
Abstract
South Africa has some of the highest rates of intimate partner and sexual violence globally, with prevalence ranging from 10% to 21% among adolescent girls and young women (AGYW). Yet, few studies characterize the relationship between violence and resilience. Identifying factors associated with resilience following exposure to violence can guide the development of strength-based interventions that change modifiable protective factors to bolster resilience. Data were derived from a cross-sectional survey of AGYW aged 15 to 24 years in South Africa that took place from 2017 to 2018. This survey was part of a national evaluation of a South African combination HIV intervention for AGYW funded by the Global Fund to Fight AIDS, TB, and Malaria. A sample of 4,399 observations was achieved through a systematic random sampling frame of 35% of households in districts where AGYW were at highest risk for HIV, and where the intervention was implemented. Resilience was assessed using the Connor-Davidson Resilience Scale. Intimate partner and sexual violence were assessed using: (a) an adapted version of a questionnaire from the World Health Organization’s 2005 multicountry study on domestic violence against women, and (b) questions on lifetime experience of forced sex/rape. Nearly a third of AGYW (29.6%) reported intimate partner emotional and/or physical and/or sexual violence in the past year. Nearly a quarter of AGYW (23.74%) reported emotional violence, 17.48% reported physical violence, and 6.37% reported sexual violence from intimate partners. Nearly 8% (7.72%) reported forced sex/rape from intimate partners and/or nonpartners. More equitable gender norms, higher social support, and hazardous drinking were positively associated with higher resilience among those who experienced physical or sexual violence. This study addresses a gap in the resilience and violence literature. Future research should focus on the development of resilience-promoting interventions for individuals who have experienced violence.
Globally, 30% of girls and women aged 15 years and older have experienced lifetime physical and/or sexual intimate partner violence (IPV) (Devries et al., 2013). There is wide variation across the world, with sub-Saharan Africa having some of the highest rates of interpersonal violence globally (Abrahams et al., 2014). In South Africa, 21.3% women have experienced lifetime sexual and physical violence (National Department of Health, 2019). Although, South African data on adolescent girls is less available than adult data, several epidemiological studies indicate concerning rates. For example, one study in Johannesburg found that 18.3% of female adolescents (15 to 19 years of age) reported experiencing sexual violence from an intimate partner in the past year (Decker et al., 2014). Another study in Cape Town identified a 10% prevalence of sexual violence (defined as ‘forced’ sex by/of a partner or non-partner) among eighth graders, typically corresponding to 13 years of age (Russell et al., 2014). Public health consequences of IPV are severe, with a range of consequences including physical illness, poor mental health, and femicide (Campbell, 2002; Ellsberg et al., 2008). In a nationally representative study of femicide that gathered data on mortality from a proportionate random sample of 25 mortuaries, the mortality rate from IPV was 8.8 per 100,000 women (Abrahams et al., 2009). Combined, these data on violence experienced by women and girls indicates that the epidemic of violence is a serious public health concern globally, and especially for South Africa.
Resilience, broadly defined, is the dynamic process that enhances the capacity of individuals to thrive after exposure to adversity (Masten, 2014; Ungar, 2012). Increasingly, work on resilience recognizes the importance of examining how different aspects of an individual’s ecosystem can contribute factors that cultivate resilience, or to processes that cultivate resilience (Ungar, 2011). Understanding how resilience relates to violence, and specifically how to cultivate resilience after exposure to violence, can guide the direction of future interventions to more effectively attenuate the long-term adverse effects of violence upon the wellbeing of girls and young women, and direct the foci of clinical responses to successfully support girls and young women in achieving optimal outcomes. A significant gap in the scientific literature exists on what factors might promote resilience among girls and women who have experienced interpersonal violence. This includes a paucity of understanding from an ecosystem perspective regarding what factors and processes at the individual, interpersonal, and community levels, might facilitate resilience after exposure to violence. For example, in a recent review of quantitative and qualitative studies of interventions with resilience-related outcomes among adults who experienced IPV and childhood violence, only 20 studies were identified. Authors concluded the evidence was too disparate and sparse, and measures of resilience inconsistent, to determine how to improve resilience. In fact, when authors used the Quality Assessment Tool for Quantitative Studies for assessing the quality of quantitative studies (with evaluation of elements such as selection bias, study design, confounders, blinding, data collection methods, withdrawals and dropouts, intervention integrity, and analyses), only three of the quantitative studies in the review had rigorous experiential design and differential ways of defining resilience. This number was too small to draw conclusions across the intervention evidence base on how to promote resilience (Moeller-Saxone et al., 2015). Only one study (Apondi et al., 2007) had a focus on an HIV affected population-in this case, individuals receiving home-based antiretroviral treatment-and included all genders and took place in Uganda. Although not focused on interventions to address resilience after exposure to violence, a related systematic review examined resilience-promoting interventions targeting reduction of sexual risk of girls and young women, offering additional insight into the state of the evidence (LoVette et al., 2019). This review of the global literature identified 25 unique interventions with only 15 of the 25 interventions reported improving relevant outcomes, and only 6 interventions tested via a randomized controlled trial design. Thus, similar to the prior review, the number of interventions in the space of resilience and sexual health for girls and young women shows that the evidence base around resilience for this population needs further development (LoVette et al., 2019). To contribute to the evidence base, this article examines two questions: (a) Does resilience differ among South African adolescent girls and young women who have experienced intimate partner and sexual violence versus those who have not? (b) What factors are associated with resilience among adolescent girls and young women who have experienced intimate partner and sexual violence? We examine these factors using an ecological model, given that resilience theory shows that factors at multiple levels of an individual’s ecosystem-individual, interpersonal/relationship, and community levels-can impact resilient outcomes (Ungar, 2011). Findings can inform the creation of resilience-focused intervention programming targeting modifiable factors that can support resilience among populations exposed to IPV and sexual violence.
