
Abstract
An emerging body of research has linked intimate partner violence (IPV) victimization with negative mental health outcomes among women in postreform China. However, limited scholarly attention has been given to the independent effects of multiple types of IPV victimization on depressive symptoms among men and women. Little is known if these independent effects will vary by gender in China where research on the association between IPV victimization and mental health did not emerge until fairly recently. Given this research paucity, this study aims to (a) examine the independent effects of different types of lifetime IPV victimization among married men and women in Sichuan province on their self-reported past 30-day depressive symptoms and (b) explore possible gender variations in these effects. The data utilized in this study came from a subsample of married men (N = 1,083) and women (N = 1,185) from the Third Survey of Chinese Women’s Social Status 2010, a representative sample of adults aged 18 to 64 in Sichuan province. Statistical analyses indicate that all types of lifetime IPV victimization are significantly and positively associated with past 30-day depressive symptoms for women, whereas for men lifetime experiences of general controlling behavior and sexual IPV were not statistically associated with depressive symptoms. Moreover, the effects of multiple types of IPV victimization on depressive symptoms do not significantly vary by gender. Bearing this gender-neutral pattern in mind, health professionals, governmental officials, and researchers are strongly encouraged to focus on both married men and women in their IPV and mental health intervention, prevention, and treatment endeavors in postreform China.
Introduction
Recent studies have demonstrated that intimate partner violence (IPV) occurs frequently around the world, cutting across all socioeconomic, cultural, and religious boundaries (Chen et al., 2016; García-Moreno et al., 2005, 2006; Ogland et al., 2014; Wong et al., 2016, 2013; Xu, 1997; Xu et al., 2011, 2019; Zhang et al., 2019; Zhang & Zhao, 2018; Zheng et al., 2019). More importantly, multiple strands of evidence show that IPV victimization is associated with a myriad of pernicious physical, mental, and reproductive health outcomes globally, which is particularly pronounced for women who have experienced either lifetime or past year/month IPV (Garcia-Moreno et al., 2006; Wong et al., 2016). Given these serious health consequences, IPV incurs a host of direct and indirect financial burdens and costs worldwide. Fearson and Hoeffler (2014) estimated that in 2013 the annual cost of IPV was about 5.2% of global GDP. Echoing these bourgeoning patterns of global evidence, an emerging body of research has linked IPV victimization with negative physical, mental, and/or reproductive health outcomes in postreform China (Chinese society after the economic reform launched by the Chinese government in 1978) (Dong et al., 2008; Parish et al., 2004; Tang, 1997; Tiwari et al., 2008, 2015; Wang et al., 2016; Yan & Tang, 2001).
While this emerging body of research is illuminating, there have been several gaps in prior research on the association between IPV victimization and mental health in postreform China. First, much of the prior research focused primarily on subpopulations that are particularly vulnerable to high risk of IPV victimization and depression/anxiety disorders, including but not limited to, clinic patients, older adults, migrant workers, divorced women, pregnant women, rural women, and women who utilized shelters (Chen et al., 2016; Dong et al., 2008; Gao & Jacka, 2012; Lin et al., 2018; Qiu et al., 2011; Tang, 1997; Tiwari et al., 2008, 2015; Wang et al., 2016; Wong et al., 2013; Yang et al., 2018; Zhan, 2006). Consequently, the research findings derived from these studies cannot be generalized to broader populations in China. Second, few studies, if any, have holistically compared and contrasted mental health outcomes across multiple types of IPV victimization, such as controlling behaviors, physical, psychological, and/or sexual IPV experienced by men and women. This is surprising because different types of IPV victimization have exhibited differential prevalence rates and severity (Tang & Lai, 2008; Wong et al., 2016), which have resulted in varying degrees of negative mental health outcomes (Tiwari et al., 2015). Third, despite the ongoing debate over gender symmetry or asymmetry in the etiology of IPV due to divergent epistemological positions and methodological approaches (Anderson, 1997, 2005; Chen & Chan, 2019; Johnson, 1995, 2006, 2011; Winstok & Straus, 2014), rarely has prior research investigated gender variations in the effects of multiple types of IPV victimization on deleterious mental health outcomes in the context of postreform China. The lone exception is research on older adults who are 60 years of age or older (Dong et al., 2008).
Given the above-documented gaps and research paucity, the current study aims to accomplish two research goals by utilizing a provincial survey from a sample of married adults in Sichuan, China. The primary goal is to examine the independent effects of multiple types of lifetime IPV victimization on self-reported past 30-day depressive symptoms among married men and women. The secondary goal is to explore possible gender variations in these effects.
To accomplish these research goals, this study utilizes and extends the definition of IPV from the World Health Organization (WHO) that defines IPV as “behavior(s) by an intimate partner or ex-partner that causes physical, sexual or psychological harm, including physical aggression, sexual coercion, psychological abuse and controlling behaviors” (García-Moreno et al., 2005; WHO, 2017). By adopting this multidimensional conceptualization of IPV that encompass such subdimensions as lifetime experiences of personal and financial controlling behaviors, physical, psychological, or emotional (verbal and nonverbal), and sexual IPV victimization (see Lin et al., 2018; Zheng et al., 2019), this study can advance the literature on IPV in contemporary China. This effort is timely because research on the association between IPV victimization and mental health did not emerge until fairly recently.
Moreover, this study also utilizes a gender perspective to establish linkages between multiple types of IPV victimization and negative mental health outcomes among married men and women. This perspective centers around differences and similarities concerning IPV victimization and mental health. Prior research has disproportionately focused on women in light of their greater propensity to experience IPV and depression/anxiety disorders (Anderson, 2002; Campbell, 2002; Coker et al., 2002; Hopcroft & Bradley, 2007; Pearson, 1995; Simon, 2002; Winstok & Straus, 2014). Recent research findings, however, suggest that men are equally likely to report experiencing multiple types of IPV perpetrated by their female partners (Winstok & Straus, 2014). More importantly, IPV victimization experienced by men also exerts negative effects on their psychological well-being in a similar fashion as reported by women (Próspero, 2007; Randle & Graham, 2011). Moving beyond the research findings based on one gender, the current study is the first of its kind in the context of postreform China to examine the effects of multiple types of IPV victimization on mental health among men and women simultaneously. Such research efforts have important implications for practice, including intervention, prevention, and treatment of IPV and mental health disorders for both genders.
