
Abstract
Medical personnel such as those working in emergency medical systems are in direct contact with the patient or the injured and are exposed to workplace violence. This study aimed to determine workplace violence against prehospital paramedical personnel and factors related to this type of violence in Iran. The cross-sectional study was conducted in 72 prehospital emergency centers affiliated with Kerman University of Medical Sciences in 2019. Using a researcher-made questionnaire, we assessed workplace violence and factors associated with this type of violence in prehospital paramedical personnel with a census method (N = 308). Data were analyzed using descriptive statistics including mean and standard deviation (SD), frequency, percentage, and analytic statistics, such as the Kolmogorov–Smirnov, ANOVA, t test, and multiple linear regression tests. The results of this study showed that the most frequent types of workplace violence were verbal violence (47%), physical violence (32.50%), cultural violence (16%), and no violence (4.50%), respectively. From the perspective of paramedical personnel, the total mean score of workplace violence was at a moderate level (52.19 ± 10.72). The most important factors affecting workplace violence from the perspective of paramedical personnel were “lack of awareness of people about the duties of emergency medical personnel” and “lack of specialists in prehospital (city or road) bases.” Majority of the paramedical personnel believed that “no reaction and observance of patients and their families’ rights” were the most important types of reactions. They also believed that violence was normal at the workplace and should not be considered in emergency medical services. Results suggest that national and local policies in Iran should provide prehospital paramedical personnel with various training courses about how to decrease the rate of workplace violence, promote public health, and decrease their psychological stresses and occupational burnout.
Introduction
Workplace violence (WPV) is a global problem and its prevalence is steadily increasing (Dehghan-Chaloshtari & Ghodousi, 2017). This type of violence is defined as any incident or situation in which a person is abused, threatened, or attacked at his or her workplace (Heydarikhayat et al., 2012). Based on the Iranian health care system, types of WPV include physical violence, verbal violence, and cultural violence. Physical violence is the use of physical strength against a person or group, including beating, kicking, slapping, stabbing, shooting, firing, throwing an object, spitting, pushing, scratching, pulling hair, hitting, grabbing, squeezing, twisting, punching, pinching or other similar things. Verbal violence is behaviors such as intimidating, insulting, humiliating and patronizing, cursing, screaming, cussing, bullying, yelling or berating, and slurring. Cultural violence is any harassment, humiliation, mockery, etc. due to ethnicity, race, language, religion, and place of birth that affect human dignity. In this study, cultural violence refers to any action regarding ridiculing the language, culture, appearance, and accent of participants (Dehghan-Chaloshtari & Ghodousi, 2017; Emam et al., 2018; Pourshaikhian et al., 2016).
Although violence occurs in all work environments, health workers are more exposed to WPV (Sheikhbardsiri et al., 2017). WPV affects people’s self-esteem and quality of work and causes inequality, discrimination, disorder, and conflict at workplace (Hosseinikia et al., 2018). It should be noted that violent acts have devastating physical and psychological effects on personnel, the most important of which are discomfort, hopelessness, fear, depression, feelings of insecurity, unwillingness to continue working, and even physical injuries (Jiao et al., 2015). It has also been found that violent acts can have undesirable effects on the quality of health care personnel and cause neglect of the necessary care for patients (Sheikhbardsiri et al., 2017).
Recently, WPV in the health system has become an important issue in policymaking. The hospital and prehospital personnel, nurses, and physicians are at greater risk of WPV (Hosseinikia et al., 2018; Sheikhbardsiri et al., 2017). Statistics show that annually 70%–80% of the physicians, nurses, emergency medical personnel, and public service staff experience one or more cases of violence (Dehghan-Chaloshtari & Ghodousi, 2017). Despite the importance of the role of hospital and prehospital personnel, health systems cannot ensure the safety of frontline personnel against WPV (Hosseinikia et al., 2018; Maguire et al., 2018).
Prehospital paramedical personnel are trained to provide medical care or interventions for injured or ill persons. They are the first ones who respond to the emergency needs of people, work in various critical situations, and react appropriately to transport patients safely to medical centers. Sometimes, they may encounter threats and violent reactions in these unstructured environments (Bernaldo-De-Quirós et al., 2015; Iranmanesh et al., 2013; Petzäll et al., 2011). Researches in recent years show that the increasing prevalence of WPV against prehospital paramedical personnel has become a threat to the emergency care system(Bigham et al., 2014). Risk of violent assault may be heightened because prehospital personnel work in isolated and uncontrolled environments, are in contact with the public and people in distress, and are associated with valuable or desirable items such as drugs, syringes/needles and expensive equipment, and patient-induced violence can occur quickly because of the nature of their work and proximity to patients (Gormley et al., 2016; Taylor et al., 2016).