Methods
Participants
This article reports on data from a cross-sectional household survey of 4,399 adolescent girls and young women (AGYW) aged 15 to 24 years that occurred from 2017 to 2018. The data were generated from the first of the two serial surveys used to evaluate a South African combination intervention designed to prevent HIV among AGYW and was delivered from 2016 to 2019. The roll-out of the combination intervention commenced first and was followed by the first of the two serial surveys used in the evaluation. The combination intervention was funded by the Global Fund to Fight AIDS, TB, and Malaria and targeted 10 districts in South Africa where AGYW were at highest risk for HIV. The intervention was designed to do the following: (a) decrease HIV incidence; (b) decrease teenage pregnancy; (c) increase retention in school; (d) decrease gender-based violence; and (e) increase economic opportunities. The intervention package included the following behavioral, biomedical, and structural HIV prevention components: (a) access to comprehensive HIV, TB, and sexual and reproductive health services and commodities; (b) rights-based sexual and reproductive health education; (c) support to keep adolescent girls in school including homework help; (d) therapeutic services for abused children; (e) financial literacy and career development; (f) vocational programs to promote economic empowerment; and (g) interventions to maximize social support and social capital. In addition, there was a (h) conditional cash incentive program that was rolled out in two districts.
Participants were identified using a stratified sampling design. In the sampling frame, intervention districts were considered as the primary strata. Sample size in each district was designed to be proportional to the AGYW in the sub-district areas or wards selected for intervention. Intervention areas mapped onto the available 2011 census small areas layer (SAL) sampling areas. These SAL sampling frames were further adjusted to the latest Geo Terra Image counts, other district council estimates, and StatsSA’s most current midyear estimates of population numbers per province, accounting for province boundaries, race, age groups, and gender. There were 2,470 SALs targeted for the intervention, with 300,000 households in which 120,000 AGYW were residing, based on the 2011 census. In the intervention areas for each district, the study selected a simple random sample of SALs. Then, a systematic random sample of 35% of the available households within each SAL was selected to generate the sample of AGYW invited to participate with all AGYW aged 15 to 24 years in sampled households receiving invitations to participate. The field team identified these preselected households using aerial maps, and determined the geographical coordinates using Geographical Positioning System. Vacant households and households where the household head declined to complete a household listing form to determine whether there were eligible AGYW resulted in the team visiting the household on the left. A choice to visit households immediately to the left of vacant households (the closest plot to the randomly chosen starting point), or where household heads declined to complete a household listing form, was a procedure put in place to limit selection bias in the sampling process, and to ensure we received a sample response at the random starting point without additional sampling.
The survey was completed in the following districts: City of Cape Town (Western Cape), Ehlanzeni (Mpumalanga), O.R. Tambo (Eastern Cape), Tshwane (Gauteng), King Cetshwayo (KwaZulu-Natal), and Zululand (KwaZulu-Natal). The overall sample realization was 60.6% in the 6 completed districts. The weighted sample size, according to sample weights based on the systematic random sample of households within each SAL, was 7,237 for this household-based sample of AGYW aged 15 to 24 years across 6 districts where AGYW were at highest HIV risk.
Participants
Adolescent girls and young women (AGYW) were eligible for inclusion based on the following criteria: (a) AGYW residing in household aged 15 to 24 years; (b) AGYW had to give informed consent, with those who were under 18 also needing parent, guardian, caregiver or household representative consent for participation; and (c) AGYW were willing to participate in the study, undergo all study procedures including providing blood samples. AGYW were excluded if they: (a) had cognitive or mental challenges (based on the assessment of the participant’s ability to comprehend the study information provided); (b) were unable to hear or speak; (c) were unable to speak English, IsiZulu, isiXhosa, Northern Sotho, Sotho, Tswana, Tsonga, Swazi, Sepedi, Afrikaans; and (d) were not available for participation between 8
Procedures
Each potentially eligible study participant was informed about the study and completed the consent form in their preferred language prior to enrolment. For potential participants under 18 years of age, parent/guardian/foster parent/caregiver consent was obtained before getting assent from the AGYW. Informed consent procedures were conducted in a private space, inside or outside the household, depending on the potential participant’s choice. The fieldworker sat with the potential participant and read the forms to her word-for-word and answered any questions for clarification from the participant.
