
Abstract
Violence is a known driver of HIV vulnerability among transgender (trans) women, who are disproportionately impacted by HIV globally. Violence is also a barrier to accessing HIV prevention, treatment, and support. Yet, little is known about the everyday experiences of violence faced by trans women living with HIV, who live at the intersection of a marginalized gender identity and physical health condition. To address this gap, this study draws on semi-structured, individual interviews conducted 2017–2018 with a purposive sample (selected based on diverse identities) of trans women living with HIV (n = 11) participating in a large, community-based cohort study in three Canadian provinces. Framework analysis was used to identify key themes, patterns within themes between participants, and patterns across themes among participants. Findings showed that trans women living with HIV experience specific contexts of violence shaped at the intersection of stigma based on gender identity, gender expression, and HIV status, among other identities/experiences. Violence experienced in childhood (e.g., familial rejection, bullying) increased trans women’s likelihood of being exposed to a violent social context in young adulthood (e.g., state violence perpetuated by the police, interpersonal violence perpetuated by sexual partners, and community violence perpetuated by society-at-large/the general public), which increased trans women’s HIV vulnerability; once living with HIV trans women were subjected to discursive violence from healthcare providers. These multiple forms of violence have serious consequences for trans women living with HIV’s ongoing social, mental, and physical well-being. The findings suggest that interventions are urgently needed to reduce violence against trans women in childhood and young adulthood, in addition to reducing violence against trans women living with HIV perpetuated by healthcare providers in adulthood, to both proactively and responsively promote their safety, health, and well-being.
Keywords
Background
Violence against transgender (trans) women constitutes a global public health crisis (Reisner et al., 2016). Broadly speaking, trans is an umbrella term used to define a diverse group of people whose gender identities or expressions differ from those societally expected as associated with their sex labeled at-birth (Nuttbrock et al., 2015). Trans women specifically include those labeled male sex at-birth who typically identify as women, trans women, and/or transfeminine. Between 2008 and 2016, 165 trans people were killed in the United States alone (Wirtz et al., 2020). Moreover, trans women of color are disproportionately affected by violence, influenced by intersecting marginalization across gender and race (Dinno, 2017; King et al., 2019). For example, analyses drawing on data from Transgender Day of Remembrance and National Coalition of Anti-Violence Programs data found that homicide rates of Black and Latina trans women were higher than among Black and Latina cisgender (cis) persons (Dinno, 2017). Cis refers to those who experience congruence between their gender identity and sex labeled at-birth (e.g., those labeled female at-birth who identify as girls/women) (Bauer et al., 2009). Among all reported trans homicides 2010–2016, 70% were among Black trans women, and 23% among Latina trans women, compared with 3% among White trans women (Dinno, 2017).
Apart from extreme physical violence, multiple other types of violence have been documented among trans women in the United States and Canada. Data from the 2015 U.S. Transgender Survey (n = 27 715) reported past-year rates of being physically attacked (5%), verbally harassed by strangers (33%), and experiencing trans-related intimate partner violence (IPV) (e.g., being told one is not a “real” woman) (27%) (James et al., 2016). Among 2,873 trans and nonbinary people participating in the 2019 Trans PULSE Canada study, 68% of participants had experienced verbal harassment, 37% physical threats or intimidation, 16% physical violence, 42% sexual harassment, and 26% sexual assault, all related to being trans or nonbinary (Trans PULSE Canada Team, 2020). After experiencing violence, trans women may have little expectation of receiving appropriate intervention and support (Ritchie & Jones-Brown, 2017). Moreover, studies have shown that police may subject trans women to violence upon reporting (Du Mont et al., 2019; Lyons et al., 2017).
Violence has manifold negative physical and emotional consequences for trans women (Baral, Poteat, et al., 2013; Henry et al., 2018; Klemmer et al., 2018; Lacombe-Duncan et al., 2020; Peitzmeier et al., 2019; Shipherd et al., 2011; Wilson et al., 2013). Violence is both a driver of HIV vulnerability among trans women, who are disproportionately impacted by HIV globally (Baral, Poteat, et al., 2013), and a barrier to engagement in HIV care for trans women living with HIV (Wilson et al., 2013). For example, in a study conducted with Black trans women living with HIV (n=67), physical assault and IPV were negatively associated with viral suppression (Bukowski et al., 2018). Studies have shown long-term negative physical consequences of sexual assault among trans survivors, including physical scarring, chronic medical conditions, and disabilities (munson & Cook-Daniels, 2016).
With respect to mental health, data from the National Comorbidity Study showed approximately 51% of trans women experienced potentially traumatic events at least once during their lifetime (Shipherd et al., 2011). With the exception of experiencing a natural disaster, 13 of the 14 potentially traumatic events could be attributed, at least for some participants, to trans identity. For example, over one third of participants had experienced the sudden death of a loved one related to trans identity and one fifth had someone threaten to kill or hurt them or had been hit, beaten up, or badly hurt by a stranger, related to trans identity (Shipherd et al., 2011). In a study of the associations between IPV and mental health among trans and nonbinary people (n = 78), all types of IPV (sexual, psychological, physical, assault with injury) were associated with anxiety, and all but physical IPV were associated with depression (Henry et al., 2018). A Canadian national community-based research study found that almost three quarters of trans women with HIV (74.1%) had reported a history of violence in adulthood, which was associated with higher depressive symptom scores ( Lacombe-Duncan et al., 2020). Another Canadian-based study found that a history of transphobic assault was associated with greater drug use among trans persons (Scheim et al., 2017). Transphobic violence has been found to also be associated with suicidality among trans adults in Canada (Bauer et al., 2015).
