
Abstract
Women in South Asia face the highest lifetime prevalence of intimate partner violence in the world, which is just one form of violence against women (VAW). In India, few women seek help after experiencing violence, particularly from formal resources, such as physicians or the police. While many studies have investigated the impact of survivor characteristics and patterns of violence on help-seeking behaviors, there is scant research on support service characteristics and their impact on help-seeking. The introduction of a novel crisis helpline in Gujarat, India provided an opportunity to better understand how successful help-seeking can be driven by the perceived and experienced characteristics of the helpline. We conducted in-depth interviews with helpline users to identify factors and pathways that promoted or discouraged help-seeking in general, help-seeking from a formal source, and help-seeking from this particular helpline. We analyzed 32 interviews of women who used the helpline. Participants were from eight districts across the state, representing a diverse range of sociodemographic backgrounds. After conducting a thematic analysis, we found that action-oriented service, timeliness, and women-focused staff influenced (positively and negatively) participants’ feelings of safety, empowerment, and trust in the helpline, which ultimately impacted their decision to seek help from the helpline or even to seek help at all. This study illuminates how service characteristics, in and of themselves, can influence the likelihood that survivors will seek help, emphasizing the need for survivors to have a voice in the growth and refinement of VAW support services. Consequently, these areas must be a focus of future research and initiatives to improve help-seeking by VAW survivors.
Keywords
Introduction
Globally, at least a third of women experience intimate partner violence during their lifetimes (World Health Organization, 2013). Intimate partner violence is one form of violence against women (VAW; Kilpatrick, 2004). VAW encompasses a broad range of violence, including physical, sexual, and psychological violence, as well as deprivation and neglect. VAW may be perpetrated by partners or non-partners, including family members, friends, and strangers. Experiencing VAW can have serious long-term impacts on physical and mental health, and broadly contributes to morbidity and mortality in low- and middle-income countries (LMIC). Numerous studies show that among VAW survivors, there is less contraceptive and condom use (Stephenson et al., 2008), less breastfeeding (Shroff et al., 2011), less perinatal care usage (Koski et al., 2011), and an elevated risk of having low birth weight babies (Murphy et al., 2001). VAW survivors face an increased risk of hypertension (Campbell, 2002; Coker et al., 2002), chronic mental illness (Campbell, 2002), HIV (Silverman, et al., 2008) and other sexually transmitted infections (Chowdhary & Patel, 2008; Sudha & Morrison, 2011).
Women in South Asia face the highest lifetime prevalence of intimate partner violence (43%) in the world (World Health Organization, 2013). Beyond intimate partner violence alone, women in South Asia face a range of VAW that is often perpetrated by non-partner family members with whom women live, such as in-laws (Fernandez, 1997; Ragavan & Iyengar, 2017; Raj et al., 2006). The burden of VAW bears heavily on India where over 650 million women reside, nearly one-fifth of the world’s female population (Lanka et al., 2014). Moreover, women experience culture-specific forms of VAW that are uncommon outside of India, such as dowry-related harassment and bride burning (Kumar & Kanth, 2004; Peck, 2012; Rastogi & Therly, 2006). The persistence of pervasive VAW is enabled by deeply entrenched norms as seen by high numbers of both men and women considering violence by husbands against wives to be justified (Lanka et al., 2014). Moreover, legally, India has only recently defined domestic violence more broadly under the law with the Protection of Women from Domestic Violence Act in 2005, which is now inclusive of physical, sexual, verbal, emotional, and economic abuse. Advancement of legal protections is a substantive and positive step, but it must be coupled with increased efforts to support women reporting VAW. Consequently, to prevent future violence and mitigate the extensive physical and psychological health consequences associated with VAW, it is critical to better understand how women seek help for VAW.
Help-Seeking by VAW Survivors
Many women who experience VAW do not seek help for their experiences (Ansara & Hindin, 2010; Cheng & Lo, 2015; Cho & Kim, 2012; Kaukinen et al., 2013; Lipsky et al., 2006). According to Liang et al.’s framework of help-seeking, there are three main processes that survivors must undergo when deciding to seek help for violence (Liang et al., 2005). First, survivors must identify and define the problem at hand. Second, they then must decide that they will seek help for said problem. Finally, they must select the form and source of support that they wish to pursue. Each of these steps influences the overall decision-making process when seeking help for VAW; each is influenced by individual, interpersonal, and sociocultural factors; and consequently they each hold the potential to be points of influence to increase survivors’ help-seeking (Liang et al., 2005).
Multiple individual and sociocultural factors can influence help-seeking, including race, age, education level, financial status, immigration status, and severity of abuse (Cho et al., 2017; Hurwitz et al., 2006; Kaukinen et al., 2013) Help-seeking may also be dependent on the patterns of violence. A US-based national survey regarding experiences of intimate partner violence, non-partner sexual violence, and stalking demonstrated that patterns and particular consequences of victimization (i.e., physical, psychological, and sexual victimization, and physical and mental health consequences) significantly influenced help-seeking choices and behaviors (Cho et al., 2017). Another study found that women who experience physical or sexual violence, especially over extended periods of time, are more likely to seek help than those who experience emotional violence alone (Duterte et al., 2008). Furthermore, women often will seek and receive advice from family members, friends, or strangers before deciding to seek help from formal sources, such as the police. The advice received and the subsequent decision regarding help-seeking from formal sources, are significantly influenced by the relationships between the victim, perpetrator, and advisor (Knoth & Ruback, 2019).
In India, less than 25% of women ever report the physical and/or sexual violence they experience (International Institute for Population Sciences [IIPS], 2017). A study examining reporting rates in 24 developing countries found India to have one of the lowest reporting rates (Palermo et al., 2014). Help-seeking attempts are often only initiated if the abuse becomes severe or public to the extent where the woman feels she is no longer able to remain silent about the incident(s) (Decker et al., 2013). Similar to other countries, research in India demonstrates associations between characteristics of violence and sociodemographic factors as key determinants of help-seeking (Leonardsson & San Sebastian, 2017). Women who experienced a combination of physical, sexual, and emotional abuse were the most likely to seek help and women who experienced sexual violence alone were the least likely to seek help (Leonardsson & San Sebastian, 2017). Whether the acts of violence resulted in injury or were considered severe were some of the strongest predictors of help-seeking behaviors. Moreover, women who were more educated, adhered to a minority religion, married later in life, or lived in southern India, rather than in northern or northeastern regions, were more likely to seek out support and help for intimate partner violence (Leonardsson & San Sebastian, 2017). Several additional cultural factors prevent Indian women from seeking help for VAW, including risks to family reputation, fear of increased violence from perpetrators, economic dependency on abusers, and societal norms of tolerance of domestic violence (Decker et al., 2013). In addition, when intersectionality is taken into account, different help-seeking patterns may emerge. For example, some have theorized that women who are more educated and reside in an urban setting may be less likely to seek help because they face increased social pressures (Mahapatro et al., 2014).
Those who do seek help predominantly reach out to informal sources such as family or friends. Only 5.7% of women experiencing violence have ever reported the violence they experience to a formal source (IIPS, 2017). Due to the predominantly multigenerational family structure and the family-centered culture in India (Ahmed-Ghosh, 2004), many survivors are more likely to seek informal, rather than formal, networks of support (IIPS, 2017). Women may only escalate to formal networks after support from informal networks is inadequate (Panchanadeswaran & Koverola, 2005). Both formal and informal supports have advantages and disadvantages; while informal networks are often more accessible and sometimes more socially acceptable, they may not provide the validation and understanding survivors are seeking due to social norms and cultural expectations (Sylaska & Edwards, 2011). Family members, friends, or neighbors may respond with shock, inaction, secret action, or shame, typically in an effort to avert family disgrace. As a result, women seeking to receive concrete long-term support and aid in escaping the violence they are facing, without having increased shame and stigma, may turn to and find more positive results from formal support networks (Panchanadeswaran & Koverola, 2005). However, formal networks may be challenging to access due to lack of available information about specific support resources, widespread mistrust of these support services, delays in obtaining help, a perceived lack of empathy, and even safety concerns in connecting with formal support sources (Davies et al., 1998; Decker et al., 2013). What is not well understood is how the availability and design of formal support services themselves influence survivors’ decision to seek help and from whom.
Support Services for VAW Survivors in India
Government departments and nonprofit organizations in India have been developing initiatives to connect women facing VAW with existing and new resources for several decades, with increased efforts in the last several years. Along with traditional police support, government services designed to address VAW include one-stop crisis centers, women’s police stations, and crisis support helplines. All-women police stations originated in the 1970s and expanded in the 1990s throughout India with the hope that police stations staffed primarily by women will help survivors feel more comfortable and secure, and encourage them to report acts of violence (Kethineni & Srinivasan, 2009). One-stop crisis centers, which have been established in multiple Indian states under the Nirbhaya Fund, are designed to provide medical and legal aid, police support, counseling services, and often temporary shelter at one convenient location for VAW survivors (Vij, 2018). However, these centers are sometimes underresourced, understaffed, and poorly integrated with medical and legal support services, adding additional stress to survivors in their time of need (Bajoria, 2017).
In January, 2013, the Indian Department of Telecommunications mandated that each state operate a women’s helpline to address the needs of women facing violence (Newberry et al., 2016). Gujarat was one of the first states to develop the required infrastructure and pilot its version of the helpline: 181 Abhayam. The helpline is meant to help any woman in crisis, anywhere, anytime. It is supported by a tripartite agreement between two state government departments—Department of Women and Child Development and the Home Department (police)—and a public–private emergency medical services provider: GVK Emergency Management and Research Institute (GVK EMRI). The helpline is available at all times, 24 hours a day, 7 days a week, year round. The helpline is staffed entirely by women counselors who are trained to provide support and connection to other services and organizations. They also dispatch rescue vans to meet women in the field to provide support and mediation, and occasionally transport or rescue. Vans are staffed with a female police officer and female counselor. Within the first 10 months, Gujarat’s 181 Abhayam helpline received 9,767 calls (Newberry et al., 2016). Since the helpline’s pilot, 181 Abhayam call center in Gujarat has seen consistent growth in call volume. In a country where few women report violence, women are reaching out to this helpline for mental health support and connection to broader resources such as legal aid, police intervention, economic support, and connection to other government resources and programs. As a result, Gujarat’s operation of 181 Abhayam has and continues to be a model for other states in India.
Research Questions
With the burgeoning growth of support services for women in India, it is critical to investigate actual help-seeking practices with respect to support services themselves within this specific cultural context. The introduction of a novel crisis helpline in Gujarat, India (Newberry et al., 2016) provided an opportunity to better understand how successful help-seeking can be driven by the availability and characteristics of support services themselves. We worked from a positive deviance approach to identify women who have successfully connected to a formal source of help (Marsh et al., 2004). A variety of fields including healthcare, education, and development have used positive deviance to understand the behaviors and strategies of individuals or organizations that successfully access resources or find solutions better than peers who face similar constraints and challenges (Baxter et al., 2019; Bradley et al., 2009; Marsh et al., 2004). It is a strength-based and human-centric approach. Specifically, we conducted in-depth interviews to answer the question: which factors and/or pathways promote or discourage help-seeking in general, help-seeking from a formal source, and help-seeking from this particular crisis helpline? We hope to use these findings to work with key stakeholders to implement quality improvement processes within the current crisis helpline and similarly VAW support services across India, other LMICs, or those working specifically with South Asian VAW survivors.
Methods
Design
Researchers conducted semi-structured, in-depth interviews to understand participants’ help-seeking decisions, specific experiences with the helpline, and the impact of those experiences on help-seeking. In-depth interviews were necessary for answering the research questions to garner information on individual experiences, decision-making processes, and motivations for behavior (Hennink et al., 2011). All aspects of the study were designed in accordance with the World Health Organization’s ethical and safety recommendations for research on VAW (Ellsberg & Heise, 2005; Watts, et al., 2001; World Health Organization, 2016).
Sampling and Recruitment
A total of 8 of the 33 districts in Gujarat were identified for participant recruitment [see Figure 1]. Districts were selected based on call volume, location type, and input from helpline program staff with the goal of having a representative and diverse sample. Selected districts represent the five regions of Gujarat: Kutch (Kutch), Saurashtra (Amreli, Rajkot), North Gujarat (Sabarkantha), Central Gujarat (Ahmedabad, Anand, Panchmahal), and South Gujarat (Surat). These districts included those with the highest call volume and major urban areas (Ahmedabad, Rajkot, and Surat) as well as areas with greater tribal population representation (Sabarkantha, Panchmahal, and Surat). District-specific recruitment lists were obtained from the helpline caller database maintained by the helpline. Recruitment lists contained names and contact information for women who were at least 18 years old, had called the helpline within the past six months, and had previously consented to a follow-up call from the helpline. These criteria guarded the safety of potential participants by ensuring that the research team only contacted women who had provided secure phone numbers and were aware that they may be contacted by the helpline. Women of all castes, religions, and socioeconomic classes who met the inclusion criteria were eligible to participate. Exclusion criteria included women below 18 years of age, women who had not previously consented to a follow-up call, women who did not speak Gujarati or Hindi, and calls documented as being made by third parties on behalf of women.
Map of Gujarat.
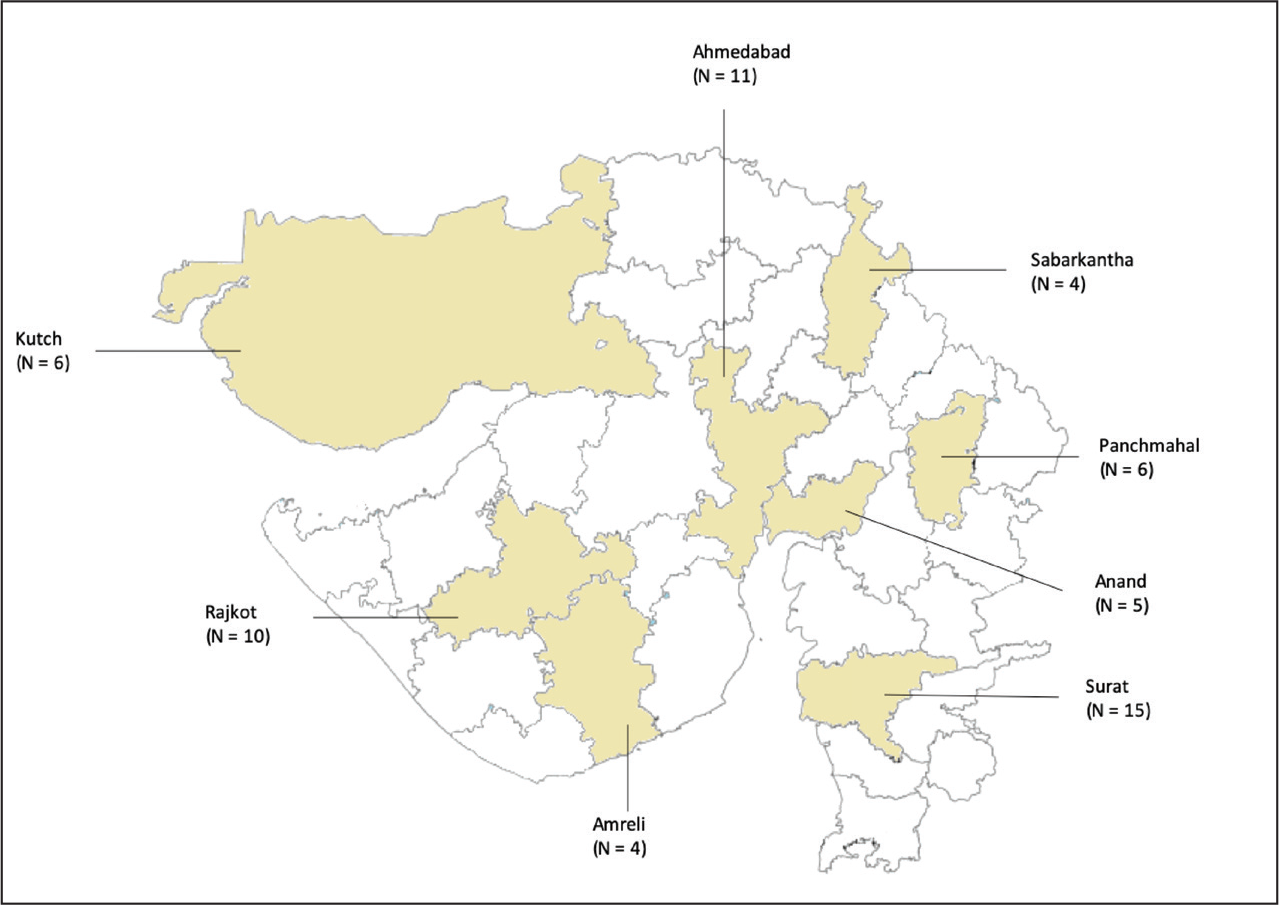
Six local research assistants, fluent in Gujarati and Hindi, were trained to complete participant recruitment, enrollment, and interviews. They called potential participants from the district-specific recruitment lists, which were generated from calls that occurred three to six months prior to potential enrollment and included only telephone numbers that women had specifically indicated were safe for follow-up calls. After consultation with helpline staff, the lag time was instituted to increase the likelihood that a participant had the opportunity to use any services to which they were referred. We used consecutive sampling, starting from the most recent caller on the list and contacting each caller moving chronologically backward until available interview times were full or there were no other callers to contact. Using an enrollment script, research assistants confirmed that they were speaking with the woman who had called the helpline and then informed her about the study. If a woman expressed interest in participating, the research assistant obtained oral consent over the phone and coordinated the date, time, and location for the interview. Oral consent was used so that participants of all literacy levels could understand the details of the study and feel comfortable with participation. We enrolled participants from July, 2017 to September, 2017.
Data Collection
Trained research assistants conducted in-depth interviews in Gujarati, the most commonly spoken language in Gujarat, and occasionally in Hindi. Before beginning each interview, the research assistants again reviewed the study purpose, risks, and benefits, and reconfirmed informed consent verbally in-person. Research assistants used semi-structured interview guides to conduct the interviews. Participants were asked about demographic characteristics, help-seeking prior to the use of the helpline, and on the day of using the helpline, expectations of the helpline prior to use, attitudes after using the helpline, impressions of the helpline, and areas of improvement for the helpline. Interview length ranged from 40 minutes to 2 hours, with a majority lasting 45–60 minutes. Most interviews were conducted in participants’ homes, per the request of the participants. All efforts to maintain participants’ privacy were made, including finding a private room within their home to conduct the interview or removing all others from the home if it was only a single room. In addition, the safety of participants and the research team remained a priority throughout the process. The research team spent significant training time discussing safety in recruiting, location scouting, and interview set-up (e.g., awareness of exits). We always had local contacts that knew when we were in the field and could assist at a moment’s notice, including involving the helpline itself or police. At the end of each interview, we turned off the recorder and asked if the participant had any additional concerns (including safety) or would like any additional resources, which we often had prepared or could find within 24 hours.
Analysis
We conducted a total of 61 interviews. Recordings were translated from Gujarati and/or Hindi to English. Then transcripts were deidentified prior to analysis. We conducted a thematic analysis as described by Braun and Clarke (2006), using a coding method to maintain internal validity and limit researcher bias (Saldana, 2015). We identified 11 of the 61 transcripts to use for code development, which had a broad demographic distribution and were representative of the demographic representation seen in the original sample. For these 11 transcripts, each researcher began by coding the transcript using an inductive approach. After every two transcripts, we systematically reviewed each transcript line-by-line, discussed and reconciled any coding differences, and finalized a codebook. We wrote analytic memos after each transcript to note themes from the transcript and to identify key findings. Through this team coding process, we finalized a set of codes to apply to the remaining transcripts. Remaining transcripts were divided equally between two different coders with the lead author acting as a second coder on every transcript. New codes were also developed in this process and added to the codebook. If we added a new code, all prior transcripts were re-reviewed for instances of that particular code. We continued to discuss theme identification and compare coding every three transcripts as we continued. This review process helped limit researcher bias and ensure that team members systematically applied the codes across transcripts (Saldana, 2015). As we proceeded, we strove to include more transcripts from young women, women from rural areas, and Muslim women as these groups were known to use the helpline less frequently than their counterparts. We achieved thematic saturation by the end of 32 transcripts (Strauss et al., 1998).
The interviews covered a range of domains surrounding the helpline and women’s individual experiences; however, this article focuses on the analysis specific to factors that promoted or discouraged a woman’s choice to seek help and the specific choice of help-seeking from the helpline. Ethical approval of the study was obtained from the Stanford Institutional Review Board (IRB #41616) and the Ethics Committee of GVK EMRI.
Results
Of the 61 participants interviewed, we analyzed 32 interview transcripts. Most participants were over 24 years of age (N = 44, 72.1%; see Table 1). Overall, 47.5% (N = 29) lived in rural areas and 93.5% (N = 58) were socially or economically disadvantaged. As noted previously, we sought to include in our analyzed sample more participants from groups known to use the helpline less frequently. Compared to the entire pool of participants, the analyzed sample included a higher proportion of participants that were 18–24 years of age (37.5% versus 27.9%), a higher proportion participants from rural areas (59.4% versus 47.5%), and a higher proportion of Muslim participants (21.9% versus 16.4%).
Demographic Characteristics of Interviewed Participants and Subset of Analyzed Transcripts.
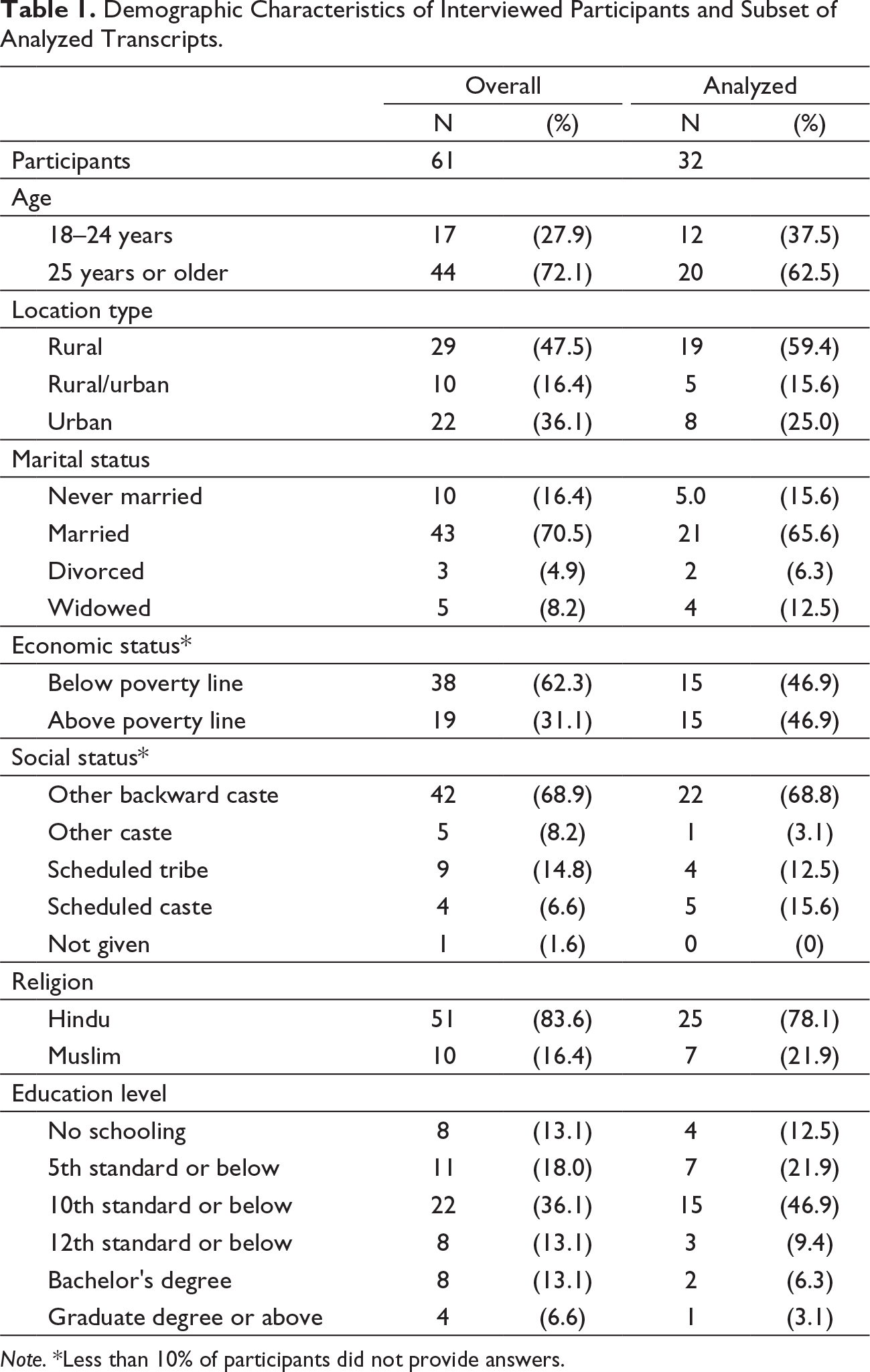
Note. *Less than 10% of participants did not provide answers.
Several themes emerged from our analysis regarding participants’ expectations of support services, selection of support services, and factors that influenced their choice of support and decision about whether to seek help at all. We presented these results under the following themes: stigma, service characteristics, service expectations, empowerment, and trust.
Stigma
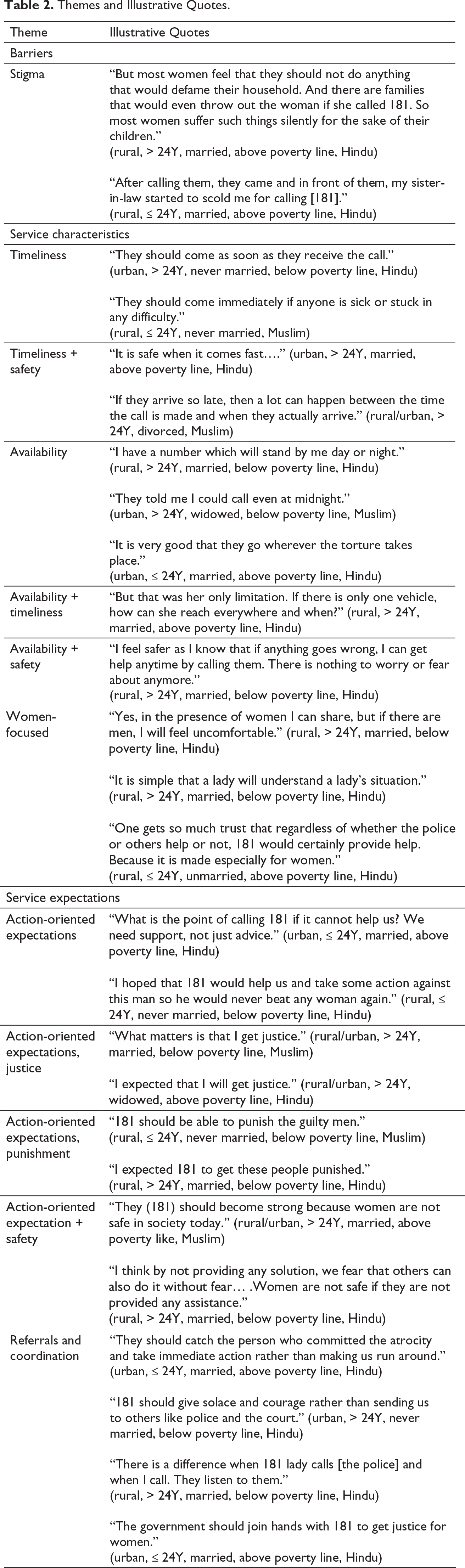
Participants were worried that calling the helpline would impact their reputations and their families (see Table 2). Moreover, women were concerned about how their families would retaliate if they called the helpline and how it might impact their futures. Some participants worried they would lose their homes, children, opportunities for education, or jobs, and would face shame within the community. Participants reported being discouraged by their families and their communities from calling the helpline. Consequently, participants believed women more broadly will continue to remain silent so long as there is discouragement from families and communities. To counter this, one participant noted, “If one woman does this [calls the helpline], other women should support her.” (rural, > 24Y, married, above poverty line, Hindu)
Themes and Illustrative Quotes.
Service Characteristics
Timeliness was the most frequently noted quality by participants. We defined timeliness as the helpline’s ability to respond or act quickly. Repeatedly, participants applauded the helpline for its quick response times (see Table 2), often noting the importance of timely arrival more than once in a single transcript. Participants would note the quick arrival of helpline vans with surprise: “…they said they would get to our place within half-an-hour. And they actually did” (rural, ≤ 24Y, married, above poverty line, Hindu). When vans were unable to swiftly arrive on scene, participants noted their disappointment and fear of what may happen while they wait, specifically connecting timeliness to their sense of safety (see Table 2).
Availability of helpline vans increased participants’ willingness to call. As opposed to timeliness, we defined availability as the helpline’s ability to respond to a call at all, regardless of time of day or place. Participants noted that they did not feel safe going outside after nightfall, making filing a police report or seeking help outside of the home difficult and potentially dangerous. Consequently, the ability of a service to be available to them 24 hours a day was important (see Table 2). Additionally, they believed, and hoped, that increasing the number of helpline vans would enable the helpline to reach women anywhere and improve response times. As articulated by one participant, availability, timeliness, and safety are intertwined features, “As I said earlier, there should be more service stations in each area so that they can arrive fast, and women can feel safer” (urban, ≤ 24Y, married, above poverty line, Muslim).
Lastly, participants found it important that the helpline was staffed by female counselors and female police constables. Based on this characteristic, they felt more comfortable and more likely to be understood. Participants noted that having female staff was a reason they would choose the helpline instead of the police (see Table 2).
Service Expectations
The vast majority of participants noted that they wanted some form of action to be taken beyond counseling alone (see Table 2). Overall, the action that participants most wanted was for an issue to be “solved” or “resolved” in a timely manner. Some participants specified a desire for “justice,” regardless of whether the complaint was for financial transgressions, sexual aggression, or physical abuse. Participants felt that achieving justice impacted safety: “Our safety lies in the fact that every woman gets justice and no one suffers. Not only for us, but for every woman. Everyone should get equal justice” (rural, ≤ 24Y, married, below poverty line, Muslim). Participants felt if justice were achieved in their cases, they would feel more empowered to seek help in the future and encourage other women to seek help as well. Similarly, many participants focused on a desire for perpetrators to be punished. Participants regarded punishment as just action and as a deterrent to future transgressions: “They should remember the punishment for a lifetime so they won’t repeat the violent behavior and will also discourage others from doing it” (rural, ≤ 24Y, married, above poverty line, Hindu). Action-oriented expectations often invoked reference to prior or current experiences in help-seeking from the police. Participants expressed a desire for the helpline to have the ability to take action that was at least commensurate with police powers or to effectively work with the police to be able to take necessary action. Even when their expectations for action were not met and they did not receive the specific help they desired, participants still noted some satisfaction or benefit from having used the service. For example, one participant noted “Yes, you feel better after informing them [181]. Even though you are not getting justice, but you feel that there can be a way out after informing” (rural/urban, > 24Y, widowed, above poverty line, Hindu).
Participants’ perspectives on referrals from the helpline and coordination with other agencies were mixed (see Table 2). Some participants expected that the helpline would need to work with other government agencies and that this was an effective part of the service. Other participants felt that the helpline should be able to address their issues directly rather than referring them to the police.
Empowerment
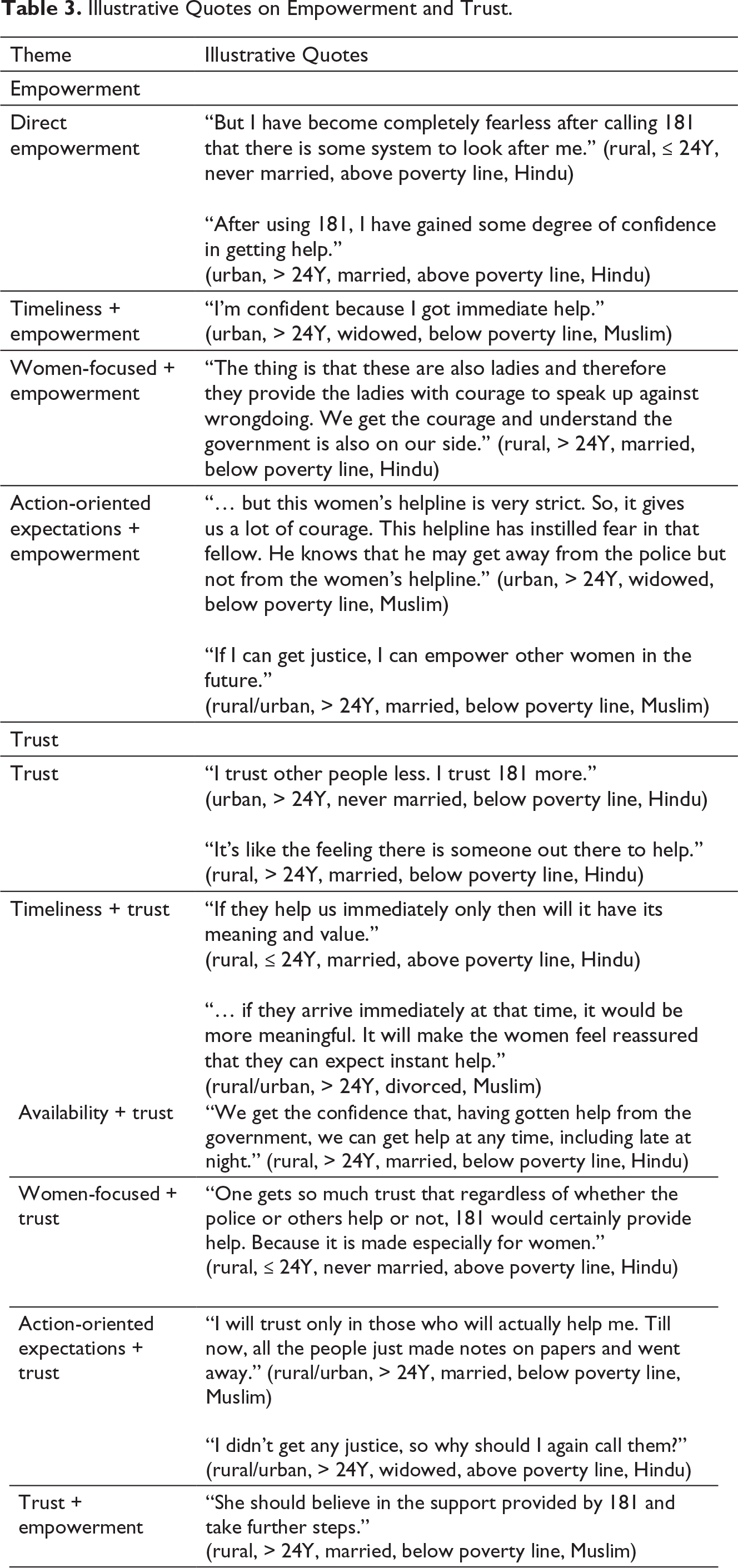
Participants felt empowered by their interactions with the helpline. We considered statements that demonstrated an increased sense of agency, self-efficacy, or access to resources as evidence of empowerment (Kabeer, 2005). Empowerment was mediated through several pathways, including factors noted earlier (see Table 3). Participants were directly encouraged by the helpline team, frequently described as being asked to have “courage.” Participants reported that the experience of having used the service gave them “courage,” decreased feelings of helplessness, and enabled them to go outside of their homes and to seek help. For some participants this was due to new knowledge gained from the helpline, such as knowing how to file a case. Further, participants felt empowered to interact with police because of the relationship between the helpline and the police: “When I went to the police station, I told them fearlessly that I had called 181 and that the woman had sent me to lodge a complaint. Earlier they would not take my complaint…” (urban, ≤ 24Y, married, above poverty line, Hindu). Moreover, participants rooted their empowerment to particular service characteristics already discussed: female staffing, timeliness, and fulfillment of action-oriented expectations.
Illustrative Quotes on Empowerment and Trust.
Trust
Service characteristics and expectations intersected to either build or decrease trust in the helpline or support services generally (see Table 3). Timeliness and the fulfillment of action-oriented expectations gave the service credibility. Availability increased trust that the helpline would be able to provide help whenever crises arose. Having women staff and a service targeted at women placed women more at ease and garnered trust.
Trust was also connected to how participants had heard about the helpline and their interest in recommending the service. Most commonly, participants chose to call the helpline after hearing about it from friends, family, and/or community organizations they trust. Few mentioned typical advertising means, such as TV, newspapers, or signs.
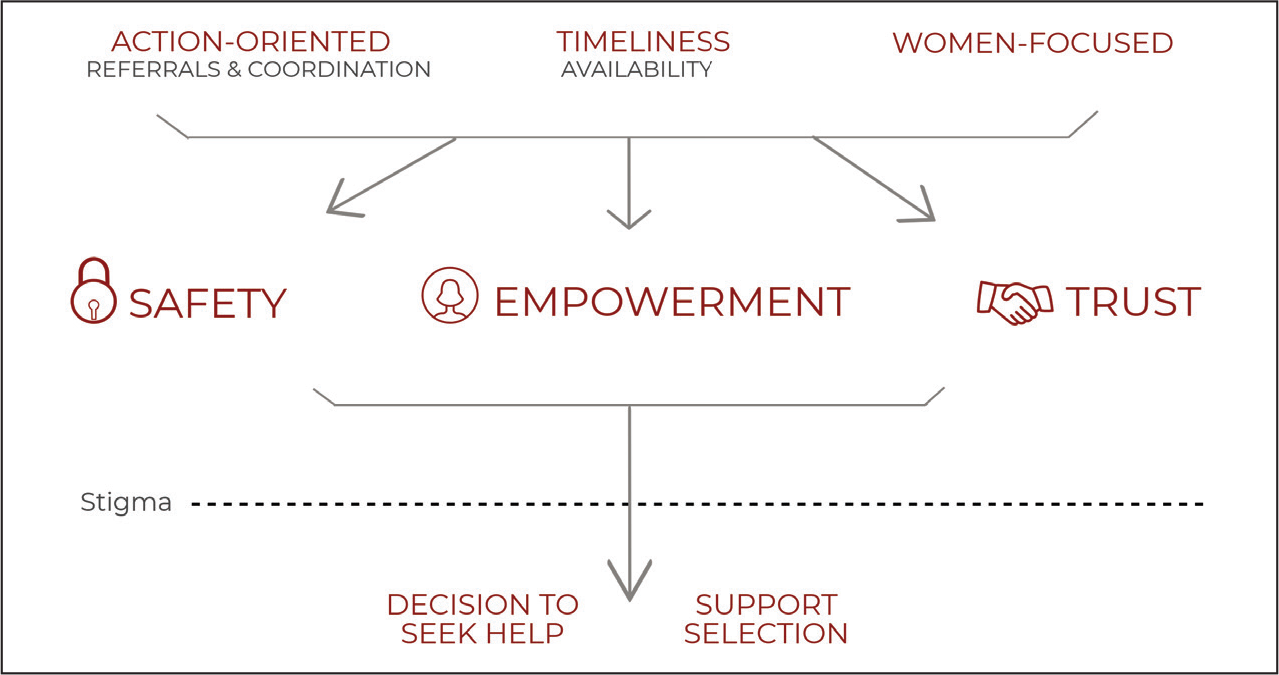
Model of Factors Impacting Help-Seeking and Support Selection
Participants identified key service qualities: timeliness, availability (which impacted timeliness), women-focused service and staff, action-oriented service, and coordination with other services (as driver of action-oriented service). These qualities directly, and through their interaction with each other, impacted women’s sense of safety, empowerment, and trust in the helpline, which ultimately influenced decisions to seek help and whether to seek that support from the helpline (see Figure 2).
Intersection of themes.
Discussion
Our work adds to the literature on help-seeking by exploring support-specific features that influence the decision to seek help and their interplay with greater individual, interpersonal, and sociocultural factors (see Figure 2). In this study, women’s perceptions of the helpline’s responsiveness were based largely on its ability to respond quickly and be available at any time of day. Timeliness served as a central anchor and created feelings of safety, trust, and empowerment. On the other hand, availability was mostly seen as enabling timeliness. Calling for help places women in a vulnerable position both with respect to the perpetrator and their families and communities. If services do not respond quickly, women are at risk for continued and possibly escalated violence or self-harm if they see no other escape and perpetrators may be more likely to abscond (Vidal & Kirchmaier, 2018). Fortunately, timeliness is a quality that can be easily measured and improved. This particular helpline already uses timeliness as a metric: They track the number of calls answered within the first ring and time from dispatch of a helpline van to its arrival on scene. Increasing the overall number of vans and distributing vans across areas, particularly rural and tribal areas, could improve timeliness. Additionally, managing expectations by informing callers of expected arrival time may also help reassure callers that help is coming, particularly in cases where secondary actions may need to be taken by the survivor.
Action taken by the service was another key contributor to women feeling safe, empowered, and having trust in support services. Understanding women’s expectations may be critical to increasing their sense of control (Cattaneo & Chapman, 2010) and improving their sense of control may contribute to women’s sense of agency, which is a critical element of empowerment. Participants often expected “justice” and “punishment,” actions typically associated with the police or courts. Women’s sense of safety was based on the belief that action taken in the present is needed to protect them in the moment and to deter future violence. To obtain justice and feel safe, women may be searching for an alternative to the police; in a study by Panchanadeswaran on women’s perceptions of police in India, 66% of participants felt the police were less useful or not useful at all (Panchanadeswaran & Koverola, 2005). This is challenging as the helpline does not and cannot have police powers, but it is meant to be tightly connected with the police. Specifically, it is supported by a tripartite collaboration inclusive of the Home Department, which oversees the police in Gujarat (Newberry et al., 2016). There are agreed upon protocols for interacting with the police and escalating challenges to higher levels of authority if required for resolution. This novel relationship can have many positive effects, ensuring women are not alone when working with the police. However, the need for referral, for example to the police, to achieve a desired impact was also sometimes seen as a negative aspect of the service—it delayed action and made women feel as though they were being shuffled around. Referrals can raise the risk of retraumatization, forcing women to re-tell their stories, and may also raise the risk of continued or worsened violence. To minimize this potential detrimental impact, it may be important to review referral processes from a trauma-informed point of view (Harris & Fallot, 2001). Specifically, the helpline must ensure that referral processes, including interactions at the point of referral and receival, recognize the woman’s experience as trauma and respond to her associated behaviors within that framework, and actively resist retraumatization (Loomis et al., 2018; Substance Abuse and Mental Health Services Administration, 2014).
Furthermore, to strengthen integration with the police, this helpline already has a female police officer on every field team that accompanies counselors to the scene. However, it is unclear what police powers this officer exercises in the field and if there is an ability to bring more services to the scene, such as filing complaints, making arrests, or placing restraining orders. A continued focus on strengthening the helpline’s relationship with the police, creating new or strengthened pathways from helpline access to police support, and providing feedback between the two are critical for women’s sense of safety, empowerment, and trust in both systems. Further, community education on the role of the police in the helpline may help to inform women’s expectations of the helpline. Literature supports this finding: that in survivors’ interactions with police, process and experience can be as impactful as outcomes (Cattaneo & Goodman, 2005; Zweig & Burt, 2007).
Additionally, participants in this study noted the importance of having predominantly women staff, yet this characteristic alone may be insufficiently survivor centered. Previous research has shown that survivors did not feel that women counselors housed within police stations in India were empowering in their approach to survivors (Panchanadeswaran & Koverola, 2005). Police stations and support services co-located within them were seen as part of the same patriarchal infrastructure. In contrast, this helpline is operationalized by a public–private partnership, wherein they are physically separate entities and may allow the helpline to be seen as independent of the police, whom women may or may not trust. However, this underscores the importance of counselor training that emphasizes communication skills that are in support of and empowering to VAW survivors. Within the Indian context, a family-centric view is dominant, which often places pressure on women to maintain harmony and put family first in the face of violence (Ahmed-Ghosh, 2004). Incorporating a survivor-centered approach may increase women’s sense of acceptance and empowerment. A survivor-centered approach recognizes a survivor’s specific situation and the ways in which their own goals may vary, and prioritizes those perspectives and goals in service development and delivery (Davies & Lyon, 2013; Goodman & Epstein, 2008; Goodman et al., 2014; Kulkarni et al., 2015).
To that end, our work places the survivor’s voice as central to the evaluation and growth of VAW support services. As advocated by Davies et al. (1998), intimate partner violence services should be focused on “woman-defined advocacy” rather than “service-defined advocacy” alone. Goodman and Epstein (2008) recommend that three principles guide intimate partner violence service development: voice, community, and economic empowerment. Incorporating users’ voices into quality improvement is necessary for the helpline to achieve its vision of effectively serving survivors of VAW.
Limitations
Recruiting only women who had access to phones may limit our generalizability. Approximately 60% of women in India are the primary owners of their phone (Rowntree, 2019), other women may still have access to a mobile phone, but it would be through friends or family. Consequently, we may be missing some of the most disenfranchised women in our study. Furthermore, we excluded women who could not speak either Gujarati or Hindi. We attempted to mitigate the potential bias this would impose by specifically recruiting Muslim women (representing the primary population speaking Urdu) and women from the northern district of Kutch (where Kutchi is primarily spoken).
During recruitment, specific issues of access to the study population emerged. Many potential participants could not agree to interviews because other family members, mainly husbands, parents, and in-laws, would not allow them to participate. This cultural norm, which was present even in the initial recruitment calls, may restrict the generalizability of our findings and may be a barrier to VAW research throughout India. Women who could not participate in an interview without the permission from a husband or other elder family member likely (a) face other gender-based barriers and (b) interact with support services from a different perspective. For example, they may feel less empowered to seek help, have different expectations from services when they do finally seek help, and therefore may value support service characteristics differently. There is much we could learn from these women and future work should integrate methods that can better work to include these women. Similar issues surfaced with interviews. The vast majority of participants wanted to be interviewed in their homes and preferred that their families stay nearby. While we were able to achieve privacy within the actual interview room, it is difficult to estimate the effect of family being present within close proximity.
Implications
Research has shown that Indian women are interested in crisis counseling (Decker et al., 2013), yet they seek help from formal sources at an exceedingly low rate—estimated 5.7% of all women experiencing violence (IIPS, 2017). Our findings may help to strengthen support service characteristics that increase help-seeking, particularly from formal sources. Moreover, many participants in this study noted their desire to make others aware of the helpline, “Each woman in every family should be made aware of it.” (rural, > 24Y, married, above poverty line, Hindu) However, it became clear that growing awareness was contingent on trust. As noted earlier, most women called the helpline after learning about it from well-known connections: family, friends, particular organizations. Our study demonstrates that every interaction with a caller matters because it is an opportunity to empower and build trust. It is not enough for support services to simply exist; in order to spread awareness and to increase use, these services must engender trust and be action oriented.
Growing national attention in India on VAW has resulted in the exponential growth of support services from governmental and nongovernmental organizations. Future research is needed to understand how this growth can drive broader change in gender norms at the community level and whether the growth of the support service environment can influence women’s conceptions of VAW, even if they are not users of the service. Additionally, if women primarily connect to services which are suggested by trust networks (e.g., friends, family, community organizations), as our study suggests, we must identify best practices for community and family engagement that can increase knowledge of and trust in services prior to the time of crisis. Finally, as migration is a common phenomenon in India for marriage and labor, research and innovation is needed to understand help-seeking strategies employed by women when they immigrate to new communities and the ways that support services can better help these women. These lines of future inquiry are in sync with national efforts by the Indian government to study helpline implementation in order to identify and incorporate best practices across states (Ministry of Women and Child Development, 2016).
Conclusion
Whereas prior literature has focused on the influence of survivor and perpetrator attributes on help-seeking, this study expands that discussion to highlight the impact of service characteristics. Based on our findings, we set forth a new model for help-seeking and support selection based on service-specific factors that can empower and enable survivors to seek help. Consequently, survivors must have a voice in the growth and refinement of VAW support services. In India, the speed of response and the strength of the response are key determinants of women’s sense of safety, empowerment, and trust in the service itself. In addition, when working closely with the police and coordinating referrals to other support services, setting expectations and ensuring supportive interactions at the point of referral and receival are critical to women’s overall perception of the service. Women’s trust in a service in turn influences whether they recommended the service to family and friends, and it is these informal networks that women noted were a major driver of support service awareness. Thus, service characteristics in and of themselves influence the likelihood that women will seek help and consequently must be a focus of future research to improve help-seeking by VAW survivors.
Footnotes
Acknowledgments
We would like to thank our research assistants whose hard work and compassion made this research possible: Parlin Christian, Neha Joshi, Rushali Patel, Shilpa Parmar, Komal Parmar, Mamta Vankur, and Nayana Vasava. We would like to thank the leadership of the 181 Abhayam Women’s Helpline: Jashvant Prajapati (Chief Operating Officer, GVK EMRI), Narendrasinh Gohil (Program Lead), Hetal Patel (Team Leader), and Meghana Patel (Team Leader).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Dr G.V. Ramana Rao is the Director of Research for GVK Emergency Management and Research Institute, the organization which operates the helpline studied.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was made possible by a Stanford University Center for Innovation in Global Health Seed Grant.