
Abstract
Intimate partner violence (IPV) is a widespread social problem affecting all populations regardless of gender, race, and socioeconomic status. The aims of this study were to examine (a) patterns of IPV among Pacific women living in New Zealand and (b) the risk and protective factors associated with IPV perpetration and victimization. As part of the longitudinal Pacific Islands Families (PIF) Study, maternal interviews, which included reports about IPV, acculturation, and sociodemographic characteristics, were administered at phases 6 weeks, 2, 6, 11, and 14 years postpartum. Age had a significant effect on perpetration of both minor and severe perpetration of IPV, and on being a victim of minor IPV. However, no significant effect was found for severe victimization. Cultural alignment also had a significant effect on perpetration of IPV with Pacific mothers who were strongly aligned to their traditional Pacific culture being significantly less likely to report minor or severe IPV perpetration compared with Pacific mothers who were closely aligned to western culture. Single mothers reported significantly more minor victimization, and those mothers who were more highly educated and were in a higher income bracket were significantly less likely to report severe physical IPV victimization. These findings can inform the timing and targeting of culturally appropriate violence prevention efforts in adolescence and young adulthood that focus on the development of healthy intimate partner relationships and effective methods of conflict resolution.
Introduction
Intimate partner violence (IPV) is described as behavior by an intimate partner that causes physical, sexual, or psychological harm. IPV is a major social problem affecting all populations regardless of gender, race, and socioeconomic status (Cho, 2012; Stewart et al., 2013) and is an important target for prevention and intervention (World Health Organization [WHO], 2013). The overwhelming global burden of IPV is mainly borne by women, with approximately 30% of women experiencing sexual or physical violence (WHO, 2013). IPV poses a significant health risk for women in New Zealand, particularly among women from select ethnic groups whose experience of social inequity may contribute to high rates of IPV (Ministry of Health, 2000), including those from the Pacific Islands who are living in New Zealand (Paterson et al., 2007).
The Pacific population living in New Zealand is ethnically heterogeneous (Samoan, 49%; Cook Islands Māori, 21%; Tongan, 20%; and Niuean, 8%), rapidly growing, youthful, and highly urbanized (Statistics New Zealand, 2013). Waves of migration to New Zealand took place in the 1950s and 1980s when Pacific people arrived from the Pacific islands of Samoa, Tonga, Cook Islands, Niue, Fiji, and the Tokelau’s. Since these migration waves, Pacific people have actively participated in the New Zealand economy and have significant social, sporting, and cultural links across New Zealand society (Sang & Ward, 2006). However, it has been well documented that compared with the general population, Pacific people living in New Zealand have higher rates of unemployment (Statistics New Zealand, 2013), lower personal and household incomes (Perry, 2014), and higher rates of poverty (Boston & Chapple, 2014).
Background
Social disadvantage has been associated with higher rates of IPV (Fanslow & Gulliver, 2015; Fulu et al., 2013) with rates of IPV tending to be higher among couples exposed to various forms of economic adversity and hardship (Bassuk et al., 2006; Cunradi et al., 2002). Low maternal education is also a significant risk factor for women being victims of IPV (Heise, 2012; Vyas & Watts, 2008). Studies have shown that having at least a secondary education is protective against the risk of IPV victimization for women (Vyas & Watts, 2008). A large World Health Organization (WHO) study revealed that the risk of IPV was reduced among couples where at least one partner had completed secondary education (Garcia-Moreno et al., 2003). In addition, single marital status (DeMaris et al., 2003) has been linked to high rates of IPV. It has been suggested that the more marginalized members of immigrant society are likely to lack the social supports that mitigate against verbal and physical aggression (Felmlee, 2001; Paterson et al., 2007).
Research in the Pacific Islands reveals that the prevalence of IPV and other types of violence is higher than the global average of 35%. For example, the rate of lifetime experience of violence is high in Tonga (79%), Samoa (76%), Fiji (72%), and Vanuatu (72%). It is suggested that IPV is deeply embedded in Pacific social and cultural values (Ministry of Social Development, 2012), with some researchers proposing that family violence may be considered normal, or at least acceptable in Pacific culture (Counts, 1990). It is likely that a lack of ties with both the culture of the homeland and the adopted country may lead to increased stress and conflict and result in increased IPV (Borrows et al., 2011; Caetano et al., 2000; Garcia et al., 2004).