Types of IPV Victimization and Depressive Symptoms
Informed by the WHO definition (García-Moreno et al., 2005; WHO, 2017), the typology of IPV victimization used in this study includes lifetime experiences of (a) controlling behaviors that involve such acts as monitoring a partner’s activities and restricting a partner’s access to financial resources; (b) physical IPV that involves slapping, hitting, kicking, and beating; (c) psychological IPV (both verbal and nonverbal) that includes insults, humiliation, and intimidation; and (d) sexual IPV that includes forced sexual intercourse and other forms of sexual coercion (García-Moreno et al., 2005; WHO, 2017). These types of IPV victimization are comparable to the well-recognized typology of IPV developed by Michael Johnson (1995, 2006) with a critical difference; that is, the controlling behaviors and intimate partner violent acts used in this study could be gender symmetric, thereby different from “patriarchal terrorism” defined as “a form of terroristic control of wives by their husbands that involves the systematic use of not only violence, but economic subordination, threats, isolation, and other control tactics” (Johnson, 1995). Indeed, it is a challenge to identify and classify controlling behaviors or intimate partner violent acts as “intimate terrorism” for men or women who have experienced IPV in survey-based studies. It requires specific and accurate knowledge about the contexts, motivations, and consequences of controlling behaviors or other types of IPV perpetration. Unfortunately, such information is often unavailable in survey research (Neal & Edwards, 2017). Therefore, this study does not define controlling behaviors or intimate partner violent acts as intimate terrorism. Instead, they are more aligned with Johnson’s typology of “common couple violence” or “situational couple violence,” which does not necessarily involve an attempt to exert control over the partner (Johnson, 2011). These types of IPV victimization may occur when couple conflicts become arguments that may turn to aggression and violence (Johnson, 2006; also see Winstok & Straus, 2014 for a more systematic review). However, it is important to recognize that physical and sexual IPV are disproportionately perpetuated by male partners than female partners (Bonomi et al., 2007; Lin et al., 2018).
To link multiple types of IPV victimization as delineated above with depressive symptoms, this study utilizes the social stress paradigm—a leading framework in the sociological study of stress and mental health—that focuses on both structural and individual sources of psychological distress and depression disorder (Avison et al., 2009; Pearlin et al., 1981). Under this paradigm, traumatic stress is recognized as a major mechanism through which experiences of IPV can lead to subsequent depressive symptoms (Campbell, 2002; Winstok & Straus, 2014). In other words, the victimization of controlling behaviors and various types of intimate partner violent acts are viewed as traumatic experiences that can result in stress, fear, and isolation, which, in turn, can lead to depressive symptomatology. Therefore, all types of IPV victimization can be conceptualized as structural or individual sources of stress or strain that will manifest themselves in depressive symptoms.
A substantial array of evidence in the West has confirmed the association between experiencing various types of IPV and depressive symptoms as explicated by the social stress paradigm. In a meta-analysis of the past studies, Golding (1999) concluded that among abused women in the United States nearly one half (47.6%) reported being depressed (Golding, 1999) or meeting the criteria for major depression (Goodwin et al., 2003). One nationally representative study indicated that women were significantly more likely than men to experience physical or sexual IPV, and for both men and women, the victimization of physical IPV was associated with increased risk of depressive symptoms (Coker et al., 2002). Another study conducted in Spain revealed that women exposed to both physical and psychological IPV or psychological IPV alone reported a higher incidence and severity of depressive and anxiety symptoms than women who did not experience physical or psychological IPV. Moreover, the same study showed that women who experienced sexual IPV in addition to physical and/or psychological IPV reported a higher severity of depressive symptoms (Pico-Alfonso et al., 2006). In the context of developing countries, the WHO study reported that women who had ever experienced physical or sexual IPV, or both, reported higher levels of psychological distress than women who had never experienced IPV (García-Moreno et al., 2005). In comparison with studies on women, research on men’s mental health consequences as victims of IPV is limited. Although in its infancy, prior studies did show that men were more likely than their female counterparts to experience psychological rather than physical IPV, which also led to depression, suicidal ideation, and other mental health difficulties (Coker et al., 2002; Randle & Graham, 2011).
With respect to postreform China, a mixed methods study conducted in Hong Kong demonstrated that women who were 18 years of age or older and who had been victims of intimate terrorism in the past year reported significantly more symptoms of depression than those who were victims of situational couple violence (Tiwari et al., 2015). In a similar vein, abused women from Hong Kong who utilized the shelter reported higher levels of depression and anxiety than their nonabused peers (Tang, 1997). In the context of the mainland, one cross-sectional study conducted in the community health service center in Wuhan reported that women who experienced physical or psychological IPV exhibited greater risk of post-traumatic stress disorder than their counterparts that had never experienced IPV (Wang et al., 2016). Taken together, the existing research provides inconsistent or inconclusive evidence to suggest that different types of IPV victimization will result in differential levels of depressive symptoms.
Turning to the relationship between experiencing controlling behaviors and depressive symptoms, research findings are extremely rare. One study conducted in the United States revealed that the effects of coercive behaviors, such as controlling a partner’s money and restricting a partner’s meeting with family or friends, on depressive symptoms are significantly stronger among female victims of IPV than male victims of IPV (Próspero, 2009). Another study conducted in Karachi, Pakistan showed that more than 50% of married women experienced different types of controlling behaviors by their husbands, such as monitoring the wife’s activities and restricting the wife’s access to certain resources. These experiences were reportedly associated with negative mental health outcomes (Ali et al., 2014). As of today, however, no such research efforts have been made in the context of postreform China.
Informed by the theoretical and empirical evidence reviewed above, it is hypothesized that there will be significant and positive associations between multiple types of lifetime IPV victimization, including experiences of personal and financial controlling behaviors, physical, psychological, and sexual IPV, and past 30-day depressive symptoms among married respondents from Sichuan, China, independent of sociodemographic backgrounds (Hypothesis 1). That is, these independent, significant, and positive associations will be observed for both married men and women.
The Missing Piece: Are There Gender Variations in the Effects of Multiple Types of IPV Victimization on Depressive Symptoms?
Gender differences and similarities in IPV victimization have been debated for more than two decades now. It still behooves researchers to continue to consider the role of gender in IPV victimization (Anderson, 1997; Johnson, 2006; Winstok & Straus, 2014). Scholars of family violence seem to generally agree that there is gender symmetry in common couple violence perpetration but there is gender asymmetry in the mental health consequences resulting from IPV victimization (Anderson, 2002; Winstok & Straus, 2014). Recent research evidence suggests that while men and women can be equally likely to be victimized by their intimate partners (Chan, 2011; Chen & Chan, 2019), female victims of IPV tend to report significantly more severe victimization of physical and sexual IPV (Campbell, 2002; Romito & Grassi, 2007). Striking gender differences exist in depression and anxiety disorders between men and women (Hopcroft & Bradley, 2007; Pearson, 1995; Salk et al., 2017; Simon, 2002), but knowledge concerning gender variations in the effects of multiple types of IPV victimization on mental health is awfully limited (Winstok & Straus, 2014).
One nationally representative study conducted in the United States reported that regardless of severity, women as victims of physical IPV were more strongly associated with psychological distress than their male counterparts as victims of IPV (Williams & Frieze, 2005). A similar finding also surfaced from an Italian study on college students, which demonstrated that female students who were victims of both psychological and physical IPV were more likely to be depressed than their male counterparts (Romito & Grassi, 2007). These gendered empirical findings appear to be congruent with Anderson’s assertion based on a nationally representative study in the United States. She concluded that there might be gender symmetry in reported IPV perpetration; however, this might not imply gender symmetry in depressive symptoms resulting from IPV victimization (Anderson, 2002).
In contrast to the study findings documented above, one recent study of a New Zealand birth cohort suggested that IPV victimization (ranging from minor psychological to severe physical IPV) exerted comparable effects on the mental health of men and women (Fergusson et al., 2005). In a similar fashion, one U.S. study revealed that male victims of IPV were just as likely as female victims of IPV to report depressive and anxiety symptoms (Próspero, 2007). This symmetric pattern was also found among African Americans. It was reported that experiencing controlling behaviors and physical IPV was equally likely to result in depression and psychological distress for African American men and women (Huang & Gunn, 2001).
