
Abstract
The aim of this study was to analyze the effect of intimate partner violence against women training program based on the theory of planned behavior on nurses’ and midwives’ approaches of violence. A randomized controlled trial was performed at nurses and midwives in Turkey, between December 2016 and August 2017. The participants were separated into an intervention group (n = 50) and control group (n = 49). According to the result of study, training given to the intervention group was more effective in increasing the intimate partner violence attitudes, practices, and reporting compared to the control group. These results show that this training program effectively developed the nurses’ and midwives’ approaches about intimate partner violence against women.
Introduction
Intimate partner violence (IPV)—actual or threatened physical, psychological, or sexual violence by a current or former partner—is the most common violence perpetrated against women (Krug et al., 2002). Violence is a global problem affecting women’s health (WHO, 2013a). World Health Organization (WHO) have reported that 4%-49% of women have experienced severe physical violence, 6%-59% have experienced sexual violence, and 20%-75% have experienced emotionally abusive act by their partners at some point in their lives (WHO, 2012). The global lifetime prevalence of intimate partner violence among ever-partnered women is 30%. In the literature, the prevalence of IPV is between 20% and 73% in studies conducted in the Middle East countries (Al-Modallal, 2017; Barnawi, 2017; Daoud et al., 2017, 2019, 2020; Eldoseri, & Sharps, 2020; Hawcroft et al., 2019; Malik et al., 2017). However, this percentage is 25.4% in Turkey, which is located in European region (WHO, 2013a). In a country-based study conducted in Turkey, the prevalence of physical violence that women have been exposed by their husbands or partners in a part of their lives is 35.5% (Hacettepe University Institute of Population Studies [HUIPS], 2014). In a meta-analysis by Ozcan et al., it has been reported that the prevalence of domestic violence against women was 57.2%, physical violence was 33.8%, verbal violence was 43.5%, emotional violence was 33.7%, economical violence was 26.8%, and the prevalence of sexual violence was 12.3%. The majority of the people who perpetrated violence were their husbands and/or partners (Özcan et al., 2016). The systemic analysis by Guvenc et al. (2014) have revealed that the intimate partner violence is between 13% and 78% in Turkey. According to these data, the prevalence of intimate partner violence is higher than the regional averages in Europe.
International Council of Nurses (ICN) expect the nurses to be in key positions in medical care, support, and counseling services for victims of violence (International Council of Nurses [ICN], 2001). Nurses and midwives have the opportunity of interacting with women in some point of their lives. Therefore, they are an important group in determining and helping the women who are exposed to violence (Gutmanis et al., 2007; O’Campo et al., 2008). It is crucial to identify and appropriately support the women who are exposed to violence to protect the health of the women and society (WHO, 2013b). Nurses and midwives have major roles and responsibilities, such as screening for violence, participating in physical examination with the women exposed to violence, keeping the medical records, assessing the current situation, informing the woman, providing security besides determining violence during home visits, intervening, and making plans for security (Bahar Özvarış et al., 2016; WHO, 2013b).
Routine screening is important in revealing cases of violence that have remained hidden. Routine screening by health care professionals significantly increases the diagnosis of IPV (WHO, 2013b). When IPV survivors or those at risk for IPV are identified early, health care professionals will be able to assist them in maintaining or ending the relationship in a safer manner. Screenings are a valuable opportunity for women to explain their experiences of violence to health care professionals. Studies have shown that survivors of violence can talk to health care professionals they trust about their experiences of IPV (Gutmanis et al., 2007; Häggblom et al., 2005; Johnston, 2006).
In many countries such as the USA, Australia, Canada, Sweden, England, and Japan, clinical guidelines have been developed for the use of health care professionals in the early detection of the experience of violence in women who are admitted to a health institution for any reason, especially women in prenatal, perinatal, and postnatal periods (O’Campo et al., 2008; O’Doherty et al., 2015; Stenson et al., 2005). Many professional health organizations encourage health care professionals to conduct routine IPV screening and recommend that all health care professionals follow guidelines that include political information and health-specific recommendations.
Screening about IPV according to “preventing violence against women” is recommended in health institutions in Turkey. There are standardized screening forms and registration forms prepared for this purpose that can be used by health care personnel. In this screening form, physical, sexual, economic, verbal/emotional violence by spouse/other family members are questioned. It is recommended to perform screenings especially in the emergency departments of hospitals and for all women of reproductive age 15 years and over who apply for primary health care, and these forms are expected to be completed by health care personnel (Bahar Özvarış et al., 2016). In Turkey, nurses and midwives working in primary health care services have important responsibilities within the scope of “preventing violence against women” (Bahar Özvarış et al., 2016). In the literature, studies (Gutmanis et al., 2007; Häggblom et al., 2005; Johnston, 2006; Lazenbatt et al., 2005) showing that interventions made by nurses and midwives to women who are exposed to violence increase the positive effects on women’s health, and this is crucially important in terms of showing the roles of nurses and midwives in primary health care services in the preventing against intimate partner violence.
When nurses and midwives encounter IPV against women, they may reflect their own negative attitudes, beliefs, and values, which may affect their ability to manage cases of violence correctly and appropriately (Allen et al., 2007; Häggblom et al., 2005; Lazenbatt et al., 2005). In the literature, there are studies showing that negative attitudes of health care providers prevent appropriate interventions to cases of violence (Furniss et al., 2007; Garcia-Morena, 2002; Waalen et al., 2000) and appropriate intervention capacity is low when encountered with intimate partner violence (Campbell, 2006; Krosnoff & Moscati, 2002; Yayla, 2009).
