
Abstract
Legally mandated treatment is common in the criminal justice system, for example, for anger management, substance misuse, and intimate partner violence. Past studies have compared voluntary and legally mandated treatment participants but have not distinguished a third, in-between group that is formally pressured to participate in treatment, but not mandated by the criminal justice system. The current study aimed to assess differences on individual characteristics (e.g., sociodemographic and psychiatric) and baseline measures of psychopathology (e.g., anger, aggression, and depression) across three levels of voluntariness and to determine whether voluntariness was associated with treatment recommendation, refusal, and completion at an outpatient anger treatment clinic. Data were retrospectively gathered from the clinical charts of 405 participants. Referrals were classified as voluntary (e.g., self-referred, 61%), formally pressured (e.g., required by work, 14%), or legally mandated (e.g., court order, 25%). Legally mandated participants were younger, more likely to have substance use disorder, less likely to be women, to have a high school education, or to be on psychiatric medications compared to the other two groups. Voluntary participants scored higher on measures of self-reported anger, depression, and stress than the legally mandated participants. Legally mandated participants in particular presented with non-clinical levels of anger and aggression. Level of voluntariness did not affect the decision to recommend individual or group therapy after an intake assessment, but legally mandated participants were significantly more likely (OR = 2.30) than voluntary participants to refuse recommended treatment. Level of voluntariness did not have a significant association with treatment completion. Findings support our distinction between legally mandated and formally pressured participants, but do not support previous research that suggests legally mandated individuals have lower attrition rates in similar treatment programs. The study has implications for the criminal justice system and for anger treatment programs who admit participants with varying levels of voluntariness.
Legally Mandated versus Voluntary Treatment
Comparisons of legally mandated and voluntary participants have been made before for substance use treatment (e.g., Werb et al., 2016) and treatment for perpetrators of intimate partner violence (see Babcock et al., 2004; Feder & Wilson, 2005; Jewell & Wormith, 2010 for meta-analytic reviews). Jewell and Wormith (2010) concluded that legally mandated participants were more likely to complete treatment than non-mandated participants. One explanation for this effect may be the influence of coercion on the therapeutic relationship, given this relationship is one of the strongest predictors of psychotherapy outcome (Horvath et al., 2011). Manchak et al. (2014) were the first to demonstrate that there was significantly greater therapist control and participant adherence when treatment was legally mandated rather than voluntary.
Babcock et al. (2004) found a small (d = .18) positive effect on recidivism for legally mandated intimate partner violence treatment; however, many of the studies that were included in their review were greatly affected by participant attrition, and effect sizes were even weaker for the five experimental studies. Feder and Wilson (2005) used more rigorous inclusion criteria by only including studies with a matched control group, statistical controls, or established equivalence between groups before treatment began. Studies also had to have a minimum 6-month follow-up with measures of objective outcomes. The authors found modest benefits from the experimental studies but these effects vanished if the victim-reported outcomes were analyzed; there was no effect in the quasi-experimental studies.
Level of Voluntariness
Terms such as involuntary, court-mandated, legally mandated, or coercive treatment are sometimes used interchangeably throughout the literature, but there are varying degrees of voluntariness in treatment (Klag et al., 2005; Prendergast et al., 2002). For instance, a child protection agency may require someone to get assessed and treated following an allegation of child abuse in order to prevent their child from being taken into state custody. An employer may require an employee to participate in assessment and possibly treatment in order to return to work after an angry episode in the workplace.
The limitation of distinguishing only legally mandated and voluntary participants is highlighted in research by Parhar et al. (2008). The authors used a coercion severity rating system inspired by Klag et al. (2005) and found that effect sizes were greater for coerced treatment (includes legally mandated treatment with minimal or inconsistent consequences for non-adherence, non-mandated treatment but with legal consequences, such as return to court, and non-mandated treatment with incentives, such as early parole release) than legally mandated treatment in both community and institutional offender treatment. There was no difference between coerced and voluntary participants in terms of positive treatment effect, whereas there was no significant treatment effect for legally mandated participants.
Treatment Attrition
Though legally mandated treatment is thought to increase participation, attrition rates are still high. Dropout was 38% in a sample of 35 intimate partner violence treatment studies (Olver et al., 2011), and between 22% and 72% in anger treatment for offenders (Henwood et al., 2015). Attrition from offender and outpatient treatment, including intimate partner violence and anger treatment programs, has consistently proven to be associated with poorer outcomes (Dowden & Serin, 2001; Olver et al., 2011; Parhar et al., 2008). In fact, Olver et al. (2011) report that recidivism rates in treatment non-completers were 10–23% higher than completers, and Henwood et al. (2015) report that all of the non-completer groups had greater recidivism than completer groups.
