
Abstract
The purpose of this study is to explore experiences of stalking behaviors among midwifery students at one Ghanaian university, as well as their association with mental health disorders. Specifically, this study had the following three aims: (a) to identify the frequency of stalking experiences in this population; (b) to explore mental health symptoms, such as depression and anxiety, within this population; and (c) to better understand intervention opportunities related to stalking, including bystander intervention and use of available resources. The study utilized an exploratory mixed-methods design with surveys (n = 118) and focus group discussions (n = 2 with 16 participants) with midwifery students recruited from a centrally located Ghanaian university campus in July of 2018 using convenience sampling. Results indicate a large percentage (80.3%) of participants have experienced stalking behavior(s) within the last six months. Multiple regression analyses demonstrate a statistically significant relationship between any stalking behaviors and depressive symptomatology as well as between unwanted monitoring/following and anxiety. This was reinforced by focus group discussions in which participants discussed the themes of: (a) types of stalking, with a heavy emphasis on using technology for unwanted following/monitoring; (b) positive versus negative perceptions of stalking intentions, where some types of monitoring and following could be seen as forms of flattery or interest; and (c) barriers to seeking help that focused on stigma, cultural barriers, systemic barriers, and personal barriers. Future research should delve more deeply into barriers to existing resources to identify ways to increase accessibility for stalking survivors in connection with mental health services. This study also highlights the need for additional research to more clearly understand stalking in Ghana so that interventions can begin to address mental health services, healthy relationships, communication, and consent.
Introduction
Gender-based violence (GBV) is a global public health epidemic affecting the health and well-being of millions of individuals (Heise et al., 2002). Stalking is a form of GBV, often perpetrated within the context of intimate relationships that is focused on power and control (Spitzberg & Cupach, 2007). Legal definitions of stalking vary, and many countries do not have laws or criminal justice policies specifically related to stalking (Spitzberg & Cupach, 2007; Stalking Risk Profile, 2014). In general, stalking is defined as a pattern of behavior directed at a specific person, which causes fear or substantial emotional distress (Fisher et al., 2002; Tjaden & Thoennes, 1998). There is a lack of empirical research on stalking likely linked to the limited focus on stalking from a policy perspective. Available research indicates, globally, stalking is prevalent among young people, including university students (Sheridan et al., 2016). As with other forms of GBV, there may be a disparity in which individuals are more likely to endorse having experienced specific stalking behaviors rather than self-identify as a stalking survivor (McNamara & Marsil, 2012). Prevalence rates vary dramatically, but most studies with university students indicate high rates of stalking (13.1%-73%) among participants (Maran & Begotti, 2019; Marganski & Melander, 2018; McNamara & Marsil, 2012; Paullet et al., 2009; Reyns et al., 2012; Spitzberg & Hoobler, 2002; Stalking Risk Profile, 2014).
Types of Stalking
Stalking includes behaviors such as unwanted contact (i.e., violating a personal protective order, showing up at one’s home), unwanted following or monitoring (i.e., using technology to monitor location), and threatened or completed harm (i.e., harming the individual being stalking or their loved ones) (Breiding et al., 2014). Stalking behaviors can take a variety of forms, including technology-facilitated stalking and physical stalking. Technology-facilitated stalking (also referred to as cyberstalking, digital abuse, cyberbullying) is the use of electronic communication technologies (e.g., phones and social media) to perpetrate stalking behaviors (Henry & Powell, 2018; Spitzberg & Hoobler, 2002). Due to the ubiquitous nature of digital technology combined with the high rates of social media use among young adults, technology-facilitated stalking is disproportionally impacting young adults (Duggan, 2017; Powell & Henry, 2016), particularly those in the university setting (Maran & Begotti, 2019; Marganski & Melander, 2018; Paullet et al., 2009; Reyns et al., 2012; Spitzberg & Hoobler, 2002). The prevalence of technology-facilitated stalking is likely underreported due to a lack of clarity on its definition, variations in measurement, and lack of reporting due to the nature of the relationship between the perpetrator and survivor (Ahlgrim & Terrance, 2021; Strawhun et al., 2013).
Stalking in Sub-Saharan Africa
Globally, stalking is gaining more recognition as a significant GBV problem faced by individuals from all identities. While there has been limited research on stalking in sub-Saharan Africa, the studies that have been conducted indicate stalking is prevalent. Research among survivors of intimate partner violence with personal protection orders from South Africa found high rates of stalking (58.2%) by an intimate partner (Pengpid & Peltzer, 2014). A study exploring the types of violence women in Mozambique experience found that 35% experienced sexual stalking (e.g., stalking of a sexual nature, including sexual suggestions and pressure to have sex), often perpetrated by someone they knew (Cruz et al., 2014). A recent study in Ghana, found that more than half (55.5%) of 371 university students had experienced stalking behaviors (Chan et al., 2020). These data demonstrate the paucity of research related to stalking behaviors and health consequences among individuals in sub-Saharan Africa and the need for additional research, particularly among young adults at highest risk for stalking.