These high rates of violence can be contextually understood as driven by social, cultural, and religious norms which denigrate trans, nonbinary (nonfeminine/masculine expressions of gender) as less than, prohibiting people from engaging authentically as themselves and trans women’s safety. Indeed, globally, trans people experience pervasive stigma and discrimination (Poteat et al., 2014). Stigma is perpetuated at a structural level through the institutionalization of discriminatory and exclusionary policies, at an interpersonal level through enacted stigma in interpersonal interactions, and at an individual level through internalized and/or felt normative stigma, whereby people adopt society’s negative attitudes toward them as their own and/or perceive that others hold negative attitudes toward them (White Hughto et al., 2015). Stigma, at least in part, explains the disproportionate experiences of violence among trans people, such as one study showing that trans college students had significantly higher odds of victimization compared with cis male or female students (Griner et al., 2017).
Trans stigma is hypothesized to influence HIV vulnerability through factors situated at multiple social ecological levels. For example, a lack of legal protections against firing a person based on gender identity may contribute to a lack of access to employment among trans women, which increases their economic insecurity and homelessness. Homelessness may expose trans women to multiple forms of violence, with consequent negative mental and physical health outcomes. Moreover, socioeconomic disparities can also contribute to engagement in sex work, a context where trans women also experience heightened exposure to violence which can increase HIV risk (Lyons et al., 2017; Poteat et al., 2014; Sevelius, 2013; Wirtz et al., 2020). For example, in a qualitative study conducted with 33 trans sex workers in Vancouver, Canada, participant narratives revealed how social and structural contexts of transphobia contributed to everyday experiences of transphobic violence in the context of sex work, fueled by clients’ discovery of a participants’ gender identity, and resultant negative police responses (Lyons et al., 2017). IPV is also a well-documented driver of HIV vulnerability among cis women, as well, with several proposed mechanisms (e.g., lack of safety to ask partners to use condoms, fear of partners’ response to being asked about safer sex, and abuse perpetrated in response to a woman being asked about safer sex) (Heintz & Melendez, 2006).
The combination of intersectional, social ecological, and life course perspectives may contribute to an in-depth understanding of violence against trans women living with HIV. Despite some growing literature in relation to trans stigma and HIV stigma, resultant violence, and HIV and mental health vulnerability, there is a limited understanding of the experiences of trans women living with HIV, who experience intersecting forms of marginalization (Lacombe-Duncan, 2016; Logie et al., 2012). Prior research has predominantly focused on the association between violence and HIV vulnerability, but not on the impact of violence in the lives of trans women who have been diagnosed with HIV, despite that it is a barrier to access to HIV and other types of health care (Wilson et al., 2013). Moreover, much of the research focuses on IPV, not on other types of violence perpetrated against trans women.
The social ecological model, emerging from the work of Bronfenbrenner (1979), has been used to understand the relationships among the multiple and interacting individual, social, and structural factors. Ecological theory emerged from systems thinking and a recognition of the interdependence of people and their environment (Bronfenbrenner, 1979; Gitterman & Germain, 2008). Since Bronfenbrenner’s (1979) initial conceptualization of an Ecological Model of Human Development, several scholars have applied the theory to various HIV topics, particularly contexts of HIV exposure (Baral, Logie, et al., 2013; Poundstone et al., 2004), but also the health and well-being of trans youth and adults (Newman et al., 2013; Newman & Fantus, 2015; White Hughto et al., 2015) as well as in explaining HIV health care access (Berben et al., 2012; Castro et al., 2015). As such, social ecological perspectives can be used, in conjunction with an intersectional approach, to explore the multilevel factors influencing experiences of violence against trans women living with HIV.
Finally, beyond the importance of exploring a multilevel and intersectional environment, another important consideration is that violence takes different forms and has different consequences across the life course, both for people living with HIV (Ruark et al., 2016) and trans people (Nuttbrock et al., 2010). Yoshihama et al. (2006) utilized a life course perspective within a social ecological approach, to understand the way that time impacts the complex relationships among multiple and interacting intrapersonal, interpersonal, organizational, and structural factors in the context of intimate partner violence, welfare receipt, and health status of low-income African American women. As such, a life course perspective has been previously applied to understand the association between interpersonal violence and poor social and health outcomes (Yoshihama et al., 2006), as well as HIV vulnerability (Ruark et al., 2016). Scholars have previously explored the impacts over the life course of sexual stigma on HIV vulnerability (Moore et al., 2019) and transphobic violence on depression (Nuttbrock et al., 2010, 2012). However, a comprehensive understanding of experiences of violence across the life course for trans women living with HIV has not been described. Taking all this together, the aim of this article is to understand the context, types, and consequences of violence experienced by trans women with HIV across the life course, from intersectional and social ecological perspectives.