This study used electronic questionnaires developed using the Mobenzi Researcher data collection software suite (
Measures
Resilience
To evaluate resilience, a 10-item version of the Connor-Davidson Resilience Scale (CD-RISC) was used (Connor & Davidson, 2003). The CD-RISC has previously demonstrated strong psychometric properties among South African adolescents (Jorgensen & Seedat, 2008). Psychological resilience, as measured by the CD-RISC 10, is a continuous measure and can range from 0 to 40 points, with higher scores indicating greater psychological resilience (Cronbach’s alpha from this study: 0.83).
Intimate Partner and Sexual Violence
An adapted version of a questionnaire from the World Health Organization’s 2005 multicountry study on women’s health and domestic violence against women was used (Garcia-Moreno et al., 2006). Ten items were used to evaluate emotional, physical, and sexual violence from an intimate partner in the year prior to the survey. An example of an emotional violence question includes, “In the past year, has a boyfriend or partner made fun of or humiliated you in font of other people? How often has this happened?”, with other forms of emotional violence including threats and intimidation. An example of a physical violence question includes, “In the past year, has a boyfriend or partner pushed or shoved you? How often has this happened?”, with other forms of physical violence including slapping, throwing objects, hitting, kicking, dragging, beating, choking, burning, and use of gun, knife or weapon. An example of a sexual violence question includes, “In the past year, have you had sex with a boyfriend or partner when you didn’t want to because he forced or threatened or pressured you or because you were unable to stop him?”, with other examples of sexual violence including sex because a boyfriend or partner threatened to go out with or have sex with another individual. Answer responses to emotional, physical, and sexual violence questions included: “never, once, more than once, I haven’t had a boyfriend or partner in the last 12 months, I prefer not to say.” In addition, questions about lifetime experience of forced sex/rape by any individual including intimate partners or nonpartners were asked.
Individual Factors
This study examined three measures at the individual level: gender norms, alcohol use, and drug use. Gender norms were assessed related to sexual relationships and gender power with 22 items adapted from the Gender Equitable Men’s Scale, a continuous measure (Cronbach’s alpha from this study: 0.71) (Pulerwitz & Barker, 2008). A participant’s score could range from 22 to 66, with higher scores representing norms reflecting greater gender equity. To measure substance use, two measures were used. The first used was the Alcohol Use Disorders Identification Test (AUDIT-C), to capture alcohol use (Cronbach’s Alpha from this study: 0.79). AUDIT-C is comparable to the full AUDIT and has been used among South African populations (Morojele et al., 2017). A participant’s AUDIT-C score can range from 0-12. Informed by the recommendation emanating from the South African study (Morojele et al., 2017), we used a cut-off score of greater than or equal to two to indicate hazardous drinking. Second, an eleven-item Drug Use Disorders Identification Test (DUDIT), was used to capture drug use (Cronbach’s Alpha: 0.87). A participant’s DUDIT score can range from 0 to 44. A cut-off score of greater than or equal to two was used to indicate a drug-use disorder, based on a recommendation emanating from a South African study (Kader et al., 2012).
Relational Factors
For relational factors, this research looked at social support. Social support was measured with the Multidimensional Scale of Perceived Social Support (MSPSS). The MSPSS is a 12-item scale designed to measure perceived social support from three sources: family, peers/friends, and a special person/significant other (Zimet et al., 1988). The scale has been previously validated as measuring social support across three sources among young people in various settings (Bruwer et al., 2008; Canty-Mitchell & Zimet, 2000). AGYW were asked to respond to 12 statements in total, four statements for each category of perceived support. Each statement had an option of responses ranging from very strongly agree to very strongly disagree, scored 1 to 7. The mean scores for the subscales of the total scales may be interpreted as follows: a mean score ranging from 1 to 2.9 could be considered low support; a score of 3 to 5 could be considered moderate support, and a score of 5.1 to 7 could be considered high support (Cronbach’s alpha from this study: overall, 0.91; family scale, 0.85; peer scale, 0.88; special person scale, 0.83).
Community Factors
For community-level factors, structured social capital (SSC) was examined using the social cohesion scale of the short version of the Adapted Social Capital Assessment Tool (SASCAT) (De Silva et al., 2006). The SSC items in the tool examine community group membership and collective action. Scoring of the SSC component on the SASCAT, a continuous measure, was done by adding scores from items assigned to group membership (out of 8), support from group (out of 6), and support from individuals (out of 8). Higher scores denote higher amount of SSC (Cronbach’s alpha from this study: 0.70).
Demographic Factors
Questions regarding age, relative socio-economic status, and receipt of social grants were included.