Nurses and midwives should have sufficient knowledge of violence for an effective preventing violence against women. Therefore, nurses and midwives should be educated in order to take preventive measures and medical interventions. In the literature, there are different studies for health care providers focusing on different methods related to intimate partner violence against women. These studies report that education changes negative attitudes of health care providers and affects screening, prevention, and reporting cases of IPV. (Baird et al., 2015; Jayatilleke et al., 2015; Kaplan & Komurcu, 2017; Sawyer et al., 2016; Schoening et al., 2004; Sis Çelik et al., 2015; Sprague et al., 2018; Spraque, 2019; Zaher et al., 2014). In this study, it has been planned to educate nurses and midwives working in primary health care services against intimate partner violence based on the theory of planned behavior (TPB).
The TPB, developed by Ajzen, is one of the theories evaluating the factors affecting behavioral changes. This theory proposes a model of how human behaviors can be directed. In order to understand whether an individual has an intention to do something, it predicts that it is necessary to know the individual’s motivational factors to perform the behavior (attitude toward behavior), how much pressure is put on that person by the people around to do that behavior (subjective norm) and whether that person has the full perception about the behavior that he/she is about to perform (perceived behavioral control). It states that, by changing these three factors, it provides a possibility for the individuals to perform the desired behavior, and they can do what they want to do (intention/behavior) (Montaño & Kasprzyk, 2015). In this study, an intervention program based on the TPB, which may affect attitudes, intentions, and behaviors of the nurses and midwives for intimate partner violence, was developed and executed. In this context, TPB can be used as a scientific road map for behavioral changes by evaluating the attitudes, intentions, and behaviors of nurses and midwives who play important roles in identifying intimate partner violence, preventing violence, and protecting women’s health.
Determining the approach of nurses and midwives toward cases of violence, raising awareness against violence, and performing supportive and assistive studies for women exposed to violence are important in the preventing violence against women. The results of this study may set a model for the education program to focusing on intimate partner violence. We think that our study will facilitate the planning of services given by nurses and midwives working in primary health care to the women who are exposed to violence. Therefore, in this study, we aimed to evaluate the effect of education program on approach of nurses and midwives for intimate partner violence that is developed based on TPB.
Materials and Methods
Study Design
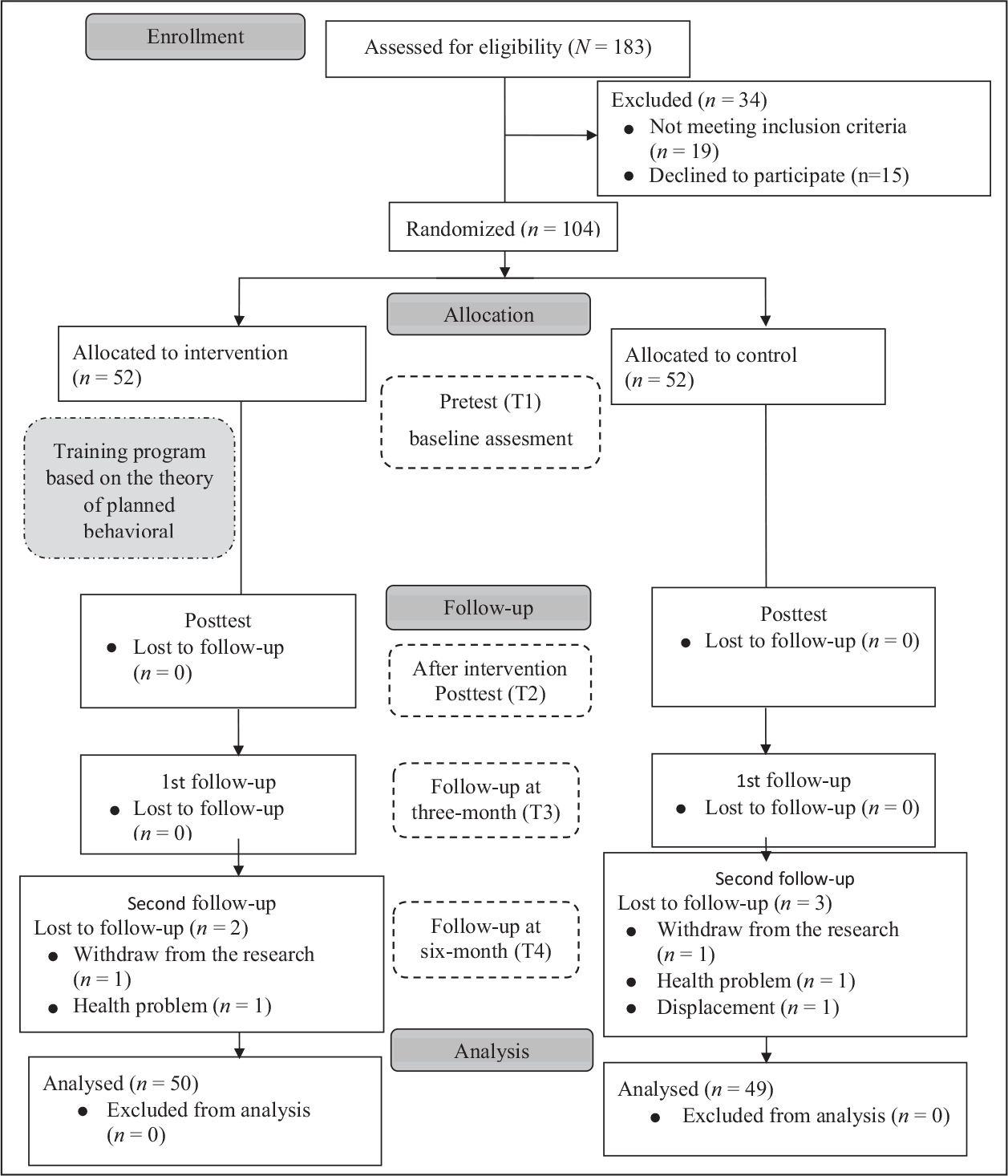
This randomized controlled trial was carried out with nurses and midwives working as family health staff in 58 Family Health Centers (FHC) in Denizli, in western Turkey, between December 2016 and August 2017. The study utilized with pretest, posttest, a three-month and a six-month follow-up evaluation. Figure 1 shows the CONSORT flow diagram of this study.