Consequences of Stalking
Experiencing stalking can lead to negative mental and physical health outcomes. Research among university students has indicated greater rates of general psychological distress and changes in routines and behaviors as a result of experiencing stalking (Amar, 2006). Studies among young adults in South Africa (Jansen van Rensburg, 2017), stalking survivors in the Netherlands (Blaauw et al., 2002), and female university students in Canada (Cripps & Stermac, 2018) have found more specific negative psychological and emotional impacts on the survivor’s mental health, including anxiety, fear, depression, hypervigilance, among other impacts. Stalking by an intimate partner has also been linked to work disruption and poor performance at work (Logan et al., 2007). Like other forms of GBV, stalking has also been linked to injury, poor current health status, and a higher likelihood of developing chronic disease (Davis et al., 2002). These data provide evidence regarding the link between stalking and acute and chronic mental and physical health conditions, as well as changes in routines related to work and school that have the ability to seriously disrupt a survivor’s life.
Purpose
At this time, stalking in Ghana has only been explored with one study, which focused on stalking experiences based on gender, as well as the duration and frequency of experiencing stalking behaviors (Chan et al., 2020). Our study aims to build on these findings by focusing more exclusively on mental health outcomes and survivor’s perceptions of stalking using a mixed-methods approach. The purpose of this study is to explore experiences of stalking behaviors among midwifery students at one Ghanaian university, as well as their association with mental health disorders. Specifically, this study had three aims: (a) to identify the frequency of stalking experiences in this population; (b) to explore mental health symptoms, such as depression and anxiety, within this population; and (c) to better understand intervention opportunities related to stalking, including bystander intervention and use of available resources.
Materials and Methods
Design
The study utilized an exploratory mixed-methods design. Approval was obtained from the Committee on Human Research, Publications and Ethics at a centrally located Ghanaian university and from the Health Sciences and Behavioral Sciences Institutional Review Board at the University of Michigan.
Recruitment and Procedures
All participants were recruited from a Ghanaian university campus in July of 2018 using convenience sampling. Participants were recruited through one student representative from each of the three midwifery cohorts (second, third, and fourth year). The student representatives met with two of the researchers, who explained the survey and the focus group discussions (FGDs). The student representatives then spoke to all students in their cohorts. The representatives provided the researchers with a date and time when the students were available to meet. Inclusion criteria for the participants were: (a) the student was enrolled in the midwifery program at the university at the time of the recruitment, (b) at least 18 years of age, and (c) able to speak and read English, the language of instruction at the university.
Students who volunteered to participate arrived at the designated classroom on the specified date and time. Study team members described the study, participants were provided with the written informed consent document, and then participants were given the anonymous survey. All participants were informed that they could skip any question they wanted to or choose not to participate at any time. All students were offered the opportunity to participate in an FGD immediately following the survey.
Quantitative Measures
Depression was assessed using the self-report Center for Epidemiologic Studies Depression Scale Revised (CESD-10), which has demonstrated high reliability (α = 0.72) and validity within the Ghanaian context (Asante & Andoh-Arthur, 2015). Items assess feelings and behaviors related to depression that an individual experienced over the last week (e.g., “I was bothered by things that usually don’t bother me.”). Responses range from 0 = “rarely or none of the time (less than 1 day)” to 3 = “all of the time (5-7 days).” This measure is composed of 10 items that are summed to create an overall score, with two items being reverse scored. Possible scores range from 0 to 30. A sum score of 10 or above can be used to indicate clinical depression.
Generalized anxiety was measured using the Generalized Anxiety Disorder Scale (GAD-7) (Spitzer et al., 2006). The GAD-7 captures feelings and behaviors related to anxiety experienced over the last two weeks (e.g., “Not being able to stop or control worrying.”). Respondents answer seven questions with response options on a scale ranging from 0 = “not at all” to 3 = “nearly every day.” Scores between 10 and 14 indicate moderate symptoms of anxiety, while scores between 15 and 21 indicate severe symptoms. Reliability of the GAD-7 (α = .67) has been assessed among females in the Ghanaian context and in other West African nations (Barthel et al., 2014).
Stalking behaviors were measured using 16 items from the stalking measure developed by Shorey et al. (2015) combined with 14 questions from the Stalking Behavior Checklist (Coleman, 1997), both of which have been previously used with university students. Respondents were asked to report how often they experienced each stalking behavior in the last six months on a 7-point scale from 1 = never to 7 = 20 or more times. Sample items included “sent unwanted messages,” “attempted to break into your home,” and “followed you.” As well as 29 questions about specific stalking behaviors, participants were asked, “How often were you fearful of someone because they left you unwanted messages, followed you, spied on you, left you unwanted gifts?” Stalking behaviors were broken into three subscales: (a) unwanted contact (13 items, scores range from 13 to 91), (b) unwanted following or monitoring (6 items, scores range from 6 to 42), and (c) threatened or completed harm (10 items, scores range from 10 to 70); see Table 2 for items in each subscale. For the regression analyses, any stalking experiences, as well as the stalking subscales, were recoded as dichotomous yes/no variables.
Focus Group Discussions
The students in their second year chose not to participate in an FGD. From the third-year cohort, seven students (7/56 = 12.5%) chose to participate in an FGD that lasted 48 minutes, and nine students (9/43 = 20.9%) from the fourth-year cohort participated in an FGD that lasted 58 minutes. In both FGDs, participants were asked questions of three broad categories: Their knowledge and attitudes of stalking behaviors (e.g., “What does stalking mean to you?”) Their knowledge and attitudes of resources related to stalking (e.g., “What resources are available around this area for people who have experienced stalking behaviors?”) Their knowledge and attitudes related to bystander intervention techniques when stalking behaviors were portrayed in a fictional example (e.g., “What do you think could have been done to intervene?”)