Several longitudinal investigations have examined age-related patterns of IPV perpetration and have found that perpetration peaks in the early twenties and declines during the latter half of the twenties (Fritz & O’Leary, 2004; Johnson et al., 2015). In contrast to these findings, other researchers have found that perpetration of IPV is relatively stable over time (Capaldi et al., 2003; Fritz & Slep, 2009), or has increased over time (Orphinas et al., 2013; Swartout et al., 2012). However, some time-stable characteristics and contexts to patterns of IPV, such as race/ethnicity and family structure, have been found by researchers (Halpern et al., 2001; Vezina & Herbert, 2007).
Understanding violence between intimate partners is multifaceted and various sociocultural theories have been put forward to comprehend this phenomenon (Bell & Naugle, 2008). Power theorists argue that the roots of violence stem not only from within the culture but also from within the family structure (Straus, 1976). Family conflict, social acceptance of violence, and gender inequality are hypothesized to interact and lead to family violence. The use of violence to resolve family conflicts is believed to be learned in childhood by either witnessing or experiencing physical abuse (Straus, 1977).
This article examines (a) patterns of IPV among Pacific women living in New Zealand over a 14-year period, and (b) the risk and protective factors associated with IPV perpetration and victimization across this time period.
Method
Participants
The Pacific Islands Families (PIF) Study is following a birth cohort of Pacific children born in Auckland, New Zealand in 2000 and their parents. All potential participants from one hospital were selected from births where at least one parent identified as being of a Pacific ethnicity and was a New Zealand permanent resident. Therefore, a small number of mothers in the cohort are non-Pacific. Mothers were approached in the hospital and gave consent to be visited when the child was 6 weeks of age to discuss participation in the study. If the mother agreed to participate in this Pacific longitudinal study, then full informed consent and all ethical procedures were carried out and the mother and child were enrolled in the PIF Study. The original cohort included 1,376 mothers of 1,398 Pacific infants (including 44 twins). Compared with data available from Statistics New Zealand’s 1996 and 2001 censuses, the inception cohort was broadly representative of the Pacific census figures (Paterson et al., 2008).
Procedures
At phases 6 weeks, 2, 4, 6, 9, 11, 14, and 17 years postpartum, individual interviews were carried out by Pacific research staff with the mothers in their homes. Once informed consent was obtained, an interview concerning child and family functioning and their personal health and lifestyle took place. Within the context of the wider interview, at ages 6 weeks, 2, 6, and 14 years postpartum we included a measure of measured IPV. In this current IPV study, there were 806 mothers. This was based on mothers who had participated in all those phases and who had completed the IPV questionnaire. Further details of recruitment and procedures are available elsewhere (Paterson et al., 2008).
Measures
IPV
Form R of the Conflict Tactics Scale (CTS) developed by Straus (1979) was used to measure IPV. First, mothers reported on their behavior toward their partner (perpetration), and second, they reported about their partner’s behavior toward them (victimization). The CTS measure produces four binary outcomes (Straus, 1979). Perpetration or victimization of minor physical violence refers to slapping, pushing, grabbing or shoving, or throwing something at their partner. Perpetration or victimization of severe physical violence is defined as kicking, biting or hitting their partner with a fist, hitting their partner with something else, beating their partner up, choking their partner, threatening them with a knife or gun, and using a knife or gun against their partner. A mother was considered a perpetrator of minor or severe physical violence if she reported any of these behaviors during the past 12 months. Likewise, she was considered a victim of minor or severe physical violence if she reported that her partner had done any of these behaviors to her in the past 12 months. We did not measure sexual or psychological harm in this study. Psychometric properties of the CTS scales are robust (Straus, 1990), and the cross-cultural validity of the CTS has been shown among many different populations (Straus, 2004).
Cultural orientation
The General Ethnicity Questionnaire (GEQ; Tsai et al., 2000) is based on four different varieties of acculturation: assimilation (replacing Pacific with New Zealand culture), integration (strongly aligned to both cultures), separation (strongly aligned to Pacific culture, weakly to dominant culture), and marginalization (weakly aligned to both cultures). We shortened and slightly modified this scale for the specific purposes of the PIF Study and developed the Pacific (PI Acculturation) and New Zealand (NZ Acculturation) versions of the GEQ (Borrows et al., 2011). The internal consistency of the measure was examined using Cronbach’s alpha and was found to be acceptable (α = .81 and .83 for the NZ Acculturation and PI Acculturation scales, respectively).