Method
Data Source
This qualitative study is embedded within the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS), a multiprovince (Ontario, Quebec, British Columbia), community-based participatory research (CBPR) cohort built and delivered through meaningful involvement of women living with HIV, and focused on health resource utilization and health outcomes among women living with HIV (n = 1,422; n = 54 trans women) (Loutfy et al., 2017). For the overarching CHIWOS study, Peer Research Associates (PRAs) recruited women living with HIV aged 16 years or older through word-of-mouth via multiple mechanisms (e.g., PRA networks, online). Venue-based sampling was also utilized whereby women were recruited from AIDS service organizations, HIV clinics, and community-based organizations. Community Advisory Boards (CABs) were formed to enhance targeted recruitment of women overrepresented in Canada’s HIV epidemic, including a trans-specific national-level CAB (Trans CAB), a group of trans people and cis allies from the CHIWOS team interested in trans health. Consistent with CHIWOS’ approach to CPBR, the primary author (ALD) engaged from the outset with trans community members to understand community needs and to increase the potential impact of this research (Israel et al., 1998; Loutfy et al., 2016; Travers et al., 2013). Specifically, community members reviewed the project proposal and met with ALD regularly throughout the entire research process, providing input on the study focus, participant recruitment, data collection materials (e.g., interview guide), and interpretation of the study findings.
Sample
For this study, a subset of trans women living with HIV (n = 11) who completed the baseline CHIWOS survey (2013–2015) participated in an open-ended, semi-structured, individual interview focused on their experiences accessing different types of health care (HIV, gender-affirming), with particular attention paid to how their social context, including experiences of violence, impacted their access to care. Interviews were conducted between May 2017 and March 2018.
Consistent with an intersectional approach that recognizes the inadequacy of using one source of oppression (e.g., trans identity) as the singular cause of health inequity (Dhamoon & Hankivsky, 2011), participants were purposively chosen to reflect various identities, including those highlighted in the literature as experiencing pervasive violence (e.g., trans women of color living with HIV) and those identified by the CHIWOS Trans CAB as understudied in a Canadian context (e.g., trans women living with HIV who are sex workers). The sample included trans women living with HIV (n = 11) from Vancouver (n = 3), Montreal (n = 3), and Toronto (n = 5). Participants ranged in age from their 20s to 60s (n = 1 20s, n = 4 30s, n = 3 40s, n = 2 50s, and n = 1 60s). Fewer than half were White (n = 4), with the remaining participants identifying as Indigenous (n = 3), Latina (n = 2), Black/African/Caribbean (n =1), and multiple races/multiracial (n = 1). The majority of women had been living with HIV for over 14 years (n = 8), with a few living with HIV for between 6 and 14 years (n = 3).
Procedure
In each setting, a PRA or the local CHIWOS coordinator made first contact with potential participants using a recruitment script. Prior to the interview, participants were made aware of the purpose of the research, as well as some characteristics of the interviewer. For 10 of the 11 interviews, following an indication of interest and permission, participant contact information was passed onto ALD, a PhD-trained researcher and Master of Social Work (MSW)-trained clinician, to set up and conduct an interview. For one of the 11 interviews, the interview was both set up and conducted by a PRA who was trained in qualitative data collection and research ethics and who had a preexisting relationship with a participant group with historically negative experiences with research (Indigenous trans women living with HIV). Only one participant contacted did not respond to a request for an interview.
The interviews ranged from 25 to 100 minutes and were conducted in private settings (e.g., participant’s home) to maximize participant comfort discussing sensitive topics with only the interviewer and participant present. A guide describing local trans-friendly resources (e.g., HIV service organizations, physical and mental health supports, community centers) was offered to each participant after their interview. The semi-structured interview guide was developed iteratively in partnership with the CHIWOS Trans CAB, pilot-tested and refined as appropriate. Interviews were recorded and transcribed verbatim. Notes were also taken before each interview about ALD’s a priori assumptions and after each interview about ALD’s initial interpretations. These notes were later used during the analysis phase whereby ALD reflected on how these a priori assumptions and initial interpretations shaped the interview itself and the data analysis. All participants provided written informed consent prior to participating in the interview. Specifically, ALD or the PRA read the consent form to the participant, invited the participant to ask questions about the consent form, and provided time for the participant to think about the consent form and discuss any concerns prior to signing. Ethics approval for this qualitative substudy, conducted in partial fulfillment of the requirements for the degree of Doctor of Philosophy of ALD, was received from the University of Toronto and Simon Fraser University/University of British Columbia/Providence Health.