Statistical Analysis
For the economic status variable, a demographic factor that was examined, a relative socio-economic status variable was created through a cluster analysis (K-modes algorithm). This analysis focused on classifying participants into two socio-economic groups-lower relative socio-economic status versus higher relative socio-economic status-based on their responses to the following variables: how often participants were away from home in the last 12 months, availability of flush toilet, potable water, electricity, car, computer, internet, refrigerator, stove, having money, saving money, owing money to others, and hunger (Rutstein & Johnson, 2004).
Independent samples t-tests for equality of means were conducted to assess associations between intimate partner and sexual violence, and resilience. To proceed with analysis based on the concept of resilience as thriving in the face of vulnerability or risk, AGYW who experienced intimate partner and sexual violence were then dichotomized into high and low resilience groups based on median-spilt CD-RISC score. The median-split resilience score for this sample was 25 (out of a possible total score of 40, with higher scores reflecting higher resilience). This resulted in two categories of individuals: those who reported high resilience (n weighted = 3,830, n unweighted = 2,329) and those who reported low resilience (n weighted = 3,830, n unweighted = 2,329). We then examined two categories for comparing factors associated with resilience among participants who experienced intimate partner physical and sexual violence: those who experienced intimate partner physical and sexual violence with high resilience (n weighted = 845, n unweighted = 503); and those who experienced intimate partner physical and sexual violence with low resilience (n weighted = 854; n unweighted = 513).
Then, a generalized linear model measured associations between individual-, relational-, and community-level variables and the outcome of high resilience (assessed continuously based on the CD-RISC scale) among those that experienced some type of physical or sexual violence. This study built a linear model, informed by other papers that used an ecological approach to model or identify individual, relational, and community factors associated with resilience among women exposed to violence (Anderson et al., 2012; Greenman & Matsuda, 2016; Howell et al., 2018; Izugbara et al., 2020). Preliminary analyses with a three-level hierarchical linear model revealed a lack of significance of relational- and community-level group effects, including negligible random-effects variance estimates. Thus, a simple linear regression was utilized. Multicollinearity between explanatory variables was assessed prior to interpretation of results using the variance inflation factor (VIF), and all values fell within an acceptable range (VIF < 2). A t-test was used to assess variable associations.