CONSORT diagram of the study.
Participants
The study was conducted with nurses and midwives working as family health staff in 58 FHC. The study population included 183 nurses and midwives. The sample of the study consisted of 104 nurses and midwives, including 52 in the intervention group and 52 in the control group.
Power analysis was performed to determine sample size. A similar previous study’s effect size was used to calculate the sample size of the study (Schoening et al., 2004). By using the data of this study, alpha error level was calculated as 0.05, effect size as 0.60, and power as 80% and sample size was calculated as 45 people for each group. It was decided that both groups should include 52 participants considering account the parametric test assumptions and the possibility of participant abandoning the study. The inclusion criteria for the participants are as follows: (a) work as family health staff and (b) voluntary participation in the study. The exclusion criteria were to receive training about the intimate partner violence against women in the last one year. The participants were assigned randomly into the intervention and the control groups by using a simple random numbers table. Participants in the intervention and control groups can influence each other in the same clinical study setting. Therefore, all participants who volunteered to participate in the research in the same FHC were in the same group. Participants were considered as cluster groups according to the FHC they worked in, and each FHC was assigned to the experimental or control group as a cluster.
The study was initially intended to have 52 participants divided as intervention and control groups. However, two participants from the intervention group and three participants from the control group loss of in the six-month follow-up of the study. The study was completed with a total of 99 participants, including 50 participants in the intervention group and 49 participants in the control group (Figure 1).
The Intervention
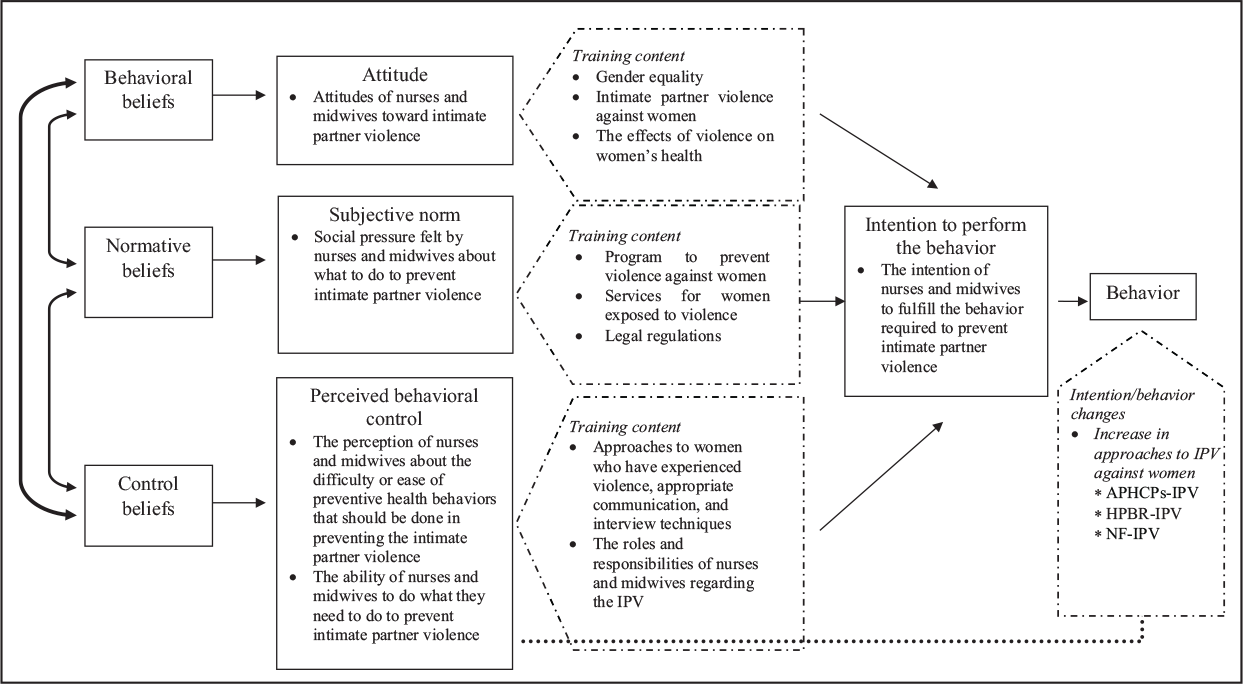
The theoretical framework of this study is based on the TPB (Figure 2). The intervention (training) program of this research was developed based on the concepts of TPB. The five-sessions training program based on the TPB was applied to the intervention group in order to improve the attitudes and practices of the participants on the intimate partner violence against women and to support reporting of intimate partner violence against women. The program was prepared by the researchers by considering the literature and the recommendations obtained from the interviews with the expert people who specialize in violence against women (Bahar Özvarış et al., 2016; Kalra et al., 2017; O’Campo et al., 2008; O’Doherty et al., 2015; Schoening et al., 2004; Sprague et al., 2018; WHO, 2013b; Zaher et al., 2014). The program sessions topics included gender equality, intimate partner violence against women, effects of violence on women’s health, prevention of violence, legal regulations, services offered, appropriate communication and interview techniques, the roles and responsibilities of nurses, and midwives in relation to intimate partner violence (Figure 2). A five-session training program were held once a week for five weeks. Each session took 60 minutes. The program included various educational tools such as a Power Point presentation, training booklet, movie screening, case study, role play, question-answer, and discussion. The data were evaluated four times before the intervention, after the intervention (15 days), and at the follow-up stage third month and sixth month.