Turning to China, even though empirical studies have yet to yield conclusive evidence to support either gender symmetry or gender asymmetry in IPV victimization and its mental health consequences in postreform China, various sources of data do exhibit similar prevalence rates of IPV perpetration for both genders if the contexts, motivations, and/or consequences of IPV are not accounted for (Chan, 2011; Ma, 2013). However, if the contexts and motivations are indeed considered, emergent research in China suggests that IPV perpetrated by women against their intimate partners is often motivated by self-defense (Fang, 2005; J. Wang & Wang, 2013). These findings along with those reviewed previously for women seem to suggest that there are gender differences in the effects of multiple types of IPV victimization on mental health with women experiencing higher levels of depressive symptoms resulting from IPV victimization. With the absence of empirical studies, these suggested gender differences make sense in the postreform era in which traditional gender norms are revitalized. Not only does this revitalization endorse traditional or patriarchal gender ideologies (e.g., separate-sphere ideologies) but also encourages women’s greater involvement in marriage/family life and justifies gender inequalities exacerbated by the market reform (Sun & Chen, 2015). As part of this revitalization of traditional gender ideologies and roles, marital relationships in the postreform era continue to be marked by a gendered division of housework and decision-making power. Such gender inequalities in marital relationships have profound implications for IPV against women and depression disorder (Ji et al., 2017; Pimentel, 2006; Xu, 1997). To summarize, as of today little is known about gender differences in the effects of multiple types of IPV victimization on mental health in the context of postreform China. This study is designed specifically to address this research paucity.
After weighting the documented gender differences and similarities in IPV victimization and its mental health outcomes, it seems reasonable and plausible to hypothesize that the positive associations between multiple types of lifetime IPV victimization and depressive symptoms in Sichuan, China, will be stronger for married women than for married men (Hypothesis 2). Stated differently, there will be significant gender variations in the effects of multiple types of lifetime IPV victimization on depressive symptoms.
Method
Data
Data used to test the two hypotheses developed above came from the Third Survey of Chinese Women’s Social Status (SCWSS) conducted in 2010, a representative sample of Chinese adults aged 18 to 64 years in Sichuan province, the People’s Republic of China. As a part of the national survey, the SCWSS 2010 was administered decennially by the All-China Women’s Federation (ACWF) and the National Bureau of Statistics (NBS). The SCWSS 2010 followed up the first and second cycles of the survey conducted in 1990 and 2000, respectively. The survey covered nine aspects of women’s lives in China, including health, education, politics, economy, social security, marriage and family, lifestyle, legal rights, and gender awareness (Third Survey of Chinese Women’s Social Status, 2013). As such, the SCWSS 2010 is the most updated and appropriate data set available for this study.
Located in the southwest region of China, Sichuan is one of the most populous and rural provinces. According to the 2010 Census, Sichuan’s population size is over 80 million and about 60% of its population reside in rural areas (Statistical Bureau of Sichuan Province, 2011). In 2010, there were 18 administrative cities and three Minority Autonomous Prefectures in the province, which constituted the sampling frame for the SCWSS 2010. Based on the available budget and population characteristics, a team of researchers from ACWF and NBS randomly selected a sample of 2,992 adults between the ages of 18 and 64 using a multistage, probability proportional to size sampling method. In the first stage, the research team randomly selected 20 out of the 57 city districts (including county-level cities) and 27 out of the 124 rural counties. In the second stage, the research team randomly selected five urban neighborhoods or streets and rural villages, respectively, from the chosen cities and counties stratified by levels of urbanization and local economic development. In the third stage, 15 households were randomly selected in each chosen neighborhood or village. Finally, 2,992 respondents were selected for face-to-face interviews by way of Kish sampling within each household that involved a simple random selection procedure to choose one of the multiple qualified respondents (Kish, 1949). Professional interviewers were recruited and trained by ACWF with interviews conducted in respondents’ homes. Because the survey was launched and organized by the government agencies, the response rate for the individual surveys was 99% (Third Survey of Chinese Women’s Social Status, 2013). This study made use of a subsample of 1,083 married men and 1,185 married women (total N = 2,268). Respondents involved in other types of romantic or intimate relationships such as cohabitation were excluded from this study as the information was not ascertained in the survey.
Measures
Dependent variable
To operationalize mental health outcomes, the dependent variable is a mean-score index of eight survey items measuring depressive symptoms. Respondents were asked to indicate how often they had felt the following over the past 30 days: (a) my sleep was restless, (b) I felt tired or had little energy, (c) I became angry easily, (d) I had crying spells, (e) I had little interest or pleasure in doing things, (f) I felt lonely, (g) I felt useless, and (h) I felt meaningless to be alive. Responses to these eight questions were recorded on a Likert-type scale with 0 = never, 1 = occasionally, 2 = sometimes, and 3 = often. These items were averaged to create a composite measure of depressive symptoms (Cronbach’s α = .81 for men and .86 for women). To overcome skewness, this mean-score index was log-transformed and the resulting variable ranges from 0.6 to 1.35 with higher values representing higher levels of depressive symptoms. It is important to note that though these survey questions were worded somewhat differently, they are consistent with the items included in the Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff, 1977).
Independent variables
Resembling the WHO multicountry study on women’s health and domestic violence against women (García-Moreno et al., 2005), this study utilized both individual and composite measures to operationalize multiple types of lifetime experiences of IPV against married men and women in Sichuan, China. First, two questionnaire items asking respondents throughout their marriage how often their husband or their wife had (a) confined their personal freedom or (b) controlled them financially were used to indicate lifetime experiences of spousal controlling behaviors. Responses were first recorded on a Likert-type scale with 0 = never, 1 = occasionally, 2 = sometimes, and 3 = often, then dummy coded with 1 = yes and 0 = no (reference).
Second, four survey items were employed to operationalize lifetime experiences of physical, psychological (verbal and nonverbal), and sexual IPV. Respondents were asked if the husband or the wife had ever (a) hit or beat you (used as an indicator of physical IPV), (b) insulted you or called you names (used as an indicator of verbal psychological IPV), (c) ignored you for several days (used as an indicator of nonverbal psychological IPV), and (d) forced you to have sex (used as an indicator of sexual IPV). Once again, responses were first recorded on a Likert-type scale with 0 = never, 1 = occasionally, 2 = sometimes, and 3 = often, then dummy coded with 1 = yes and 0 = no (reference).
In addition to these individual measures, three composite IPV victimization measures were constructed to approximate the severity of IPV victimization concomitantly. They are (a) a mean-score index of experiencing controlling behaviors with Cronbach’s α = .60 for men and .61 for women (ranging from 0 to 3); (b) a mean-score index of four types of IPV victimization with Cronbach’s α = .64 for men and .64 for women (ranging from 0 to 2.67); and (c) a mean-score index of total IPV victimization, including both controlling behaviors and violent acts, with Cronbach’s α = .65 for men and .72 for women (ranging from 0 to 2.67). The original Likert-type scale (0 = never, 1 = occasionally, 2 = sometimes, and 3 = often) was used to compute these composite measures with higher values indicating higher levels of IPV victimization. As can be observed, though marginally acceptable (DeVellis, 2016), the reliability coefficients for all the victimization index variables are uniformly lower than expected. However, this should not pose major threats to the research findings because the principal emphasis of this study is on the independent effect of each individual measure of IPV victimization rather than various composite measures of IPV victimization. The latter only plays a minor or secondary role.