All analyses incorporated sampling weights to account for complex survey design and the unequal probability of selection for each survey participant. The prevalence and proportions reported in the paper reflect these weights. Standard errors for cluster sampling were also adjusted for using the svy package in Stata. All analyses were conducted using Stata.
Results
Participant Demographics
From a weighted sample size of 7,237, N = 4,399 unweighted participants were (almost all) South African citizens (98.79%), with most participants self-identified as “African” (89.81%). More than half of the participants reported that they were in school at the time they were surveyed (56.17%), with 81.72% of the 15-to-19-year age group reporting they were at school, compared to 22.76% of those in the 20-to-24-year age group. Most participants (79.66%) were in the low socioeconomic (relatively poorer) group. Almost a fifth (18.34%) of participants reported that someone in their household had gone a day and night without eating because of lack of food in the prior month. Nearly half of participants (42.24%) reported that the members of their household depended on social grants, which cover a variety of government funded welfare grants based on economic need, child and older adult care, disabilities, and more. Over two-thirds (67.31%) reported having a partner in the last year.
Resilience and Prevalence of Intimate Partner Violence and Sexual Violence
Intimate Partner Violence Perpetrated by a Boyfriend or Partner During the Past Year Among Adolescent Girls and Young Women, and Interpersonal Forced Sex, in Six Districts in South Africa, 2017-2018
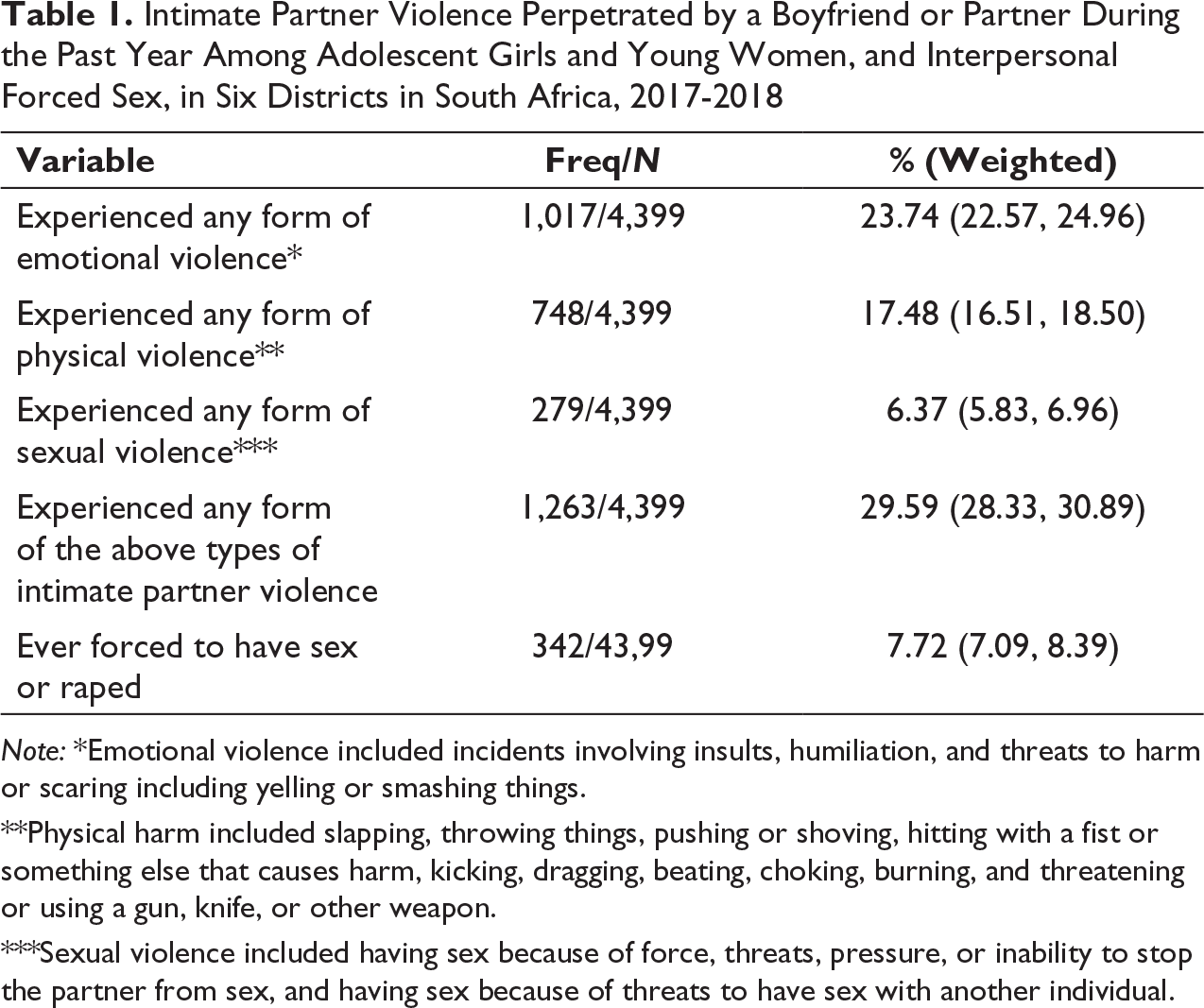
Note: *Emotional violence included incidents involving insults, humiliation, and threats to harm or scaring including yelling or smashing things.
**Physical harm included slapping, throwing things, pushing or shoving, hitting with a fist or something else that causes harm, kicking, dragging, beating, choking, burning, and threatening or using a gun, knife, or other weapon.
***Sexual violence included having sex because of force, threats, pressure, or inability to stop the partner from sex, and having sex because of threats to have sex with another individual.
Resilience Higher Among Those Who Have Not Experienced Intimate Partner Violence and Sexual Violence
Bivariate Associations Between Resilience and Intimate Partner Violence Perpetrated by a Boyfriend or Partner During the Past Year Among Adolescent Girls and Young Women, and Interpersonal Forced Sex, in Six Districts in South Africa, 2017-2018
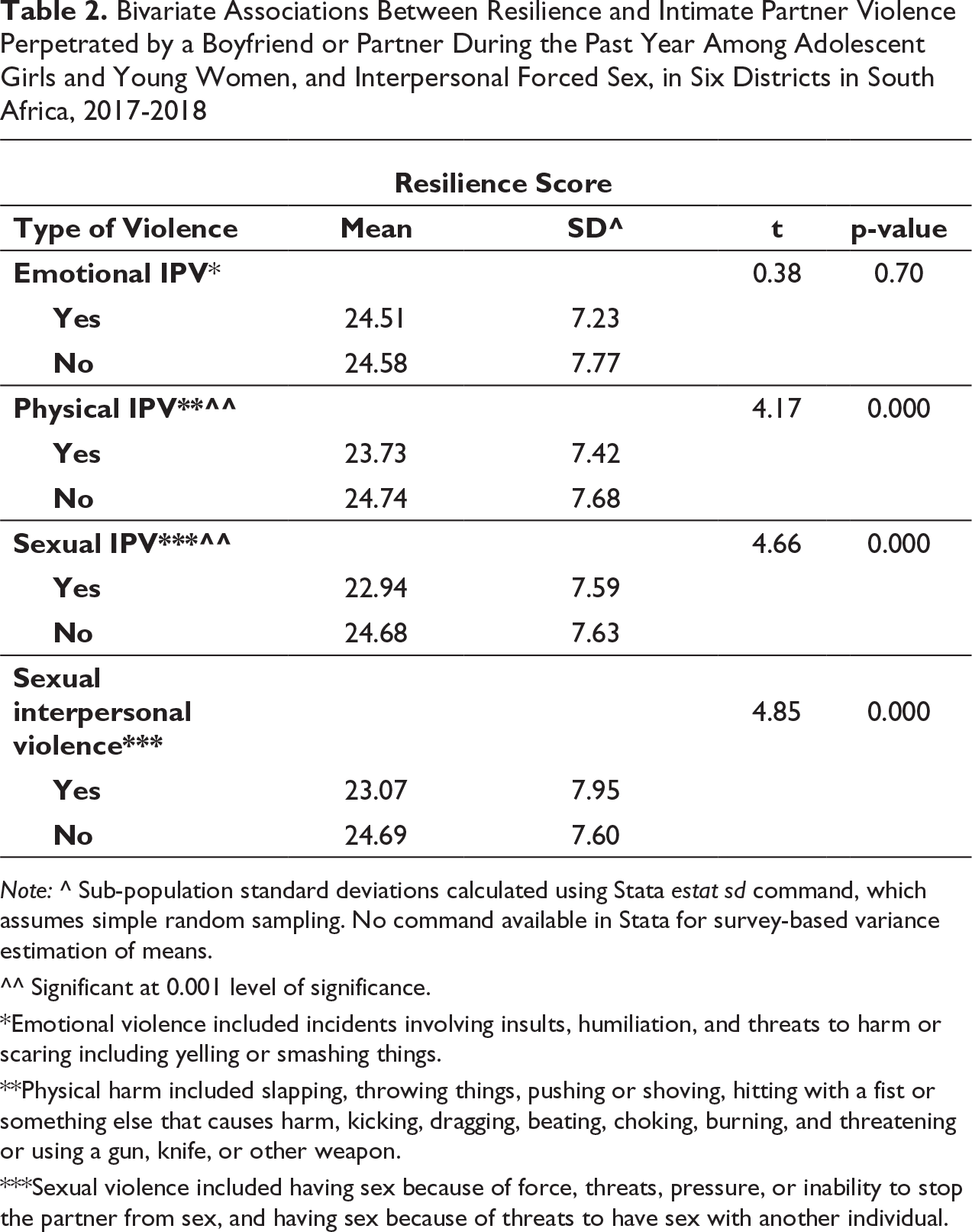