Sociodemographics
Ethnicity was self-reported at the beginning of the longitudinal study. We used baseline (at 6 weeks) household income as a proxy for socioeconomic status. We recorded maternal age, living arrangements, and highest education level at baseline. Socioeconomic status was measured at every phase; however, the baseline measure was used in this article as there were numerous phases.
Statistical Analysis
Percentages and means (where appropriate) are presented for the demographic characteristics of mothers included in this study. We used mixed effects logistic models, with random intercept, to consider the correlated results of repeated measure data. We allowed for nonlinear trends over time by estimating a spline model, identifying two time intervals. Two different linear trends were produced: from baseline (6 weeks) to 6 years follow-up, and from 6 to 14 years follow-up. We calculated unadjusted crude models for each and adjusted models using the process of forward stepwise selection to identify the best fitting and most parsimonious model among sociodemographic characteristics. Interaction effects were also investigated. Significance was tested at the p = .05 level. All analyses were completed using Stata version 14.0.
Results
Overall, 806 mothers were included in this study. Mothers were included in the data analysis if they had completed the CTS measure, and if they had participated in all the phases. Table 1 presents the sociodemographic characteristics of the mothers. At baseline, 75% of mothers were aged between 20 and 34 years, 67% were born outside of New Zealand, and 85% lived with the father of the cohort child. With respect to acculturation, 32.7% of mothers were characterized as assimilationist, 33.5% as segregationist, 18.4% as integrators, and 16.4% as marginalists. The number of maternal participants in each phase differs due to recruitment figures and to the relative number of mothers who did not complete the CTS measure.
Sociodemographic Characteristics of the cohort.
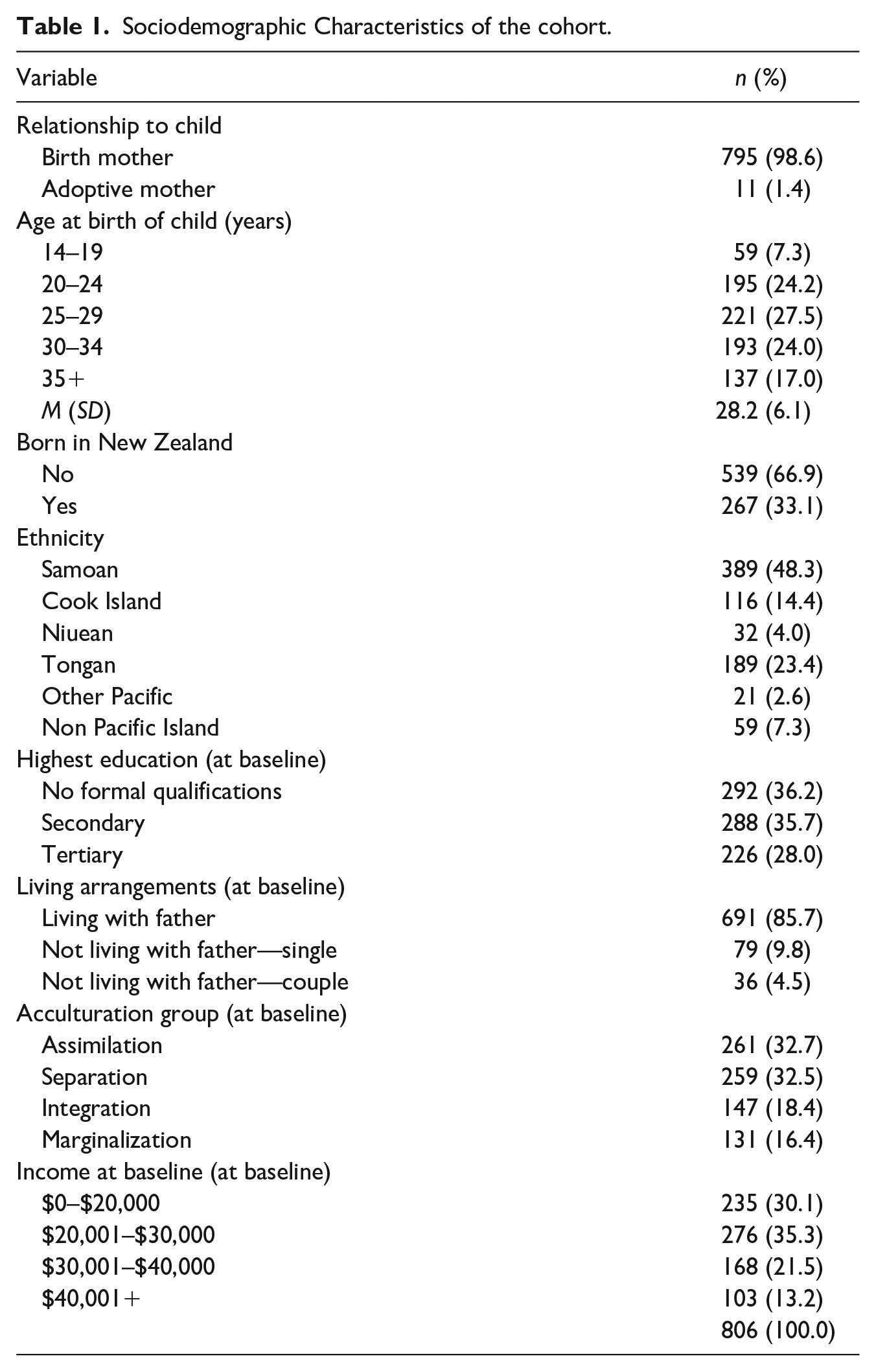
Table 2 shows that reported perpetration and victimization were most prevalent at baseline and 2 years post childbirth. At the 6-week and 2-year time points, 35.2% and 30.4% of mothers reported perpetration of minor IPV, respectively. This decreased to 14.5% by the 14-year phase (12 years later). At time points (6 weeks and 2 years), 18.9% and 17.9% of mothers reported perpetration of severe IPV. This decreased to 6.7% by the 14-year phase. Age had a significant effect on perpetration of both minor and severe perpetration of IPV.
Percentage Reporting Different Types of Violence, by Follow-Up Time.
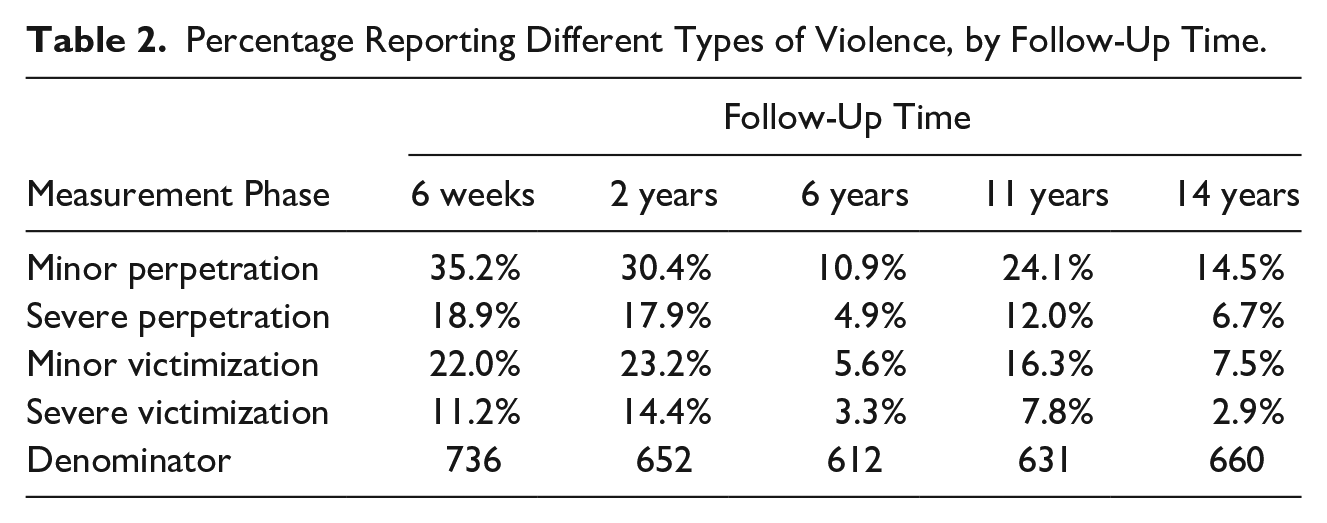
At time points (6 weeks and 2 years), 22% and 23.2% of mothers reported being a victim of minor IPV. This decreased to 7.5% by the 14-year phase. At time points (6 weeks and 2 years), 11.2% and 14.4% of mothers reported being a victim of severe IPV. At the 14-year phase, this had fallen to 2.9%. Age had a significant effect on being a victim of minor IPV but there was no significant effect on severe victimization of the mother.