Structuring the study according to the theory of planned behavior.
Data Collection
Data were collected four times between December 2016 and August 2017 through a pretest given at before intervention (T1), a posttest given at 15 days after intervention (T2) and a follow-up test at three months (T3) and six months (T4) after intervention. Data were collected by researcher.
Instruments
Data were collected using a demographic data form, The Attitudes and Practices of Health care Providers Regarding Intimate Partner Violence (APHCPs-IPV) survey scale, The scale of Health Professionals’ Intentions/Behaviors Regarding Reporting Intimate Partner Violence (HPBR-IPV), and the notification form for intimate partner violence against women (NF-IPV).
Demographic data form
The demographic data form included questions about nurses’ and midwives’ age, education level, position, and years of experience.
The Attitudes and Practices of Health Care Providers Regarding Intimate Partner Violence survey scale (APHCPs-IPV)
The APHCPs-IPV survey scale was originally developed by Gutmanis et al. (2007). The scale was adapted into Turkish by Gezgin and Toraman (2014). The Turkish version of the scale of 42 items and consists of eight subscales. The subscales are (a) preparedness (items 2, 8, 14, 15, 16, 17, 23, 27), (b) self-confidence of the practitioner (items 3, 11, 13, 19, 26, 29, 40), (c) lack of control (items 1, 4, 6, 7, 9, 21, 38), (d) comfort following disclosure (items 24, 25), (e) professional support (items 28, 39, 41, 42), (f) practice pressures (items 12, 31, 33, 35, 36), (g) abuse inquiries (items 5, 10, 18, 20, 22, 30), and (h) practitioner consequences of asking (items 32, 34, 37). The questionnaire began with a practice scenario regarding a pseudonymous patient. The respondents were asked to respond to 42 items designed to reflect either a barrier or a facilitator to their current practices of routine inquiry—termed screening in the survey questions—using either their own experience or the provided scenario. It is scored on a 4-point scale ranging from 1 to 4 (1—strongly agree, 2—agree, 3—disagree, and 4—strongly disagree). The APHCPs-IPV scale total scores range from 42 to 168. Cronbach’s alpha of the Turkish version of the APHCPs-IPV general scale was 0.66. The test-retest correlation coefficient was 0.90 for the total scores of the Turkish version (Gezgin & Toraman, 2014). Higher scores reflected greater self-reported preparedness, self-confidence, feelings of professional support, comfort with abuse inquiries, and comfort with discussions following disclosure as well as decreased concern about the consequences of abuse inquiries and decreased feelings of no control and system pressures (Gutmanis et al., 2007).
The scale of Health Professionals’ Intentions/Behaviors Regarding Reporting Intimate Partner Violence (HPBR-IPV)
The HPBR-IPV scale was developed by Koştu and Uysal Toraman (2016) based on the TPB. The scale consists of 21 items that aim to assess the intention/behavior of health care providers to report their intimate partner violence. Likert-type scale items answered from 1 to 7 (1—do not agree, 7—strongly agree). The HPBR-IPV scale scores range from 21 to 147. Values close to the highest score that can be taken from the scale are positive and values close to the lowest score reflect negative intent/behavior. Cronbach’s alpha of the HPBR-IPV was 0.96. The correlation coefficient for test-retest reliability was 0.97 (Koştu & Uysal Toraman, 2016).
The Notification Form for Intimate Partner Violence against women (NF-IPV)
The NF-IPV form was created by the researcher to determine of the participants how much intimate partner violence against women reported to the Provincial Health Directorate on a monthly basis.
Data Analysis
The data were evaluated with IBM Predictive Analytics Software (PASW) Statistical Product and Service Solutions (SPSS, Chicago, IL, USA) version 22.0. Descriptive characteristics were evaluated with frequencies, percentages, means, and standard deviations. The chi-square test was used to test homogeneity. The two-way repeated measures analysis of variance and Friedman analysis of variance were used to compare the intervention and control groups. In further analysis, paired sample t-tests with Bonferroni adjustments and Wilcoxon signed ranks test with Bonferroni adjustments were used. Cohen’s d effect sizes were performed to examine differences in the mean percentage change in the outcome variables between the groups over time. A p value less than .05 were considered significant.
Ethical Consideration
The study protocol was approved by the institutional review board of the Ege University Faculty of Medicine Clinical Research Ethics Committee. Written informed consent was obtained from participants included in the study. The participants were informed that their participation was voluntary and that they could withdraw from the study at any time. After the study was completed, the nursing interventions offered to the intervention group were also given to the control group. Rules specified in the Helsinki Declaration were observed in the data collection phase.
Results
Descriptive characteristics of participants. Characteristics of the intervention and control groups are shown in Table 1. The descriptive characteristics of the nurses and midwives in the intervention and control groups in this research were tested for homogeneity to confirm that there were no differences. The experimental and control groups were statistically similar (p > .05) and homogenous (Table 1).
Findings on intimate partner violence against women of participants. The mean of pretest, posttest, and follow-up test scores obtained from the intervention and control groups were compared in APHCPs-IPV survey scale. Mean scores for the APHCPs-IPV and its subscales are shown in Table 2. The difference between the pretest, posttest and follow-up test values were significant in the intervention group (F = 121.783, p < .001), and control group (F = 16.717, p < .001). The difference between the intervention and control groups’ APHCPs-IPV scores were not significant T1 (t = –0.637, p = .526), but they were significant T2 (t = 4.446, p < .001), T3 (t = 5.595, p < .001), and T4 (t = 7.085, p < .001). The effect sizes of the APHCPs-IPV survey scale scores changes between T1 and T4 of the intervention group was measured as large effect (0.88).
Characteristics of the Intervention and Control Groups (n = 99).
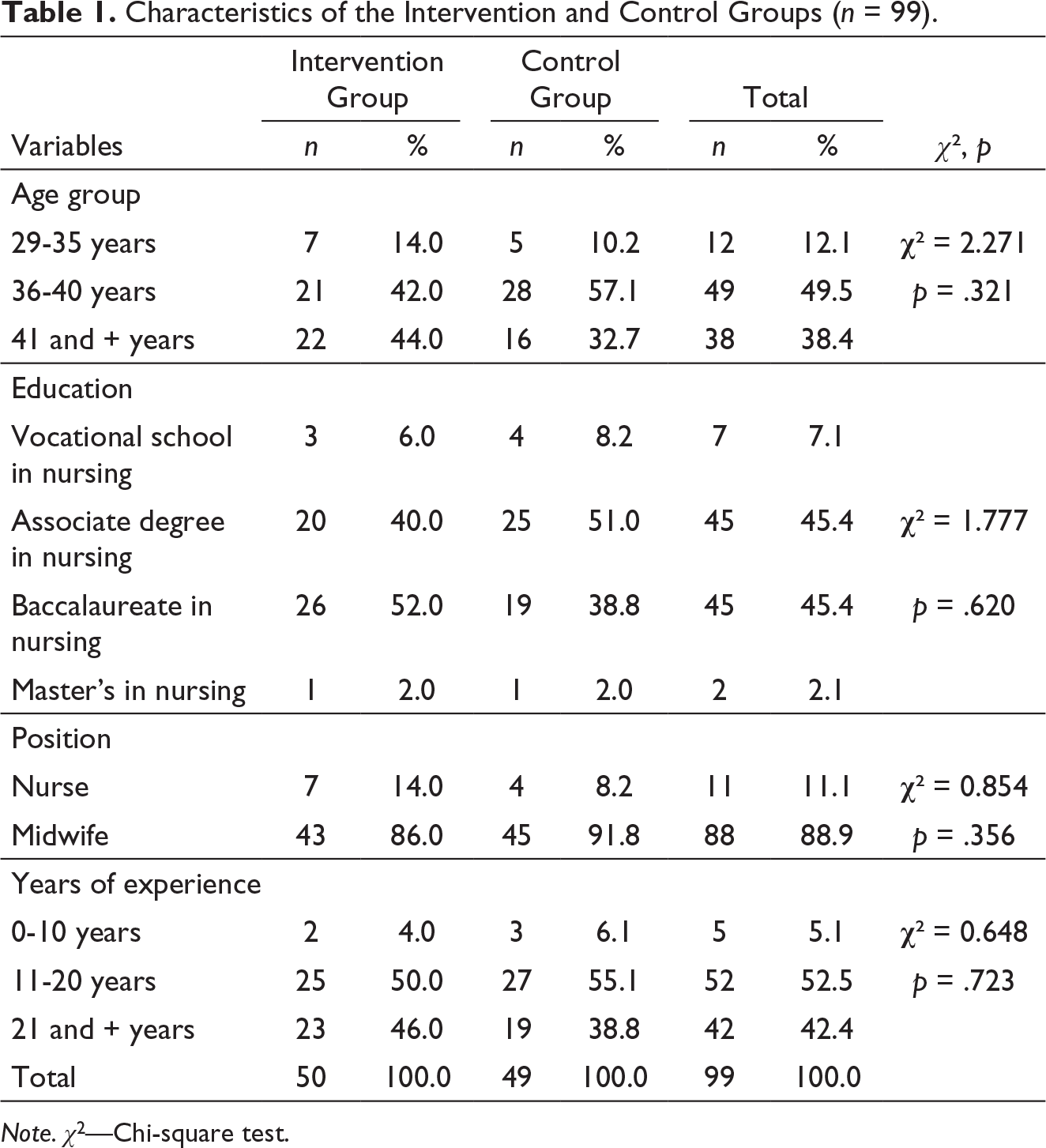
Note. χ2—Chi-square test.
Pretest, Posttest, and Follow-up APHCPs-IPV Scores in Intervention and Control Groups.
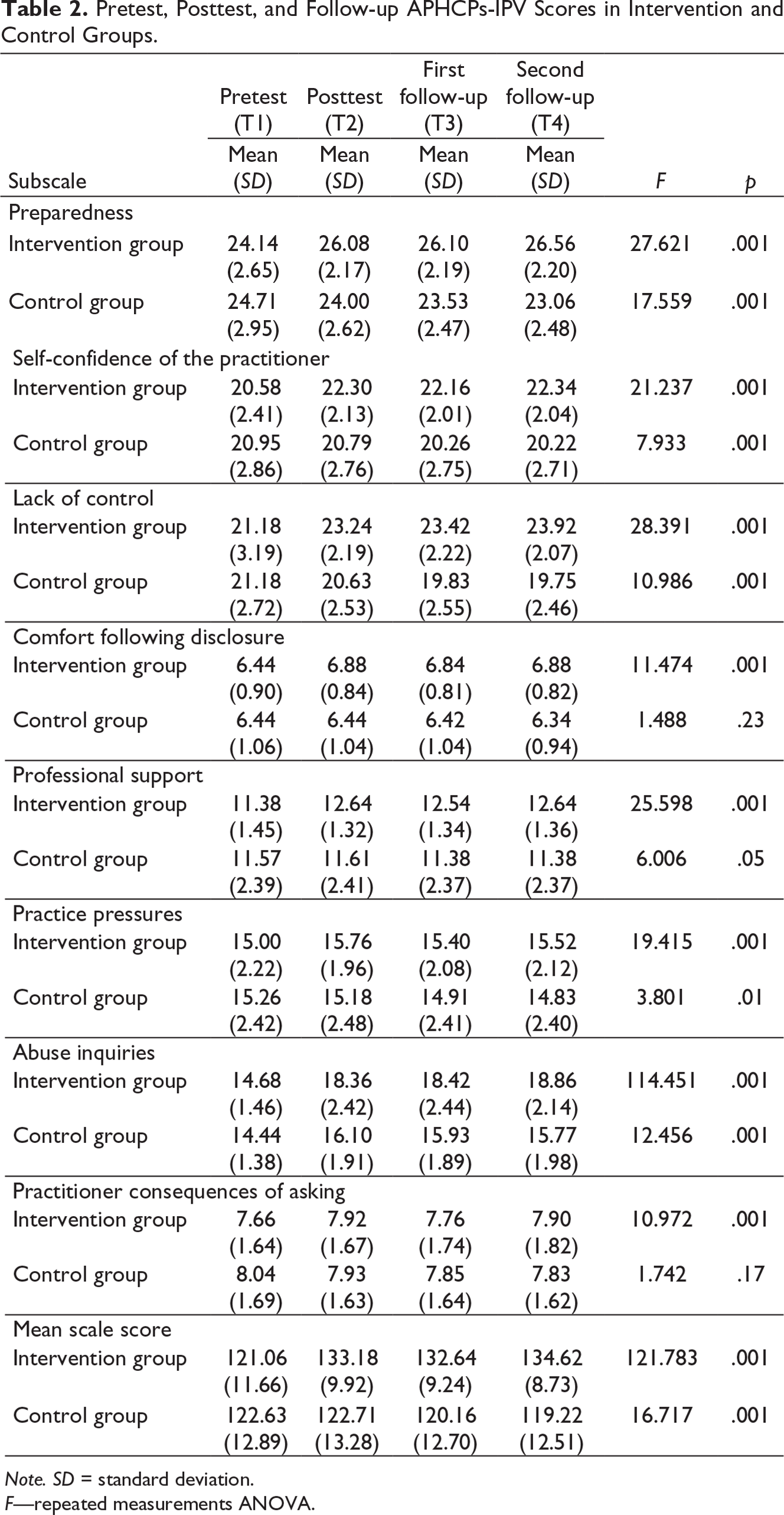
Note. SD = standard deviation.
F—repeated measurements ANOVA.
Pretest, Posttest and Follow-up HPBR-IPV Scale Scores in Intervention and Control Groups.
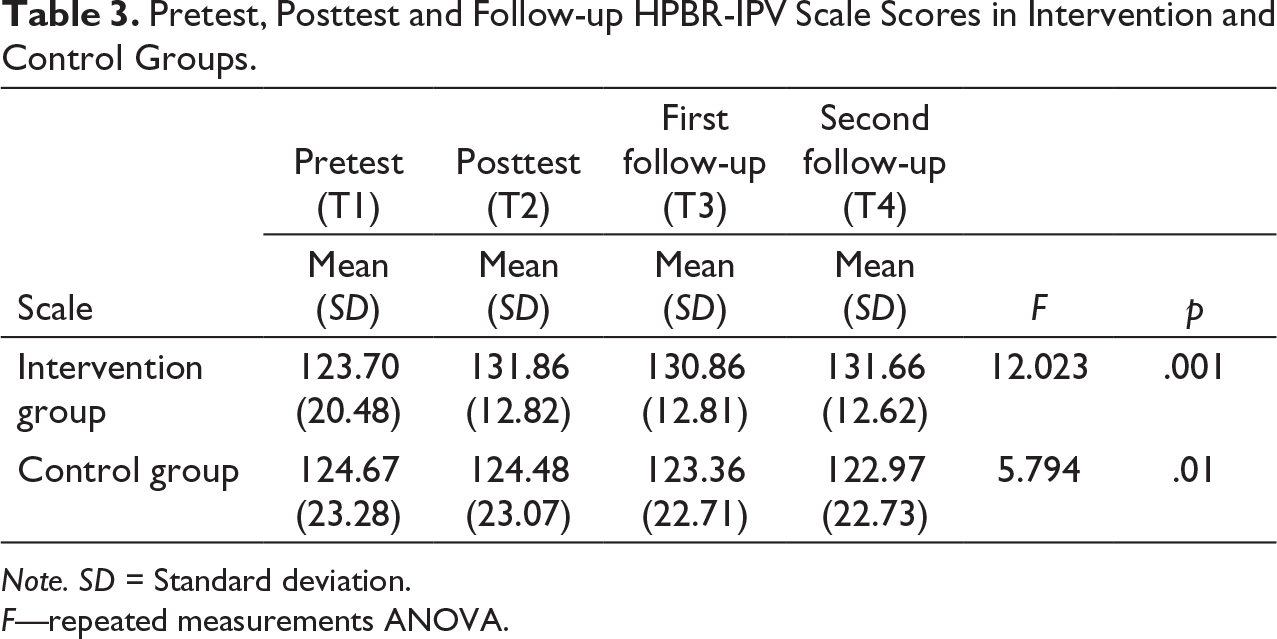
Note. SD = Standard deviation.