Data Analysis
Framework analysis was used, a form of qualitative content analysis (QCA) that has become increasingly popular in health research (Gale et al., 2013; Ritchie & Spencer, 1994). QCA allows for the interpretation of the content of textual data through a systematic process of coding and identifying themes (Hsieh & Shannon, 2005). Framework analysis is a flexible approach, combining inductive (open) and deductive (framework) coding (Bradley et al., 2007; Gale et al., 2013). The analysis involves a series of six steps from familiarization with the data at the initial stage through to mapping and interpretation at the final step (Ritchie & Spencer, 1994). These six steps were taken by ALD: (a) familiarization with the data as a whole; (b) development of the analytic framework, involving line-by-line open coding of three interviews (one from each province), an inductive approach (Kondracki et al., 2002); (c) continued development of the analytic framework, involving returning to the original research questions and interview guide to expand the code list, combining codes into a preliminary analytic framework organized thematically, developing a code book with descriptions of each code, testing the analytic framework on three more interviews, and revising the analytic framework to account for new insights; (d) indexing each of the 11 transcripts in NVivo 11.4.0 (QSR International Pty Ltd., 2012), a systematic process of applying the analytic framework to textual data (line-by-line coding, using a deductive approach); (e) charting data into framework matrices, defined as a table with numerous cells that summarize the data by codes (columns) and participants (rows), allowing for both data reduction (summarizing participant perspectives by theme/code) as well as keeping each participant’s narrative intact through a summary of their story across themes; and (f) mapping and interpretation, involving reviewing the charting and writing a summary description of the data and noting trends and negative cases within themes and subthemes as well as across participants. The charting and summary data were reviewed by ALD’s doctoral supervisor and a member of the Trans CAB. Although transcripts and notes were not returned to individual interview participants due to feasibility (time and funding limitations) (traditional member checking), the trans members of the CHIWOS Trans CAB provided debriefing and interpretation of findings, a type of member checking involving data interpretation by people with a shared experience to the participants (Barusch et al., 2011).
Findings
Findings showed that trans women living with HIV experience specific contexts of violence shaped at the intersection of stigma based on gender identity, gender expression, and HIV status, among other aspects of their identities/experiences. Moreover, findings showed the salience of specific forms of stigma (e.g., trans stigma, HIV stigma) at particular points in trans women’s lives. Familial rejection related to trans identity and gender nonconformity and other adverse childhood experiences increased trans women’s likelihood of being exposed to a violent social context in young adulthood influenced by intersecting identities. Specifically, trans women experienced state violence perpetuated by the police, interpersonal violence perpetuated by sexual partners, and community violence perpetuated by society-at-large/the general public, which increased their HIV vulnerability. Once living with HIV trans women was subjected to discursive violence from health care providers, primarily related to HIV status and trans identity. These multiple forms of violence had serious consequences for trans women living with HIV’s ongoing social, mental, and physical well-being. Figure 1, developed from the data, visually depicts the findings.
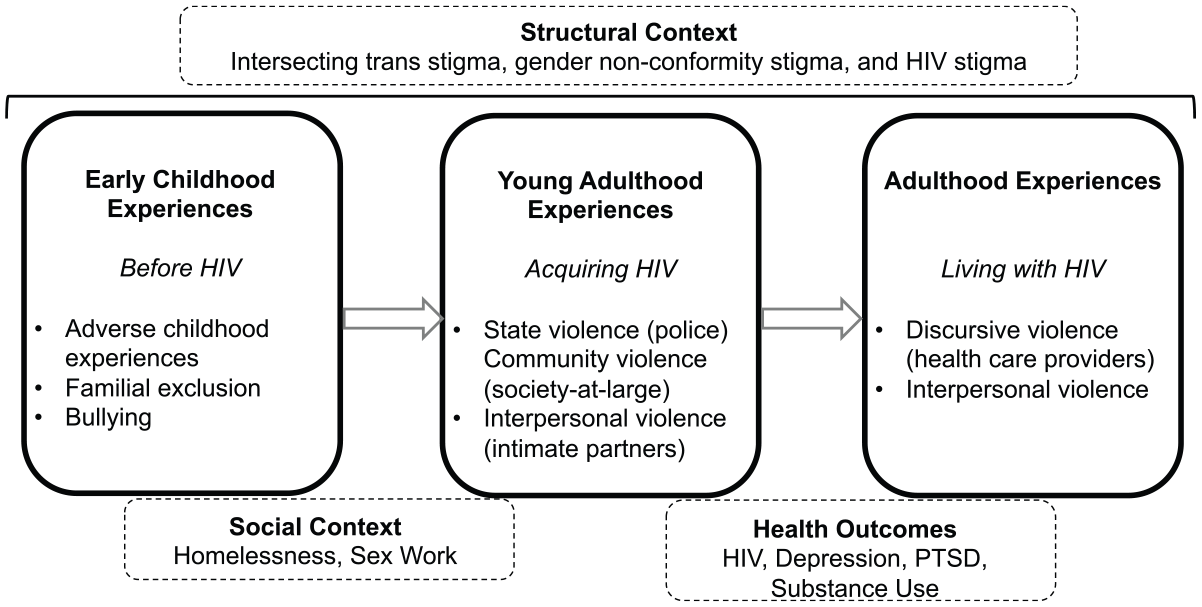
Context, types, and consequences of violence across the life course among trans women living with HIV.