A series of multiplicative (interaction) terms were computed involving all types of IPV victimization and gender to explore gender variations in the effects of IPV victimization on depressive symptoms. In so doing, the respondent’s gender was used chiefly as a moderating variable. Significant multiplicative terms in the subsequent statistical analysis will signify the presence of the moderating or interaction effects, namely, gender variations in the effects of IPV victimization on depressive symptoms.
Control variables
This study included a number of sociodemographic characteristics as statistical controls that might confound the association between IPV victimization and depressive symptoms. Age of the respondent was measured in years. The respondent’s personal annual income of all sources was measured in Chinese Yuan, which was log-transformed to reduce skewness. Educational attainment of the respondent was measured as levels of education ranging from 1 = no formal education to 8 = postgraduate education. Employment status was dummy coded with 1 = unemployed or not working and 0 = employed either full-time or part-time. The family living arrangement or family structure was dummy coded with 1 = extended family and 0 = nuclear family. The number of children the respondent has ever had was measured in actual number. Finally, the respondent’s residence was dummy coded with 1 = urban and 0 = rural.
Analytic Strategies
To estimate the independent effects of multiple types of lifetime IPV victimization on past 30-day depressive symptoms and assess gender variations in these effects, a total of six ordinary least squares (OLS) regression models were estimated separately by gender, one for each type of controlling behaviors and violent acts. This modeling strategy allowed us to (a) systematically evaluate the net or independent effects of each type of IPV victimization on depressive symptoms and (b) assess if gender moderated these effects. For the composite measures of IPV victimization, three OLS regression models were estimated separately by gender as well. These models explored the effects of combined controlling behaviors, violent acts, and total IPV victimization on depressive symptoms, respectively. When assessing gender variations in the effects of IPV victimization on depressive symptoms (i.e., moderating or interaction effects), formal statistical tests were conducted for all the interaction terms. All missing values (one missing value in the dependent variable for married men and two missing values in both the dependent and IPV variables for married women) were replaced with the estimates generated from the multiple imputation procedure in SPSS version 26 via the chained equations imputation method (IBM Corporation, 2017).
Results
Table 1 displays the descriptive statistics for all the variables under this study by gender. As can be seen from the table, male respondents are, on average, older, better educated, and more likely to be employed than their female counterparts. About 39% of the respondents resided in urban areas at the time of interview, which is nearly identical to the provincial population proportion (about 40%) based on the 2010 census (Statistical Bureau of Sichuan Province, 2011). It is also observed that more than one third of the respondents (37%) indicated that they lived in an extended household at the time of interview.
Sample Characteristics by Gender (N = 2,268).
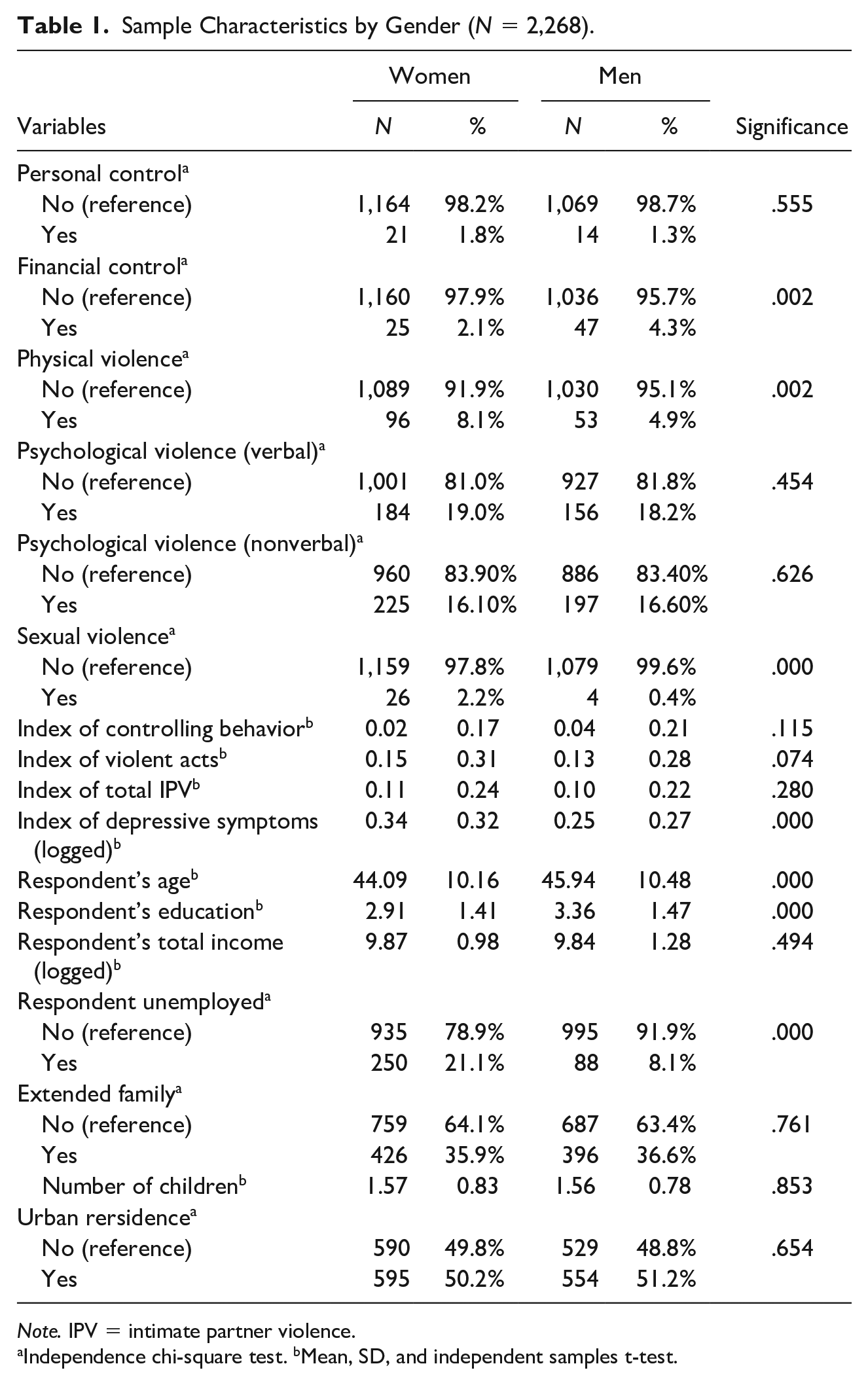
Note. IPV = intimate partner violence.
Independence chi-square test. bMean, SD, and independent samples t-test.