Note: ^ Sub-population standard deviations calculated using Stata estat sd command, which assumes simple random sampling. No command available in Stata for survey-based variance estimation of means.
^^ Significant at 0.001 level of significance.
*Emotional violence included incidents involving insults, humiliation, and threats to harm or scaring including yelling or smashing things.
**Physical harm included slapping, throwing things, pushing or shoving, hitting with a fist or something else that causes harm, kicking, dragging, beating, choking, burning, and threatening or using a gun, knife, or other weapon.
***Sexual violence included having sex because of force, threats, pressure, or inability to stop the partner from sex, and having sex because of threats to have sex with another individual.
Summary of Linear Regression Analysis Predicting Resilience Among AGYW Who Experienced Physical/Sexual IPV and/or Sexual Interpersonal Violence, in 6 Districts in South Africa, 2017-2018
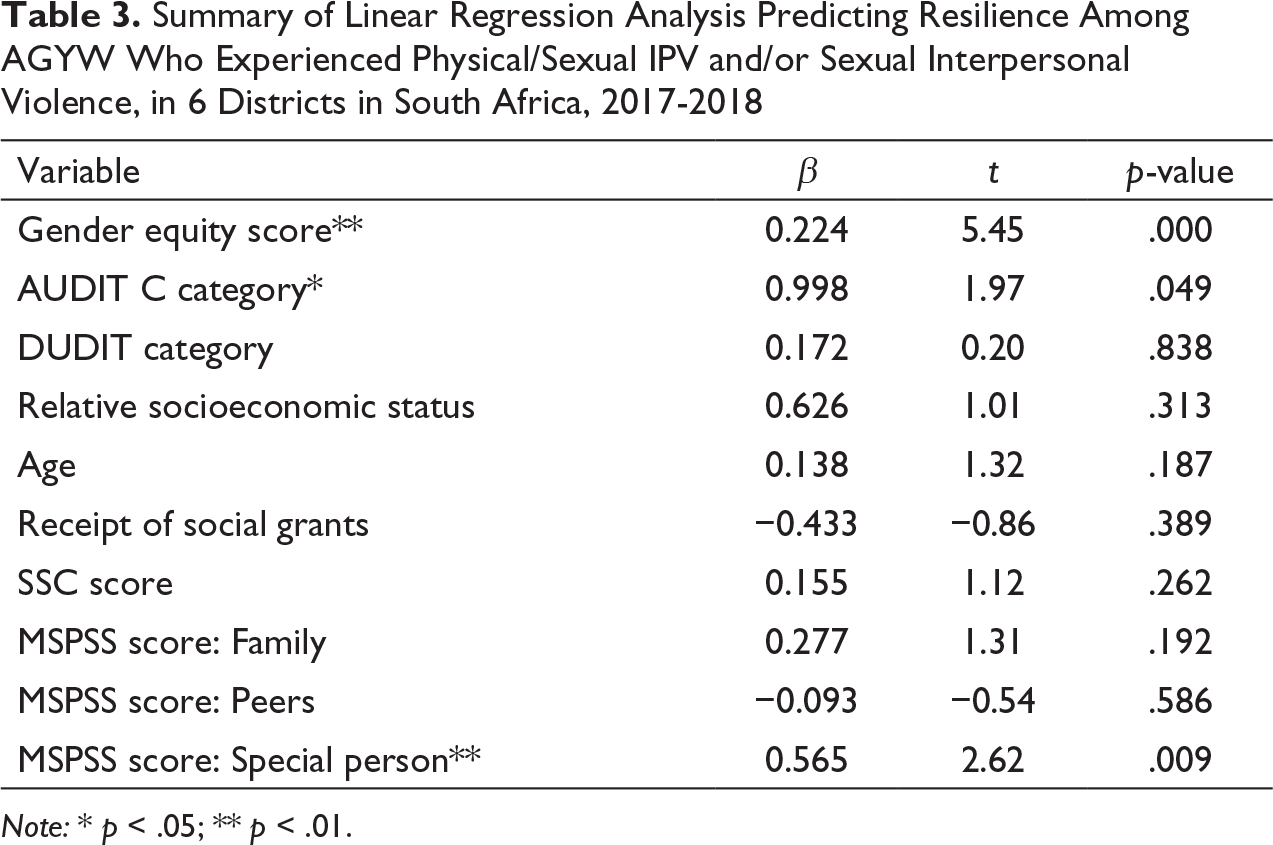
Note: * p < .05; ** p < .01.
Predictors of High Resilience Among AGYW Who Experienced Physical and/or Sexual Intimate Partner Violence and/or Sexual Interpersonal Violence
The linear model was run on a sub-sample of AGYW who experienced physical/sexual IPV and/or sexual violence (n unweighted = 1,016, n weighted = 1,700) (see Table 3). More equitable gender norms, higher social support from a special person, and hazardous drinking were all positively associated with higher resilience among those who experienced physical or sexual violence. A one-point increase on the Gender Equitable Men’s Scale was associated with a 0.22 point increase in an AGYW’s resilience score (p < .001). A one-point increase on the MSPSS special person scale was associated with a 0.57 point increase in an AGYW’s resilience score (p = .009). On average, those who had an AUDIT-C score indicating hazardous drinking reported a resilience score that is one point higher than those without hazardous drinking (p = .049). An AGYW’s age, drug use, relative socioeconomic status, and receiving social grants were not associated with resilience. Furthermore, SSC and social support from peers and family were not associated with increased resilience.
Discussion
This study addresses a gap in the literature around the role of resilience and intimate partner and sexual violence among a population facing some of the highest rates of gender-based violence in the world. This study demonstrated resilience scores were lower among AGYW who experienced physical violence from intimate partners, and sexual violence from intimate partners as well as nonpartners. Among AGYW who experienced intimate partner and sexual violence, findings also showed more equitable gender norms, higher social support from a special person, and hazardous drinking were associated with increases in resilience. These findings provide important implications for future programming and policy to improve the health and well-being of AGYW in South Africa.