The impact of individual-level factors on treatment attrition have remained fairly consistent across the literature. Men who drop out of treatment for offending are more likely to be younger, unmarried, unemployed, have less education, lower incomes, a greater criminal history, and have substance use problems (Daly & Pelowski, 2000; Jewell & Wormith, 2010; Olver et al., 2011). Jewell and Wormith (2010) did not find a significant effect for anger and depression on attrition in their meta-analysis.
Anger Treatment
Though anger can also have positive effects such as increasing motivation and goal-setting behavior (Del Vecchio & O'Leary, 2004), it has also been associated with a range of negative consequences. For example, a recent meta-analysis found a large effect size for the association of anger and aggression (Chereji et al., 2012) and high levels of anger are often present in common mental disorders such as mood, anxiety, and impulse-control disorders (Lench, 2004). There is also evidence that high anger is related to physical health problems such as an increased risk for cardiovascular disease (Helmers et al., 1994; Suinn, 2001). We define dysfunctional anger as frequent, intense, or chronic that results in significant distress or impairment, for example, when someone’s difficulties with anger result in the loss of relationships, employment, or legal trouble. The prevalence of dysfunctional anger in the general population is unclear, but a survey of 529 practicing psychologists and psychiatrists found that participants with chronic anger problems were just as common as those with generalized anxiety disorder, where the latter has a prevalence of 3% in the general population (Lachmund et al., 2005). In a sample of over 9000 Americans, Kessler et al. (2006) reported a lifetime and 12-month prevalence of 7% and 4%, respectively, for Intermittent Explosive Disorder, the most anger-relevant diagnosis in the DSM-5. Intermittent Explosive Disorder is characterized by recurrent episodes of impulsive, aggressive outbursts that can include property damage, “road rage,” or assaults. However, Intermittent Explosive Disorder does not capture other types of dysfunctional anger, such as ruminative anger that builds over time or suppressed anger that results in passive-aggressive behavior.
People with dysfunctional anger can be referred for anger treatment. Anger treatment is a common recommendation for individuals who have been repeatedly aggressive, including assaults, workplace aggression, and intimate partner violence (e.g., DiGuiseppe & Tafrate, 2003). These referrals often go beyond recommendations, where the courts may mandate anger treatment as a condition of sentencing, or someone incarcerated for violent offenses may be legally mandated to participate in anger treatment in order to be eligible for early release. Legally mandated treatment can be contrasted with voluntary treatment, where the person recognizes they need treatment and seek it out. There is also an in-between level of voluntariness, which we refer to as formally pressured, where someone is not legally mandated but is pressured to seek treatment by others, for example, a condition of return by an employer after an angry or aggressive episode at work (e.g., Geck et al., 2017).
Present Study
Before we conclude that level of voluntariness is linked to differences in treatment outcome or recidivism, we need to determine if differences in treatment recommendation, refusal, or non-completion are better explained by demographic or clinical differences between those who are legally mandated, formally pressured, or voluntary.
In the present study, we first compared anger clinic participants in these three groups on demographic and clinical characteristics. We expected significant differences on multiple characteristics; for example, because legally mandated participants have criminal justice involvement, by definition, we predicted they would be more likely to be male, younger, more likely to have criminal histories, and more likely to use substances than other participants, given ample evidence that criminal justice involved people differ from others in these ways (H1: Bonta & Andrews, 2016; Public Safety Canada, 2019).
We also predicted that voluntary participants would score higher than formally pressured or legally mandated participants in terms of their anger scores and psychopathology, because they voluntarily sought treatment, which we presumed was due to their distress or impairment (though it could have been for other reasons). In contrast, legally mandated participants, and perhaps formally pressured participants, would score lower in anger and psychopathology and higher on impression management because they were referred because of others’ concerns (e.g., aggression in the workplace or an assault charge) and either did not think they had an anger problem or were more likely to deny having problems (H2: e.g., Mills & Kroner, 2005, 2006).
We then examined the relationship between degree of voluntariness and treatment recommendation, refusal, and completion to see whether level of voluntariness helped explain differences in treatment course after controlling for demographic and clinical characteristics that differed between groups. We predicted there would be no difference in treatment recommendation across levels of voluntariness (H3), because treatment recommendations were supposed to be based on the clinical assessment and the presentation of dysfunctional anger, irrelevant of the referral source. However, we did predict that legally mandated participants would be more likely to attend treatment (indicated by attendance of at least one therapeutic session) and more likely to complete treatment than voluntary participants, with formally pressured participants in between (H4 and H5, respectively: consistent with, e.g., Jewell & Wormith, 2010).