Crude model estimates show significant reductions in the probability of mothers reporting violence (minor and severe, perpetrator and victim) from baseline to 6 years, but that after 6 years, the reporting of violence plateaued, and there was no significant change from 6 to 14 years follow-up. Figure 1 illustrates the predicted probability of violence at different time points.
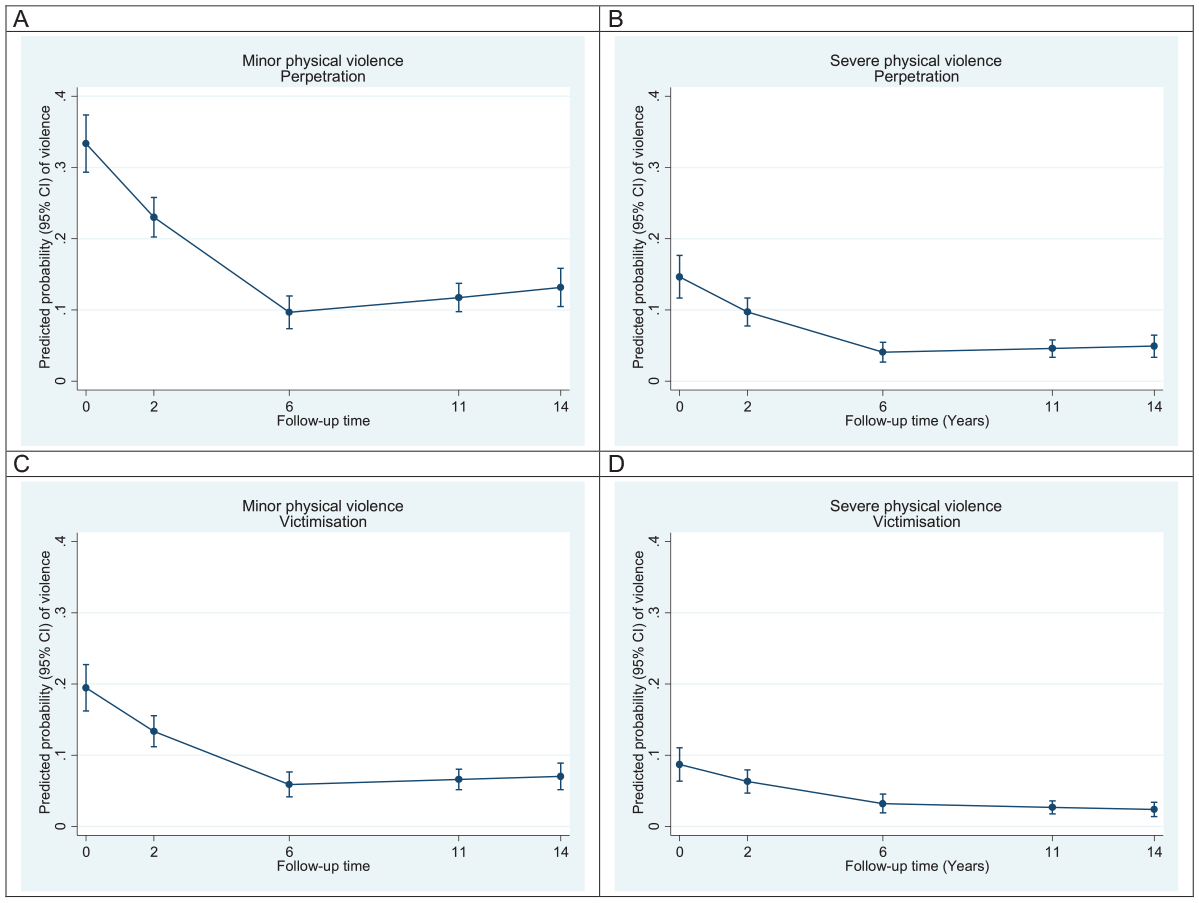
Predicted probability (mixed logistic model) of reporting violence, by type of violence.
Table 3 shows that after adjusting for associated factors, each year from baseline to 6 years, the odds ratio for reporting perpetration of minor physical violence was 0.775 (95% confidence interval [CI] = [0.737, 0.815]) indicating a 22% reduction yearly. The unit increase in the time (continuous) provided the odds ratio of 0.775 for the perpetration of minor physical violence (binary) relative to that year. From 6 to 14 years this estimate was 1.040 (95% CI = [0.998, 1.083]) indicating no significant change in the likelihood of reporting perpetration of minor violence. The model shows two patterns emerging, one being the decline to 6 years, and then the plateau to 14-year measurement points. Table 3 also presents the variables that are significantly associated with the different IPV outcomes. Cultural alignment had a significant effect on perpetration of IPV. Women who were strongly aligned with Pacific culture (separationists) were significantly less likely to report minor or severe perpetration of IPV with approximately 50% less likely to report this compared with assimilationists.
Multiple Mixed Logistic Regression, by Each Outcome.
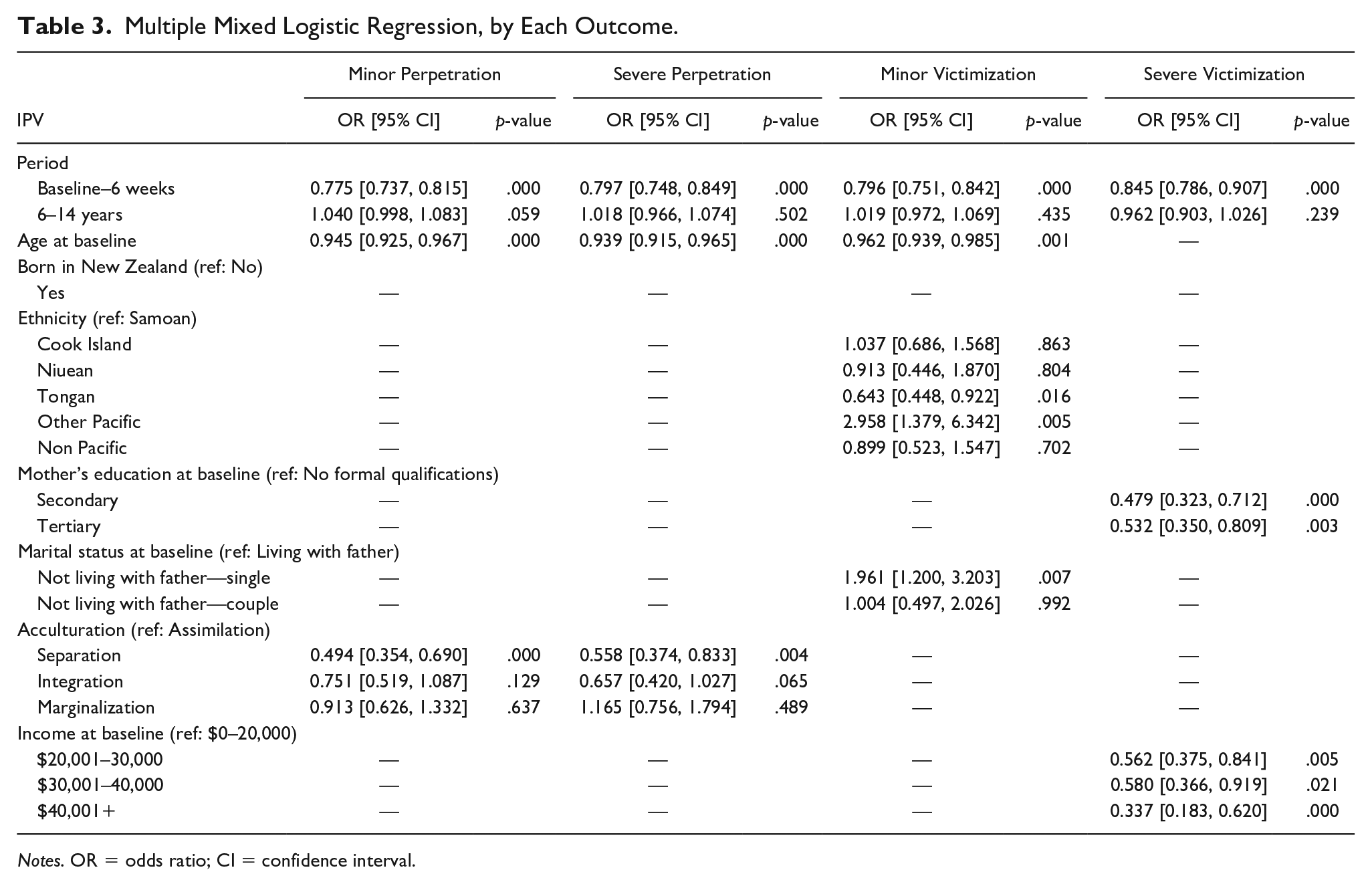
Notes. OR = odds ratio; CI = confidence interval.
For victimization, we found that single mothers not living with the father of the child were nearly twice as likely 1.961 (95% CI = [1.200, 3.203]) to report being a victim compared with mothers living with the father. Mothers with a secondary education 0.479 (95% CI = [0.323, 0.712]) were significantly less likely to report being a victim of severe violence than those with no qualifications. Similarly, mothers with a tertiary level education reported significantly less severe victimization than mothers with no formal qualifications. Higher levels of income were also associated with reduced levels of reporting severe victimization.
Discussion
IPV is a public health and human rights issue with numerous social and economic effects experienced by women. This article explored the patterns of minor and severe IPV perpetration and victimization over a 14-year period among Pacific women living in New Zealand. We found that in this cohort of Pacific mothers, the time points at which reported violence was the most prevalent were at 6 weeks and 2 years post childbirth. Thirty-five percent of mothers reported minor perpetration at 6 weeks, this reduced to 14.5% at 14 years. Twenty-two percent of mothers reported being a victim of minor physical violence at 6 weeks, this reduced to 7.5% at 14 years follow-up. Across time, there was also a general pattern of fewer women reporting severe physical perpetration and victimization across time. After 6 years, maternal reporting of violence, both perpetration and victimization, plateaued, and there was no significant change between the 6- and 14-year follow-up. This is in line with other findings that have shown that young women of reproductive age face a substantially higher risk of experiencing IPV than older women (Stockl et al., 2014). The combination of younger age, lower income, and single parenthood has been associated with a high risk of IPV (Thompson et al., 2006; Vest et al., 2002). It is likely that stress in romantic relationships around this period may lead to increased violence among spouses (Bair-Merritt et al., 2008). Consistent with other New Zealand surveys, the majority of IPV incidents reported by the PIF Study maternal respondents did not involve severe violence with the potential to result in injury or death (Marie et al., 2008; New Zealand Family Violence Clearing House, 2007).
Minor Perpetration and Victimization
We found that older mothers were significantly less likely to report minor victimization or perpetration of violent behavior toward their partner. Maternal reports of perpetration of minor IPV were highest in the postpartum period at 6 weeks (35.2%) and 2 years (30.4%) after the birth, respectively. Older mothers were also significantly less likely to report being a victim of minor IPV. The reporting of minor victimization of IPV was also highest in the postpartum period, at 6 weeks (22%) and 2 years (23.2%), respectively. In line with other studies, we found that being a single mother who did not live with the father was significantly associated with a higher risk of minor victimization (Huang et al., 2018; Thompson et al., 2006).
Severe Victimization and Perpetration
Perpetration of severe IPV was also significantly higher at the 6-week baseline (18.9%), and 2-year (17.9%) measurement points. These findings are in line with earlier findings that there is an increased risk of involvement in IPV for young women in the postpartum period (Harrykissoon et al., 2002; Martin et al., 2001; Stockl et al., 2014). Maternal age was not significantly associated with a decrease in maternal reports of severe victimization. Women who were significantly less likely to experience severe victimization were those with higher education and those in a higher income bracket. Other studies have found that higher educational attainment protected women against victimization (Cunradi et al., 2002; Heise, 2012; Victor et al., 2017; Vyas & Watts, 2008) and that the risk of violence was significantly higher for women on low incomes (Capaldi et al., 2012; Thompson et al., 2006). Women with education or who contribute financially may have a higher status in their household and be less vulnerable to violence. However, the resource-based power theory states that power within a family is a function of the ownership of resources that allows for decision-making autonomy (Goode, 1971). Thus, more resources equal more power (Jasinski, 2001). Conversely, it is posited that because these resources are often supplied by the man in the family, violence may arise in a struggle to maintain power when the female partner attains higher status (Gage & Hutchinson, 2006; Tomes, 1978).