Data Analysis
Means and standard deviations were calculated for continuous variables, and frequencies are reported for categorical variables. We calculated a series of odds least-squares (OLS) regressions to estimate the effect of stalking on mental health outcomes. Four models were estimated for each mental health outcome, including depression and anxiety. For both outcomes, the first model estimates the effect of any stalking behavior experienced in the last six months. Additionally, we calculated three models to estimate the effect of each form of stalking (unwanted contact, unwanted following/monitoring, and threatened or completed harm) on both mental health outcomes. All models control for age and relationship status (married, in a relationship, or not in a relationship). All analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY).
Qualitative data from the FGDs were audio recorded and transcribed verbatim. The data were then analyzed by three of the authors using the constant comparative method of analysis to identify themes related to knowledge and attitudes about stalking behaviors, resources, and bystander intervention (Glaser, 1978, 1992). Each author read through the full transcript to capture general thoughts, followed by an in-depth reading of the transcript to identify and label general codes. Next, the authors came together to develop categories for the codes. Finally, the two FGD transcripts were reviewed and categorized until each author believed that data saturation had occurred within their coding scheme (Morse et al., 2002). After this, consensus was achieved with all authors. An audit trail and validation with colleagues was used to maintain validity (Sandelowski & Barroso, 2003).
Triangulation of the survey data and FGD themes was then used to ensure completeness of data and to explain concepts and relationships that have not been well explored in Ghana (Bekhet & Zauszniewski, 2012). The FGD themes were therefore reviewed, interpreted, and ultimately described with the survey data results in mind to ensure completeness of the data interpretation.
Results
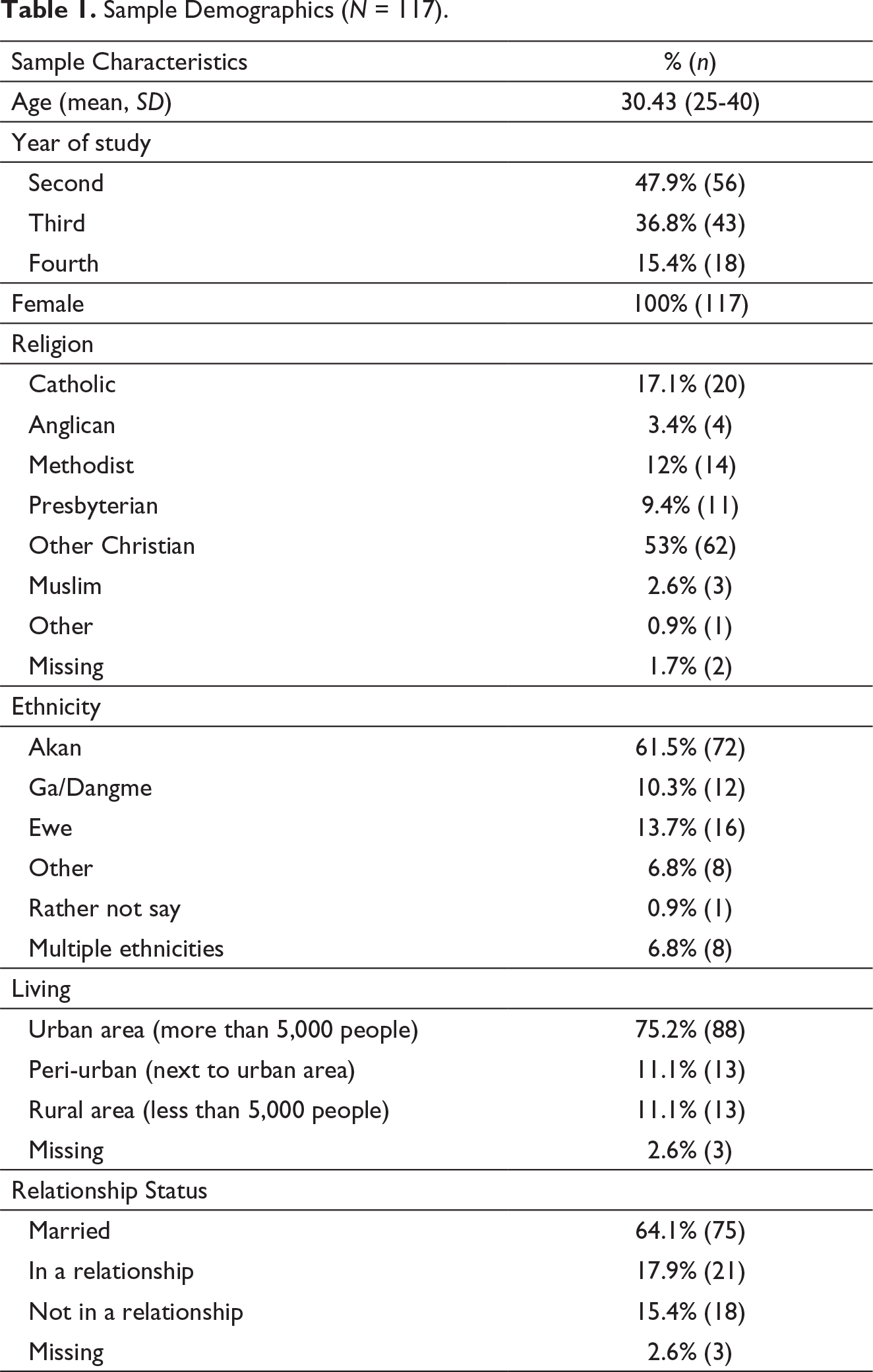
Characteristics of the Survey Sample
Sample Demographics (N = 117).