Childhood Before HIV: Familial Rejection and Other Adverse Experiences
Participant narratives revealed multiple early experiences of familial rejection and bullying related to trans identity and gender nonconformity, and a general lack of access to safety in their childhood. Challenges in early childhood included parental substance use issues, “I also have lots of addiction in my family” (Participant 7) and mental health issues, “I used to live with her [my mom] only because she had severe mental health issues” (Participant 4). Some adverse childhood experiences were tied closely to trans and/or gender nonconformity stigma, including abuse, neglect, and homelessness, “You know my Mom kicked me out . . . Because I was trans” (Participant 1), resulting in additional challenges with internalized trans stigma, “I mean I struggled a lot with my identity in and out of the group homes and foster homes” (Participant 5).
Young Adulthood Before HIV: State, Community, and Interpersonal Violence and HIV Vulnerability
As a result of adverse childhood experiences, the majority of participants had some period of homelessness early in their transition. During young adulthood, other forms of marginalization (e.g., trans stigma and xenophobia contributing to a lack of access to employment) compounded challenges of staying housed: “I was already a refugee and I haven’t a permit for work so I try to, to keep my apartment but it was difficult. Didn’t know the language, nobody give me a job because I was a trans” (Participant 1). Further with respect to employment challenges, trans women experienced enacted trans stigma (difficulty accessing employment due to discrimination), anticipated trans stigma (fear of going outside during the day), and internalized trans stigma (general discomfort with physical appearance), contributing to sex work being one of the only options for employment: So, my transitioning, it started in the sex work domain. Because back then it was still very difficult for us to find a job and besides, I was trying to get rid of my masculinity, my testosterone that it couldn’t let me be free to go outside during the day. (Participant 11)
Sex work in and of itself, as well as violence from sex work, brought participants into frequent contact with police. These interactions were most often negative, and characterized by police targeting trans women due to their engagement in sex work, “So I chatted with him for a few minutes, and named a price and I hopped in the car and he drove off and in two minutes he reached into his pocket flashing his badge, undercover” (Participant 3) and/or disregarding their concerns, “Even if you tell the police they don’t always help . . . they treat you like you’re the problem” (Participant 2). Participants described not only having their concerns disregarded by police, as exemplified in Participant 2’s quote, but they also experienced physical and verbal violence from police in the context of sex work: And back then we used to work on the streets as well, so the police was very hard on myself. Before, I didn’t have any trouble with the police, so when they start hitting me and insulting me and stuff, I defend myself very much, because for me the police was something more than treating me badly. (Participant 11)
The words “something more than treating me badly” were Participant 11’s way of describing police violence as punishment for not only sex work engagement but also her identity as a trans sex worker. Trans women also perceived that they were being targeted by police outside of the context of they, themselves, engaging in sex work, due to police assumptions of their involvement in sex work: I was living close to the street where there were plenty of transsexual prostitution. At this moment, I no more do prostitution. And I go to a theatre, not a cinema. And I was classy and things like that, sexy, classy. And the police follow me because maybe I was looking a bit, I’m a transsexual. They follow me until I am in my house. (Participant 9)
The participants also noted that they experienced physical violence, primarily from strangers and sex work clients. Violence was experienced in relation to both trans identity and gender expression. As Participant 1 described, “Even I got shot on the street because a guy found out I was trans and not female-female.” Participant 6 further elaborated on the impact of gender expression, and in particular, gender-conformity, to her safety: I’ve been violated so many times because I was not passable, I guess to society’s eye, you know what I’m saying? So, if one is not passable, then society can be quite cruel . . . (Participant 6)
Sexual violence, and in particular rape, was also perpetuated by both strangers and sex work clients, heightened in contexts of homelessness and street-based sex work. For two participants, rape led to their HIV acquisition. As Participant 1 describes, “But I was raped. So and I think one of the guys who did it was infected. And that rape was brutal to me.” Participant 6 described a physical altercation during sex work negotiation: . . . So, I was in a daze from him talking to me like that, he went around to the driver . . . to the passenger side, opened the door and sprayed something in my face and my eyes. My eyes, I couldn’t open them, they were burning. My nose, I couldn’t breathe, my mouth . . . (Participant 6)
Later, she further described the following scenario: I went in there . . . well, I had a bad date, he had stabbed me a half inch away from my kidney with a butcher knife. Raped me. (Participant 6)
Even in the absence of personally experience physical violence, participants were palpably aware of the risk of violence they faced: As a trans woman we are the most highly murdered of any gender. We have like 70% chance of being murdered because of our gender without anything else. And when we are murdered it’s very violent usually, like stabbed 70, 80, 90 times. (Participant 3)