Turning to gender variations in IPV victimization, it is observed that while male respondents (4.3%) were significantly more likely than female respondents (2.1%) to report experiencing financial control exerted by their partner (p < .01), female respondents (2.2%) reported a higher percentage of experiencing sexual IPV than their male counterparts (0.4%; p < .001). In both cases, however, the small cell counts are noted, which can pose problems for multivariate statistical analyses. As expected, a significant gender difference exists in physical IPV victimization where female respondents reported a higher victimization rate (7.9%) than male respondents (6%). This difference is statistically significant at the .05 level. Moreover, gender symmetric patterns (i.e., insignificant gender differences) are found in psychological or emotional IPV victimization (18.2% and 19% for male and female respondents, respectively) and in all composite measures of controlling behaviors and violent acts. Finally, as anticipated, there is a striking gender difference in the log-transformed mean scores of past 30-day depressive symptoms with female respondents scoring significantly higher than their male counterparts (p < .001).
Tables 2 and 3 feature the results from the multivariate OLS regression models by gender. Table 2 reports the independent effects of multiple types of lifetime experiences of controlling behaviors and violent acts on past 30-day depressive symptoms for married women. As hypothesized, throughout the regression models (Models 1–6), married women who experienced all types of controlling behaviors and intimate partner violent acts reported significantly higher levels of depressive symptoms than those who did not report experiencing IPV, net of statistical controls (significant levels range from p < .05 to p < .001). It is also observed that physical and psychological IPV victimization exhibits more significant effects on depressive symptoms than other types of IPV victimization for married women. Given these results, Hypothesis 1 is supported by the data for married women.
OLS Regressions to Predict Depressive Symptoms: IPV Individual Measures (Married Women).
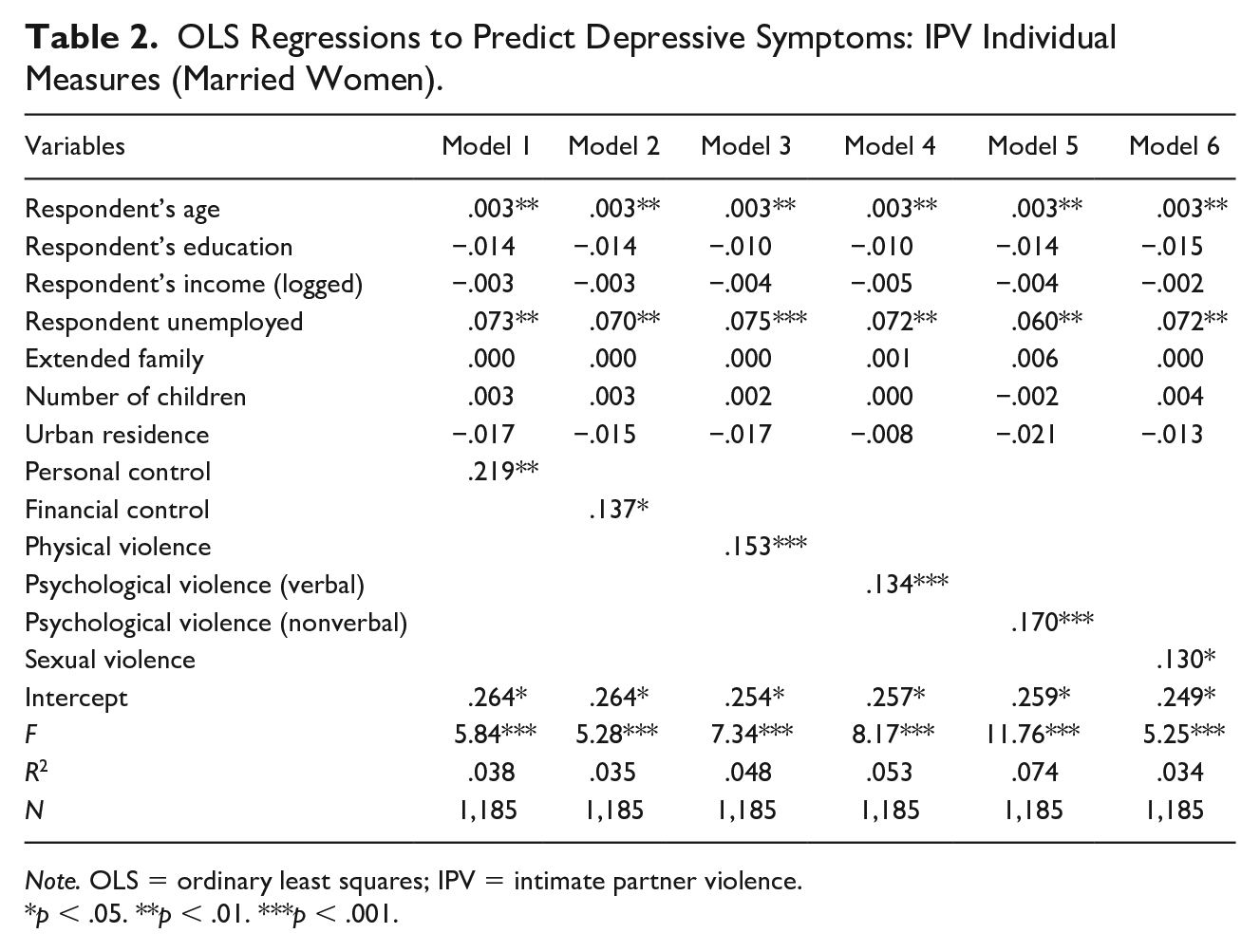
Note. OLS = ordinary least squares; IPV = intimate partner violence.
p < .05. **p < .01. ***p < .001.
OLS Regressions to Predict Depressive Symptoms: IPV Individual Measures (Married Men).