F—repeated measurements ANOVA.
Notification of NF-IPV in Intervention and Control Groups.
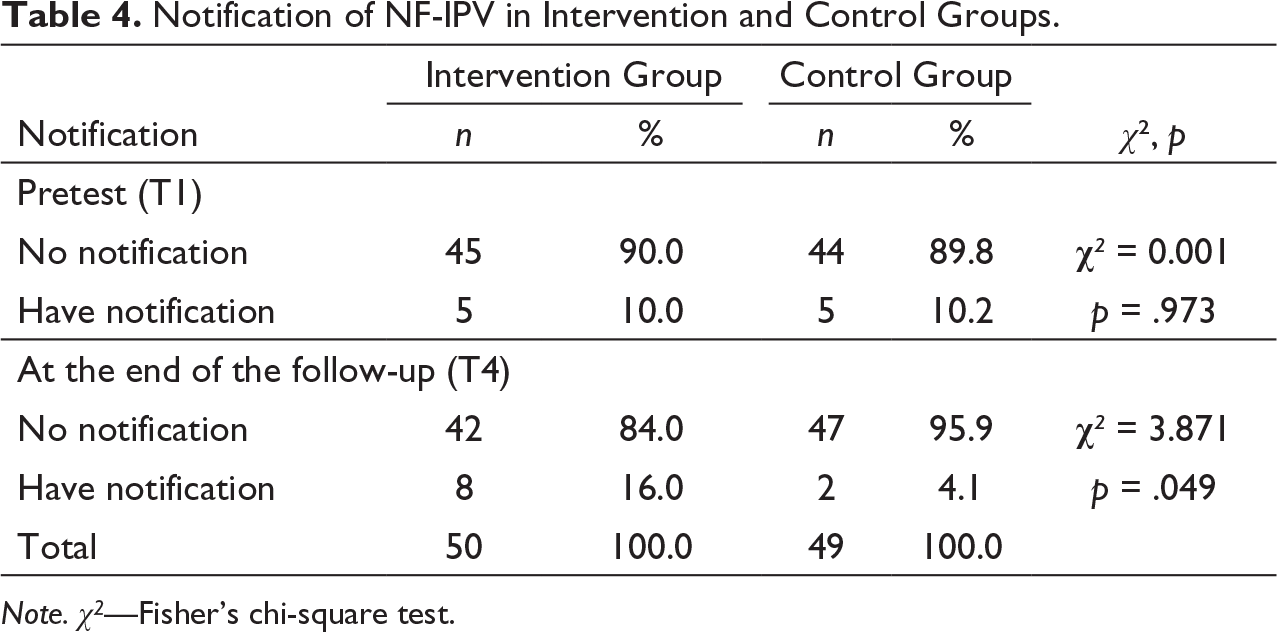
Note. χ2—Fisher’s chi-square test.
Discussion
Women who are exposed to violence often require and seek for medical care and majority of these women visit health facilities at least once in their lifetime (Rivas et al., 2015). These women feel more relaxed in expressing themselves to nurses and midwives (Cann et al., 2001; Orhan & Gölbaşı, 2011; WHO, 2013b). In the “WHO violence against women guideline” (2013), it is suggested that it is of major importance to improve the attitudes of the nurses and midwives who offer health service to victims of violence, and they should be properly educated to have strong knowledge and skills for identifying the women who are exposed to violence (WHO, 2013b).
When we investigated the attitude and practices of the nurses and midwives to IPV victims, we determined that nurses and midwives in the intervention and control groups had similar attitudes before the education program. When we examined the average total scale score at the end of the follow-up after the training program, we determined that while the attitudes and practices of the nurses and midwives in the intervention group for IPV victims improved positively over time, the attitudes and practices of the nurses and midwives in the control group did not change significantly. The education program based on the TPB positively improved the attitudes of nurses and midwives in the intervention group. Similar to our study, it has been reported that education programs on violence against women conducted in different periods have improved the attitudes and practices of nurses and midwives. Baird et al. (2015) have reported that the negative attitudes and behaviors of midwives who have been educated for violence against women have changed over time. Jayatilleke et al. (2015) have reported that the behaviors of educated midwives have significantly improved against victims of violence. In a study by Sis Çelik et al. (2015) it has been reported that the education on violence against women has reduced the negative attitudes of nurses and midwives toward violence. In another study, it has been stated that education on violence toward women affects the attitudes of individuals and attitude can be changed by education (Kıyak & Akın, 2010). In their systematic review, Sawyer et al. (2016) have concluded that educational interventions have a positive effect on development of knowledge, attitudes, skills, and behaviors of health workers related to IPV. Other similar studies report that education positively improves the attitudes and behaviors of health workers (Kaplan & Komurcu, 2017; Schoening et al., 2004; Sprague et al., 2018). The results of our study are similar with the literature and shows the importance of education of nurses and midwives about violence against women. According to our results, the planned education positively affects the attitudes and behaviors of nurses and midwives for intimate partner violence against women.