Participant 3’s quote highlights transmisogyny, stigma against trans women whereby they are ridiculed, dismissed, and violated not only for their defiance of gender norms, but specifically due to expressions of femaleness or femininity (Serano, 2007). Participants were also accustomed to experiencing violence in everyday interactions from the general public/society-at-large due sometimes to their trans identity (Participant 11 and Participant 1) and other times in relation to multiple identities (Participant 3): I got into the plane and there was this guy sitting next to where I was sitting. And he said something in French that he probably believed that I couldn’t understand, but I understood when I went to the bathroom. So, when I come back from the bathroom I told him, listen it’s [my trans identity] not contagious what I have and you are not stick with me. (Participant 11) And she [a woman on the subway] look at me and she says, “Oh I know you a man. Oh I know.” She didn’t even say trans. She said man. (Participant 1) I was at [X intersection] one night . . . And one guy behind he says to his friend, oh that one in front of us used to be a man and she’s HIV positive. I just turned around like that and I looked at him and I said you know what, you’re 100% right. And let me tell you something, I’m more of a woman than you’ll ever be able to handle in your life but I said I’m still more of a man than you’ll ever be so keep your fucking comments to yourself. (Participant 3)
Adulthood Living With HIV: Discursive Violence in Health care and Negative Social, Physical, and Behavioral Health Consequences
After gaining access to services to address experiences of violence, trans women living with HIV described being subjected to additional violence at the hands of health care providers: Oh yeah, I’ve been called male, oh that men. I have been called male. I say don’t call me that. Don’t call me man, don’t call me man. I’m a miss. And one of the nurses, sometimes the nurses they would address, a couple of times, the other nurses, and even in a lab, to get your blood work. (Participant 2) They treat you different. They start treating me different. They don’t want to touch me. They ask me all the time do you want a female or a man. In that tone, like, you know. (Participant 1)
At times, participants were unable to identify the type of stigma manifesting in the interaction, demonstrating the intersection of multiple stigmas. For example, Participant 10 described the following encounter in an emergency room: I went to emergency room. Oh my god yeah, I’m not sure if it was my [HIV] status or gender or whatever but obviously at the time I only had my . . . I had to use my decision/notice of decision for my status at [place of employment] and that had my birth name on it. Between that and doctor resident looking, they just became completely phobic and it was so crazy, they’re like oh yeah I’m coming back and it was like every few seconds a new nurse or someone would come into the room and look . . .
Many participants highlighted trauma, depression, and substance use in response to daily marginalizing conditions, including a continued lack of access to the social determinants of health and violence. Trans stigma and now HIV stigma were pervasive barriers to seeking and maintaining employment. As Participant 3 stated, And she said, I don’t know how my husband will . . . if he wants you or not [because of your HIV status]. She said I don’t even know how comfortable I am with you making me a sandwich.
Substance use was often described as occurring in response to contexts of discrimination. Moreover, participants expressed difficulty ceasing drug use when faced with continuous stressors of daily life: I recently had quit using illicit drugs and that was something that was a part of my life for the better part of like over 10 years. So it was very hard to let go of, you know, the escape, reality, and just how light it made me feel. It took away the burden. (Participant 4) I stayed clean for four and a half years. And then my mom was on her deathbed and I managed to stay clean nine months, and then all hell broke loose, I lost it, I lost it. (Participant 6)
Participants also described having depression; as Participant 2 described, “I have slight depression but I have . . . I’ve been 30 years, over 30 years in my condition . . .,” characterized by fatigue (Participant 2) and shame (Participant 4). Finally, multiple participants were aware of the traumatizing conditions and the impact of this on their mental health, which was also notable during the interview itself: I’ve had a lot of trauma done, a lot of trauma done to my head, just . . . And now I’m still . . . I’m really, really starting to get emotional right now . . . I’ll get all teary-eyed and then I’ll just go into a darker place and I don’t want to go there, not today. (Participant 6)
Moreover, as exemplified in the following two quotes, both trauma and depression exacerbated social isolation for trans women living with HIV: I’m just becoming reclusive. It’s this weird, it’s just . . . see I start going into a trance that’s what happens to me right now. I don’t know what’s something happened to me. It could be a trauma I don’t know what it is. (Participant 2) Sometimes when I’m feeling crappy I don’t want to talk to anybody. (Participant 3)
Discussion
Trans women experience multiple types of violence, across multiple contexts, with resultant negative consequences for their social, physical, and emotional well-being (Figure 1). Most importantly, findings suggested that violence is experienced differentially at different points in trans women’s life course and HIV trajectories, which may inform several specific violence reduction strategies. Furthermore, findings demonstrated how trans women’s lives are shaped first by intersecting trans and gender nonconformity stigma operating at structural, interpersonal, and intrapersonal levels, which increases exposure to contexts of violence, social isolation, and socioeconomic deprivation, and ultimately increases the risk of HIV acquisition. Subsequently, trans women living with HIV experience intersecting trans, gender nonconformity, and HIV stigma, among other forms of marginalization similarly operating at structural, interpersonal, and intrapersonal levels. The pervasiveness of intersecting stigmas in the lives of trans women living with HIV has been well-documented (Logie et al., 2012, 2017).
This study compliments quantitative studies documenting social and economic disadvantage of trans women living with HIV relative to cis people living with HIV (Denson et al., 2017; Dowshen et al., 2016; Mizuno et al., 2015) by documenting how intersecting stigmas may directly contribute to severe depression, trauma, and substance use or indirectly contribute to these individual level experiences through social isolation (Logie et al., 2012). The findings of the present study suggest that addressing the manifestation of intersecting stigma—violence—at multiple levels and across multiple contexts, may have an impact on HIV prevention among trans women, broadly, in addition to increasing access to care among trans women living with HIV and promoting their overall well-being.