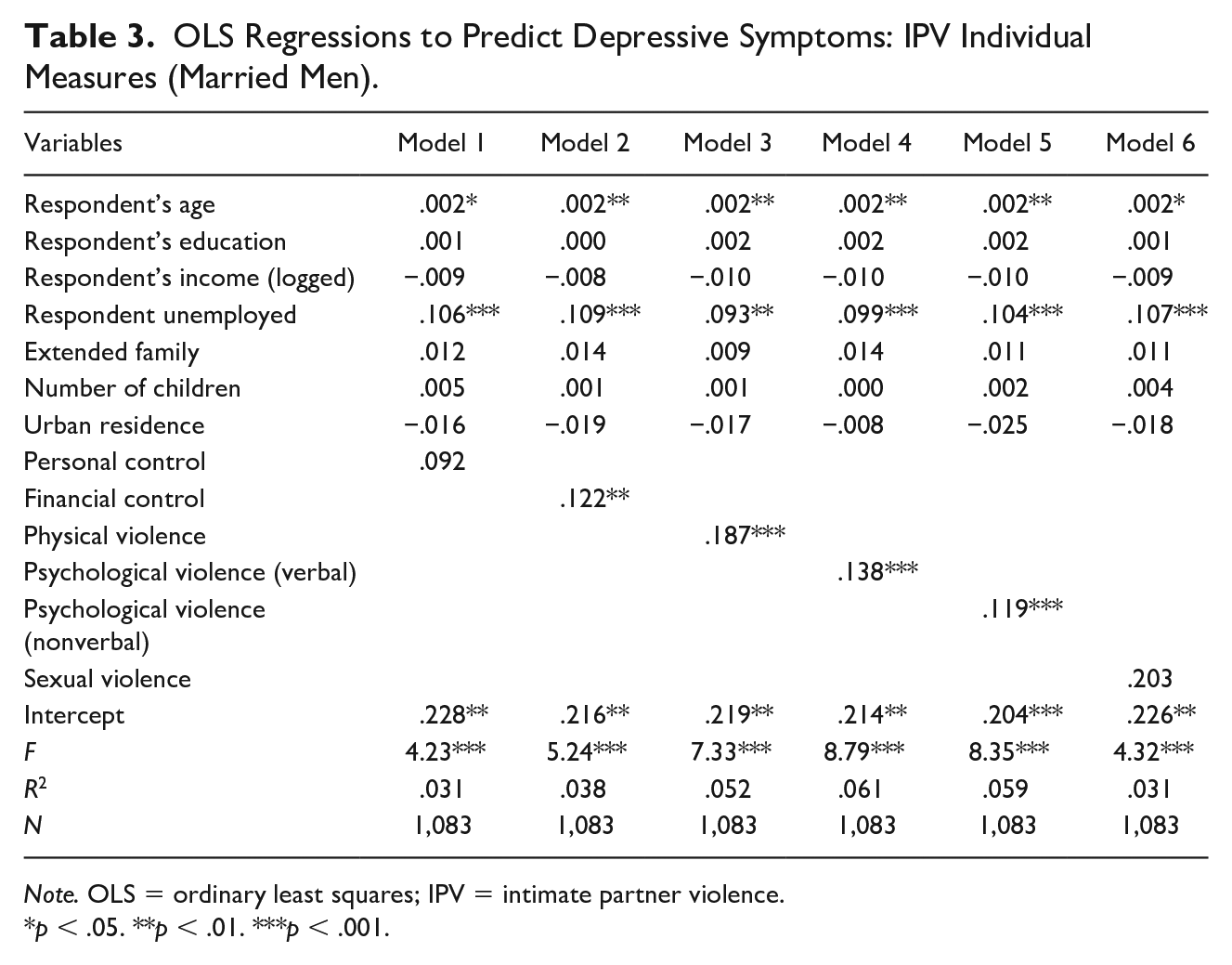
Note. OLS = ordinary least squares; IPV = intimate partner violence.
p < .05. **p < .01. ***p < .001.
In a similar fashion, Table 3 displays the independent effects of multiple types of lifetime experiences of controlling behaviors and violent acts on past 30-day depressive symptoms for married men. Even a cursory review of the table suggests nearly identical patterns for married men compared with married women with two important exceptions. First, contrary to what was found for married women, the regression coefficients for personal controlling behavior and sexual IPV victimization are not statistically significant for married men. However, married men who experienced all other types of IPV reported significantly higher levels of depressive symptoms than those who did not experience these violent acts (significant levels range from p < .01 to p < .001). These results are consistent with those reported in Table 2 for married women. Once again, it is observed that physical and psychological IPV victimization exhibits more significant effects on depressive symptoms than other types of IPV victimization for married men. With these results, Hypothesis 1 is partially supported for married men.
Table 4 reports the effects of three composite measures of lifetime experiences of IPV on past 30-day depressive symptoms. Model 1 includes the index of controlling behaviors, which is a mean-score composite as a severity measure of controlling behaviors. Not surprisingly, the effects are positive and highly statistically significant for both married men and women (p < .001). Model 2 estimates the independent effects of the mean-score index of four types of intimate partner violent acts. Once again, this index variable serves as a severity measure of IPV victimization. Consistent with Model 1, there are statistically significant and positive effects on depressive symptoms for both married men and women (p < .001). Finally, Model 3 examines the effects of a mean-score index of total IPV victimization, which is a combination of experiencing controlling behaviors and intimate partner violent acts, on depressive symptoms. As surmised, the regression coefficients are statistically significant and positive for both married men and women (p < .001). These results also provide systematic support for Hypothesis 1.
OLS Regressions to Predict Depressive Symptoms: IPV Composite Measures by Gender.
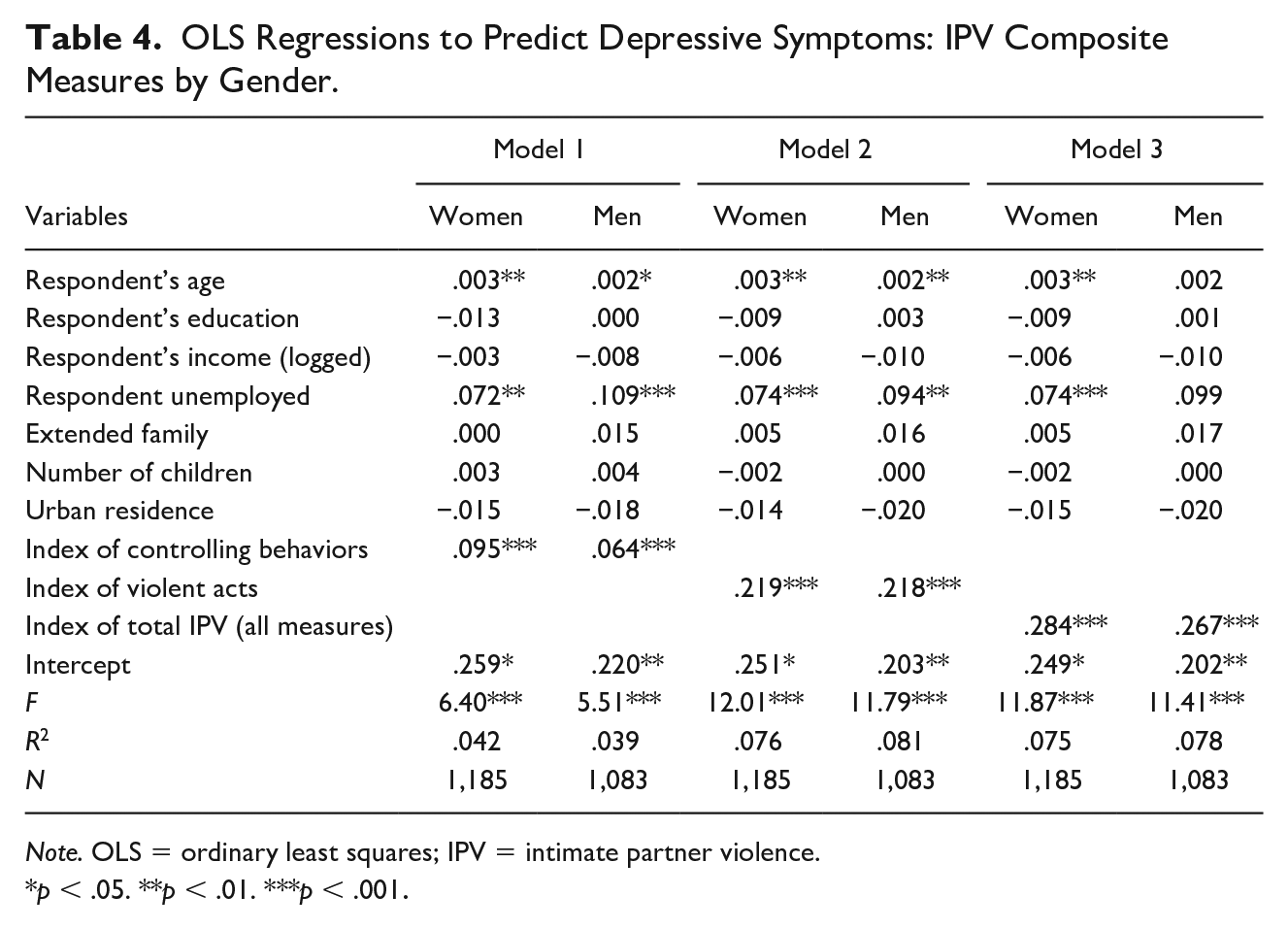
Note. OLS = ordinary least squares; IPV = intimate partner violence.
p < .05. **p < .01. ***p < .001.
