investigators’ clinical experience alone. As McLennan et al. (2020) suggested that issues, including limited item coverage, collapsing of items and response options, a simplistic scoring approach, and the lack of psychometric assessment, should be addressed in the questionnaires of measuring ACEs. Our study focused on the dimension deduction of existing items and the improvement of CECA.Q3’s feasibility, the strengths of the CECA.Q3 remained in this brief version. In other words, the CECA.Q3-BF has satisfactory reliability and validity as a self-report measure for ACE focusing on parental care and abuse.
We noticed some item discrepancies in the subscales when maternal and paternal adversities are evaluated separately, indicating that mother and father play different roles and emphasize different aspects in the children’s development, especially in early childhood. For example, in the CECA.Q3-BF, the retained items in Antipathy and Neglect for mother and father are similar, while the items in Psychological Abuse for father are much less and quite different from those for mother. Mothers may play a more critical role in psychological interactivities with children compared with fathers. Sex differences in the study sample may be another reason. As there were more female participants in the study, they may have a closer relationship with their mother when they were young.
However, there are several limitations to be noted. First, as this study was conducted in a clinical sample, the CECA.Q3-BF and the new cutoffs are only applicable to the clinical population with mental disorders. The results of dimension reduction analysis and thresholds for diagnosis may vary for the general population. Second, the sample size of this study was not large, which may affect the data analyses to detect correlations among items and reduce dimensions. The small sample size also limited the application of factor analyses to all the items in the CECA.Q3 simultaneously. Thus, the interpretation of the results should be cautious because the results were generated from analyses by subscale. Third, as this study was conducted in one single clinical setting in Montreal, Canada, the reliability and validity of the CECA.Q3-BF need to be further tested, including test–retest reliability, content validity, construct validity, across a variety of clinical settings with different prevalence of mood disorders and in a different sociocultural context. In addition, categorical principal component analyses failed to detect redundant items in the subscale Parental Loss, Support, Physical Abuse, and Sexual Abuse due to the potential reasons mentioned above. Also, open-ended questions, such as “please describe your experience,” were not able to be dealt with by quantitative methods. Focus group discussions with key informants can be held in the future to shorten those categorical subscales and detailed follow-up questions. Furthermore, McLennan and colleagues (2020) pointed out issues like lack of coverage on peer victimization, exposure to community violence, low socioeconomic status, poverty, and parent mental illness, and simple scoring system that assumes the weight of each item treated equally on the influence of outcomes are important to study ACEs. Because these issues were not covered in the CECA.Q3 and this study focused on the dimension deduction of existing items and the improvement of CECA.Q3’s feasibility, therefore we cannot address these issues. Finally, like the CECA.Q3 and all other retrospective measurement tools for childhood adversities, information collected using the CECA.Q3-BF is prone to recall and information bias. It is reported that retrospective reports are likely to underestimate the incidence of abuse/neglect (Hardt, & Rutter, 2004). Conclusions drawn from the retrospective recall of childhood adversities should be interpreted with caution.
Conclusion
Overall, the CECA.Q3-BF offers a briefer but accurate measurement of childhood adversities particularly focusing on parental care and abuse. Although the accuracy of this brief form needs to be replicated by other studies, it could facilitate the application of the CECA.Q3-BF in the clinical settings, as it significantly reduces the length of the interview and therefore has increased compliance from respondents. Future research on ACEs could use the CECA.Q3-BF as a start point to study childhood experiences on parental care and abuse and expand the item coverage of ACEs, such as peer victimization, exposure to community violence, low socioeconomic status, poverty, and parent mental illness, as needed.
Supplemental Material
sj-pdf-1-jiv-10.1177_0886260520933038 – Supplemental material for Development and Validation of a Brief Form of the Childhood Adversities Questionnaire Among a Population of Mood Disorders
Supplemental material, sj-pdf-1-jiv-10.1177_0886260520933038 for Development and Validation of a Brief Form of the Childhood Adversities Questionnaire Among a Population of Mood Disorders by Muzi Li, Tamara Cassis, Carl D’Arcy, Nancy Low and Xiangfei Meng in Journal of Interpersonal Violence
Supplemental Material
sj-pdf-2-jiv-10.1177_0886260520933038 – Supplemental material for Development and Validation of a Brief Form of the Childhood Adversities Questionnaire Among a Population of Mood Disorders
Supplemental material, sj-pdf-2-jiv-10.1177_0886260520933038 for Development and Validation of a Brief Form of the Childhood Adversities Questionnaire Among a Population of Mood Disorders by Muzi Li, Tamara Cassis, Carl D’Arcy, Nancy Low and Xiangfei Meng in Journal of Interpersonal Violence
Footnotes
Author Contributions
T.C. and N.L. conducted the data collection. M.L. conducted the data analysis and prepared the draft of this manuscript, with XM’s feedback on all steps of analysis, interpretation, and manuscript drafting. C.D. assisted with the interpretation of results. All authors contributed to the writing and editing of the manuscript and have approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by clinical research scholar awards to N.L. from the Research Institute of the McGill University Health Center (MUHC RI) and the Fonds du recherché du santé du Québec (FRSQ). X.M. received a scholar award from the Fonds de recherche du Québec-Sante, Canada, and research funds from the Canadian Institute of Health Research (CTP-79839, PJT-148845) and the Canada First Excellence Research Fund provided to McGill University for Healthy Brains for Healthy Lives.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.