Implications for Practice
Multilevel implications for practice can be mapped onto the findings (Figure 2). First, overarching implications are noted at structural, interpersonal, and intrapersonal levels. Structurally, human rights protections on the basis of gender identity and gender expression are necessary for the protections of the health and human rights of trans women. Although Canada has been a leader in advancing the rights of sexual minority populations (Government of Canada, 2017), the rights of trans people have lagged behind. Gender identity and expression were only recently added as prohibited grounds of discrimination to the Canadian Human Rights Act in 2017, although various provincial and territorial protections previously existed and trans people were already often protected under the grounds of sex. Studies have shown that these laws have downstream positive impacts on mental health and well-being of trans people. For example, Blosnich et al. (2016) utilized Veterans Administration Data to explore whether indicators of community- and state-level lesbian, gay, bisexual, and transgender (LGBT) equality were associated with trans veterans’ mental health, finding that employment nondiscrimination protection was associated with a 26% decreased odds of mood disorders and 43% decreased odds of self-directed violence.
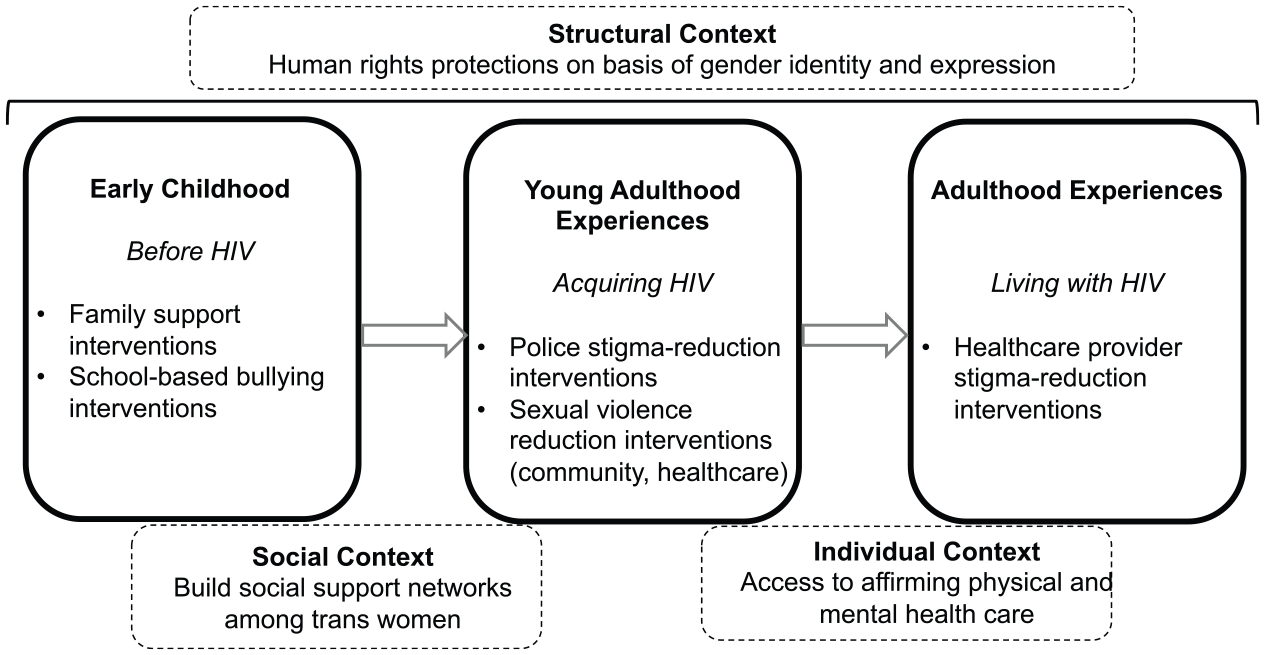
Implications for multilevel violence reduction strategies across the life course.
At a social level, interventions that increase social support are needed to reduce exposure to violence, as well as to mitigate the negative effects on trans women’s mental health (Nemoto et al., 2011; Pinto et al., 2008). A qualitative study conducted with 20 trans women elucidated the myriad of ways that social networks among trans women of color resulted in increased access to resources for daily living, as well as increased advocacy at a structural level (Pinto et al., 2008). A quantitative study exploring depression among trans women sex workers (n = 573) found that satisfaction with social support was significantly associated with lower rates of depression (Nemoto et al., 2011). Importantly, gender-based violence interventions must attend to the specific experiences of trans women, including trans women who experience intersecting forms of marginalization (e.g., trans women living with HIV, trans women who are sex workers).
At an individual level, mental health counseling from an affirmative and intersectional lens may reduce internalized stigma among trans women, and among trans women living with HIV (Puckett & Levitt, 2015). Klemmer et al. (2018) found that body satisfaction mediated the association between transphobia-based victimization and anxiety and depression. Clinical interventions that promote body satisfaction may also prevent negative mental health outcomes. Moreover, gender-affirming HIV care may promote HIV care engagement among trans women (Rebchook et al., 2017). However, the importance of addressing upstream determinants of violence cannot be understated.