Prevalence of Stalking Behaviors in the Last 6 Months (N = 117).
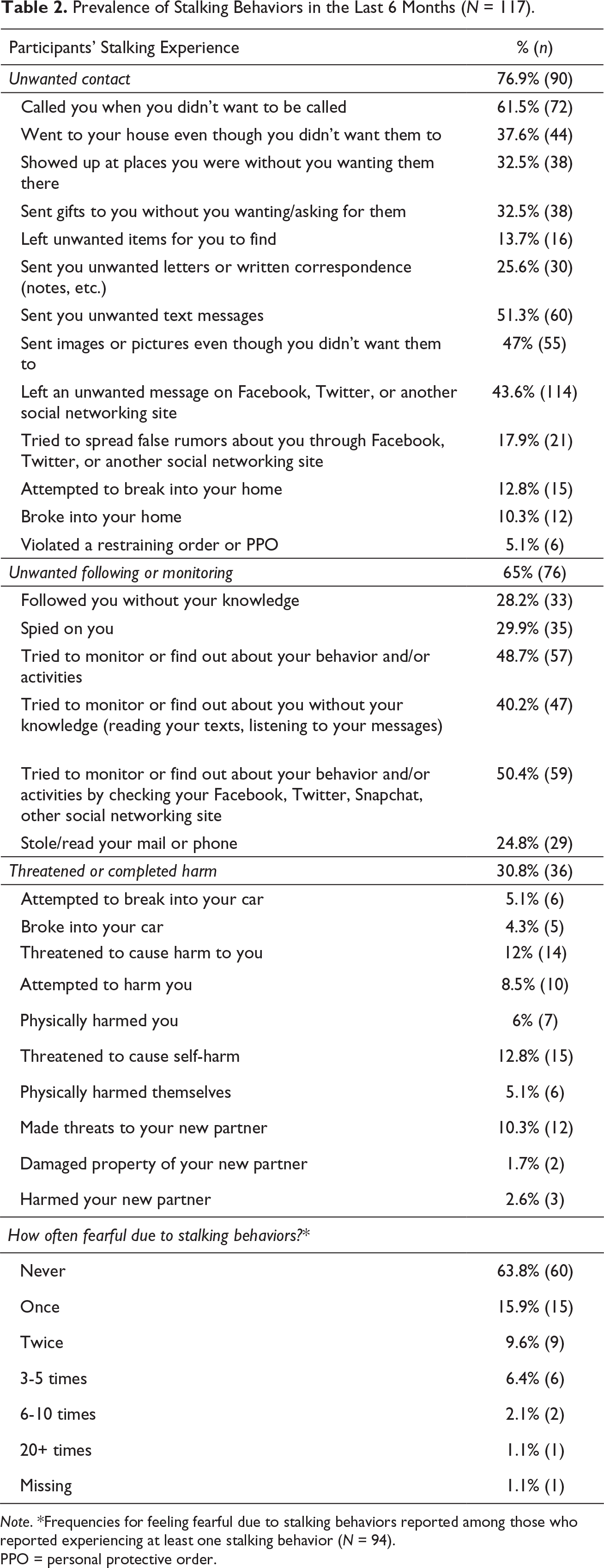
Note. *Frequencies for feeling fearful due to stalking behaviors reported among those who
reported experiencing at least one stalking behavior (N = 94).
PPO = personal protective order.
Mental Health Outcomes (N = 117).