Studies on violence against women have shown that health care workers have positive intentions or behaviors to report when faced with violence (O’Doherty et al., 2015; Sarıbıyık, 2012; Sis Çelik et al., 2015). Our results showed that the average scores for intention/behavior to report for IPV against women was similar in both groups before the education, however, the average score increased in the intervention group after the education. On the other hand, there was no significant change in the control group in terms of average score after the education. We can suggest that the education program has positively affected the intention/behavior of the nurses and midwives in the intervention group to report against violence. Similarly, Sarıbıyık (2012) has shown that 82.2% of nurses and 78.9% of midwives would report when faced with violence against women. In a study by Yayla (2009), 66.4% of nurses and 61% of midwives have stated that they would report if they ever faced an act of violence against women. In this context, our results support the literature.
It is important that the records of cases of violence against women are complete, accurate, and clear (WHO, 2013b). There are programs to prevent violence against women in Turkey. Within the scope of this program, first of all, in-service trainings are given to health care personnel working in emergency health care and primary health care services to increase their sensitivity to violence against women and to do IPV screening, treatment policy, reporting to police and social services. When faced with violence against women, health care workers in Turkey, primarily to make the medical care and treatment by providing the safety of women exposed to violence, violence to record findings, to be present in the reporting and notification. There are legal regulations regarding this (Bahar Özvarış et al., 2016; The Protection of Family and Prevention of Violence Against Women Code, 2012).
In health institutions of Turkey, “Domestic Violence Against Women Registration Form” is used to record the information obtained from the victim during the interview, which aims to obtain and evaluate the history of violence against women. In this form, information on application, information about women exposed to violence, contact information, history of violence, risk assessment data, and information about the intervention of health care personnel against the victim woman. Health personnel make a report of violence by filling this form. When faced with violence, health institutions report violence against women to the local health authorities at the end of each month (Bahar Özvarış et al., 2016). In our study, while 90% of nurses and midwives in the intervention group did not report any cases of intimate partner violence before the education, only 10% reported a case. After the education, the rate of completing a form for violence against women has increased. The statistical analysis between the groups showed that this increase is significant. Completing the violence victim notification form against women appropriately and correctly will ensure that the violence cases are correctly evaluated, the victims of violence are directed to the services they require, and they receive appropriate support. In addition, the information obtained through this form is important for monitoring, rehabilitation, and support (Bahar Özvarış et al., 2016). The health care workers are legally obliged to report on violence, when faced with violence against women (Bahar Özvarış et al., 2016; WHO, 2013b). However, literature shows that the rate of completing a violence notification form is quite low. In the systematic analysis by Kalra et al. (2017), it has been suggested that the attitude of health care workers toward violence against women may reduce the rate of reporting the cases of violence. It has been shown that physicians and nurses in primary care clinics complete a violence notification form only for 23.6% of violence cases against women (Çatak, 2015). Uysal (2006) has reported that only 10% of health care personnel start the legal procedure by completing a notification form. Kaplan and Komurcu (2017) have reported low rates of reporting a case of violence.
According to the Protection the Family and Prevention of Violence Against Women program in Turkey (2012), physicians, dentists, pharmacists, midwives, nurses, and other health care providers should fill out the notification form of violence when faced with violence against women and should report the cases. However, despite the existence of a variety of legal arrangements in the Turkish legislation, the successful response to violence victims is dependent on providers’ knowledge, attitudes, and preparedness (Koştu & Uysal Toraman, 2021; Sarıbıyık, 2012; Taskiran et al., 2019). On the other hand, the family is seen as a private institution in Turkish society. The society believes that problems within the family should be solved by the family. Nurses are also affected by this view and may accept the same attitudes (Efe & Taşkın, 2012).
Studies have shown that, when nurses and midwives face with violence against women, they rather prefer to treat the patient and give medical care instead of reporting the case (Christofides & Silo, 2005; Häggblom et al., 2005; Kıyak & Akın, 2010; Orhan & Gölbaşı, 2011; Stenson et al., 2005). However, the first step in dealing with women who are exposed to violence is to ensure the safety and to provide appropriate treatment and care (Bahar Özvarış et al., 2016; WHO, 2013b). It has been reported that 28.8% of nurses and midwives have informed the patient and 26.9% of them have stated that they mentally comforted the patient (Orhan & Gölbaşı, 2011). Stenson et al. (2005) have reported that midwives listened to the stories of the women who are victims of violence, and they provided psychological support and information about where they could get help. On the other hand, some studies have reported that nurses experience difficulties in knowing how to ask the appropriate questions, what to do or what so say (Beynon et al., 2012; Cox et al., 2001; Häggblom et al., 2005). Therefore, it is recommended that nurses should be supported with necessary information and education to ensure a more effective role in meeting the physical, emotional, and safety requirements of women who are victims of violence (O’Campo et al., 2008).
Conclusion
We determined a significant difference between the intervention group, which was trained based on TPB, and control group about IPV in terms of mean scores of attitude and practices and intention/behavior to report IPV against women. In addition, there is a significant difference between the intervention and control groups with respect to completing the form of IPV against women after the education program.
To conclude, the results of our study show that the training program for IPV against women based on the TPB given to nurses and midwives can directly affect the intention/behavior of reporting violence against women by improving their attitudes and practices.
Limitations
The limitation of the study was that the data obtained is based on the self-report of the participants. The attitudes of nurses and midwives regarding intimate partner violence were also limited to the factors measured by the scales used in the study.
Footnotes
Acknowledgments
The author(s) would like to thank all nurses and midwives who took part in the study.
Declaration of Conflicting Interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.