There were no significant differences found in IPV reports among the Pacific ethnic groups; however, the mother’s cultural orientation did reveal significant associations with IPV. Mothers who described themselves as separationist (strongly aligned with Pacific Island culture and weakly aligned with the dominant New Zealand culture) were significantly less likely to report perpetration of minor and severe physical violence toward their partner than mothers who described themselves as assimilated (identified with New Zealand rather than Pacific Island culture). Acculturation researchers have consistently demonstrated that those who stay closer to their traditional culture are less likely to report violence (Borrows et al., 2011; Caetano et al., 2000; Garcia et al., 2004). These findings suggest that established ties with Pacific homeland traditions may protect against stress and conflict in the family. Nero (1990) stated that the stressors associated with Western influence on Pacific people are likely to exacerbate violence in the home. Duituturga (1988) pointed out that there may be unique challenges faced by Pacific women raising families in New Zealand, which may increase the likelihood that they will experience IPV. So, mothers who have weaker ties with Pacific traditions may develop conflicting expectations about their partner and familial roles, often leading to tension and possible violence.
Across time, there was a general pattern of fewer women reporting minor and severe physical perpetration and victimization up to the 6-year measurement point, after which the IPV reports plateaued over the next 8 years. These findings are in-line with other studies that suggest that age is protective against IPV in adulthood (Capaldi et al., 2012), and with findings from multi-wave prospective studies demonstrating the decline of IPV with age (Kim et al., 2008). In this cohort, there was a significant reduction in IPV with age except for severe victimization. Although severe victimization did decline over time it did not reach significance. This may be due to the significant impact of maternal education and earning power on the occurrence of IPV as women got older and more able to take up employment opportunities.
Strengths and Limitations
The PIF Study provides information from a large and culturally diverse cohort of Pacific families within New Zealand. It has a strong longitudinal design and has utilized sophisticated analytical techniques to examine the PIF Study data over time (Paterson et al., 2008). The CTS provides a standardized definition of mild, moderate, and severe IPV and is a critical instrument for measuring IPV events (Williams et al., 2008). The questionnaires in the PIF Study are administered either in an interview format or in a computerized format by trained researchers, which contributes to reliability and validity. However, some participants may under-report their own behaviors due to the social (un)acceptability of revealing IPV behaviors and may be more likely to report these behaviors if data collection was completely anonymous (e.g., online). While we acknowledge these limitations, in large-scale studies, such as the PIF Study, self-report is usually the most feasible option for measurement, and online data collection is difficult because many participants do not own a computer.
Although many studies show that adults involved in IPV are more likely to come from disadvantaged backgrounds (Cunradi et al., 2002), preventive measures should be directed at all families, regardless of socioeconomic status. The measure of socioeconomic status used in this article was from baseline which does not present a full reflection of that maternal respondent’s situation across time. These findings suggest that educational attainment is an important goal for women as educational qualifications combined with the ability to attract a higher income may provide the tools to protect women from severe victimization. Gender relations at a micro-level are affected by a range of cultural, institutional, and political influences acting in different spheres of men’s and women’s lives (Vyas & Watts, 2008). We need to understand how women’s relative power or ability to resolve conflict increases as they develop social and economic empowerment skills.
This longitudinal data reveals a peak in IPV during the postpartum period, with a slow decline to 6 years after the birth, after which IPV remains reasonably stable over the next 8 years. These two patterns are likely to reflect patterns of many health and psychosocial factors that cause stress for the individual and contribute to an increase in conflict. There remain significant gaps in our understanding of the situational and background factors that affect the way that risk factors for IPV develop and change over time. These findings can inform the timing and targeting of culturally appropriate violence prevention efforts in adolescence and young adulthood that focus on the development of healthy intimate partner relationships and effective methods of conflict resolution.
Footnotes
Acknowledgements
The authors gratefully acknowledge the study participants and the Pacific Islands Families (PIF) Advisory Board.
Authors’ Note
Opinions expressed or conclusions drawn in this paper are those of the authors and should not necessarily be regarded as those of the National Institute for Public Health and Mental Health Research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Pacific Islands Families (PIF) Study is funded by the Foundation for Research, Science & Technology, and the Health Research Council of New Zealand.