The findings from this study offer relevant information to those addressing high rates of IPV and sexual violence experienced by South African AGYW. Results show positive associations between resilience and equitable gender norms among AGYW who experienced both physical and sexual violence. This indicates that content around gender norms should be more clearly incorporated into programming and policies focused on supporting AGYW who have experienced IPV and sexual violence, as focusing on more equitable gender norms may promote resilience. Resilience-based interventions could build upon programs created to address violence towards AGYW, which have consistently included dialogue around gender norms, and have also sought to intervene beyond the individual level, by addressing additional social and structural determinants of health such as economic empowerment (Amin & Chandra-Mouli, 2014; Gupta et al., 2013). Including community- and structural-level components in future programming to address harmful gender norms is critical in creating change as gender norms are reinforced socially and as well as through systems and policies (Jewkes et al., 2015).
The findings around gender norms also demonstrate the need to include boys and young men in conversations around equitable gender norms, including conversations around masculinity. One literature review examined 58 studies of programming that included boys and men to promote sexual and reproductive health, and found that programming using a gender-transformative approach and promoting gender-equitable relationships was more effective in creating behavior change than programming with a narrow and individual focus (Barker et al., 2010). In South Africa, reducing violence by changing gender norms may also help to reduce HIV risk among AGYW. Two South African studies implementing community and structural interventions to reduce IPV and HIV risk showed potential effectiveness for changing gender norms and reducing IPV, but results for HIV risk were mixed, suggesting more long-term programming is needed to change other risk behaviors (Pettifor et al., 2018; Pronyk et al., 2006). Additionally, the finding around special support of a special person, or significant other, and resilience offers an opportunity for researchers and professionals to consider dyadic or couples’ intervention within this context, which has been identified by other South African studies as supporting resilience among women who have experienced violence (Machisa et al., 2018).
