
Abstract
Intimate partner violence (IPV) during pregnancy is a significant issue. Nevertheless, the prevalence of IPV and its adverse outcomes in pregnant women in Saudi Arabia are not well documented. This study examines the prevalence of IPV, its relationship with women’s background characteristics, and its effect on adverse pregnancy outcomes. A cross-sectional study was conducted using a convenience sample of 684 women who were either pregnant or in the first six weeks postpartum in Riyadh, Saudi Arabia. IPV severity was measured using the Composite Abuse Scale. The results showed that 28.9% of the women included in this study experienced IPV. Smoking habit, income, polygamous marriage, presence of chronic diseases and sexual dysfunction, and number of children were significantly associated with IPV severity. In each one-unit increase in total IPV severity, the possibility of the occurrence of preterm labor, vaginal bleeding, dehydration, gestational diabetes, urinary tract infection, spontaneous abortion, and intrauterine growth retardation significantly increases. Furthermore, regarding the types of abuse, we found that for each one-unit increase in verbal abuse, the possibility of the occurrence of preterm labor, dehydration, urinary tract infection, and intrauterine growth retardation significantly increases. Moreover, for each one-unit increase in physical abuse and one-unit increase in controlling behavior, the possibility of the occurrence of intrauterine growth retardation significantly increases. The current results highlight the importance of paying substantial attention to IPV and its types as a health issue that increases the risk of adverse pregnancy outcomes in women. A clinical assessment during pregnancy is needed to identify and manage cases of IPV survivors and ultimately reduce their risk of IPV.
Introduction
Intimate partner violence (IPV) against women is a global public health concern, with 30% of women, at the global scale, having experienced it (García-Moreno, 2013). IPV is a pattern of coercive control (Gou et al., 2019), physical and sexual violence, or psychological abuse (Center for Disease Control and Prevention, 2018). Pregnancy is a milestone in the lives of individuals and is a sensitive time, when women become vulnerable to IPV because of pregnancy-related stress, with men using power to control women or resorting to a previous pattern of violence (Taillieu & Brownridge, 2010). Among murdered pregnant or postpartum women, more than half had experienced intimate partner homicide (Cheng & Horon, 2010). Research has examined the prevalence of IPV during pregnancy, suggesting that IPV escalates or remains the same during pregnancy (Brownridge et al., 2011), whereas another study suggested that IPV during pregnancy occurs at lower levels than that throughout a lifetime in most countries (Devries et al., 2010). However, it occurs not only during the antenatal period but also during preconception and postpartum (Groves et al., 2015; Taillieu & Brownridge, 2010).
In different part of the world, it is estimated that IPV during pregnancy can range from 1.4% to 57% (Australian Institute of Health and Welfare [AIHW], 2015; Daoud et al., 2012; Devries et al., 2010; Shamu et al., 2011; Wang et al., 2017). These studies suggested wide-ranging estimates resulting from IPV conceptualization and measures, various samples, and more importantly sociocultural differences. The prevalence of IPV (Ozaki & Otis, 2017; Rodriguez Martinez & Khalil, 2017) and the extent of protection of women from abuse are influenced by cultural norms (Hatcher et al., 2013; Pun et al., 2016). Cultural structure and socioeconomic status shape couples’ attitudes and behaviors during pregnancy and postpartum (Chimatiro et al., 2018; Taşçi-Duran & Sevil, 2013). Based on the perception of cultural society, husbands or partners might be seen as protectors who help relieve maternal stress of pregnant women (Alio et al., 2013). Several variables are associated with women experiencing IPV during pregnancy, including socioeconomic status, age, and minority group status (Taillieu & Brownridge, 2010). Several studies have shown the education and occupation of a partner to be risk factors for IPV during pregnancy (Azene et al., 2019; Martin et al., 2004). Moreover, the number of children in the family may be linked to the prevalence of IPV experiences among pregnant women (Peedicayil et al., 2004; Wang et al., 2017). Smoking is also associated with IPV during pregnancy (Cheng et al., 2015; Crane et al., 2013). In general, IPV can lead to serious health side effects; therefore, IPV during pregnancy has a negative impact on the mother and fetus and increase the risk of abortion (Pallitto et al., 2013) and preterm birth (Hill et al., 2016). It has also been shown to increase newborns’ risk of low birth weight and of being small for their gestational age 4.2-fold and 4.8-fold, respectively (Alhusen et al., 2015). The negative health effects may be explained by the theory of allostasis, which states that stress during pregnancy leads to allostatic responses that manifest as adverse pregnancy outcomes (Shannon et al., 2007). That is to say, allostasis is a theory that explains psychoneurohormonal responses to stress (McEwen, 1998). Adverse pregnancy outcomes are defined as health issues during pregnancy that affect the health of the mother and fetus, causing health problems, such as gestational diabetes, hypertension, severe nausea, and vomiting (hyperemesis gravidarum), and urinary tract infection (Center for Disease Control and Prevention, 2020).
A majority of the existing studies on IPV during pregnancy have been conducted in Western countries. Therefore, research on the pregnancy outcomes related to IPV in developing countries is needed because the effects of IPV on pregnancy might differ across cultures (Hill et al., 2016). IPV is a cultural issue, and therefore, perceptions, conceptualizations, and interpretations of IPV vary across nations (Martín-Fernández et al., 2020). In Arab countries, including Saudi Arabia, women have recently become empowered and have begun participating fully in the labor force (Naseem & Dhruva, 2017). In addition, collectivist attitudes in the Arab world, as well as attitudes toward gender roles, influence understandings of IPV (Mojahed et al., 2020). For example, 49% of Saudi women believe that they should obey their husbands’ diktats, and 80.5% of women think that IPV is a family issue (Eldoseri et al., 2014), thus about 41% decided not to seek help and disclose their IPV experience (Alhalal, Ta’an, et al., 2019). However, the country passed the Law of Protection from Abuse that bans abuse and mandates reporting by professionals and citizens (Bureau of Experts at the Council of Ministers, 2013) as well as providing domestic violence hotline. Among Saudi women the prevalence of IPV during lifetimes ranges from 34.3% to 57.7% (Alhalal, Ta’an, et al., 2019). Therefore, research findings produced by Western scholars cannot be generalized to women in Saudi Arabia as their contexts are different.
Although the impact of IPV during pregnancy on maternal and fetal health is critical, only a handful of studies on IPV committed against pregnant Arab women have been conducted. They showed that experiencing IPV was significantly associated with pregnancy (Daoud et al., 2017) and that 6.9–44.1% of pregnant women experienced IPV (Abdelhai & Mosleh, 2015; Anson & Sagy, 1995; Clark et al., 2009; El-Zanaty et al., 1996; Fisher et al., 2003; Hammoury & Khawaja, 2007; Hammoury et al., 2009; Ibrahim et al., 2015; Khawaja & Tewtel-Salem, 2004; Okour & Badarneh, 2011; Oweis et al., 2010). Some of these studies focused only on physical violence during pregnancy (Hammoury & Khawaja, 2007; Khawaja & Tewtel-Salem, 2004), whereas others examined other aspects of abuse, using single-item questions. For example, the Hurt-Insult-Threaten-Scream inventory has four items on the frequency of being hurt, insulted, threatened, or cursed (Abdelhai & Mosleh, 2015), and the Abuse Assessment Screen has five items on feeling afraid and being emotionally, physically, and sexually abused (Hammoury et al., 2009). Moreover, only one study focused on the maternal and fetal outcomes among pregnant Egyptian women (Ibrahim et al., 2015). In Saudi Arabia, two studies have investigated the prevalence of IPV during pregnancy and found that 21–78% of Saudi women experienced IPV during pregnancy (AboulAzm et al., 2009; Rachana et al., 2002). The maternal health effects of IPV have been documented, including abruptio placentae, low weight gain during pregnancy, and premature labor (AboulAzm et al., 2009; Fageeh, 2014; Rachana et al., 2002). However, these studies were limited in the manner in which they developed their own scales to examine IPV without examining their reliability and validity (AboulAzm et al., 2009; Rachana et al., 2002). In addition, Rachana et al. (2002) focused only on physical abuse and overlooked how sexual and psychological abuse affects maternal health. Moreover, coercive control is an essential aspect of violence because it is highly linked to gendered IPV (DeKeseredy & Schwartz, 2011; Stark, 2007), and it might negatively restrict women’s choices toward productive health, prenatal care, and nutrition.
The issue of adverse pregnancy outcomes as a result of IPV in relation to Saudi women has received limited attention. A comprehensive understanding regarding the adverse pregnancy outcomes in the context of IPV on women in Saudi Arabia is needed to raise the profile of IPV as a health issue meriting healthcare system attention. Pregnancy is a unique period when women interact with the healthcare system, giving the latter an avenue to identify IPV survivors, provide needed services, and tailor interventions aimed at preventing violence, protecting women, and mitigating its negative consequences. Policymakers should make decisions and advocacy efforts in addressing IPV, armed with adequate knowledge of the adverse effects of IPV on pregnancy. The finding can then be used in other Arab contexts because the term “Arab” denotes an ethnoreligious grouping that unifies people, language, and religion, thereby influencing its homogeneity (Dhaouadi, 2013) and cultural uniformity (Obeidat et al., 2012).
This study explores the prevalence of IPV, its relation to women’s background characteristics, and its adverse effects on pregnant and up-to-six-weeks postpartum women in Saudi Arabia. The study has the following hypotheses based on the theory of allostasis: (a) higher levels of total IPV severity increase the likelihood of women in Saudi Arabia experiencing adverse pregnancy outcomes and (b) higher levels of sexual, verbal, and physical abuse and controlling behaviors meted out to women increase the likelihood of Saudi women experiencing adverse pregnancy outcomes. The adverse outcomes are preterm labor, premature rupture of membranes, gestational hypertension, gestational diabetes, vaginal bleeding, abnormal placentation, nausea and vomiting, dehydration, urinary tract infection, spontaneous abortion, induced abortion, and intrauterine growth retardation.
Method
Study Design, Setting, and Participants
A hospital-based cross-sectional observational study was conducted. A convenience sample of pregnant women was recruited from the obstetrics and gynecology (OB/GYN) outpatient, inpatient, and emergency departments at a teaching hospital in Riyadh, Saudi Arabia. Women who were pregnant for more than six weeks of gestational age and those within the first six weeks of the postpartum period were invited to participate in the study. However, women accompanied by their husbands or child aged more than 2 years who could verbalize were excluded on the basis of WHO guidelines to protect woman safety (World Health Organization, 2014). Even so, a majority of women were not accompanied by anyone. In total, 750 women were selected; however, 38 women refused to answer the questionnaires. Thus, 712 women were enrolled in the study, with a response rate of 94.9%. Twenty-eight participants had substantial missing data; therefore, only 684 participants were included in the analysis. The sample size was calculated using the logistic regression test on G*Power with an alpha of 0.05 and a power of 0.80, detecting odds ratios (ORs) equal to 1.3. Therefore, the adequate sample size was 568.
Data Collection
Data were collected between December 2019 and March 2020. The study was advertised in the hospital as one on women’s health, aimed at understanding the stress during pregnancy and postpartum periods and certain health outcomes. The data collectors screened the selected women for eligibility. After providing a verbal description of the study purpose, informed consent was obtained from each woman before data collection began. Data were collected using structured interviews as all questionnaires were self-reported. Standardized protocols were used to conduct the interviews in a private area where women could answer in privacy. Each interview took approximately 10–15 minutes to complete.
Ethical Consideration
The institutional review board of the hospital (#) approved the study before data collection. To protect the women, personal identification information was not collected in order to ensure anonymity and confidentiality. The data file was encrypted and saved in a password-protected laptop with a back-up copy saved on a memory stick. The data collectors were trained, and if signs of distress were observed, support was provided to the women enrolled. The national 24-hour domestic abuse hotline for the Ministry of Social Affairs was given to any woman who asked for help related to abuse. At the end of each interview, debriefing was conducted inquiring into how the women felt upon finishing the interview.
Measures
To gather data on the background characteristics of the women enrolled in this study, survey questions were used. These questions asked the women about their age, education, income, employment status, number of years of marriage, smoking, polygamous marriage, the use of contraceptives, and the presence of chronic diseases. Their electronic medical records were assessed to retrieve information related to pregnancy outcomes.
IPV severity was assessed using the Arabic version of the Composite Abuse Scale (CAS) (Alhalal, Ford-gilboe et al., 2019). It is a 30-item self-report scale that measures women’s experience of IPV in the past 12 months (Hegarty et al., 2005). The women can rate each item using a 6-point Likert scale, ranging from 0 (never) to 5 (daily). The total score can be computed by summing the scores on all items to measure IPV severity, yielding score ranges from 0 to 150. The widely used cutoff scores of 3 and 7 have been used as criteria for exposure to IPV (Gartland et al., 2016; Loxton et al., 2013). The CAS was translated, and its validity among Saudi women was assessed (Alhabib et al., 2013). On the basis of the validity, a 27-item version of the CAS with the subscales of sexual abuse, verbal abuse, physical abuse, and controlling behaviors (Alhalal, Ford-gilboe, et al., 2019) was used. The current study showed reliability because the Cronbach’s alpha was 0.954 for the total score, 0.851 for sexual abuse, 0.770 for verbal abuse, 0.930 for physical abuse, and 0.926 for controlling behaviors.
Analysis
All data analyses were performed using Statistical Package for the Social Sciences (SPSS), version 26 (IBM Corp., Armonk, New York, USA). Data were examined to assess the extent to which data was missing. Afterward, data were analyzed using three steps. First, descriptive analysis was conducted to assess the participants’ background characteristics. Second, the relationships between the participants’ background characteristics and IPV severity were assessed using the Spearman and point-biserial correlation coefficients. In addition, the Kruskal–Wallis test and the Mann–Whitney U-test were conducted to evaluate the differences in IPV severity between different categories of the participants’ background characteristics. Third, the study hypotheses were tested using binary logistic regression using each adverse outcome as a dependent variable, and potential confounding factors were controlled. These confounding variables were selected on the basis of the existing literature, which revealed that a woman’s age, education, income, and smoking habit might influence pregnancy outcomes (Jesmin et al., 2014; Luo et al., 2006). Logistic regression was first performed using total IPV severity as an independent variable to determine how well total IPV can predict each adverse outcome (dependent variable). Binary logistic regression was performed again using the four abuse types (sexual abuse, verbal abuse, physical abuse, and controlling behaviors) as independent variables and each adverse pregnancy outcome as a dependent variable to assess how the type of abuse can predict adverse outcomes. Although significant relationships were found between the types of abuse, there was no evidence of multicollinearity. We tested 12 adverse outcomes: preterm labor, premature rupture of membrane, gestational hypertension, gestational diabetes, vaginal bleeding, abnormal placentation, nausea and vomiting, dehydration, urinary tract infection, spontaneous abortion, induced abortion, and intrauterine growth retardation. These adverse outcomes were coded as binary outcome variables (presence or absence). Given the possibility of these adverse pregnancy outcomes being interrelated, we assessed the associations among them using Chi-square analysis while examining the Phi coefficient to determine the strength of the association. Total IPV severity and abuse types have many skewness and kurtosis issues: total IPV severity (skewness = 3.79; kurtosis = 15.53), sexual abuse (skewness = 2.95; kurtosis = 9.05), verbal abuse (skewness = 2.76; kurtosis = 8.39), physical abuse (skewness = 4.32; kurtosis = 20.47), and controlling behaviors (skewness = 4.43; kurtosis = 20.32). Thus, a square root transformation was performed for total IPV and each type of abuse to be used in regression analyses.
Result
Participants’ Background Characteristics
The background characteristics of the participants (n = 684) are summarized in Table 1. Most participants (41.8%) were aged between 31 and 40 years. Moreover, most participants (57.9%) were housewives, and only 11.7% completed a university degree. Only 5.1% of the participants were smokers. In terms of their personal income, the majority (85.4%) earned less than SR 10,000. Among the pregnant women, the gestational age on average was 26.40 weeks (SD, 9.24 weeks; range, 6–40 weeks). Only 13.9% were within the first six weeks of the postpartum period. On average, they had 2.43 children (SD, 1.61; range, 0–10), and they had been married for 7.53 years on average (SD, 5.56 years; range, 0–30 years).
From the cutoff score for IPV on the 27-item CAS, we can infer that 28.9% of the women experienced IPV during the past 12 months. The mean total IPV severity was 5.02 (SD, 12.11; range, 0–85). On average, they experienced sexual abuse to the extent of 0.57 (SD, 1.149; range, 0–10), verbal abuse to the extent of 1.72 (SD, 3.39; range, 0–22), physical abuse to the extent of 1.05 (SD, 3.56; range, 0–30), and controlling behavior to the extent of 1.46 (SD, 4.92; range, 0–34).
Relationship Between Participants’ Background Characteristics and IPV Severity
The Spearman and Point-biserial correlation coefficients showed that the number of children (rs = .122; p = .005), income (rs = .083; p = .030), smoking (rpb = .328, p < .001), polygamous marriage (rpb = .273; p < .001), presence of chronic diseases (rpb= .188; p < .001), and sexual dysfunction (rpb = .111; p = .004) were significantly correlated with IPV severity, whereas age (rs = .047; p = .224), education (rs = –.069; p = .073), and occupation (rs = –.077; p = .054), and being a mother (rpb = .028; p = .460) were not significantly correlated with IPV severity.
Background Characteristics for the Participants and IPV Severity (n = 684).
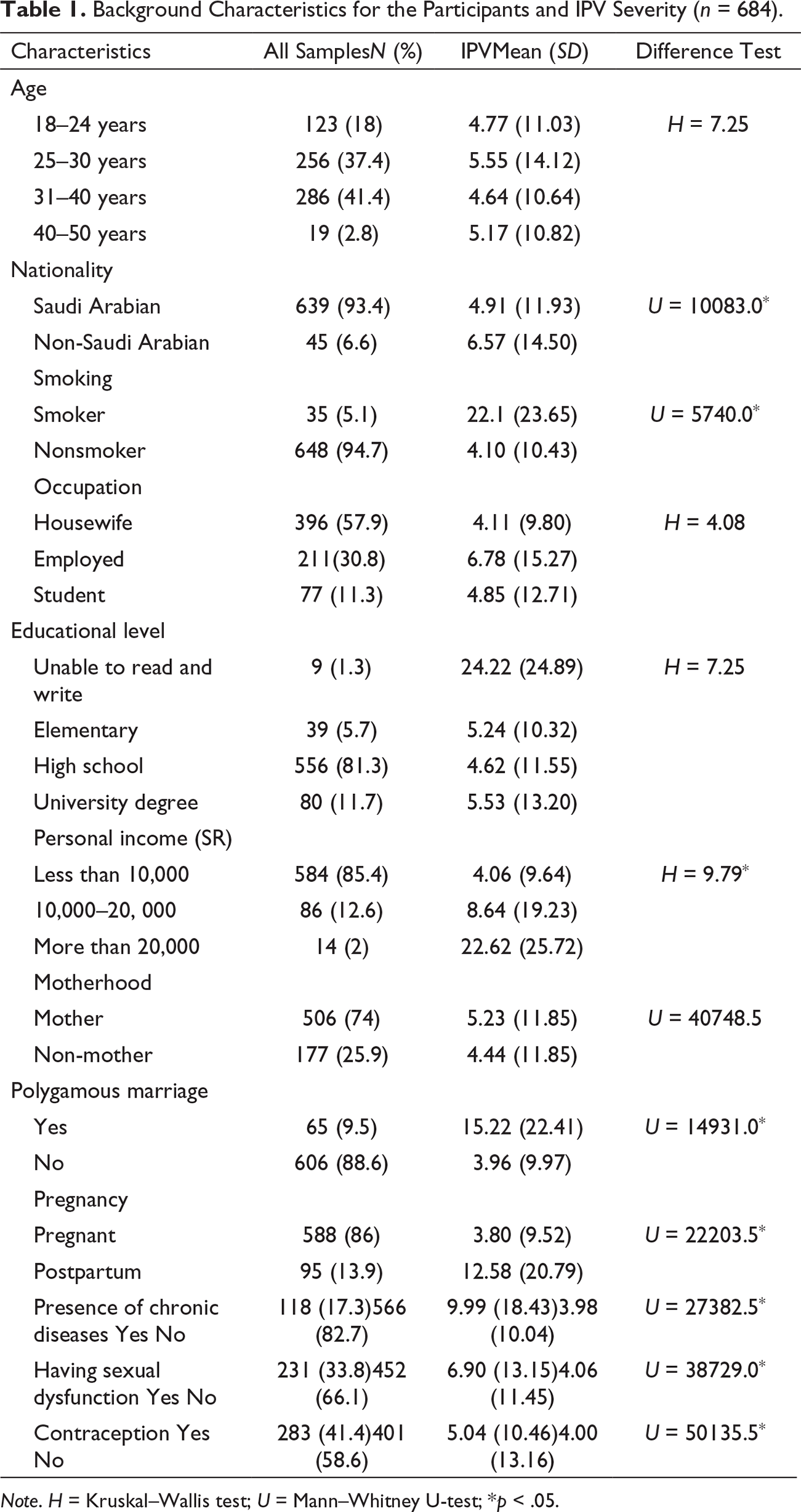
Note. H = Kruskal–Wallis test; U = Mann–Whitney U-test; *p < .05.
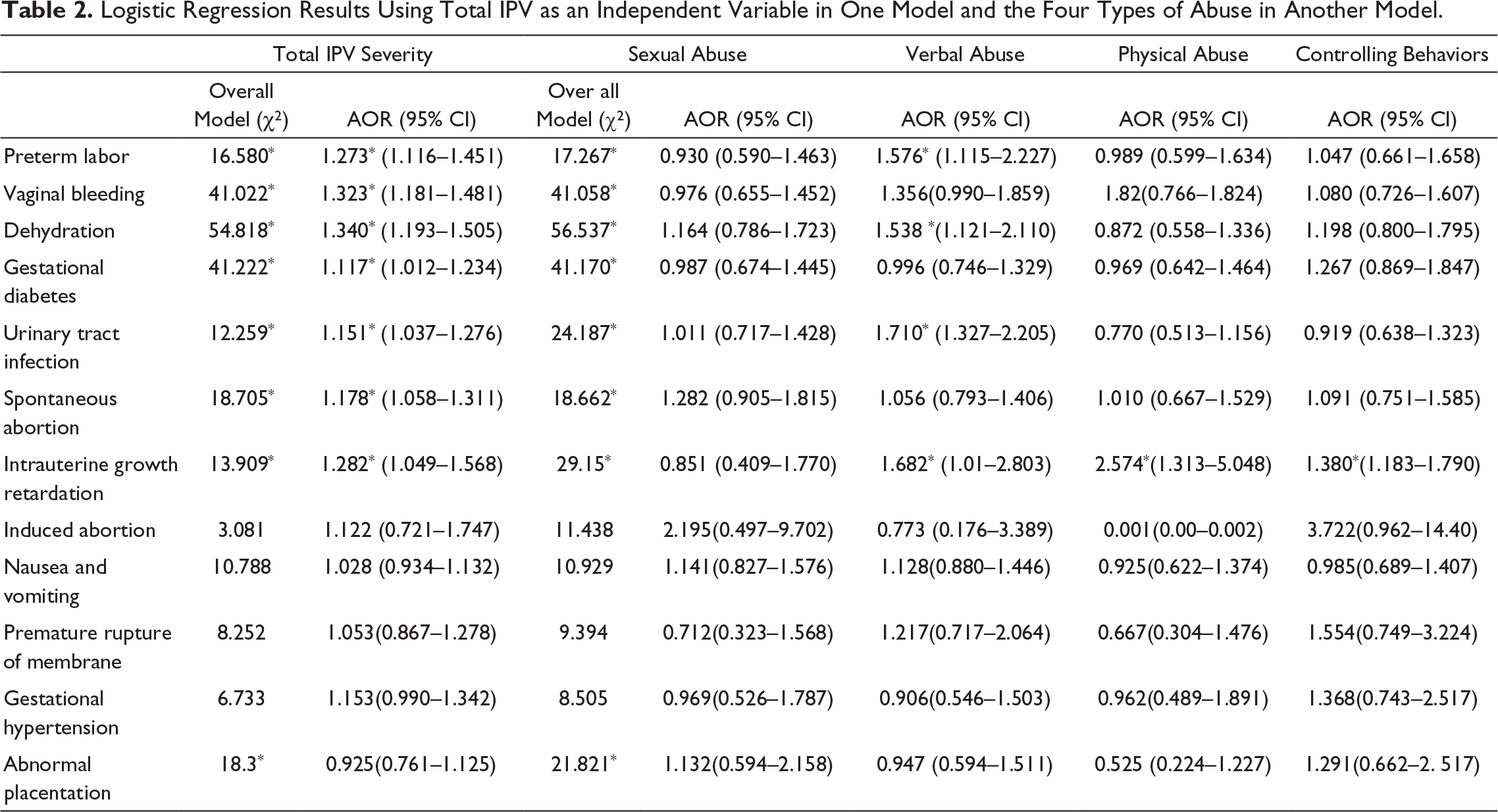
Logistic Regression Results Using Total IPV as an Independent Variable in One Model and the Four Types of Abuse in Another Model.
Prediction of Adverse Pregnancy Outcomes
First, the analyses showed significant and nonsignificant associations among the 12 adverse pregnancy outcomes; even so, all significant associations were weak as Phi coefficients ranged from 0.079 to 0.254. Logistic regression was performed using transformed total IPV severity as an independent variable to determine how well total IPV could predict adverse outcomes, and it was performed again using the transformed abuse types to assess how well they could predict the adverse outcomes. Potential confounding factors (age, education, income, and smoking habit) were included in all logistic regression analyses.
Preterm labor.
Using preterm labor as an outcome variable, the model with IPV severity was statistically significant (χ2 = 16.580; df = 5; p = .005) and correctly classified 92.1% of the cases. IPV severity was significantly associated with the increased likelihood of preterm labor (onset of labor before 37 weeks of gestation) with an adjusted OR of 1.273 (95% CI, 1.116–1.451) as each increase in IPV severity led to a 27.3% increase in the odds of preterm labor. The model of the four abuse types was statistically significant (χ2 = 17.267; df = 8; p = .027). However, only verbal abuse was significantly associated with the increased likelihood of preterm labor with an adjusted OR of 1.576 (95% CI, 1.115–2.227) as each increase in verbal abuse led to a 57.6% increase in the odds of preterm labor.
Vaginal bleeding.
Using vaginal bleeding as an outcome variable, the model of IPV severity was statistically significant (χ2 = 41.022; df = 5; p = .001), and it correctly classified 88.4% of the cases. IPV severity was significantly associated with the increased likelihood of vaginal bleeding with an OR of 1.323 (95% CI, 1.181–1.481) as each increase in IPV severity led to a 32.3% increase in the odds of vaginal bleeding. The model of the four abuse types was statistically significant (χ2 = 41.058; df = 8; p = 0.001); however, abuse type did not independently predict vaginal bleeding in the participants.
Dehydration.
Using dehydration as an outcome variable, the model of IPV severity was statistically significant (χ2 = 54.818; df = 5; p = .001) and correctly classified 90.2% of the cases. IPV severity was significantly associated with the increased likelihood of dehydration with an adjusted OR of 1.340 (95% CI, 1.193–1.505) as each increase in IPV severity led to a 34% increase in the odds of dehydration. The model of the four abuse types was statistically significant (χ2 = 56.537; df = 8; p = .001). However, adjusting for all abuse types, only verbal abuse was significantly associated with the increased likelihood of dehydration with an adjusted OR of 1.538 (95% CI, 1.121–2.110) as each increase in verbal abuse led to a 53.8% increase in the odds of dehydration.
Gestational diabetes.
Using gestational diabetes as an outcome variable, the model of IPV severity was statistically significant (χ2 = 41.222; df = 5; p < .001), and it correctly classified 83.7% of the cases. IPV severity was significantly associated with the increased likelihood of gestational diabetes with an adjusted OR of 1.117 (95% CI, 1.012–1.235) as each increase in IPV severity led to an 11.7% increase in the odds of gestational diabetes. The model of the four abuse types was statistically significant (χ2 = 41.170; df = 8; p < .001); however, no abuse type independently predicted gestational diabetes in the participants.
Urinary tract infection.
Using urinary tract infection as an outcome variable, the model of IPV severity was statistically significant (χ2 = 12.259; df = 5; p = .031), and it correctly classified 82.9% of the cases. IPV severity was significantly associated with the increased likelihood of urinary tract infection with an adjusted OR of 1.151 (95% CI, 1.037–1.276) as each increase in IPV severity led to a 15.1% increase in the odds of urinary tract infection. The model of the four abuse types was statistically significant (χ2 = 24.187; df = 8; p = .002). However, adjusting for all abuse types, only verbal abuse was significantly associated with the increased likelihood of urinary tract infection with an adjusted OR of 1.710 (95% CI, 1.327–2.205) as each increase in verbal abuse led to a 71.0% increase in the odds of urinary tract infection.
Spontaneous abortion.
Using spontaneous abortion as an outcome variable, the model of IPV severity was statistically significant (χ2 = 18.705; df = 5; p = .002), and it correctly classified 84.3% of the cases. IPV severity was significantly associated with the increased likelihood of spontaneous abortion with an adjusted OR of 1.178 (95% CI, 1.058–1.311) as each increase in IPV severity led to a 17.8% increase in the odds of spontaneous abortion. The model of the four abuse types was statistically significant (χ2 = 18.662; df = 8; p = .017), but no abuse type independently predicted spontaneous abortion in the participants.
Intrauterine growth retardation.
Using intrauterine growth retardation as an outcome variable, the model of IPV severity was statistically significant (χ2 = 13.909; df = 5; p = .016), and it correctly classified 96.3% of the cases. IPV severity was significantly associated with the increased likelihood of spontaneous abortion with an adjusted OR of 1.282 (95% CI, 1.049–1.568) as each increase in IPV severity led to a 28.2% increase in the odds of spontaneous abortion. The model of the four abuse types was statistically significant (χ2 = 29.15; df = 8; p < .001). Physical abuse was significantly and independently associated with the increased likelihood of intrauterine growth retardation with an adjusted OR of 2.574 (95% CI, 1.313–5.048) as each increase in physical abuse led to a 157.4% increase in the odds of intrauterine growth retardation. Furthermore, verbal abuse significantly and independently associated with the increased likelihood of intrauterine growth retardation with an OR of 1.682 (95% CI, 1.010–2.803) as each increase in verbal abuse leads to a 68.2% increase in the odds of the occurrence of intrauterine growth retardation. Controlling behaviors were significantly independently associated with the increased likelihood of intrauterine growth retardation with an OR of 1.380 (95% CI, 1.183–1.79) as each increase in controlling behavior led to a 38% increase in the odds of intrauterine growth retardation.
Induced abortion.
Regarding induced abortion, total IPV severity (χ2 = 3.081; df = 5; p = .787) and the model of the four abuse types (χ2 = 11.438; df = 8; p = .178) did not significantly predict it.
Nausea and vomiting.
For nausea and vomiting, total IPV severity (χ2 = 10.788; df = 5; p = .056) and the model of the four abuse types (χ2 = 10.929; df = 8; p = .206) did not significantly predict it.
Premature membrane rupture.
For premature membrane rupture, total IPV severity (χ2 = 8.252; df = 5; p = .143) and the model of the four abuse types (χ2 = 9.394; df = 8; p = .310) did not significantly predict it.
Gestational hypertension.
For gestational hypertension, total IPV severity (χ2 = 6.733; df = 5, p = .241) and the model of the four abuse types (χ2 = 8.505; df = 8; p = .386) did not significantly predict it.
Abnormal placentation.
For abnormal placentation, total IPV severity (χ2 = 18.3; df = 5; p = .003) and the model of the four abuse types (χ2 = 21.821; df = 8; p = .005) were significant, but none of the abuse variables were independently significant.
Discussion
This study showed that 28.9% of the women who participated experienced IPV during the past 12 months. In addition, smoking, personal income, polygamous marriage, the presence of chronic diseases and sexual dysfunction, and number of children were significantly associated with IPV severity. Moreover, a dose–response relationship between IPV and adverse pregnancy outcomes was observed. Each increase in total IPV severity increased the likelihood of preterm labor, vaginal bleeding, dehydration, gestational diabetes, urinary tract infection, spontaneous abortion, and intrauterine growth retardation. Regarding the four abuse types, verbal abuse significantly increased the risk of preterm labor, dehydration, urinary tract infection, and intrauterine growth retardation, whereas physical abuse and controlling behaviors increased the risk of intrauterine growth retardation.
The prevalence of IPV in the current sample (28.9%) is higher than that in other countries that use the same scale (CAS), such as Australia (19.7%; Gartland et al., 2014) and the United Kingdom (6.2% to 19.5%; Estrin et al., 2019), and Nigeria (24.8%; Adebowale & James, 2020). These differences in prevalence are not surprising because the sociocultural context shapes individuals’ norms and attitudes toward IPV (Hardesty & Ogolsky, 2020). This study, with its findings of IPV prevalence, is almost comparable to a study that assessed only the prevalence of physical violence during pregnancy (21%) in Saudi women (Rachana et al., 2002). However, that study has a major drawback, which is the lack of a comprehensive, reliable, and valid measurement tool. It is also possible that Saudi women do not report IPV because they perceive IPV to be a private family matter (Eldoseri et al., 2014), possibly distorting the prevalence estimate. Women who do not disclose IPV might have different circumstances and characteristics. However, structured interviews with trained female data collectors might reduce nondisclosure and improve the accuracy of estimations.
Recognizing the risk factors for IPV in pregnant women is important for healthcare providers in order for them to have an idea about these characteristics and improve identification. The existing literature from different countries highlighted the victim-related characteristics that are associated with IPV during pregnancy (Taillieu & Brownridge, 2010). In our sample, age, working status, and education were not significantly related to IPV during pregnancy. This is inconsistent with studies that consider younger (Groves et al., 2015) or older ages (Kita et al., 2014) as a risk factor for IPV during pregnancy but conforms to women and pregnancy in other contexts (Farrokh-Eslamlou et al., 2014; Islam et al., 2021) as age was not found to be a risk factor. Although studies in Saudi Arabia highlighted age as a risk factor for lifetime IPV (Alhalal, Ta’an, et al., 2019), IPV during pregnancy has different patterns and characteristics. Its insignificant relation to women’s education and occupation is consistent with the findings of other studies (Abebe Abate et al., 2016; Farrokh-Eslamlou et al., 2014).
Personal income, smoking habit, being in a polygamous marriage, the presence of chronic diseases and sexual dysfunction, and number of children were significantly associated with IPV, and this is consistent with the results of other studies to some extent (Taillieu & Brownridge, 2010). Although studies considered income a protective factor (Heaman, 2005), the current study shows that women with higher income have higher IPV severity perhaps because the perpetrators try to be in control of women who are the main financial provider for the household, which does not sit well with their husbands. The association of IPV with smoking has been confirmed in other studies on pregnant women (Cheng et al., 2015), and a meta-analysis found the association between smoking and IPV to be stronger during pregnancy (Crane et al., 2013). The significant differences in IPV severity between smoking and nonsmoking women in this study can be explained by the fact that women cope with IPV-related stress by adopting negative behavioral activities, including smoking. Smoking has increased in Saudi Arabia (Moradi-Lakeh et al., 2015), and 3.9% of women are smokers (Algabbani et al., 2018). The finding that polygamous marriage or having multiple partners increases the risk of higher IPV severity conforms to that of other studies (Alquaiz et al., 2021; Barnawi, 2015; Vung & Krantz, 2009). A polygamous marriage might create a negative dynamic marital relationship, which might result in higher IPV severity. In our current study, there were also differences in IPV severity between women with chronic diseases and sexual dysfunction and those without the said afflictions. Similarly, evidence highlighted that women with disabilities experience higher levels of IPV (Coker et al., 2005; Valentine et al., 2019). However, chronic diseases and sexual dysfunction might occur because of long-term exposure to IPV (Wong & Mellor, 2014). In our study, sexual dysfunction is defined as a problem in orgasm, arousal, and sexual pain. Sexual health continues to be a sensitive indicator of the quality of the relationship between partners, and the negative impact of IPV on women’s sexual function has been repeatedly demonstrated (Hastuti et al., 2011; Jamali & Javadpour, 2016). Nevertheless, in our current study, it was impossible to distinguish whether IPV leads to the occurrence of disabilities or it is the other way around. The number of children is significantly associated with IPV. A study found that pregnant women with three or more children were at a 0.6-fold increased risk of experiencing IPV (Peedicayil et al., 2004) and that the number of children is the only significant effective factor on the prevalence of IPV during pregnancy in China (Wang et al., 2017). This could be explained by the stress resulting from the responsibility of providing care to a greater number of children and the expected child. A significant difference in IPV severity between women who use contraception and those who do not was observed. This can be explained by two scenarios: either women who insist on using contraception experience more IPV or, as IPV increases, women seek out contraception to avoid unwanted pregnancies. However, this finding contradicts previous studies’ finding that women who avoid contraception are at increased risk of IPV (Maxwell et al., 2015) because IPV severity may decrease contraceptive efficacy. Differences in sociocultural values and varying access to contraception between different populations might account for this inconsistency.
IPV represents a unique risk to adverse pregnancy outcomes. It became evident in this study that IPV increases the likelihood of nine pregnancy-related complications with ORs ranging from 1.117 to 2.574. This result is similar to other studies that found that in the IPV context, the odds of the occurrence of pregnancy-related outcomes ranged between 1.30 and 1.62 (Sharps et al., 2007). Our current study revealed that after adjusting for confounding factors, in each one-unit increase in total IPV severity, the likelihood of preterm labor, vaginal bleeding, dehydration, gestational diabetes, urinary tract infection, spontaneous abortion, and intrauterine growth retardation increases by 1.273, 1.329, 1.323, 1.340, 1.117, 1.151, 1.178, and 1.282, respectively. Adjusting for confounding factors and the types of abuse, a one-unit increase in verbal abuse increases the likelihood of preterm labor, dehydration, urinary tract infection, and intrauterine growth retardation by 1.576, 1.538, 1.710, and 1.682, respectively. A one-unit increase in physical abuse increases the likelihood of intrauterine growth retardation by 2.574. Furthermore, a one-unit increase in controlling behaviors increases the likelihood of intrauterine growth retardation by 1.380. These eight pregnancy outcomes have also been documented in other studies with different sociocultural contexts (Alhusen et al., 2015; Martin-De-las-heras et al., 2019). In a recent systematic review, IPV was associated with abortion, preterm labor, low birth weight, premature rupture of the membranes, and perinatal death (Pastor-Moreno et al., 2020). However, studies in Saudi Arabia focusing only on physical abuse documented menorrhagia, low weight gain during pregnancy, preterm labor, premature birth, abortions, abruptio placentae, low birth weight, postpartum hemorrhage, postpartum depression, and delivery by cesarean section as pregnancy-related outcomes (AboulAzm et al., 2009; Fageeh, 2014; Rachana et al., 2002). Thus, our current study adds to the current body of literature by revealing that the risk of experiencing adverse pregnancy outcomes increased because of IPV, controlling for the participants’ demographic characteristics. In addition, our current study showed that verbal abuse consistently significantly increases the risk of adverse pregnancy outcomes. This conforms to a study that showed that psychological IPV is the only risk factor of urinary tract infection and vaginal infections in pregnant women (Martin-De-las-heras et al., 2019). This highlights the importance of the psychological status of women. Thus, physical abuse should not only be the main focus. Verbal abuse or psychological abuse in pregnancy is usually not well tested in existing studies (Coker et al., 2002; Hill et al., 2016).
Maternal psychological stress during pregnancy can lead to preterm birth (Wadhwa et al., 2011). It stimulates a neuroendocrine response, which releases catecholamines, cortisol, and β-endorphin. Elevated cortisol in chronically stressed pregnant women is associated with an increase in placental corticotropin-releasing hormone (Hill et al., 2016; Wadhwa et al., 2011). In addition, psychological stress during pregnancy might lead to immune system dysregulation because of high levels of inflammatory cytokines and low levels of the anti-inflammatory markers (Hill et al., 2016; Wadhwa et al., 2011), leading to increased risk of infection (Culhane et al., 2001), such as urinary tract infections, and contributing to placental insufficiency and preterm birth (Nath et al., 2007). Stress is linked to reduced uterine and umbilical blood flow leading to fetal hypoxia (Wadhwa et al., 2011). Fetal hypoxia might cause intrauterine growth retardation or preterm birth (Hill et al., 2016).
Given all these facts, the study findings have implications. It becomes essential to assess all women for IPV and recognize it as a modifiable risk factor in providing care. One of the challenges in addressing IPV is the sensitivity of the topic from a sociocultural perspective and inadequate preparation of the healthcare provider. The study findings revealed the importance of clinical implications. A routine assessment of pregnant women for IPV in antenatal clinics is recommended in order to identify women at risk of adverse pregnancy outcomes. It can prepare the ground for using such valuable information on IPV to predict negative health issues, allowing for early detection and on-time intervention. Healthcare professionals should consider IPV an underlying factor increasing women’s risk of adverse health conditions. Healthcare providers have to be trained and empowered to address IPV as a health issue. IPV as a health issue has to be integrated into the curricula of healthcare professionals in order to prepare them in identifying and managing the issue. To tackle IPV, a multi-sectoral response is necessary, emphasizing the integration of IPV prevention programs in healthcare systems, development of clear and practical health policies and protocols, and establishment of good referral systems. Developing interventions that target healthy relationships, specifically during pregnancy, is necessary. A shift in public attitude toward IPV, from its being a private family matter to its being a health issue, is significant to encourage women to cultivate help-seeking behaviors. Further research is needed in the Arab context to focus on neonatal health outcomes and women’s mental health outcomes during the first year of postpartum. Studies exploring the biological mechanisms underlining the effect of IPV on pregnancy-related outcomes are required.
Saudi Arabia has universal health coverage, and therefore, recruiting women from public hospitals might increase the generalizability of the current findings. Also, the high response rate (94.9%) in this study might enhance the generalizability of the findings to a larger population. The selected hospital is a referral hospital in which people are referred from different parts in Saudi Arabia. The sample included women of different socioeconomic statuses (e.g., housewives, laborers, and other disparate women with various educational levels), and in addition to Saudi women, the current sample also included non-Saudi women who spoke Arabic. Therefore, women from different Arab countries currently residing constituted 6.6% of the sample. Therefore, these findings can be applied to the situations of other pregnant Arab women in different parts of the world as Arab cultures are linguistically, religiously, and culturally similar (Dhaouadi, 2013).
Nevertheless, the findings of our current study should be interpreted while recognizing several important limitations. The use of a convenience sample may have led to a biased sample. The use of a cross-sectional design limited our ability to identify a causal relationship between IPV severity and adverse pregnancy health outcomes. To protect women’s safety, women who were accompanied by their husbands were excluded from the study as women are usually afraid of possible retaliation, confinement, and retribution by their husbands for speaking out (Vranda et al., 2018). Excluding these women may have distorted our results as this group might have displayed different characteristics when compared with what women who were unaccompanied did. However, very few women were excluded for this reason. Although the data on the adverse pregnancy outcomes were collected from the participants’ medical records, IPV data were collected using a self-report scale, which may have led to recall bias and limited the accuracy of the women’s reporting, given the stigmatic nature of the issue. Another limitation of the current study is that the inclusion of only women in the first six weeks postpartum instead of including those in the first year of postpartum might have queered the pitch in identifying the effect of IPV on postpartum women’s health.
Conclusion
This study revealed that 28.9% of pregnant and post-partum women in Saudi Arabia experienced IPV. Smoking, personal income, polygamous marriage, the presence of chronic diseases and sexual dysfunction, and number of children were significantly associated with IPV severity. Moreover, a dose–response relationship between IPV and adverse pregnancy outcomes was demonstrated. The greater the total IPV severity the more the likelihood of adverse outcomes. This largely hidden issue among pregnant women needs to be addressed in the healthcare system. Healthcare providers must routinely assess and identify IPV during antenatal care visits as well as consider pregnancy a “window of opportunity” to address IPV.
Footnotes
Acknowledgments
The authors acknowledge the support from Samiyah Alanazi, Lamees Jamour, Munirah Alabdulwahab, and Fatima Mohamed.
Authors' Note
Dr Khalid Akkour is now affiliated with King Saud University, Riyadh, Saudi Arabia.
Declaration of Conflicting Interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.