With respect to temporally specific interventions, the study findings call for specific interventions in early childhood (e.g., family support interventions, school based-bullying reduction interventions). Familial rejection contributes to internalized stigma and sexual risk practices (Moore et al., 2019). Other studies have documented early experiences of familial rejection among lesbian, gay, bisexual, transgender, and queer (LGBTQ) people, in addition to pervasive school-based bullying and early experiences of sexual violence (Juárez-Chávez et al., 2018). These studies have called for interventions with parents to address sexual and gender diversity (Juárez-Chávez et al., 2018). In early adulthood, apart from a significant need for employment and education support programs that facilitate trans women’s entry into the workforce, there is a need for strategies to reduce violence perpetuated by police, given that the police are the primary source of potential support after experiencing violence. Health care settings must also learn strategies for affirmative sexual violence screening and intervention (Du Mont et al., 2019).
Sexual violence against trans women is a critical public health concern, as a known contributor to HIV vulnerability among cis and trans women alike (Logie et al., 2017). Although health care environments have been found to be stigmatizing for trans women broadly, trans women living with HIV in this study were exposed to discursive violence from health care providers not only on the basis of their gender identity or expression but based on their HIV status. Strategies are needed, such as health care provider stigma-reduction interventions, that reduce provider-level stigmatization of trans women living with HIV.
Importantly, the findings of the present study suggest that trauma-informed care may be a salient model of care for services supporting trans women living with HIV (Elliott et al., 2005). Many of the principles of trauma-informed care (e.g., create a positive relational collaboration and an environment of safety, respect and acceptance) are well-aligned with trans women living with HIV’s needs as identified and desires as self-described in the current study (Elliott et al., 2005).
Most importantly, strategies for violence reduction must not only take into account the perspectives of trans women, including trans women living with HIV, but should be led by trans communities. This strategy is consistent with an empowerment intervention approach, described as “a social process for people to gain mastery over their lives and the lives of their communities” (Glanz et al., 2008, p. 294). The overarching modality entails affected communities developing skills, knowledge, and confidence in their abilities to solve problems they encounter. As the case is in other places, existing trans community organizations and networks systems should be supported to create resilience and accelerate community-led social change that they desire (Kubicek et al., 2013).
This study has potential for informing policy in the areas of interventions that tackle violence against trans women as a public health menace that it is. Such policy should exercise zero tolerance toward all forms of violence against trans women at all levels and provide them with opportunities that are seen to be empowering. Such policies should focus on reducing discrimination and stigma that are more structural, human rights protections, and address the social determinants of health.
Through our analysis we identified differences in how women described violence at different points in their lives. However, exploring a life course perspective was not the primary goal of the study at study outset. Future studies should use robust methodologies, such as life chart intervention (Nuttbrock et al., 2010, 2012) with more participants, to more holistically examine complex interactions between stigma, violence, and health outcomes for trans women living with HIV. Given that this study was conducted in partial fulfillment of ALD’s doctoral degree, the majority of the analysis was conducted by her solely. Although some scholars suggest that multiple coders enhance demonstrated reliability for semi-structured research, others have suggested it keeps the analysis superficial (Morse, 2015). As such, the combination of lone-working with review of an earlier stage of the analysis by ALD’s doctoral supervisor and a member of the Trans CAB may have promoted a balance between rigor and depth. Although intersectional findings were emphasized, some participant narratives were focused on experiences of violence related to one identity (e.g., trans stigma, HIV stigma, or sex work stigma), consistent with a unidimensional rather than intersectional approach. This phenomenon is consistent with social science research suggesting that characteristics most salient to one’s personal identity are most susceptible to stigma and other threats (Thoits, 2013). Thus, participants may have been most likely to speak about violence in response to the identity that most closely affected their sense of self. These findings further underscore the importance of developing intersectional interventions that can holistically address the multifaceted experiences of diverse trans women living with HIV across race, sex work engagement, and socioeconomic status, among other facets of identity and experience that are most important to them.
Conclusion
The body of literature on trans women living with HIV has increased. However, there is still a wide gap. This qualitative study showed the multilevel, intersecting factors that contribute to violence against trans women, and how this violence influences, and is influenced by, HIV. These factors, including familial and state violence, stigma and discrimination, lack of recognition and respect for their affirmed gender, and exclusion from employment and educational opportunities, must be addressed to promote holistic well-being and to reduce HIV disparities among trans women. Moreover, interventions that address intersecting identities and experiences and that consider trans women’s experiences across the life course may be most helpful at mitigating violence and the resultant negative consequences.
Footnotes
Acknowledgements
The authors acknowledge the participants of the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS). The authors also wish to acknowledge the administrative and recruitment support of the CHIWOS co-principal investigators Dr. Mona Loutfy, Dr. Angela Kaida, and Dr. Alexandra De Pokomandy; provincial coordinators Angela Underhill, Rebecca Gormley, Karène Proulx-Boucher, and Yasmeen Persad; and the entire Peer Research Associate Team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Social Science and Humanities Research Council (SSHRC) Doctoral Fellowship.