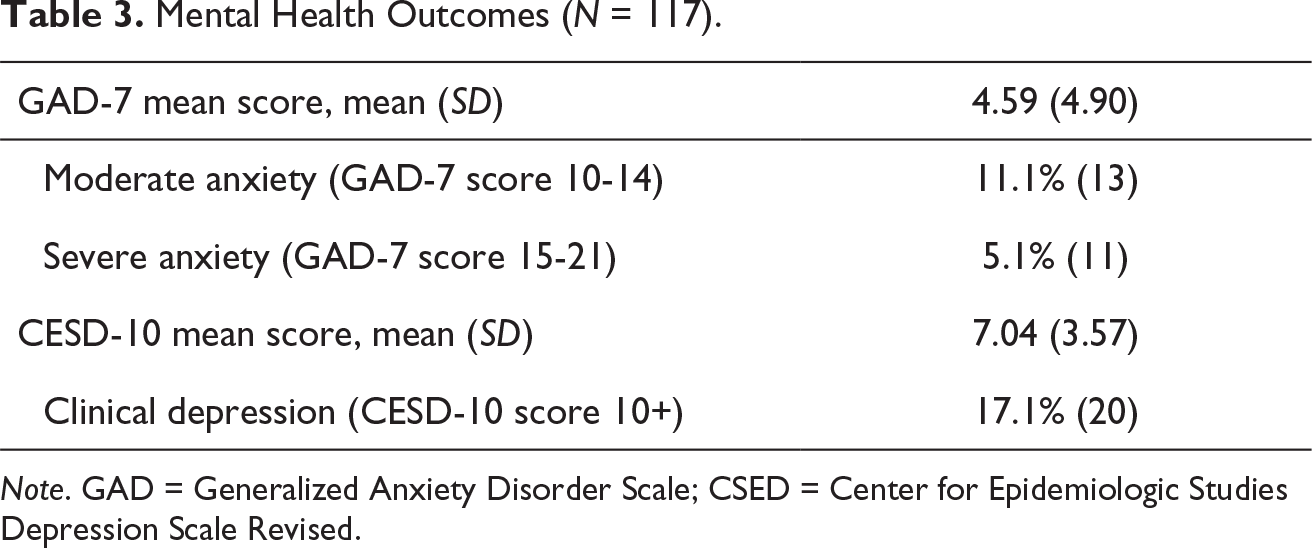
Note. GAD = Generalized Anxiety Disorder Scale; CSED = Center for Epidemiologic Studies Depression Scale Revised.
Regression Analyses
Multiple Regression Results of Depression Symptomatology as Measured by the CESD-10 by Stalking Experiences in the Past 6 Months.
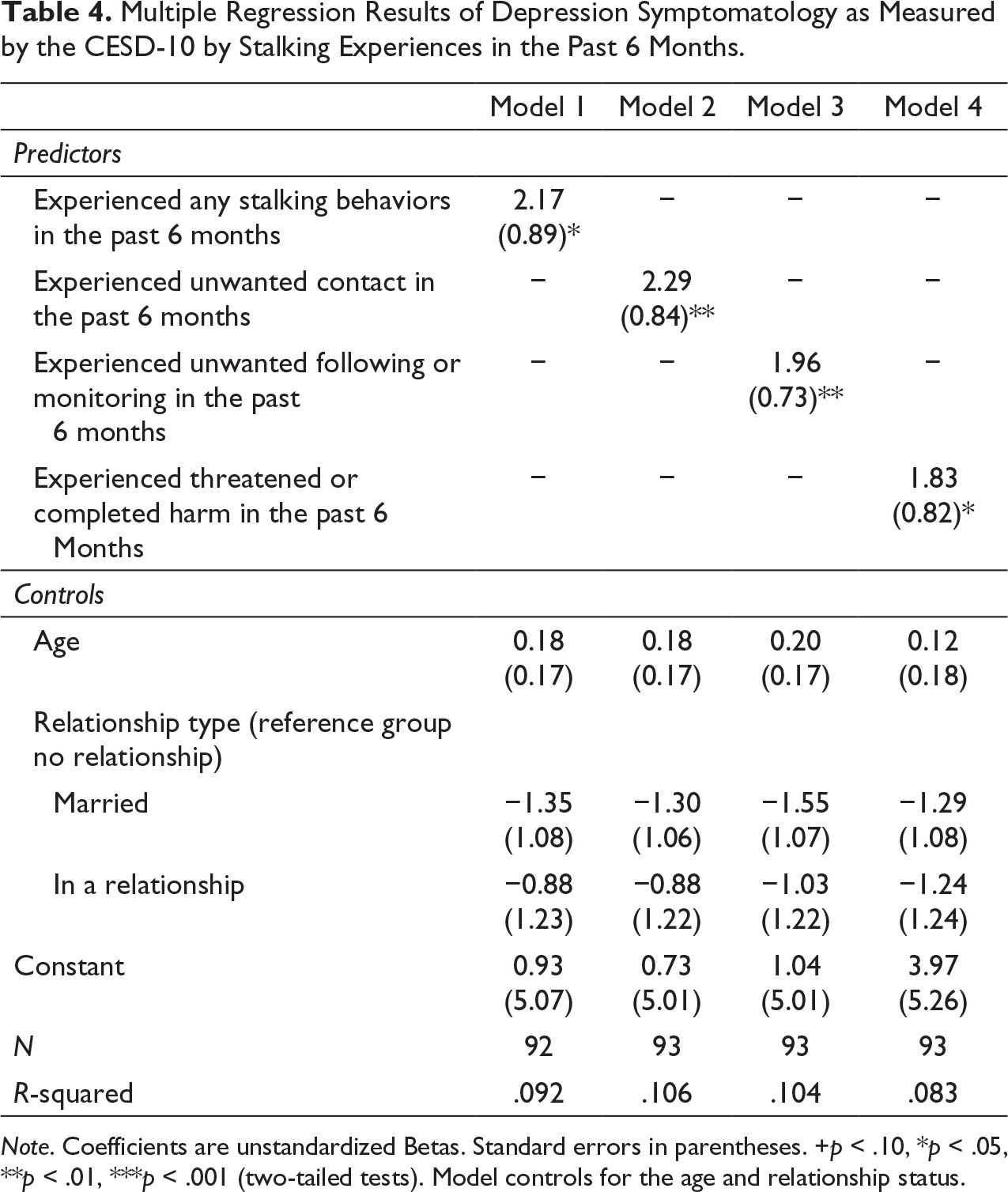
Note. Coefficients are unstandardized Betas. Standard errors in parentheses. +p < .10, *p < .05, **p < .01, ***p < .001 (two-tailed tests). Model controls for the age and relationship status.
Multiple Regression Results of Anxiety Symptomatology as Measured by the GAD-7 by Stalking Experiences in the Past 6 Months.
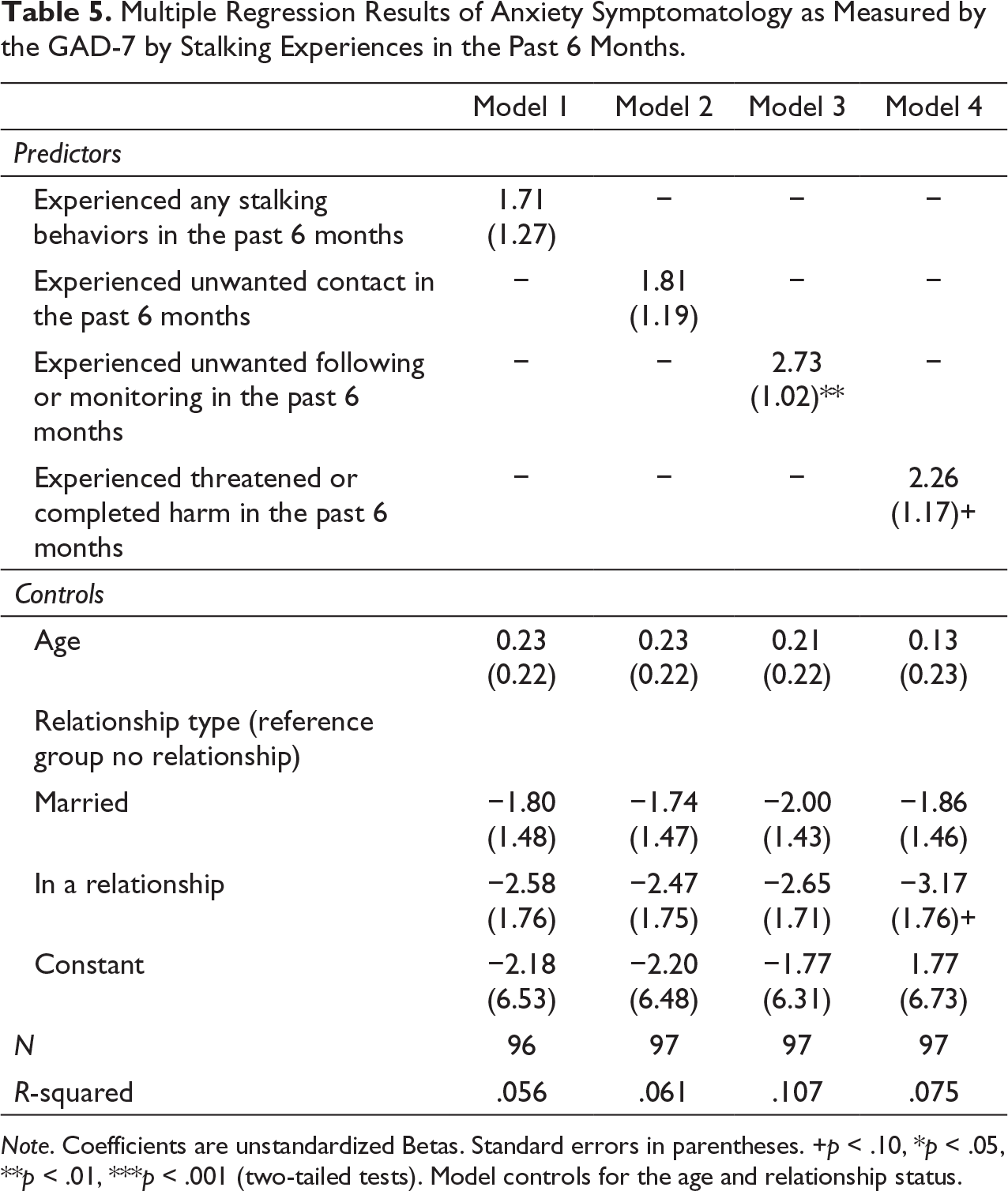
Note. Coefficients are unstandardized Betas. Standard errors in parentheses. +p < .10, *p < .05, **p < .01, ***p < .001 (two-tailed tests). Model controls for the age and relationship status.
Stalking Themes
A total of 16 students participated in two FGDs. Three themes emerged from the qualitative data: (a) types of stalking, (b) positive versus negative perceptions of stalking intentions, and (c) barriers to seeking help.
Types of Stalking
Participants discussed several types of stalking that corresponded with the quantitative categories of stalking that included: (a) unwanted contact, (b) unwanted following/monitoring, and (c) threatened or completed harm.
Participants described unwanted contact as physically following an individual or knowing their schedule and appearing unannounced at their house, school, or place of employment. For instance, one participant described their personal experience as “The stalking behavior I experienced … the person knew my schedule. Every now and then he’s at my place. He doesn’t care the number of hours he has to spend waiting.”
Unwanted following/monitoring was primarily described by participants as using technology-based modalities to track someone or message them constantly. One participant described stalking using technology-based modalities as “Someone always looking through your phone, checking your messages, your mail, and always trying to find out who else call you today, who didn’t call you today, what did you do.”
Finally, threatened or completed harm was linked to escalating violence and could involve threats to the individual or their friends and family. For example, one participant noted that physical stalking was often associated with escalating violence: “Sometimes they tend to follow you. Most often it is [an] ulterior motive. Either they want to harm you or do any form of abuse to you. It can be rape; it can be violence.” Another participant noted how friends and classmates can experience threats or harm: “…and he sees you with another colleague who is a guy, then that guy is doomed. He’ll be punishing that guy only really because it turns that he has an interest in you.”
Positive Versus Negative Perceptions of Stalking Intentions
Participants delineated a clear difference between positive and negative perceptions of stalking intentions. Positive stalking intention was described as men who were interested in getting to know a woman and wanting to be their friend, which was more well received if the woman was interested in the man. This is reflected in a quote by one of the participants:
We can have positive stalking. Like the person admires you, the person wants to be close to you and always follows you around without your knowledge but not necessarily the person harming you or something. Their intentions should not always be bad. At times they are positive intentions and at times they are negative.
Another participant described their behavior when interested in another person as, “more or less like stalking, but this, you’re not doing this to harm the person. Yes. It’s like a positive something.”
Negative stalking intention usually was described as having a more sinister element. The fear of negative stalking is reflected by one participant who noted, “Most of the time it’s obsession. They want to have you by force. So, whether you resist, or you don’t resist, they want you. So, they are coming for you.” The participants identified obsession, financial gain, or sexual drive as motives for stalking. They also mentioned that negative stalking intention usually resulted in violence or abuse, such as rape or assault. This is illustrated by one participant’s statement, “If it’s in the negative. I’ll be much afraid, yes. Because my life would be in trouble.” This element of fear or distress is foundational to the definition of stalking.
Barriers to Seeking Help
Participants noted that there are social structures in place to assist with experiences of GBV, such as stalking. These include the Ministry for Gender and Social Protection, the police, hospitals, social workers, and psychological counseling units. However, participants noted a number of barriers in accessing services at these structures, such as stigma, cultural barriers, systemic barriers, and personal barriers.
One woman described stigma as follows:
So people feel they would kind of be left alone, …. So that’s the stigma I’m talking about. So, people face such cases and they don’t, they just want it to be settled in their families and is like there is, there is a taboo. You shouldn’t even speak of it outside. It’s just known among the few people [who] just got to know of it and that’s it. Case closed.
Other participants reported that even if they go to the police, they may be questioned about, “What happened?,” “Are you sure?,” “Why did you go to [insert location]?,” and “Can you bring evidence?”
The cultural context also creates barriers to both identifying stalking behaviors and receiving resources. Participants discussed how nonverbal cues and their upbringing makes it difficult for them to verbally say yes to relationships and sexual behaviors. Participants described this as being related to religion and the “upbringing we all had … in Africa.” This means that many interactions involve nonverbal cues that can be misinterpreted. One participant stated,
Sometimes the person, the person sees you and he says something, you give a wink and the person realizes that, okay, I can take it up to that point. Or the person sees you, … because there are people there you don’t talk. I can just raise the shoulders to let the person know I’m in. But I can’t talk because there are people here. If the person says something you give the person a smile to let him know that I can still continue.
Systemic barriers discussed included the need to pay for transportation, the materials for a clinical exam, and the lack of resources related to forensic exams and mental health services. This is reflected in a quote from one participant who said, “It looks like it’s not much integrated in our system. Things are not up and doing. So, we lack that basic protection from these structures, that could have helped to protect the individuals.” Participants recognized the benefit of utilizing psychological counseling as a resource for cases such as stalking, but also noted barriers. One participant noted:
The counseling problem is sometimes you have to pay for the counseling. And it’s not like you have the money to go pay for the counseling. It makes it difficult for people to access those units because of what you have to provide before you get that counseling.
Another participant mentioned that people unfamiliar with an area, such as summer students on campus, may not know how or where to access counseling through their university.
Personal barriers were present when the individual had a relationship with the stalker or children were involved. This sentiment is illustrated by the following quote: “These situations where there are kids involved, the woman is being abused by the husband, because of the kids, she has to stay and take care of them.” Meanwhile, participants alluded to the fact that stalking is an issue they need to deal with on their own or with friends and family in comments such as “manage it on your own.”
Triangulation of Results
A mixed-methods approach allows for triangulation of the data to provide a more complete picture of stalking among university students in central Ghana. The survey data indicate that a large percentage of participants report experiencing stalking behaviors within the last six months. The FGDs expand our understanding of these stalking behaviors by introducing the taxonomy of positive and negative perceptions of stalking intentions that participants use to differentiate flattering and desired attention from unwanted and more sinister behaviors.
Both survey and FGD data highlight the relationship between stalking and mental health symptomatology. In particular, the survey data demonstrate the significant relationship between any type of stalking and depressive symptomatology, as well as the significant relationship between unwanted following/monitoring and anxiety. The FGD data further illuminate the unique barriers to accessing mental health resources in Ghana. Mental healthcare access is limited by physical availability and cost. Further, difficulty accessing needed resources may contribute to an exacerbation of mental health symptomatology.
Discussion
The results demonstrate a relationship between mental health, primarily depression, and experiences of stalking among female university students in Ghana. The FGDs also demonstrate the unique role that systemic and cultural nuances play in understanding stalking, relationships, and perceptions of behavior.
The connection between stalking, depression, and anxiety among university students has been documented outside of Ghana (Amar, 2006); however, the current study demonstrates there is also a relationship between stalking and mental health that may warrant further research in Ghana. Current assessments of mental health services in low- and middle-income countries suggest a high level of unmet need for mental health services, with only 25% of mental health service seekers having access to services (Badu et al., 2018). Research in Ghana has noted there are numerous barriers to accessing mental health services, including individual barriers like attitudes/stigma, perceived efficacy of treatment, and knowledge about services, as well as systemic barriers such as cost, transportation, and location of services (Badu et al., 2018). There have been attempts to centralize services for survivors of GBV in Ghana into a “one-stop” clinic that incorporates physical health, mental health, social, and legal services. However, these efforts are generally regional and inaccessible to those in rural or peri-urban locations. It is clear stalking survivors would benefit from more accessible mental health services to address acute mental health concerns and prevent long-term sequelae.
The survey data indicate experiencing stalking behaviors was not uncommon, while participants in the FGDs introduced the idea that perhaps not all stalking experiences are perceived as having negative intentions. The two disparate types of perceived stalking intentions described by participants reinforce the notion that some forms of power and control may be accepted in Ghanaian culture, as illustrated by national data that justifies intimate partner violence in certain scenarios (Dickson et al., 2020). Importantly, the perception that there may be socially acceptable stalking behaviors is not limited to Ghanaian culture. Research in the United States has found that certain stalking behaviors, particularly those that are technology-facilitated, such as multiple messages or social media monitoring, can be perceived as part of a courtship experience or as helping to assess compatibility (Cruz et al., 2014; Howard et al., 2019; McKenna et al., 2002).
Additionally, although 80.3% reported an experience of at least one stalking behavior, 35.1% of those who experienced stalking reported feeling fearful due to these stalking behaviors. Because the presence of fear or distress defines stalking, it is vital to understand if this discrepancy is due to a positive perception of stalking intentions on the part of the individual involved—such as those who described stalking in courtship situations—as this may account for an important gap between how stalking is measured/defined and how some people perceive and discuss their experiences of stalking behaviors. Additional research is necessary to further understand this phenomenon of perception versus definition related to the presence of fear or distress in stalking in Ghana.
The FGDs also elicited important information about the use of nonverbal cues to show interest in a potential partner and highlighted the significance of a participant’s cultural and religious upbringing in contributing to their knowledge and attitudes about stalking. This has been illustrated in past work in Ghana about other forms of GBV (Munro-Kramer et al., 2020). These nonverbal cues have the potential to lead to confusion about a potential partner’s desire and could also contribute to the way in which stalking behaviors are perceived (positively or negatively).
In discussions about GBV, stalking is often overlooked, and the lack of clear definitions, research, and policy has contributed to ambiguity in what can and should be classified as a stalking behavior (Spitzberg & Cupach, 2007; Stalking Risk Profile, 2014). This could have implications for future education and research. More education may be needed to help university students and young adults understand healthy relationships and which behaviors may indicate potentially unhealthy or even abusive behaviors, especially within technology-facilitated modes of communication. It also appears that intentionality needs further exploration and that, in the future, researchers may want to investigate the motives behind stalking-like behaviors (i.e., to do harm or to initiate a relationship).
Limitations
As an exploratory study, researchers deemed it important to use a mixed-methods approach to try to understand the nuances of stalking experiences, which highlighted the prevalence and understanding of stalking among Ghanaian university students. However, the study had some limitations. First, the sample was comprised entirely of female-identifying university students at a single institution in central Ghana, which precludes generalizability. Second, the self-reported nature of the data could have led to bias in terms of social desirability. Researchers tried to mitigate this factor by having the surveys be anonymous. Third, the surveys were distributed in a paper format, which may have contributed to missing data or misread/misinterpreted questions. Fourth, the FGDs only included those that self-selected to participate, leading to potential bias. It is possible that some individuals with personal experiences of stalking may not have felt comfortable talking about them in a group and therefore chose not to participate in the FGDs. Fifth, although research shows most stalking is carried out in intimate relationships (Spitzberg & Cupach, 2007), participants in this study were not asked to identify the nature of the relationship with the person (or people) who carried out the stalking behaviors. Finally, causality cannot be established with the cross-sectional data. Future research should focus on a more diverse sample that includes nonfemale-identifying individuals. Future researchers should also consider the format for data collection. There is much more to learn about the experiences of stalking in Ghana, and additional research with a broader population, especially around cultural norms and values relating to relationships, is needed.
Conclusions
This study illustrates that large numbers of Ghanaian university students have experienced stalking behaviors. Future research should delve more deeply into barriers to existing resources to identify ways to increase accessibility for stalking survivors in connection with mental health services. This study also highlights the need for additional research to understand stalking more clearly in Ghana so that interventions can begin to address mental health, healthy relationships, communication, and consent.
Footnotes
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the Office of Global Public Health through the University of Michigan in March 2018.