Literature Review
Dadashzadeh et al. (2019) studied Iranian pre-hospital nurses’ strategies to manage WPV and showed that they received little training and insufficient support, and were poorly prepared to manage WPV. Another study addressed prehospital personnel’s perception of verbal abuse and the associated factors in three regions in the south of Chile and showed that 51.4% of the professionals and 46.6% of the paramedical technicians were verbally abused during last year. In total, 17.6% of the paramedical technicians and 13.5% of the professionals perceived verbal abuse (Campo & Klijn, 2017). A study was conducted in Riyadh, Saudi Arabia to evaluate the prevalence of WPV (physical and verbal) among emergency medical services (EMS) workers and the results showed that 65% of the respondents experienced WPV. Verbal abuse (61%) was the most common type of violence reported. The majority of the attackers were patients’ relatives (80%) followed by patients themselves (51%) (Alharthy et al., 2017). Benjamin et al. in India studied WPV among prehospital care providers and showed that the overall prevalence of any WPV was 67.9%. The prevalence of physical violence and verbal violence was 58% and 59.8%, respectively (Lindquist et al., 2019).
The Research Aim and Questions
Despite the great importance of WPV and its destructive effects, this problem has not yet been taken into account seriously in the Iranian healthcare system. Therefore, the purpose of this study is to investigate WPV against prehospital paramedical personnel in emergency medical centers of Kerman University of Medical Sciences. In other words, the present research attempts to answer the following questions: (a) what is the level of WPV in prehospital paramedical personnel? (b) Is the level and type of WPV different in terms of the demographic characteristics of the participants? (c) What are the most important factors affecting the WPV from the perspective of prehospital paramedical personnel? (d) What are the most important types of reactions of paramedical personnel to WPV? (e) What are the most important reasons for the reaction to WPV from the perspective of prehospital paramedical personnel? The results of this study can help community health authorities and managers of the health services organization reduce violence against prehospital paramedical personnel thorough promoting good relationship between prehospital paramedical personnel and people of the community including patients and their families.
Method
Design
The Ethics Committee of Kerman University of Medical Sciences approved this study. A cross-sectional design was employed in 2019. The code of ethics is IR.KMU.REC.1399.379.
Respondent Characteristics and Setting
The target population of this study was paramedical personnel working in the EMS centers. By using a census method, the sample size included 308 paramedical personnel from road (N = 205), and urban (N = 103) prehospital bases supervised by Kerman University of Medical Sciences. Confidentiality was kept by putting no name or other personal information in the questionnaires. The coresearchers distributed the questionnaires to the participants in prehospital emergency centers who filled in the questionnaires during their working hours. In total, 308 questionnaires were distributed; 223 questionnaires were returned of which 23 incomplete questionnaires and 85 other ones were excluded because of no delivery. The overall response rate was 72.4%.
Inclusion and Exclusion Criteria
Inclusion criteria consisted of participants with a bachelor’s degree in nursing or an associate degree or bachelor’s degree in prehospital emergency nursing, at least one year of work experience in a prehospital emergency center, and their willingness to participate in the study; exclusion criteria included lack of consent for participating in the study and incomplete questionnaires.
Data Collection
For data collection, the research team initially developed a questionnaire after an extensive review of the relevant literature to achieve good content validity (Amini et al., 2020; Dadashzadeh et al., 2019; Hosseinikia et al., 2018; Pourshaikhian et al., 2016; Rahmani et al., 2012; Sahebi et al., 2019). We developed the Persian questionnaire for Persian-speaking study participants. The questionnaire has four parts. The first part is about the demographic characteristics of the personnel including age, sex, education level, marital status, work experience, type of base (city and road), number of missions, working hours, and employment status. The second part contains 18 items to investigate WPV including physical violence with 6 items, verbal violence with 7 items, and cultural violence with 5 items based on a five-point Likert scale (1 = never, 2 = seldom, 3 = sometimes, 4 = oftentimes, and 5 = always). The minimum score was 18, and the maximum score was 90. Scores ranging from 18 to 42 would be considered low WPV, scores ranging from 43 to 66 would be considered moderate WPV, and scores ranging from 67 to 90 would be considered high WPV. The third part assesses the most important factors affecting WPV from the perspective of prehospital paramedical personnel and the fourth part assesses the types of reactions of the prehospital paramedical personnel to WPV, and their reasons for the reaction to this type of violence.
Ten professors of Kerman University of Medical Sciences (emergency medicine physician, community health nurse, psychological health physician, and social medical expert) approved the content validity of the questionnaire. A pilot study was conducted on the questionnaire of the WPV to determine the reliability; 30 paramedical personnel not involved in the study process were asked to complete the questionnaire. Cronbach’s α coefficient was applied to assess reliability; according to the results, Cronbach’s α coefficient was (α = .87).
Data Analyses
Data were analyzed using descriptive statistics, including mean and SD, frequency, percentage, and analytic statistics, such as Kolmogorov–Smirnov test, to indicate whether the data were sampled from a population with a normal distribution (Table 1). The independent t test and one-way ANOVA were used for comparative of WPV mean score base of participant’s demographic characteristics also multiple linear regression was used to determine the impact of demographic variables on WPV using the version 20, SPSS Inc., Chicago, IL software. There was a significant difference at the level of p < .05.