Interestingly, hazardous drinking among AGYW who experienced intimate partner and sexual violence also appeared to be associated with higher resilience. This finding may point to alcohol as a coping mechanism, albeit a negative coping strategy, occurring alongside resilience processes. One study among South African women highlighted narratives of drinking to cope with stressors, and also drew attention to the ways drinking served as a way to engage socially and temporarily empower women in a context of imbalanced power dynamics (Choi et al., 2014). Future research examining resilience and trauma related to IPV and sexual violence needs to consider measuring concepts and outcomes longitudinally to increase our understanding of how resilience and alcohol use change over time. This unexpected finding is especially important considering this population’s overall exposure to traumatic events. Previous research examining associations between traumatic experiences and hazardous drinking among South African women found traumatic experiences, including physical and sexual abuse, were associated with hazardous drinking and that post-traumatic stress disorder mediated a significant portion of the relationship between number of traumatic experiences and drinking behavior (Watt et al., 2012). In addition to conducting longitudinal research, future interventions promoting resilience among AGYW experiencing violence should integrate programming and offer resources to address substance use and mental health. The findings around alcohol and resilience also highlight the potential costs of resilience, and possible consequences of attempting to overcome persistent adversity among a population facing some of the highest rates of gender-based violence in the world. Studies based in the US have described the phenomenon of being psychologically resilient, or strong, but physically vulnerable (Erving et al., 2020). Additional resilience research should seek to examine this phenomenon with relevant health outcomes within the South Africa context, especially among women who have experienced trauma and violence (Ungar, 2013). This additional research can help identify areas of policy to create equitable environments that focus on “changing the odds” for young women at risk, rather than just beating the odds through resiliency (Seccombe, 2002).
This study has several limitations. Analyses were performed on only cross-sectional data, which prevents us from making inferences around causality. Future research should seek to measure resilience as well as other individual and community-level factors at multiple time-points to address limitations related to direction of associations and temporality. While all measures were used previously in South Africa, not all were specifically validated for this age group of AGYW in South Africa. Additionally, this study includes only self-reported data, which means the data are subject to limitations of other self-measurements, such as social desirability bias. Researchers attempted to limit this bias by using tablets to administer the questionnaire, and having participants respond to sensitive questions related to substance use and violence privately, but these steps may not have addressed these limitations fully. While these are limitations to the study, there are some strengths. These data are derived from a rigorous systematic sample, allowing one to generalize results to girls and young women of this age group from sites in South Africa facing high HIV burden. Furthermore, this study focused on girls and young women, who bear a disproportionate burden of violence; as such, this study offers insights into directions for further resilience research in girls and young women from other regions who have experienced interpersonal violence including directions for resilience promoting factors that are worth investigating in other settings.
Conclusions
South African AGYW live within a context of heightened gender-based violence, but the concept of resilience remains unexamined. This study used a representative household-based sample to examine differences in resilience based on experiences of violence, and to identify factors associated with resilience among AGYW who experienced intimate partner and sexual violence. Increasing our understanding of how resilience is manifested among this population offers a strengths-based approach to preventing and addressing violence against AGYW. Findings from this study offer potential areas of intervention that can be targeted to potentially increase the efficacy strengths-based programming to address IPV and sexual violence. This study also demonstrates a need for more longitudinal resilience research to capture the complex interactions of resilience and health over time. Finally, additional research and advocacy is needed to develop policy aimed at reducing the high rates of trauma and violence experienced by South African girls and young women.
Footnotes
Author’s Note
Ashleigh LoVette is also affiliated with Johns Hopkins University, School of Nursing, Baltimore, MD, USA.
Acknowledgment
We acknowledge and thank the adolescent girls and young women (AGYW) and their caregivers who participated in this survey.
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The AGYW intervention was funded by the Global Fund to Fight AIDS, TB, and Malaria. The combination HIV prevention interventions were implemented in 10 districts in South Africa by a range of government departments and civil society organizations that were appointed by the organizations responsible for the management of the AGYW program: Western Cape Department of Health, KwaZulu-Natal Treasury, Kheth’Impilo, Soul City Institute for Social Justice, and the Networking HIV and AIDS Community of Southern Africa (NACOSA). The program was aligned with the She Conquers campaign and was implemented with support from the South African National AIDS Council (SANAC) through the Country Coordinating Mechanism (CCM) and the CCM Secretariat. This research has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention, under the terms of Cooperative Agreement Number 1U2GGH001150. This work was also supported by the Social Impact Bond Study of the South African Medical Research Council, funded by the Global Fund to Fight AIDS, TB, and Malaria. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies.