
Abstract
Military sexual trauma (MST; i.e., sexual harassment and/or sexual assault during one’s military service) is highly prevalent among female veterans and is associated with numerous adverse health and psychosocial sequelae. When institutions fail to prevent sexual trauma from happening or respond in an unsupportive manner (i.e., institutional betrayal [IB]), MST survivors typically report more severe health-related outcomes. Although the Institutional Betrayal Questionnaire.2 (IBQ.2) was developed to assess IB, no studies have examined the factor structure or dimensionality of the IBQ.2 among MST survivors. In addition, initial research has reported differing factor structures for this measure. The present study examined the dimensionality and factor structure of the IBQ.2, and tested for differential item functioning (DIF) based on whether military sexual assault was experienced. The sample comprised 235 female veterans who reported a history of MST in an anonymous national survey. Rasch analysis suggested multidimensionality and DIF based on history of military sexual assault. Exploratory factor analysis and parallel analysis suggested the IBQ.2 comprises three factors: (1) Environment Leading to MST, (2) Institutional Response to MST, and (3) Institutional Belongingness following MST. Although these results suggest that the IBQ.2 is multidimensional, the three-factor model had significant issues with respect to dimensionality, item fit, and person separation and reliability. Thus, using the full IBQ.2 may be more advantageous. Further examination of the IBQ.2 is warranted to ensure optimal assessment of IB in relation to MST, irrespective of whether the MST comprised sexual harassment or sexual assault, as well as to ensure that the IBQ.2 is culturally meaningful for MST survivors.
Military Sexual Trauma: Prevalence and Sequelae
Despite concerted efforts to prevent sexual assault in the U.S. Armed Forces, sexual assault (i.e., “intentional sexual contact characterized by use of force, threats, intimidation, or abuse of authority or when the victim does not or cannot consent;” Department of Defense [DoD], 2017, p. 20) remains prevalent (DoD Sexual Assault Prevention and Response Office, 2019). In Fiscal Year 2018, an estimated 20,500 service members experienced sexual assault, which is an increase from prior years (DoD Sexual Assault Prevention and Response Office, 2019). Of note, the estimated prevalence of sexual assault in the active-duty force uniquely increased for women, who represent the majority of service members who reported experiencing sexual assault during this time (DoD Sexual Assault Prevention and Response Office, 2019). Sexual harassment (i.e., “unwelcome sexual advances, requests for sexual favors, and deliberate or repeated offensive comments or gestures of a sexual nature;” Office of the Under Secretary of Defense for Personnel and Readiness, 2018, p. 7) in the Armed Forces has also continued to occur at high rates, with 21.3% of women reporting that they experienced a sexually hostile work environment in the prior 12 months (DoD Office of People Analytics, 2017).
The Department of Veterans Affairs (VA) has implemented screening for experiences of sexual assault and sexual harassment that occurred during active duty, active duty for training, and inactive duty for training, referred to as military sexual trauma (MST; U.S. Government, 2014). Over 5.1 million veterans have been screened for MST within the Veterans Health Administration (VHA; Department of Veterans Affairs Office of Mental Health and Suicide Prevention, 2019). Of those, women have screened positive at disproportionately high rates (29.1%), compared to men (1.6%; Department of Veterans Affairs Office of Mental Health and Suicide Prevention, 2019). Despite efforts to increase MST reporting (Foynes et al., 2018), these rates are likely underestimates (Bovin et al., 2019).
Extensive research has illuminated the substantial health-related and psychosocial impacts of MST on service members and veterans (Stander & Thomsen, 2016; Surís & Lind, 2008). Among women, MST is associated with increased risk for posttraumatic stress disorder (PTSD), depressive disorders, substance use disorders, anxiety disorders, eating disorders, somatoform disorders, as well as suicidal ideation and suicidal self-directed violence (Goldberg et al., 2019; Kimerling et al., 2007; Kimerling et al., 2016; Monteith, Holliday, Hoyt, et al., 2019; Yaeger et al., 2006). Women who experience MST are also at elevated risk for obesity, hypothyroidism, liver disease, sexual dysfunction, and sexually transmitted infections (Frayne et al., 2003; Kimerling et al., 2007; Pulverman et al., 2019; Turchik et al., 2012). Moreover, MST is associated with interpersonal difficulties, homelessness, and lower quality of life (Brignone et al., 2016; Luterek et al., 2011; Sadler et al., 2000; Surís et al., 2007).
These negative sequelae are particularly severe when the MST comprised sexual assault (Blais et al., 2019; Holliday et al., 2019; Monteith, Menefee, et al., 2016; Street et al., 2008) or when other types of potentially traumatic events have also been experienced. For example, in a study of women veterans, there was an interaction between MST and combat exposure, such that women who experienced MST and higher levels of combat reported more severe PTSD symptoms (Scott et al., 2014). Moreover, women who experience MST frequently experience other types of interpersonal violence, particularly childhood sexual abuse and adult sexual assault (Kelly et al., 2011; Surís & Lind, 2008). Nonetheless, MST is associated with adverse health outcomes (e.g., PTSD, anxiety, hostility, lower health-related quality of life) even when accounting for childhood and civilian sexual violence (Luterek et al., 2011; Surís et al., 2007). Additionally, MST is more strongly associated with PTSD than pre- and post-MST trauma (Himmelfarb et al., 2006), suggesting that the experience of MST is particularly detrimental.
The Role of Institutions in Military Sexual Trauma
In recognition of the broad array of negative outcomes that can ensue following MST, researchers have begun to examine factors that can influence recovery, including interpersonal (Laws et al., 2016; Monteith, Hoffmire, et al., 2018) and institutional factors. Burgeoning research suggests that institutions play a critical role in facilitating or impeding recovery (Campbell et al., 2009; Smith & Freyd, 2014).
Accordingly, Smith and Freyd (2013, 2014) proposed the concept of institutional betrayal (IB) to describe when institutions fail to prevent trauma from happening or respond in an unsupportive manner (e.g., minimize or deny the experience). For numerous reasons, IB has been posited to be particularly salient in the context of MST (Smith & Freyd, 2013; Monteith, Bahraini et al., 2016). Women have described MST as occurring in a broader institutional context in which sexual harassment was expected, constant, and normative (Brownstone et al., 2018; Burns et al., 2014). Despite some perceived improvements, service members have continued to report perceptions of a male-dominated culture in which inappropriate gender-related jokes and scenarios increased the likelihood of experiencing sexual harassment and assault (DoD Office of People Analytics, 2018). In addition, the majority of sexual assaults (73%) perpetrated against servicewomen occur at military locations (DoD Office of People Analytics, 2017). Alleged offenders are typically in the military (90%) and frequently comprise high-ranking individuals (57%; DoD Office of People Analytics, 2017). Women have also described experiencing MST at a particularly vulnerable time (i.e., early in their military careers; Brownstone et al., 2018). These findings may help to explain why MST survivors commonly indicate that a military institution contributed to the MST by creating an environment in which MST seemed normal, common, and more likely to occur (Monteith, Bahraini et al., 2016).
IB can also occur in the aftermath of MST—for example, in relation to reporting or the pursuit of legal recourse. Women have described feeling silenced and disempowered by the experience of MST (Brownstone et al., 2018). Only a minority (31%) formally report sexual assault to a military authority (DoD Office of People Analytics, 2017), which may derive from fears regarding personal safety, career repercussions, blame, confidentiality, and of being perceived and treated differently (Brownstone et al., 2018; Burns et al., 2014; Dardis et al., 2018; Mengeling et al., 2014; Monteith, Bahraini et al., 2016; Wolff & Mills, 2016). These factors may be further impacted when betrayed by a fellow unit member (Blais et al., 2018).
When disclosure does occur, negative reactions are common—tending to be deficient in support, documentation, and pursuit of justice, while also comprising threats or being told not to tell anyone (Dardis et al., 2018; Mengeling et al., 2014; Wolff & Mills, 2016). Women who formally report sexual assault have also reported experiencing high rates of social or professional retaliation, punishment, and adverse administrative reactions (62%; National Defense Research Institute, 2014). In addition to being blamed for being sexually assaulted, women have indicated that there are rarely consequences to the assailants (Burns et al., 2014; Mengeling et al., 2014). Approximately one-third of servicewomen report dissatisfaction with their chain of command in their sexual assault response (DoD Office of People Analytics, 2017). These experiences can lead to disillusionment, a sense of betrayal, and no longer feeling valued by the military institution (Brownstone et al., 2018; Dardis et al., 2018; Monteith, Bahraini et al., 2016), at times, culminating in premature separation (Dichter & True, 2015; DoD Office of People Analytics, 2017). Moreover, the sequelae of IB can be extensive, encompassing PTSD and depressive symptoms, as well as increased odds of attempting suicide (Andresen et al., 2019; Dardis et al., 2018; Monteith, Bahraini et al., 2016).
Taken in aggregate, women who experience IB in relation to MST are likely to need health services to address MST-related sequelae. However, MST survivors may attribute their prior negative experiences to other federal institutions, such as the VA, and thus delay engaging in care (Holliday & Monteith, 2019; Monteith, Bahraini, et al., 2018). Because the VA provides MST-related care free-of-charge (Foynes et al., 2018), accurately identifying IB among survivors of MST is integral to ensure that appropriate services are provided to this subset of veterans.
Measurement of Institutional Betrayal
Unfortunately, knowledge regarding optimal ways to assess IB remains limited. Smith and Freyd (2013) first developed the Institutional Betrayal Questionnaire (IBQ), Version 1, to assess IB in regard to unwanted sexual experiences, with seven items summed to create an overall score of IB. In their initial sample of college women, the IBQ was unidimensional. Scores did not significantly differ based on unwanted sexual experience types (e.g., verbally versus physically coerced) or continued association with the institution.
Smith and Freyd (2017) subsequently refined the IBQ to create the IBQ.2, adding 5 items regarding additional institutional actions that can occur following sexual assault (e.g., denying one’s experience, mishandling one’s case, creating an environment in which continued membership is difficult). Reffi et al. (2018) examined the IBQ.2 in a mixed-gender sample of adult sexual assault survivors (i.e., those reporting an unwanted sexual experience after age 14). However, the single factor model was not replicated in a confirmatory factor analysis. Rather, they found support for a two-factor structure (based on a different version of the IBQ by Tamaian and Klest, 2018, which assessed IB in relation to the medical system) comprised of: (1) Leading to Sexual Victimization, and (2) Response to Sexual Victimization. In addition, while the Response to Sexual Victimization factor demonstrated convergent and discriminant validity, the Leading to Sexual Victimization factor was not significantly correlated with study variables. The authors concluded that IB may thus be best “represented by more than one factor” (p. 16). Thus, findings regarding the factor structure of the IBQ.2 remain mixed.
Furthermore, studies examining the IBQ.2 factor structure have relied on traditional psychometric methods. No studies have examined the IBQ.2 factor structure or psychometric properties using modern psychometric methods, such as Rasch analysis. Complementing classical test theory (CTT) approaches, Rasch offers a more powerful examination of item and scale functioning than when relying on CTT methods alone (Tennant & Conaghan, 2007). In addition to explicitly testing for unidimensionality, the Rasch model weights individual items based on their contribution to the underlying construct (hierarchy) and allows transformation of raw scores into continuous linear data, contributing to more accurate and meaningful comparison of scores across people (Bahraini et al., 2018).
Moreover, despite research suggesting particularly high levels of IB among MST survivors (Monteith, Holliday, Schneider et al., 2019), compared to other samples in which the IBQ.2 has been examined, no studies have examined the factor structure of the IBQ.2 in MST survivors. The present study sought to address these gaps by using Rasch analysis to examine the dimensionality and factor structure of the IBQ.2 among female veterans who reported experiencing MST. We also examined whether there was differential item functioning (DIF) on the IBQ.2, based on MST type (i.e., sexual assault versus sexual harassment only).
Method
Participants and Procedures
We addressed these aims with cross-sectional data from a national survey of female veterans, conducted in 2018–2019 (Monteith et al., 2020). Inclusion criteria included being a female veteran, age 18 to 89, and enrolled in VHA care. We used VA Corporate Data Warehouse (CDW) data and stratified random sampling based on age and geographic location to construct the initial sampling frame of 3,000 female veterans. We excluded individuals if they were deceased, had inconsistent data regarding sex or age, or did not have a valid mailing address. To ensure that our sample was not overly reliant upon veterans currently using VHA care, our initial sampling frame was equally divided between veterans who had used VHA care in the past year, had used VHA care prior to the past year, and had never used any VHA care.
We sent letters inviting participation to the 3,000 veterans in our sampling frame. Mailings included an invitation letter with instructions for participation, a postcard consent form, the survey, a stamped addressed return envelope, and a debriefing form. Measures relevant to the current manuscript are described below. Participation was anonymous and could occur by mail or online. No payment was provided for participation. Two subsequent reminder mailings were sent inviting participation. This study was approved by the local institutional review board. Underlying materials related to this manuscript can be accessed by contacting the lead author.
After accounting for undeliverable mailings (n 642; 21.4%), the overall response rate was 19.6% (n 463). We removed anyone who reported male birth sex (n 3), current active status or full-time Guard or Reserves (n 6), having previously taken the survey (n 2), or who only answered study eligibility questions (n 4), resulting in 448 respondents. For the present aims, we only included those who screened positive for MST when completing the survey (n 284; 63.4%); thus, we removed those with a negative MST screen, who declined to respond to both MST screening questions, or who had mixed responses of “no” and “decline to respond.” Of those, 49 (17.3%) had missing IBQ.2 data (Items 1–12) and were removed. Thus, our analytic sample included 235 female veterans who screened positive for MST and had complete IBQ.2 data. There were significant differences between the analytic sample and those excluded due to missing IBQ.2 data regarding age, ethnicity, branch (Army), and service era (Korean War, Post-Korean War, or Vietnam; all ps < .05), but not in regard to other sociodemographic or military service variables, VHA use, or type of MST experienced.
Measures
Department of Veterans Affairs Military Sexual Trauma Screening Questions.
MST was assessed with the same two questions used nationally within VHA to screen for MST: (1) “When you were in the military, did you ever receive unwanted, threatening, or repeated sexual attention (e.g., touching, cornering, pressure for sexual favors, or inappropriate verbal remarks, etc.)?” [sexual harassment]; (2) “When you were in the military, did you have sexual contact against your will or when you were unable to say no (e.g., after being forced or threatened or to avoid other consequences)?” [sexual assault] Response options included yes, no, or decline to respond. A positive MST screen is indicated by an affirmative response to at least one of these questions. The MST screening questions have demonstrated convergent validity in prior research, including correspondence to a lengthier measure of military sexual harassment and assault with more extensive response options (i.e., Sexual Experiences Questionnaire, Department of Defense; Mengeling et al., 2019).
Institutional Betrayal Questionnaire-2.
Participants who screened positive for MST were asked to complete the IBQ.2 (Smith & Freyd, 2017), which has been used previously to assess IB regarding MST (Monteith, Bahraini et al., 2016). Participants were instructed to: Think about larger military institutions to which you belong or have belonged, which may or may not call to mind specific individuals. This may include large systems, such as the military in general, or an entire branch of the Armed Forces. It may also include a smaller system, such as a military academy, military base, or specific unit.
Twelve items assessed whether a military institution had played a role in the MST, with response options of no (scored as 0) or yes (scored as 1). Responses of N/A were coded as 0. Items are summed to create an overall score, with higher scores indicative of more IB.
Other variables.
Sociodemographic and military service characteristics were assessed via self-report. VHA use was determined from CDW.
Analytic Plan
To describe the sample, we used SAS v9.4 (SAS Institute, 2016) to compute descriptive statistics for sociodemographic and military characteristics and VHA use. We examined if there were differences in these characteristics based on military sexual assault history (yes/no), using t-tests for continuous variables and Chi-square or Fisher’s Exact tests for categorical variables.
Rasch analysis.
The Rasch analysis was conducted using Winsteps Version 4.4.1 (Linacre, 2019) and consisted of examination of (a) overall and item-level fit; (b) person separation and reliability; (c) principal components analysis of Rasch residuals; and (d) DIF. The criteria used to evaluate these measurement properties are defined below.
Overall and item fit.
Overall fit was examined to determine if the data showed acceptable fit to the Rasch model by assessing the mean infit and outfit for person and item mean squares (MNSQ). 1.0 is the expected value (Linacre, 2002). Values less than 1.0 indicate observations are too predictable (redundancy). Values greater than 1.0 indicate unpredictability. In item-fit analysis, MNSQ values between .6 and 1.5 are considered acceptable (Wright & Linacre, 1994).
Person separation and reliability.
The person separation index indicates the extent to which a measure (i.e., IBQ.2) can separate persons into different levels of a trait or construct (i.e., IB). A person separation index of 1.50 or above represents an acceptable level of separation (Fisher, 1992; Wright & Masters, 1982). When expressed as reliabilities, they range from .0 to 1.0 (i.e., .9 = 3 or 4 levels, .8 = 2 or 3 levels, and .5 = 1 or 2 levels; Linacre, 2012). The higher the value, the better the separation that exists, and the more precise the measurement.
Principal component analysis of Rasch residuals.
A principal component analysis of Rasch residuals (PCAR) was conducted to determine whether substantial subdimensions existed within IBQ.2 items. The following criteria were used to determine unidimensionality (Linacre, 2006): (a) the variance explained by the measurement dimension was at least 40%, (b) variance explained by the first principal component of the residuals was no more than 15%, and (c) the eigenvalue of the first contrast was less than 2.
Differential item functioning.
We evaluated if there was DIF based on history of military sexual assault. For the DIF analyses, those who did not answer the question regarding military sexual assault or who declined to respond (n 8) were excluded. Items that were both statistically and clinically significant (i.e., at least a .6 logit difference between those with and without a history of military sexual assault; Linacre, 2012) were considered to have DIF.
Exploratory factor analysis.
We also conducted an exploratory factor analysis (EFA) in SAS v9.4 to determine factor structure. Factors were extracted using the maximum likelihood method, followed by promax oblique rotation, as it was expected that the factors would be correlated. The EFA was followed by a parallel analysis to confirm the number of factors (O’Connor, 2000).
Results
Sample Characteristics
Demographic and Military Service Characteristics for the Overall Sample and Based on Military Sexual Assault History (N = 235).
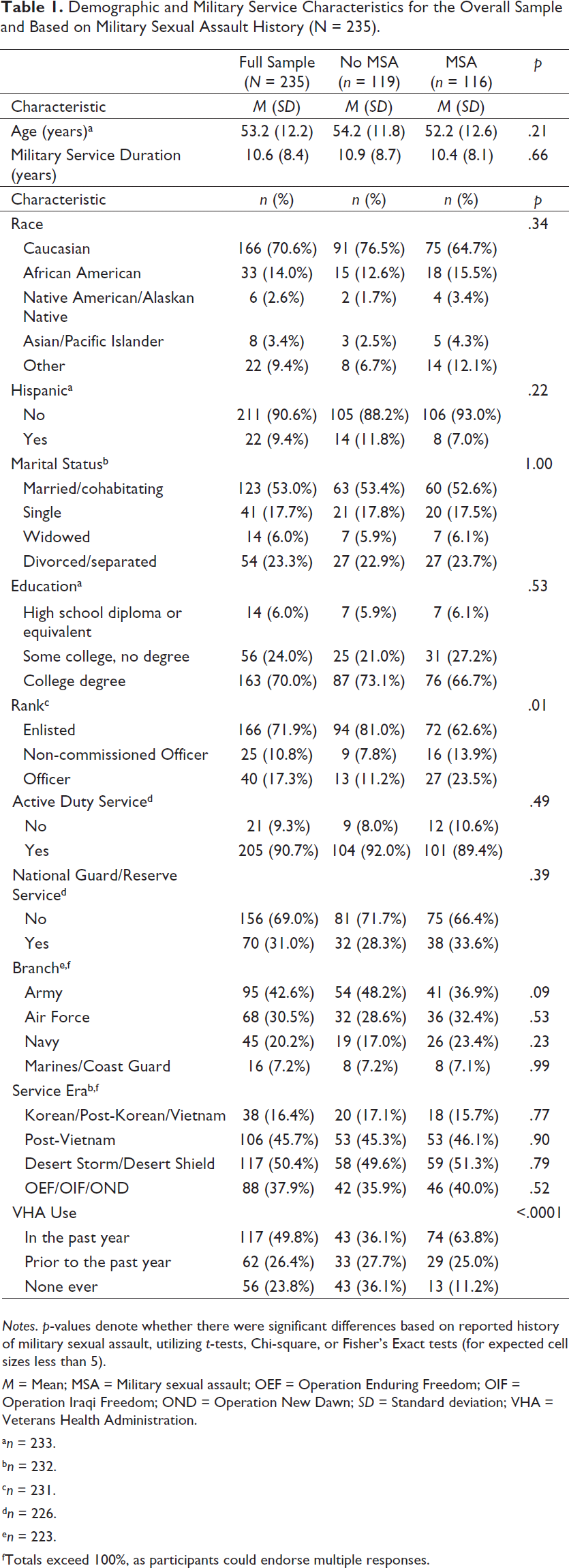
Notes. p-values denote whether there were significant differences based on reported history of military sexual assault, utilizing t-tests, Chi-square, or Fisher’s Exact tests (for expected cell sizes less than 5).
M = Mean; MSA = Military sexual assault; OEF = Operation Enduring Freedom; OIF = Operation Iraqi Freedom; OND = Operation New Dawn; SD = Standard deviation; VHA = Veterans Health Administration.
an = 233.
bn = 232.
cn = 231.
dn = 226.
en = 223.
fTotals exceed 100%, as participants could endorse multiple responses.
Rasch Analysis of the Full Institutional Betrayal Questionnaire.2
Overall Fit.
IBQ.2 Measurement Properties.
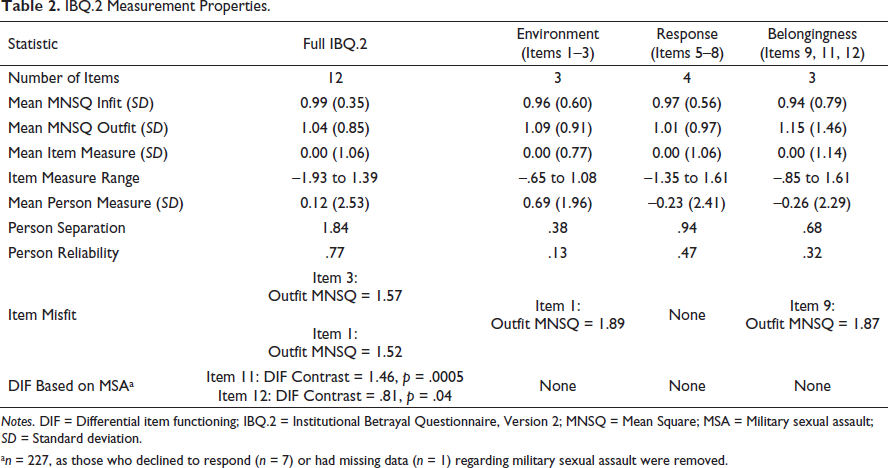
Notes. DIF = Differential item functioning; IBQ.2 = Institutional Betrayal Questionnaire, Version 2; MNSQ = Mean Square; MSA = Military sexual assault; SD = Standard deviation.
an = 227, as those who declined to respond (n = 7) or had missing data (n = 1) regarding military sexual assault were removed.
Item and Person Statistics.
Item and person measure statistics are in Table 2. Item fit scores ranged from .80 to 1.33 (Infit MNSQ) and .68 to 1.57 (Outfit MNSQ). Person fit measures ranged from .49 to 2.20 (Infit MNSQ) and .28 to 4.68 (Outfit MNSQ). Removal of individuals with outfit MNSQ > 3 (n 7) did not significantly affect results, so these individuals were retained for subsequent analyses. The mean locations for persons (0.12) and items (0) were similar, suggesting, on average, items were not too easy or hard to endorse for this sample.
Principal components analysis of residuals.
IBQ.2 Dimensionality Criteria.
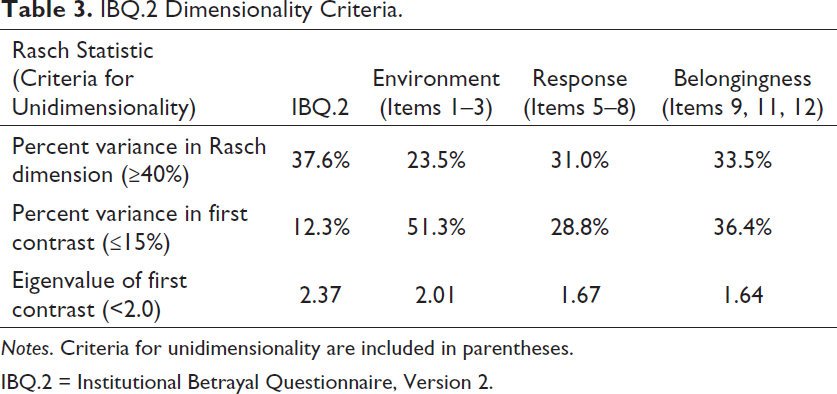
Notes. Criteria for unidimensionality are included in parentheses.
IBQ.2 = Institutional Betrayal Questionnaire, Version 2.
Differential item functioning.
When we tested the full IBQ.2 for DIF based on military sexual assault history, Items 11 and 12 had significant DIF (Table 2). This indicates that it was significantly easier for those with a history of military sexual assault to endorse that the institution created an environment where they no longer felt valued (Item 11) or where continued membership was difficult (Item 12), compared to those without a history of military sexual assault.
Exploratory Factor Analysis and Parallel Analysis
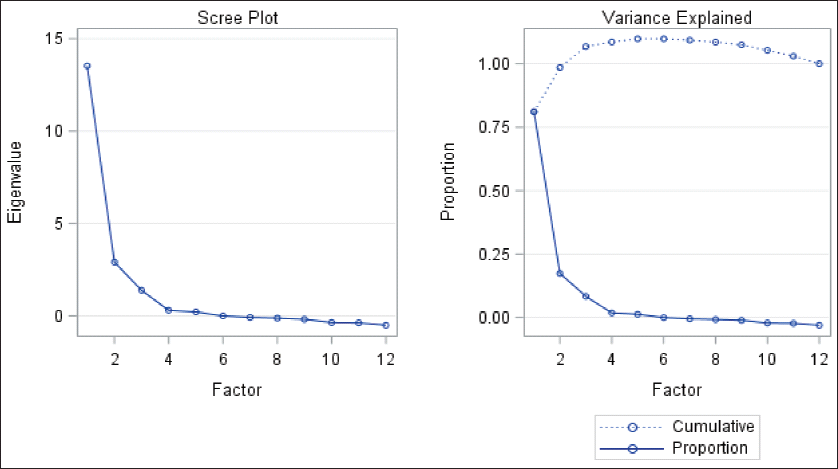
Given that the results of the PCAR did not fully support the unidimensionality of the IBQ.2, a factor analytic approach was utilized to further examine factor structure. We determined the number of factors to retain based on visual inspection of the Scree plot, Kaiser’s criterion (i.e., number of eigenvalues ≥1), proportion of variance accounted for, and a parallel analysis. The EFA scree plot was indicative of three factors (Figure 1). Similarly, three factors had eigenvalues >1, with each accounting for ≥5% of the variance (Table 4). In addition, the first three eigenvalues from the actual data in the parallel analysis (Table 4) were larger than the corresponding first three 95th percentile random data eigenvalues, while the fourth eigenvalue from the actual data was smaller than the fourth 95th percentile random data eigenvalue, also suggesting a three-factor structure. We removed items with factor loadings <.40 (Items 4 and 10) and assigned items to a specific factor based on their highest loading (Table 5). This resulted in subscales for: (1) Environment Leading to MST (heretofore abbreviated as “Environment”); (2) Institutional Response to MST (abbreviated as “Response”); and (3) Institutional Belongingness following MST (abbreviated as “Belongingness”).
IBQ.2 Scree Plot.
Exploratory Factor Analysis and Parallel Analysis of the IBQ.2.
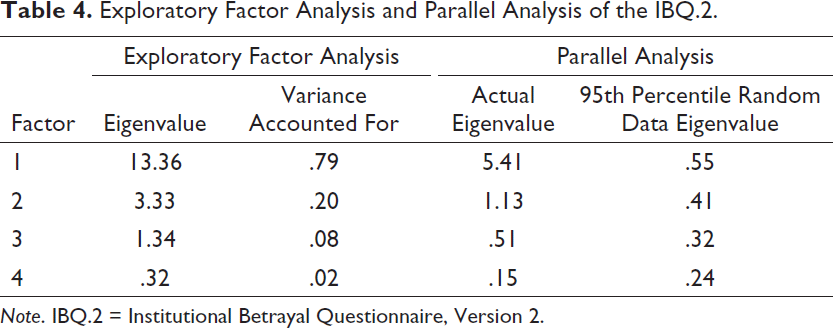
Note. IBQ.2 = Institutional Betrayal Questionnaire, Version 2.
Rasch Analysis of the Three Institutional Betrayal Questionnaire-2 Factors
Table 3 displays the results of the PCAR for the three proposed factors identified through EFA and parallel analysis. Overall, results did not support unidimensionality of the three factors. Although the eigenvalues were less than or just above 2, the other two criteria were either well below (i.e., percent variance in Rasch dimension) or above (i.e., percent variance in first contrast) acceptable thresholds. Furthermore, examination of Rasch measurement properties (Table 2) revealed misfitting items for the Environment and Belongingness factors. In addition, all three factors demonstrated low person separation and reliability, indicating that they were not sensitive enough to distinguish between different levels of IB.
Discussion
Burgeoning research highlighting the multitude of ways in which IB can occur in relation to MST, as well as recent interest in applying the concept of IB to understanding health outcomes following MST (Holliday & Monteith, 2019), emphasize the import of determining optimal ways to assess IB among MST survivors. Although the IBQ.2 has been used previously in research with MST survivors (Monteith, Bahraini et al., 2016), to our knowledge, this is the first study to examine the dimensionality and measurement properties of the IBQ.2 in this population using a combination of traditional psychometric methods (EFA) and Rasch analysis.
Consistent with prior research (Reffi et al., 2018), our findings provide evidence to suggest that the IBQ.2 may be multidimensional. Unlike previous studies, the use of Rasch analysis enabled a more detailed examination of the measurement properties of IBQ.2 factors identified through EFA. Specifically, Rasch analysis of the three-factor model revealed significant issues with respect to dimensionality, item fit, and person separation and reliability. Although unidimensionality of the full IBQ.2 was not fully supported, it had several advantages over the three-factor model, including greater measurement range and precision, reliability, and differentiation of IB levels. Moreover, the item hierarchy was consistent with expectations regarding the theoretical ordering of IB experiences (i.e., likelihood of an item being endorsed).
These findings raise an important issue about the concept of dimensionality. A key consideration when examining dimensionality is whether multidimensionality in the data is considerable enough to merit dividing items into separate domains. This is especially important as dividing items into smaller scales may come at a cost to other psychometric properties. Taken together, findings from this study do not support separating the IBQ.2 into different domains, since doing so did not produce differentiated unidimensional scales. Additionally, separation further degraded other measurement properties (e.g., person separation, reliability).
Our findings also highlight different areas for potential scale refinement. For example, removing misfitting items (i.e., Item 3) may improve measurement properties of the instrument. Further research is needed to understand the impact of removing these items on dimensionality. Removal of misfitting items should also be evaluated against the impact on clinical utility. This could include evaluating the effect of item removal not only based on fit statistics, but also against other clinical criteria, such as ability to detect group differences (Smith et al., 2007). Similarly, examining the impact of DIF on dimensionality and overall measurement properties is another important area for future investigation. Two items, which reflect the institution creating an environment in which the MST survivor no longer felt like a valued member or where continued membership was difficult, had DIF based on history of military sexual assault. It may be the case that a different version of the IBQ.2 is needed for those with a history of military sexual assault or that this needs to be accounted for when scoring the measure. Future research focused on measure refinement should consider incorporating qualitative methods to ensure the IBQ.2 is culturally meaningful and valid for MST survivors.
Our findings have important implications for research and clinical work with MST survivors. Given varying factor structures of the IBQ.2 in different samples of survivors of unwanted sexual experiences (Reffi et al., 2018; Smith & Freyd, 2013), additional psychometric evaluation is warranted. In addition, understanding factors inherent to the institutional response to MST and the broader environment in which MST occurs appears salient. By identifying these latent factors, providers can understand mechanisms of IB that can be assessed and intervened upon. Notably, however, research targeted at attenuating IB following sexual harassment or assault does not presently exist. In addition, while MST survivors who experience IB report more severe mental health symptoms (Andresen et al., 2019; Dardis et al., 2018; Monteith, Bahraini et al., 2016), research to further demarcate the health and psychosocial sequelae of IB is warranted. Moreover, research that examines IB in relation to help-seeking (c.f. Holliday & Monteith, 2019) is needed to fully understand how experiencing IB influences recovery.
While the current study builds upon prior examination of the IBQ.2, it is important to interpret findings within the context of limitations. First, rates of undeliverable mailings were high. Additionally, participants with missing IBQ.2 data were excluded from the analytic sample, yet differed on a few demographic and military service characteristics. Third, although items scored as “N/A” were scored as 0, it is difficult to ascertain if this biased results. Fourth, measurement of military sexual harassment and sexual assault was based upon brief yes/no items, precluding more in-depth examination of whether the IBQ.2 had DIF based on other MST-related characteristics (e.g., frequency, duration). The current study also focused exclusively on women who experienced MST and on veterans enrolled in VHA care. Given rates of MST among those who identify as transgender (Lindsay et al., 2016), and research suggesting that IB is salient among men who experience MST (Monteith, Gerber, et al., 2019), examination of the IBQ.2 among transgender and male veterans is warranted. Moreover, by exclusively sampling veterans enrolled in VHA care, it is possible that veterans with the most severe experiences of IB were excluded (c.f. Holliday & Monteith, 2019). Research on the IBQ.2 with other samples of MST survivors, including those not enrolled in VHA care, is warranted.
This is the first study to examine the IBQ.2 among female veterans who experienced MST. Use of EFA and Rasch analysis suggested that, although this measure may be multidimensional, data do not support separating items into different factors. Refinements to the full scale using a combination of traditional and modern psychometric methods, such as Rasch analysis, may help improve measurement properties and clinical utility. Further examination of IBQ.2 remains warranted, particularly regarding optimal methods of scoring to ensure the measure accurately assesses IB among survivors of MST, irrespective of whether they experienced military sexual harassment or assault. Such efforts are essential for ensuring continued research on the impact of IB on health and recovery.
Footnotes
Acknowledgment
We would like to thank the female Veterans who participated in this study. This material is based upon work supported in part by the Department of Veterans Affairs (VA) and the Rocky Mountain Mental Illness Research, Education and Clinical Center for Suicide Prevention.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The views expressed are those of the authors and do not necessarily represent the views or policy of the VA or the U.S. Government. The authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.