Test of Normality (Kolmogorov–Smirnov).
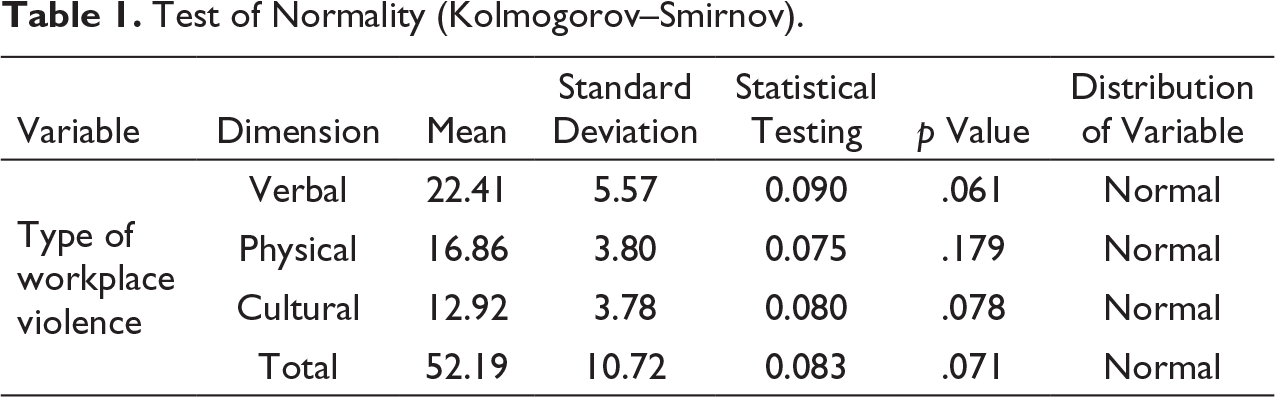
Note. Bold values are significant at the level of p < .05.
Results
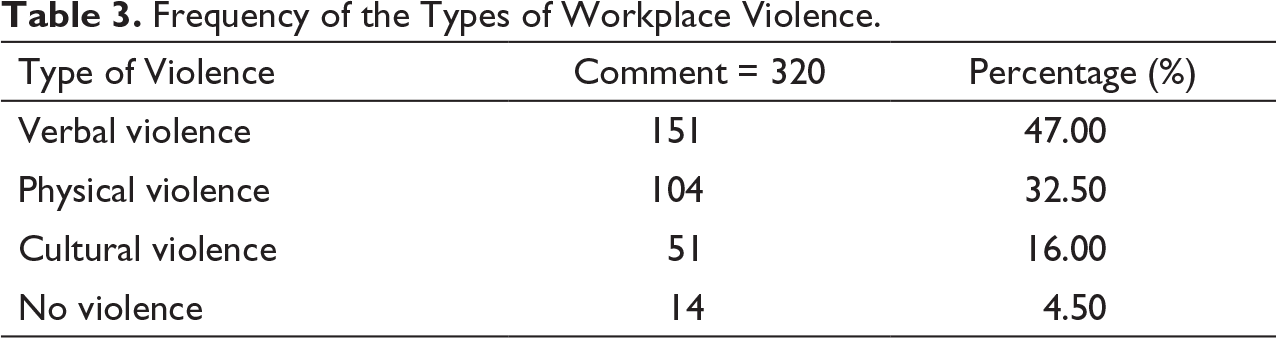
In this study, all participants (n = 200) were male and the majority of them (N = 95, 47.5%) had Associate Degree’s in nursing. Other demographic characteristics are listed in Table 2. Base of collected comments 320 of participants for reason multiple-choice questions, the results showed that the most frequent types of WPV were verbal (47%), physical (32.50%), cultural (16%), and no violence (4.50%), respectively, (Table 3). According to the results, the total mean scores of WPV from the perspective of paramedical personnel was at a moderate level (52.19 ± 10.72).
Demographic Characteristics of the Research Sample.

Frequency of the Types of Workplace Violence.