Last but not least, Table 5 displays the interaction effects of multiple types of IPV victimization and gender on depressive symptoms. A quick glance of the table indicates that none of these interaction terms is statistically significant at the .05 level. These findings suggest that there is a gender parity or symmetry in the effects of multiple types of lifetime IPV victimization on the mental health of married respondents from Sichuan, China. As such, Hypothesis 2 is strongly rejected.
Gender Differences in the Effects of IPV Victimization on Depressive Symptoms.
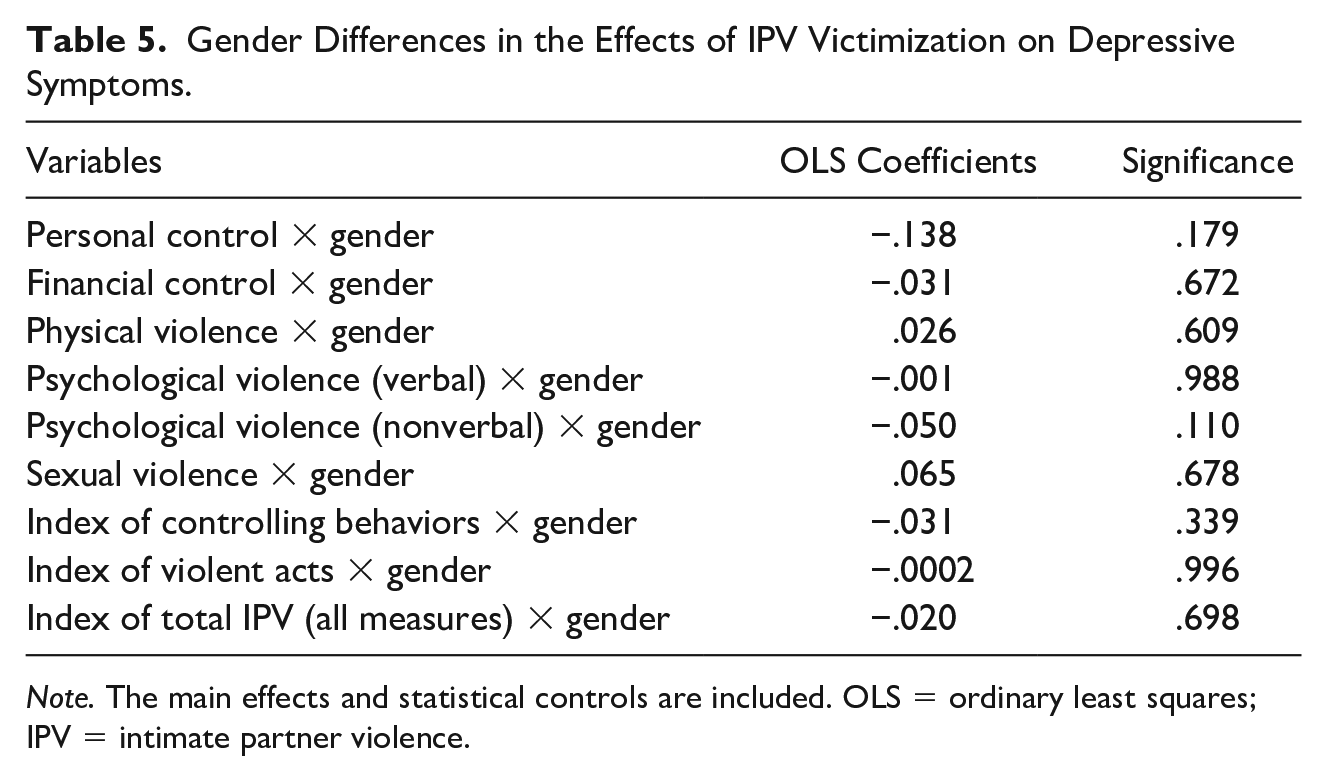
Note. The main effects and statistical controls are included. OLS = ordinary least squares; IPV = intimate partner violence.
Two sociodemographic characteristics emerged as significant and consistent predictors of depressive symptoms. The regression results reported in Tables 2–4 show that the respondent’s age and unemployment are positively associated with depressive symptoms for both married men and women. While these results are in line with prior research findings, to focus sharply on IPV, no further interpretations are rendered.
Conclusion and Discussion
The primary goal of this research was to establish multifaceted linkages between multiple types of lifetime IPV victimization and past 30-day depressive symptoms among married men and women in postreform China. One of the surprising findings was that both male and female married respondents in this provincial survey reported much lower lifetime IPV victimization rates than the estimates from previous studies. For example, 8.1%, 19%, and 2.2% of female respondents in this study reported experiencing lifetime physical, psychological, and sexual IPV, respectively, which are lower than the national estimates of 14.2%, 42.6%, and 9.8%, respectively, for physical, psychological, and sexual IPV (Tang & Lai, 2008). Likewise, male respondents in this provincial survey also reported lower than expected lifetime IPV victimization rates: 4.9%, 18.2%, and 0.4%, respectively, for experiencing physical, psychological, and sexual IPV, which are also substantially lower than the past 4-month IPV victimization rates from a community study conducted in Beijing, namely, 25.8%, 45.4%, and 14.4%, respectively, for physical, psychological, and sexual IPV (Hou et al., 2011). One possible reason for these lower than expected rates is that the survey was conducted by the government agencies that might have inadvertently affected respondents’ willingness to report being victimized by their spouse, which might be perceived as politically incorrect and socially undesirable. With respect to controlling behaviors, there are no national or regional estimates readily available for comparison. Although one recent study from southern China included a number of controlling behaviors, no prevalence rates were reported for the studied controlling behaviors (Lin et al., 2018).
In spite of these possibly underreported IPV victimization rates, considerable evidence emerged from this study unequivocally indicated that, regardless of sociodemographic characteristics, all types of lifetime IPV victimization significantly elevated married respondents’ depressive symptoms in Sichuan, China with two exceptions for married men. As reported previously, personal control and sexual IPV experienced by married men did not significantly affect their depressive symptoms as the stand-alone measures of IPV victimization. In the case of sexual IPV victimization, the sample size was so small that the regression estimate could be unreliable. Nevertheless, given the patriarchal hierarchy and unequal gender roles in Chinese families and marital relationships (Ji et al., 2017), using violence to control the husband both personally and sexually by the wife would be extremely unlikely. However, by combining controlling behaviors and intimate partner violent acts experienced by married men to approximate severity of IPV victimization, both composite measures were significantly and positively associated with depressive symptoms. For married women, the husband’s personal and financial controlling behaviors along with multiple types of intimate partner violent acts against the wife (e.g., physical, psychological, or sexual IPV) elevated married women’s depressive symptoms both individually and collectively, irrespective of sociodemographic backgrounds. Taken together, these insights expand our understanding of the pernicious effects of multiple types of lifetime IPV victimization on the mental health of married men and women in contemporary China.