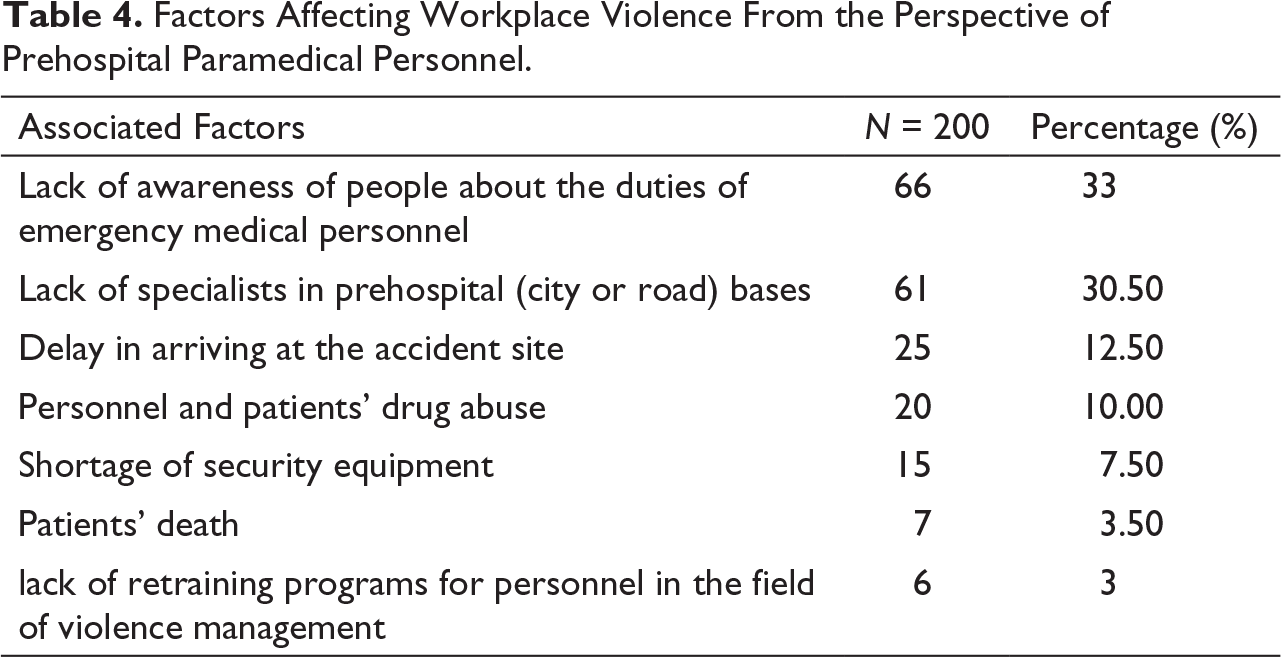
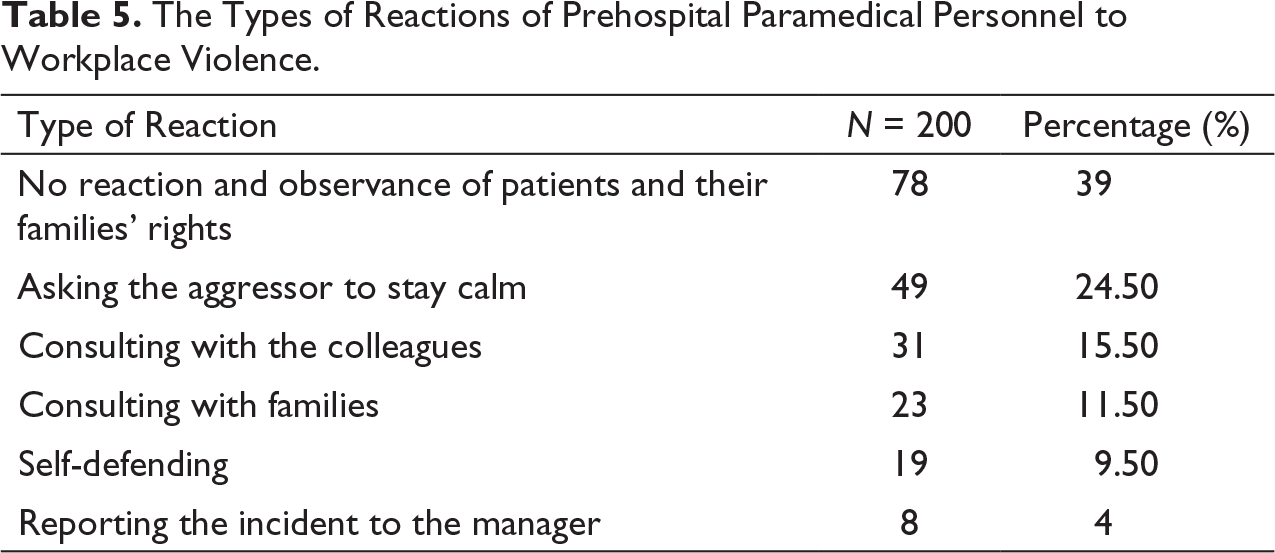
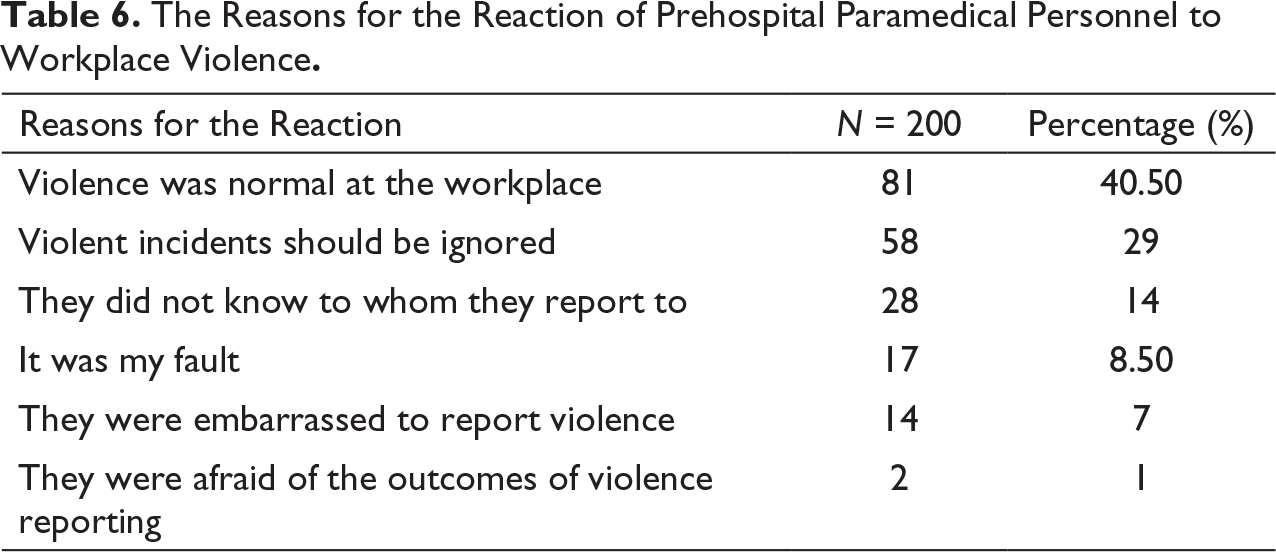
The results showed that the most important factors affecting WPV were “lack of awareness of people about the duties of emergency medical personnel” and “lack of specialists in prehospital (city or road) bases” the least important factors were “lack of retraining programs for personnel in the field of violence management” and “patients’ death” (Table 4). The majority of paramedical personnel (N = 78, 39%) believed that “no reaction and observance of patients and their families’ rights” were the most types of reactions to WPV (Table 5). Furthermore, the majority of participants (N = 81, 40.5%) reported that violence was normal in their workplace (Table 6).