The secondary goal of this investigation was to critically assess gender variations in the effects of multiple types of lifetime IPV victimization on depressive symptoms. As noted previously, there were more gender symmetric than gender asymmetric patterns across multiple types of IPV victimization. For example, this study revealed gender asymmetric patterns in financial controlling behavior against men and physical as well as sexual IPV against women. Even though both anecdotal and research evidence support the tendency for Chinese wives to control their husbands’ access to family finance in postreform China (e.g., 60% of Chinese women reportedly controlled family finances in 2016; see Yan, 2016), a gender asymmetric pattern in sexual IPV victimization must be interpreted with care as only four men and 26 women reported experiencing sexual IPV. As a cautionary note, social desirability must be taken into consideration as well when rendering substantive interpretations. In terms of physical IPV victimization, it was clear that more married women than married men from this study reported experiencing this particular type of IPV, which echoes previous research findings (Chen & Chan, 2019).
While married women reported significantly higher levels of depressive symptoms than did married men, the effects of multiple types of lifetime IPV victimization on past 30-day depressive symptoms did not significantly differ by gender. This gender parity was uniform across all victimization measures, including controlling behaviors and intimate partner violent acts in terms of prevalence and severity. With these findings in mind, it is concluded that IPV victimization as a source of stress can have similar deleterious effects on all married individuals’ mental health regardless of gender and sociodemographic backgrounds. This key gender-neutral pattern is not only congruent with prior research conducted among older adults in postreform China (Dong et al., 2008; Yan & Tang, 2001) but also consistent with the research findings from the West (Coker et al., 2002; Pico-Alfonso et al., 2006). However, these gender-neutral findings are highly unanticipated in the wake of the resurgence of traditional gender norms and gender inequalities in both the public and private spheres in the postreform era (Ji et al., 2017; Sun & Chen, 2015). Well-designed replication studies using nationally representative surveys are recommended. In addition, since the IPV incidents occur in the dyadic relationships, the gender-neutral findings reported here concerning the effects of IPV victimization on depressive symptoms should be replicated as well by incorporating IPV perpetration in future research.
By design, this study is a secondary analysis of the survey data collected by the Chinese government agencies. As a result, there are several data-related limitations. One of the notable limitations to this study is that the measurement of depressive symptoms did not come from a standard instrument such as CES-D, albeit the indicators are comparable with the items included in CES-D. Moreover, alternative mental health measures (other than depressive symptoms) were not included in the survey. This lack of alternative mental health measures might have yielded research bias as gender difference is more salient in depression or depressive symptoms irrespective of the location, method of assessment, and research measurement (Salk et al., 2017; Winstok & Straus, 2014). Multiple instruments to measure mental health outcomes are recommended for future research.
Second, the indicators of controlling behaviors and intimate partner violent acts included in the survey are limited, which generated lower than expected reliability coefficients for the IPV victimization index variables. A full range of such measures included in the WHO violence against women instrument is recommended. This instrument features seven indicators of controlling behaviors, six indicators of physical IPV, four indicators of psychological IPV, and three indicators of sexual IPV (Ellsberg & Heise, 2005; García-Moreno et al., 2005). These multiple indicators can help improve the instrument’s measurement reliability (DeVellis, 2016).
Third, it is important to note that the survey used in this study did not include direct measures of IPV perpetration as incorporated in the Conflict Tactics Scales (CTS; see Straus et al., 1996). Neither did the survey ask questions that can be utilized to gauge the contexts and motivations of engaging in IPV. These limitations are noteworthy for two specific reasons. First and foremost, since the IPV incidents occur in the relationships that involve two acting partners, the experience of IPV victimization may implicitly imply IPV perpetration by the intimate partner. However, to better understand the dynamics and consequences of IPV, both partners’ reports regarding their experiences of IPV perpetration and victimization are highly desirable (see Neal & Edwards, 2017). To this end, CTS can be used to gauge both respondents’ as well as partners’ IPV perpetration and victimization concurrently such that the linkages between IPV perpetration and depressive symptoms can be investigated as well in postreform China. Second, given the patriarchy family system and pervasive gender inequalities in contemporary Chinese marriages (Pimentel, 2006), it would be erroneous for this study to assume that Chinese wives are as violent as their husbands without systematic knowledge about both partners’ motivations to engage in IPV. The mixed methods that incorporate in-depth interviews with both partners can help gather such important information to fully understand the perceptions, contexts, motivations, and consequences of IPV perpetration in addition to IPV victimization.
Another visible limitation is a possible underreporting problem for personal controlling behavior and sexual victimization, especially for married men. These underreporting tendencies are also observed in similar studies conducted in other Asian countries for women who serve as a reporting spouse (Xu et al., 2019). Future research can benefit from concerted efforts to avoid or minimize possible underreporting problems by using self-administrated questionnaires or laptop computers to ensure and maximize privacy, which may help facilitate more honest and accurate reporting.
Moreover, the survey utilized in this study did not include questions that could help ascertain respondents’ cohabitational experience or status. Consequently, respondents who were in cohabitational union at the time of interview were excluded, thus limiting the generalizability of the study findings to those who are romantically involved but not formally married. Future research should consider IPV and its mental health consequences in this type of intimate union as premarital cohabitation has increasingly become commonplace in postreform China (Yu & Xie, 2015).
Finally, resembling all cross-sectional studies, the associations between multiple types of lifetime IPV victimization and past 30-day depressive symptoms reported in this study are not necessarily causal. Suffice it to say that until the onset of IPV and depression can be determined, the causal relationship between IPV victimization and depression will remain unclear. In fact, the relationship between IPV victimization and depression can be reciprocal (Devries et al., 2013; Lin et al., 2018). Thus, panel studies are needed in the future to address these potential causal and/or reciprocal relationships.
To summarize, like many countries around the world, IPV is a complex experience of violence in postreform China. As indicated in this study, the concomitance or cooccurrence of multiple types of controlling behaviors, physical, psychological, or sexual IPV experienced by married men and women can indeed increase their depressive symptoms. Therefore, viewing IPV as a single category of violence is not only simplistic but also inappropriate. The different experiences of controlling behaviors, physical, psychological, and/or sexual IPV must be taken into consideration holistically when evaluating the impacts of IPV victimization on mental health. This is true for both married men and women. As such, focusing on women alone is far from realistic in postreform China. Stated differently, focusing on one gender for the study of IPV, interventions aimed at violence prevention, and mental health treatment can lead to inaccurate interpretations of violence and, more importantly, missed opportunities for violence prevention and treatment. Health professionals, governmental officials, and researchers are strongly encouraged to focus on both married men and women in their IPV and mental health intervention, prevention, and treatment endeavors in postreform China.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Sichuan University (2018hhf-07 and 2020zy-gg8).