Factors Affecting Workplace Violence From the Perspective of Prehospital Paramedical Personnel.
The Types of Reactions of Prehospital Paramedical Personnel to Workplace Violence.
The Reasons for the Reaction of Prehospital Paramedical Personnel to Workplace Violence.
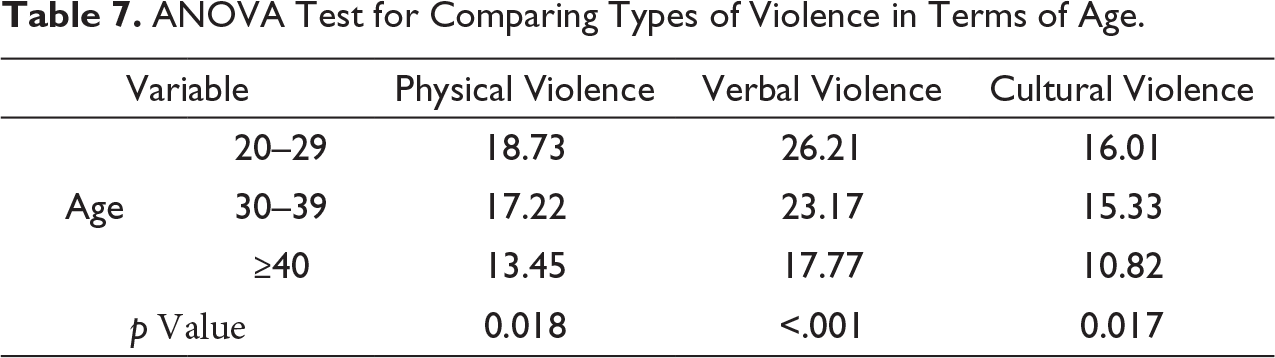
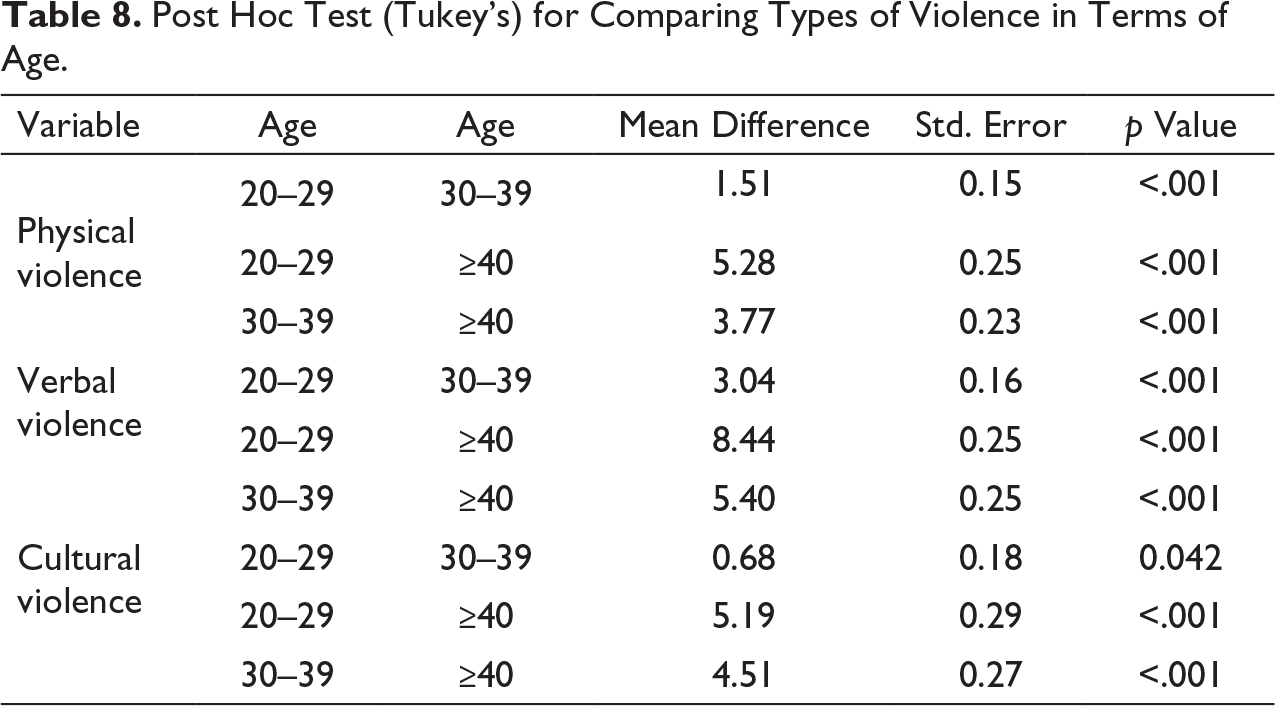
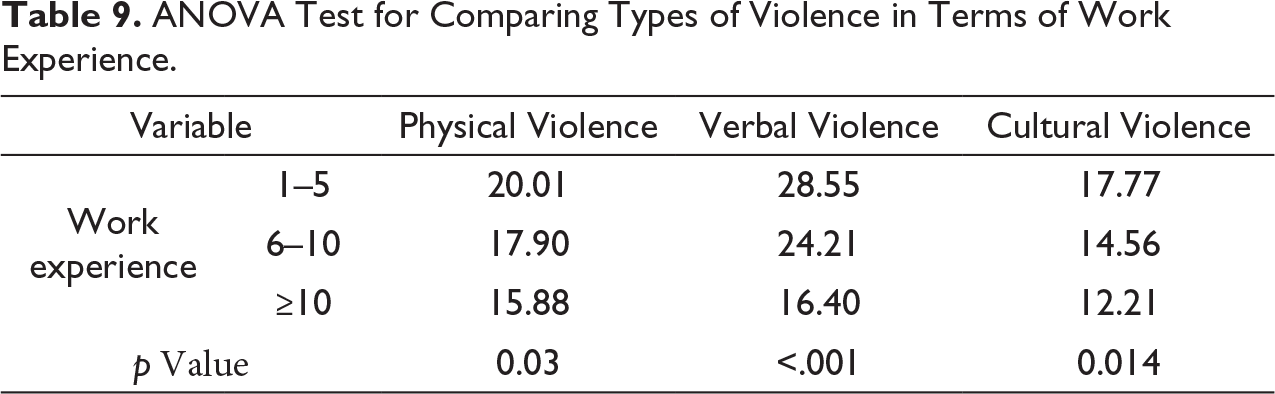
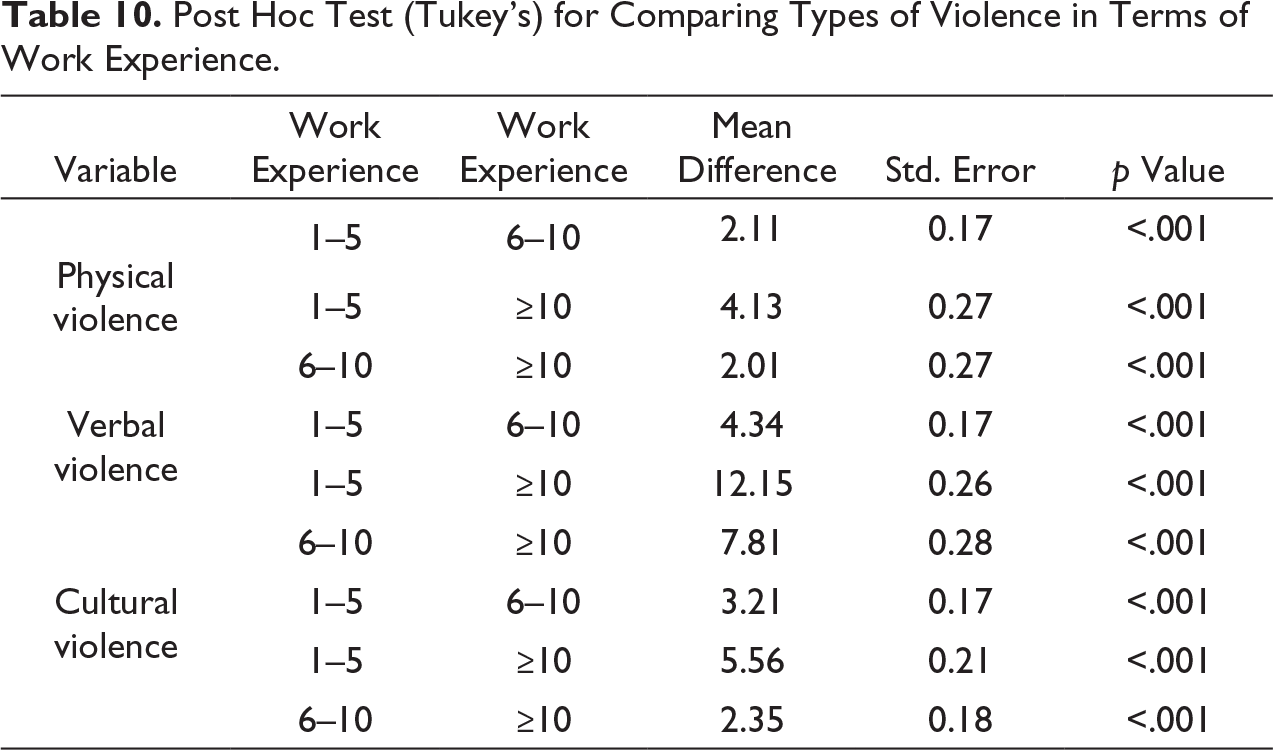
The ANOVA test showed a statistical difference between the age variable, physical violence (p = .018), verbal violence (p < .001), and cultural violence (p = .017). Post hoc test (Tukey’s) showed that the paramedical personnel aged above 40 years had the least exposure and 20- to 29-year-old paramedical personnel had the most exposure to the WPV (Tables 7 and 8).The ANOVA test showed a significant difference between the work experience variable, physical violence (p = .03), verbal violence (p < .001), and cultural violence (p =.014). Post hoc test (Tukey’s) showed that the paramedical personnel with more than 10 years of work experience had the least exposure and paramedical personnel with 1–5 years of work experience had the most exposure to the WPV (Tables 9 and 10).
ANOVA Test for Comparing Types of Violence in Terms of Age.
Post Hoc Test (Tukey’s) for Comparing Types of Violence in Terms of Age.
ANOVA Test for Comparing Types of Violence in Terms of Work Experience.
Post Hoc Test (Tukey’s) for Comparing Types of Violence in Terms of Work Experience.
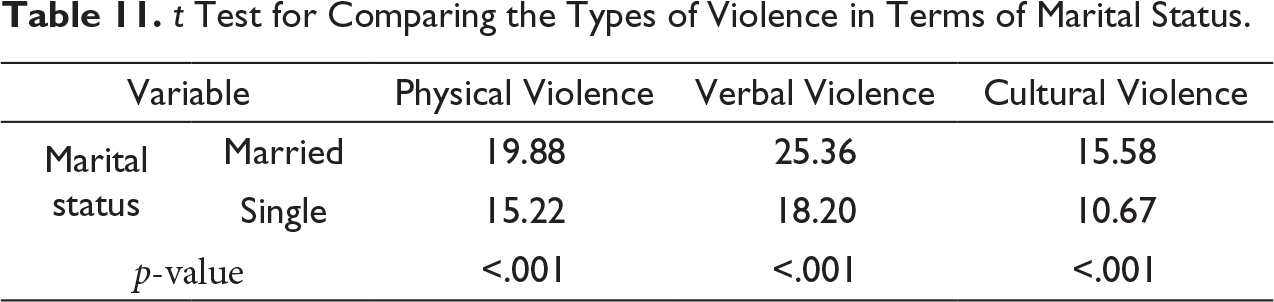
The t test showed a statistically significant difference in the mean scores of physical violence (p < .001), verbal violence (p < .001), and cultural violence (p < .001) in terms of marital status, so that the single paramedical personnel were exposed to the least WPV compared with the married personnel (Table 11).
t Test for Comparing the Types of Violence in Terms of Marital Status.
The Multiple linear regression showed a negative relationship between WPV, age, and work experience. So that with increase age and work experience decreased WPV among employees. Between these variables based on β coefficient, work experience had the most impact on WPV among paramedic personnel. Also, the Multiple linear regression showed a significant relationship between WPV and marital status, so that WPV between married personnel was more than singles (Table 12). No statistically significant difference was found between other demographic variables and various types of WPV.
Multiple Linear Regression: Impact of Age, Work Experience, and Marital Status on Violence.

Note. There was no multicollinearity (tolerance = 0.645, VIF = 2.102).
Discussion
Everyone is worried about the increasing prevalence of WPV, which involves physical, verbal, cultural, racial-ethnic, and sexual violence (Emam et al., 2018). The results of this study showed that most paramedical personnel in (city or road) medical bases were exposed to verbal violence and the total mean score of the WPV from the perspective of paramedical personnel was at a moderate level. These results are consistent with the results of studies conducted by (Alharthy et al., 2017; Emam et al., 2018; Franz et al., 2010; Gormley et al., 2016; Zampieron et al., 2010). They showed the prevalence of verbal violence between 20% and 90%. The possible reason for the high frequency of verbal violence is that patients’ families are afraid of losing their patients because prehospital paramedical personnel may not deliver the patients to the nearest medical center. The low level of cultural violence in this study is that Kerman University of Medical Sciences selected native paramedical personnel at road and urban bases, so most respondents had the same culture.
The results of the present study showed that the most important factor in the occurrence of WPV was the lack of awareness of people about the duties of the prehospital paramedical personnel. This result is consistent with the results of studies conducted by (Dehghan-Chaloshtari & Ghodousi, 2017; Hosseinikia et al., 2018). Many people do not have a correct perception of the responsibilities of prehospital paramedical personnel and in many times cannot distinguish physicians from the paramedical personnel and expect an appropriate treatment and the prescription of various medications for their patient, and when such an expectation is not satisfied, they display violent behavior. In addition, results of the study showed that the least important factor affecting the incidence of violence was lack of retraining programs for personnel in the field of violence management. The probable reason for this result is that the Emergency Management Training Center in Kerman University of Medical Sciences has done for all personnel (including upon arrival) one-month training courses, which includes how to communicate with the patient, their families and the injured, and also other required training items for performing a prehospital successful job mission in city and road bases.
The results of this study also indicated that the paramedical personnel’s no reaction and observance of patients and their families’ rights were the most important types of reactions to the violence s. This result is in line with the studies of (Gates et al., 2006; Talas et al., 2011). A possible reason may be that prehospital personnel have expected violence from the patient and his/her family (because patients are not psychologically and physically in good condition and their relatives are anxious and concerned about them); therefore, they prefer not to respond to such violent behaviors and attempt to make the attacker calm.
In response to the question, what are the most important reasons for the reaction to WPV? Most participants reported that this was not an important issue and considered the WPV a part of their occupation and there was no need to pay attention to it. These results are line with the studies of (Alharthy et al., 2017; Heydarikhayat et al., 2012). They showed that only 10% of the personnel reported the incidence of violence. Those who did not report violence believed that reporting was useless, caused trouble, did not help change the current condition and prevent occupational violence.
The results of the present study showed a negative relationship between the age, work experience, and WPV in paramedical personnel. This result is line with the studies of (Alharthy et al., 2017; Dehghan-Chaloshtari & Ghodousi, 2017; Ghasemi et al., 2009; Mozafari & Tavan, 2013). With increasing age and work experience, the paramedical prehospital personnel can gain important skills to reduce violence including emergency scene management, anger management techniques and patient relaxation techniques especially the patient’s family in stressful conditions.
Our results also showed a significant relationship between the marital status and WPV. The incidence of violence in married individuals is higher than that of the single individuals. (Aghajanlou et al., 2010; Paryad et al., 2015) reported a statistically significant difference between the incidence of physical violence and marriage. The increased level of violence observed among the married individuals in the present study may be due to the insults made by patients and their companions or other people in the prehospital emergency against the family members of the staff, which may expose them to physical violence.
Strengths and Limitations
A strength point of this study is that it addressed WPV in a different society of Iranian health system that past studies have rarely dealt with all dimensions of WPV against prehospital paramedical personnel and rarely have considered factors related to this type of violence at EMS in all provinces of Iran. The present study had some limitations. First, the study could not investigate other important factors causing violence of the patients and their families against emergency medical personnel. Second, the data were collected retrospectively, which might lead to recall bias. Accordingly, qualitative research should be conducted in this regard.
Conclusion
The present study showed that prehospital paramedical personnel were exposed to a variety of occupational violence, including verbal, cultural, and physical violence. Regarding the high workload of prehospital personnel in urban and road bases in Kerman province, and various daily missions, and direct contact with various patients and their relatives, they are exposed to all kinds of violence. Therefore, the Ministry of Health and Emergency and Disaster Management Center should pay particular attention to this group of personnel and provide necessary training to familiarize the community with the prehospital personnel through national media. Furthermore, they should select personnel with specialized skills for this profession who have to complete an educational course. Further studies are suggested to examine the causes of violence against emergency medical personnel from the viewpoint of patients and their relatives.
Footnotes
Acknowledgments
We would like to thank all the people who helped us to perform this study, especially paramedic personnel of Kerman Medical Emergency Management Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.