Method
Participants
Participants were 405 adults assessed between March 2007 and December 2014 at an outpatient clinic for individuals with dysfunctional anger. Most of the participants were male (80%), White (73%), and were on average 35 years old (SD = 12.7). At the time of assessment, 32% of the sample lived with a partner, 25% lived with their parents, and 24% lived alone. Sixty-eight percent of the sample were not in a relationship. Just over half (59%) of the sample had a high school education, while 40% were unemployed, with 35% employed in full-time positions and 14% in part-time positions at the time of initial assessment. Over half of the sample (61%) had a criminal history upon presenting to the clinic.
Clinically, 85% of the sample was diagnosed at the initial assessment with at least one psychiatric disorder. The most common primary disorder was Substance Use Disorder (30%), followed by Mood Disorder (22%) and Anxiety Disorder (12%); 91 (22.5%) individuals had a personality disorder diagnosis. Seventy-one percent of the sample reported historical outpatient psychiatric treatment while 29% had a history of inpatient psychiatric admissions.
Setting
The anger clinic offers outpatient assessment and treatment—individual therapy, group therapy, and/or medication—offered by a psychiatrist or social worker. All participants assessed at the clinic required a formal referral. Initial intake assessment included a comprehensive self-report biographical assessment, completion of a battery of standardized measures, a biopsychosocial interview with the social worker, and a comprehensive clinical interview with the psychiatrist. Based on the interviews and standardized measures, the psychiatrist made a determination about whether the individual is experiencing dysfunctional anger. If they were determined to have dysfunctional anger, the individual was offered treatment at the clinic.
Individuals could receive individual and/or group therapy. Individual treatment may be offered in lieu (or in addition to) group treatment if there is a long wait until the next group rotation begins, if the individual is not comfortable participating in a group or if they require more intensive treatment in addition to weekly groups. Within the sample that attended treatment, 41% participated in both group and individual therapy, 42% participated in individual therapy only, and 17% participated in group therapy only, where participation meant attending one or more sessions.
Group therapy was based on the principles of Rational Emotive Behavioral Therapy (REBT; David et al., 2018) and ran weekly for a period of 14–16 weeks. Attendance records indicate whether participants were absent or present for each group session. During the final group session, participants completed a subset of standardized measures to provide post-tests to compare back to their pre-treatment baseline scores. Considering their attendance, quality of participation, and their pre-post scores, a collaborative decision was made regarding the individual’s need for further treatment. In some cases, participants were invited to attend a subsequent group. Treatment gains are shown by a majority of therapy participants after 8 to 12 sessions (e.g., Glancy & Saini, 2005; Howard et al., 1986). Given this, 10 sessions (individual or group) were chosen as the cut-off for whether a participant “completed” anger treatment or not, for the purposes of this study.
Procedure
The study used a retrospective design, analyzing data collected between 2015 and 2017. Clinical charts were used to code a range of demographic (e.g., age, gender, employment, and marital status), clinical (e.g., history of psychiatric treatment, substance use, and diagnoses), and legal variables (e.g., criminal history). All information related to referral status or indicative of voluntariness was captured as free-written to ensure appropriate detail was maintained.
In order to classify the sample by voluntariness—legally mandated, formally pressured or voluntary—all referral documentation and reports were carefully considered. A quarter (25%, n = 100) of the sample were considered legally mandated, 14% (n = 58) were considered formally pressured, and 61% (n = 247) was classified as voluntary. The following definitions were adapted from previous work (Klag et al., 2005; Parhar et al., 2008) when classifying each participant.
Legally mandated: Legally mandated referral referred to individuals who would face legal consequences if they did not attend. This kind of referral most often came from the courts (e.g., a judge’s order) or it was an explicit condition of their sentence or probation or parole conditions. Evidence of legally mandated referral usually came in written form from a legal source. Consequences of failing to comply may result in a stricter sentence, return to custody, or additional probation or parole restrictions.
Formally pressured: Formally pressured individuals were under formal (organizational) pressure to attend the clinic but were not legally mandated. Pressure could come from social service agencies, workplaces, or lawyers acting on behalf of the participant. Pressure was defined as a formal consequence for not agreeing to attend the clinic for assessment. For example, a child protection agency might require going to the clinic in order to retain custody or access to one’s child, or an employer might require assessment as a condition of returning to work. An example of a criminal justice referral without legal mandate was when a defense lawyer suggested their client should go for an assessment in anticipation of upcoming court proceedings, or when a probation or parole officer recommended treatment but it is not a specified probation or parole condition. Approximately, a third of the formally pressured group was referred through child protection, a third were referred through the workplace, and a third were referred by a defense lawyer. Some cases involved multiple forms of pressure, for example, someone pursuing changes in child custody or access were referred by child protection and were instructed to do so by their lawyer.
Voluntary: Individuals were considered voluntary if they self-referred for treatment without any indication of formal organizational or legal penalties if they did not attend the clinic. This group included individuals who self-referred; sought a referral after being encouraged by a partner, family member, or friend; or were recommended by a community health provider. Though the person might have felt pressured to seek treatment, for example, if a partner threatened the end of the relationship if they did not, we did not have information about level of motivation for treatment or the level of encouragement or pressure from others.
The study included three binary dependent variables: anger treatment recommendation, refusal, and completion. All of these dependent variables were coded from the clinical files. Anger treatment recommendation was made after the intake process outlined above; if the participant was recommended for treatment by the clinic psychiatrist, it was explicitly stated in the clinical file. Anger treatment refusal was coded as any individual who was recommended for treatment but did not show up to at least one therapeutic session. The participant may have either explicitly denied treatment or the file indicated that despite being recommended, they did not initiate treatment at the clinic following the intake assessment. Completion was coded dichotomously if the individual did (1 = yes) or did not (0 = no) complete 10 or more individual and/or group treatment sessions. This was coded using a count of the number of therapeutic sessions attended in the clinical file and based off evidence that treatment gains that will be made are often evident at this point (e.g., Howard et al., 1986).
Inter-Rater Reliability
Inter-rater reliability for group classification was calculated for a randomly selected 20% (n = 84) of the sample by two research assistants. The absolute agreement between the two raters was 91.7%; kappa was .84 (95% CI: 0.74, 0.95), which was described by Landis and Koch (1977) as “almost perfect agreement.” The lead author blindly rated the seven cases where there was disagreement by the two raters to make the final classification decision. There were no instances among these seven cases where the three raters assigned someone to all three different voluntariness categories.
Clinic Measures
Statistical Analyses
In order to test the hypotheses, a series of statistical analyses were conducted to assess how the legally mandated, formally pressured, and voluntary groups differed, and to determine if level of voluntariness had an effect on several treatment-related outcomes. Given the retrospective clinical data used in this study, there were missing data throughout all analyses; the adjusted sample sizes can be found in the tables. To assess voluntariness group differences across the sociodemographic, psychiatric, and baseline measures, both analysis of variance (ANOVA) and chi-square analyses were used, depending on whether the independent variable was continuous or nominal. Post-hoc tests were conducted on ANOVA results when a significant main effect was found. When Levene’s Test indicated that we violated the assumption of homogeneity of variances, the non-parametric equivalent for the main effect (Welches’ test) and post-hoc (Tamhane) was reported, in addition to adjusted degrees of freedom. When Levene’s Test was non-significant, Fisher’s Least Significant Difference (LSD) post-hoc test was used. Standardized residuals greater than +/− 1.96, which are the z-score equivalent to p < .05, were used to determine which cells were significantly discrepant from the others within chi-square analyses.
A series of three binary logistic regression analyses were conducted to assess the effect of voluntariness on three dichotomous treatment outcomes: anger treatment recommendation, anger treatment refusal, and anger treatment completion. Referral status was dummy-coded with voluntary being the reference group in all analyses; odds ratios were interpreted for the formally pressured and legally mandated group in reference to the voluntary group. The covariates for these analyses were the subset of variables that significantly differed between groups in the univariate analyses. These predictors were entered in a first block, while referral status was entered in a second block, to determine whether voluntariness could account for any variance in the treatment outcome above that accounted for by the other chosen covariates. Odds ratios and confidence intervals are reported for these regression models.
Results
Group Differences on Sociodemographic and Psychiatric Characteristics
Sociodemographic and Psychiatric Differences Between Legally Mandated, Formally Pressured, and Voluntary Participants at an Anger Disorders Clinic.

Note. *p < .05, **p < .01 for overall test; bolded values in chi-square tests indicate standardized residual value is beyond the +/− 1.96 (i.e. p < .05) threshold highlighting where the category proportion is significantly discrepant from what was expected.
aPost-hoc test indicates that voluntary participants were significantly (p < .01) older than legally mandated and formally pressured individuals, but no difference existed between formally pressured and legally mandated group;
bFisher’s Exact Test.
cOther includes: Asian, Middle Eastern, and Latino;
dOther includes: ADHD, autism-spectrum, impulse-control disorder, paraphilia, and psychotic disorder;
eIncludes cannabis which was illegal at the time of study data collection;
The overall n reflects the entire sample; there are missing data throughout some of the categories;
Baseline Measures of Anger, Aggression and Psychopathology between Legally Mandated, Formally Pressured, and Voluntary Participants at an Anger Disorders Clinic.
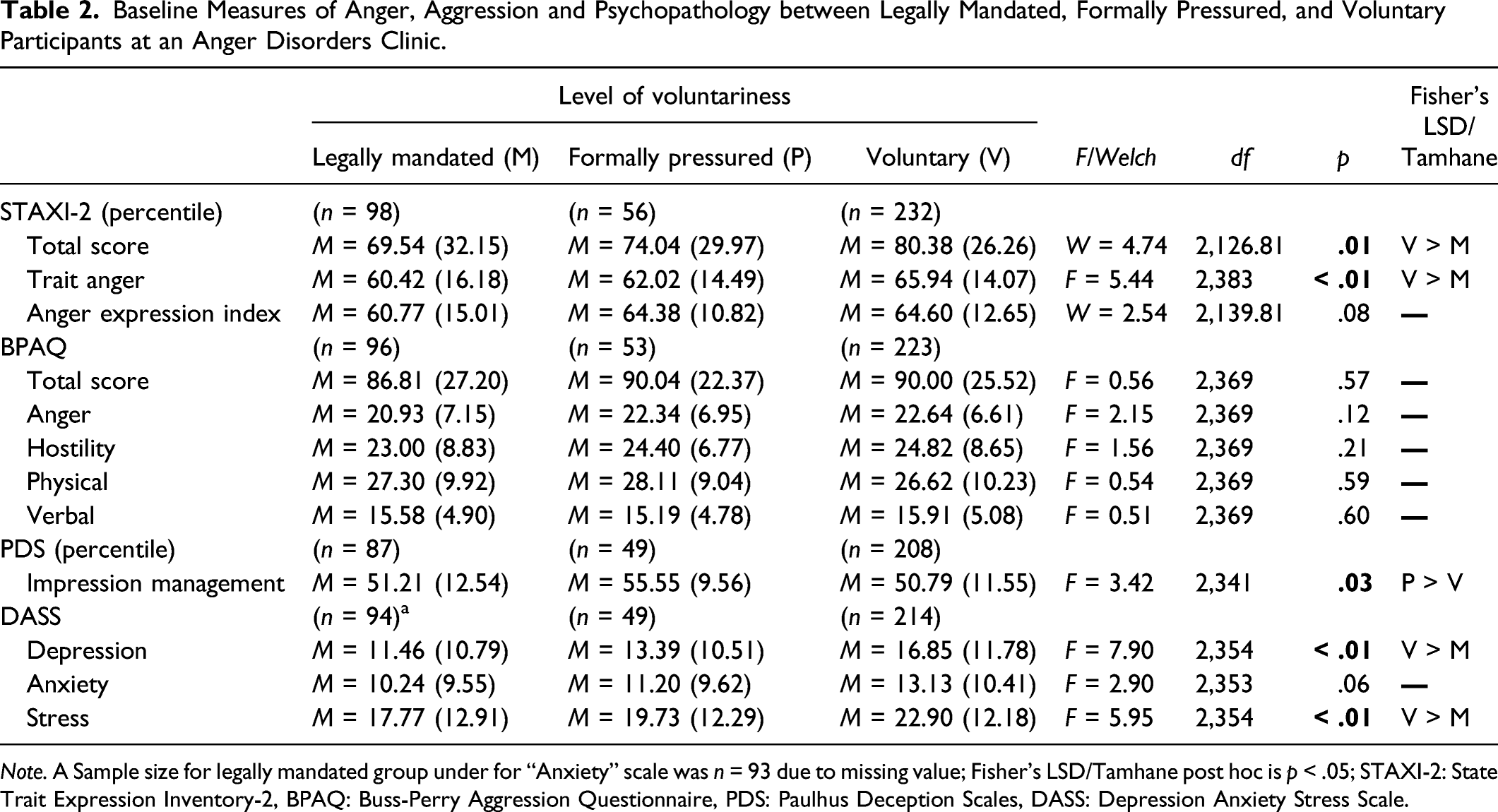
Note. A Sample size for legally mandated group under for “Anxiety” scale was n = 93 due to missing value; Fisher’s LSD/Tamhane post hoc is p < .05; STAXI-2: State Trait Expression Inventory-2, BPAQ: Buss-Perry Aggression Questionnaire, PDS: Paulhus Deception Scales, DASS: Depression Anxiety Stress Scale.
Level of Voluntariness on Treatment Recommendation, Refusal, and Success
The first block predictors included age, gender, whether one had a lifetime primary mood, and/or substance use disorder and STAXI-2 total score. Impression management was not selected as a predictor because all groups were within a single standard deviation of each other, were within the “average” range, and this variable had 15% missing data. Missingness on impression management was not statistically related to any of the other covariates, or to treatment refusal or completion, but was statistically related to treatment recommendation (p = .024), as those with missing data were less likely to be referred to treatment. Including impression management would have substantially reduced the power within each analysis, so sensitivity analyses were conducted to assess its impact on overall model results. All models were found to meet the assumptions for multicollinearity (as indicated by Tolerance and VIF statistics) and linearity.
Anger Treatment Recommendation
Binary Logistic Regression Examining the Effect of Voluntariness on Anger Treatment Recommendation.

Anger Treatment Refusal
Binary Logistic Regression Examining the Effect of Voluntariness on Treatment Refusal.

Anger Treatment Completion
Binary Logistic Regression Examining the Effect of Voluntariness on Treatment Completion.

Sensitivity Analyses with Impression Management
Sensitivity analyses were conducted including impression management as a predictor in the three previous binary regression analyses to assess the impact on the results. In both the treatment referral (Table 3) and treatment completion (Table 5) analyses, the inclusion of impression management did not impact the results. There was little change in the effect sizes across variables and impression management itself was non-significant. In the sensitivity analysis on the treatment refusers outcome, impression management was significant in the final model (OR = .947, p < .01). Trait anger was no longer significant, but the effect size remained stable (OR = 1.01, p = .23); the direction of the effect remained the same for referral status, though legally mandated referral became non-significant (OR = 1.54, p = .29) and formally pressured became significant (OR = 3.32, p < .05). Given that inclusion of impression management in the sensitivity analyses resulted in a reduction of power, effect sizes are most important to consider rather than statistical significance levels. Effect sizes remained in the same direction, and for the most part remained very consistent with the main analyses, which provides further justification for excluding impression management from the main set of analyses.
Discussion
Legally mandated, formally pressured, and voluntary participants statistically differed on several sociodemographic and psychiatric characteristics, including baseline measures of psychopathology. As predicted, legally mandated participants differed from other participants by being younger, male, with less education, and more involvement in substance use. Though formally pressured participants showed few statistical differences from the other groups, they did present with a distinctive profile, with most of the group mean scores on measures of anger and psychopathology falling between those of the legally mandated and voluntary participants (Klag et al., 2005; Parhar et al., 2008; Prendergast et al., 2002). As anticipated, voluntary participants presented with a more serious clinical profile, in that they had the greatest proportion of previous inpatient or outpatient psychiatric treatment, and scored higher on self-report measures of anger, depression, and stress.
We inferred that distress or impairment motivated voluntary participants to seek help at the clinic; however, participants were not directly asked about their motivations for treatment (or lack thereof). Though none of the three groups demonstrated elevated scores beyond “average” on Impression Management, correlation analyses suggest that there was a negative relationship with total self-reported anger scores. However, given that this was present across the entire sample to some degree, the pattern is consistent with our hypothesis that many legally mandated participants are referred to the anger clinic not because they are experiencing frequent, intense, or chronic problems with anger, but because their criminal charges involved aggression and the referrer thought that anger treatment could reduce the likelihood of future aggression. Similarly, widely reported poor treatment effects in the intimate partner violence treatment literature are suggested to be the result of treatment approaches that do not consider different offending patterns (e.g., only violent with partner and not in other situations) and individual needs (Butters et al., 2020).
As predicted, level of voluntariness was not associated with the decision to recommend treatment or not. Indeed, the only significant predictor of treatment recommendation was total anger score. Unexpectedly, legally mandated participants were more rather than less likely to refuse treatment, suggesting the legal mandate was not sufficient to compel accepting the recommendation. Non-adherence with legal conditions is very common, for instance, the successful completion of community supervision in offenders in the United States has been reported to be as low as 59% (Glaze & Bonczar, 2006). It must also be considered that legally mandated participants may have faced unique barriers to attend and complete treatment, including limited access to transportation and support (Bunting et al., 2018). Likewise, we do not know if non-attendance was the result of other external factors such as a new hospitalization or new arrest that prevented the person from attending, even if they wished to. It is not known what if any consequences were faced by legally mandated (or formally pressured) participants who refused treatment, but this study suggests the legal mandate itself is not sufficient, without additional motivation, incentive, or support—and removal of systemic barriers—to participate in treatment.
Finally, level of voluntariness was not associated with treatment completion, unlike previous research showing that legally mandated participants are more likely than voluntary participants to complete treatment (Jewell & Wormith, 2010). It is unclear why this was the case, but we did note that a large minority of the treatment participants did not complete 10 or more sessions, suggesting completion was a challenge across levels of voluntariness. However, this high attrition rate is not unique to this program. Attrition rates for CBT-informed anger management programs range from 22 to 71.7% (Henwood et al., 2015). One clinical implication of this finding is that motivational engagement or enhancement could be helpful in increasing treatment participation and thus completion.
An interesting secondary finding from this study was that formal psychiatric diagnoses were uncommon except for substance use disorders, which were found for almost half (46%) of the sample. This reflects the prominence of substance use problems in this sample and may also reflect an association between substance use and the only anger-related psychiatric diagnosis in the DSM-5, Intermittent Explosive Disorder (Coccaro et al., 2017). It may also reflect the absence of other anger-related diagnoses, as we would expect a substantial proportion of at least voluntary participants to show dysfunctional anger. As we noted in the Introduction, Intermittent Explosive Disorder requires recurrent, intense episodes of verbal or physical aggression, and so does not capture individuals with dysfunctional anger who are not aggressive or express their anger in passive-aggressive ways.
Limitations
There are some important limitations that must be considered in interpreting these findings. First, the results of our sample might not generalize to other anger clinic samples or to samples comprising more women. Though the ethnic makeup of the sample was representative of the national population (Statistics Canada, 2017), it might not be representative of other anger treatment programs, particularly those offered in the criminal justice system given persons of color are overrepresented in that system. Most of the sample (80%) were men, which is notably different from the general population. Moreover, a previous study found that women who were referred for an anger assessment scored much higher in anger than men, despite being similar in terms of aggression (Healey et al., 2019). Results of this study might have differed if the sample was more gender-balanced or was comprised primarily of women. Another demographic characteristic to consider is age, as all participants were adults and results might be different for youth who are referred to an anger clinic at different levels of voluntariness. An interesting additional consideration for youth is parent/guardian influence, where the youth may not be interested in anger assessment or treatment but is compelled by their parent or guardian.
Second, the data for this study were clinical and retrospective, which means it suffers from various amounts of missing data. In addition, despite reporting average levels, the correlations suggest that socially desirable responding may have been an issue across the entire sample, though formally pressured and legally mandated groups had stronger effects. The individual clinical interviews were designed to complement these baseline measures, but it does not eliminate the risk for impression management.
Related to this limitation, referral source is not always indicative of motivation to participate in anger treatment. A “voluntary” participant may have presented as such but still be under pressure from another person, such as a spouse, but did not disclose that pressure during their intake assessment. Similarly, a “legally mandated” participant may also recognize they have dysfunctional anger and therefore be intrinsically motivated to receive treatment. This is demonstrated in Wild et al., 2016 study of substance use treatment, where a third of the legally mandated participants felt no perceived coercion upon treatment entry.
Our voluntary group combined people who sought help on their own and those who were encouraged by a partner, family, or friends. Though there was no external pressure in the form of employment or legal repercussions, coming to the clinic because one’s partner or family threatened separation is not entirely voluntary. The formally pressured group constituted a wide range of referrals, which in turn varied in levels of coercion. We were unable to tease apart the formally pressured group further to reflect this, though the inclusion of a middle group at all between voluntary and legally mandated is an innovation in this area of research.
Though our three voluntariness groups were heterogeneous, the distinction was nonetheless useful given there were meaningful differences between them in terms of participant characteristics and treatment participation. Limitations in how we defined voluntariness and classified participants could be addressed by asking participants to rate their perceived level of voluntariness and rating referrals by level of voluntariness, to see if they individually or jointly help explain variation in treatment participation, refusal, completion, and ultimately outcomes.
One of the limitations of our treatment completion variable is the selection of 10 sessions as the criterion for “completion.” Though research suggests that a majority of participants would show treatment gains by 10 sessions (e.g., Glancy & Saini, 2005; Howard et al., 1986), individual pace varies, and some participants may have made little or no gains by 10 sessions. Also, group therapy entry was rolling, so many participants might have joined in the last few sessions of one group and then completed additional sessions in the next group. Their experience of group therapy would be different from someone who began therapy with a group and attended at least 10 sessions with mostly the same group members. Similarly, the experience of someone who attends 10 sessions consecutively could be quite different from someone who attended 10 sessions sporadically, but our criterion did not distinguish attendance sequence. This study would have been strengthened if completion was based on reaching a clinical target or pre-post change on anger and related measures. This analysis was not possible because only 60% of individuals who attended at least 10 sessions had post-treatment scores, most likely due to absenteeism on the last session of a group or due to participation in individual therapy where post-measures were inconsistently administered. More consistent post-treatment data collection would address this issue.
Implications for Practice
We found that legally mandated anger treatment participants did not show elevated anger scores compared to the other two groups. Moreover, the most common diagnosis was substance use disorder, with almost half (46%) meeting criteria for one or more substance use disorders. The second most common diagnosis was personality disorder (19%). These results suggest that many legally mandated participants at this clinic are being referred to anger treatment not because they have problems with dysfunctional anger but because they have engaged in violent or aggressive behavior. Given the robust relationship between substance use and risk of aggression and violence (Boles & Miotto, 2003), substance use may have been a more prominent antecedent for prior aggressive behavior than dysfunctional anger in some participants. Anger treatment to reduce future aggression is not warranted for someone who does not have dysfunctional anger (Novaco, 2013, p. 215). Instead, other treatment may be more helpful in reducing future violence or aggression, such as substance use treatment if substance use is a problem and associated with violence or aggression (e.g., getting into bar fights while intoxicated).
Another important implication is that mandating treatment is no guarantee that the person will actually participate in treatment, given the legally mandated participants were more rather than less likely to refuse treatment and did not differ in the likelihood of completing at least 10 sessions. We did not have data to test our hypothesis that legally mandated participants were willing to refuse or drop out of treatment because there were no or weak consequences for not following through on the mandate. This result suggests the importance of future research looking at motivational enhancement and incentives for treatment participation in relation to outcomes.
Last, it is important to point out that this study was not an evaluation of an outpatient anger treatment program. We did not compare treatment participants to others through study designs that allow some inference about treatment efficacy, such as a randomized clinical trial, wait-list control, or matched comparison analysis. We also did not have recidivism or other follow-up data and so could not relate clinical scores and pre-post change to behavioral outcomes. Our interest in this study was distinguishing treatment participants by level of voluntariness, introducing a third group between voluntary and legally mandated participants.
Future Directions
The results of this study, along with Parhar et al. (2008), suggest several directions for future research. The first is that we categorized clinic referrals into voluntariness groups, collapsing across potentially meaningful differences in coercion. For example, being told that assessment and possibly treatment are required to have custody or access to one’s children may be perceived as higher stakes than being told to do the same by a workplace, when someone is not particularly happy about the job or are confident they can find another job easily. Future research could rate participants on a continuum of voluntariness, and examine how these ratings are correlated with clinical outcomes. Another avenue is to ask participants to rate their own perceived level of coercion (e.g., Wild et al., 2016), and see how perceived coercion relates to outcomes and to researcher ratings based on referral information.
Another direction for further work is to attempt to obtain collateral information about anger as well as other psychological problems. As noted earlier, one of the possible explanations for why legally mandated participants did not report particularly high levels of anger or mood problems is that they were minimizing the extent of their concerns because of the mandate, whereas the voluntary participants felt no pressure to respond in a socially desirable way. This could be examined by examining the association between voluntariness and anger with other sources of information, such as ratings of anger by people close to the participant.
There is plenty of evidence that attrition from offender treatment is associated with negative long-term outcomes such as recidivism (Henwood et al., 2015; Olver et al., 2011). Future research could follow the clinic participants, whether treatment was completed or not, to examine reoffending, and whether treatment dosage is associated with better outcomes. This is especially important considering that this study demonstrated that attrition is common, even with legally mandated participants who were recommended for treatment.
Finally, we were originally interested in whether level of coercion was specifically related to pre-post change in anger. This analysis was not possible due to the amount of missing data. Though clinical need and flexibility are important in the field, inconsistency in admission to groups, attendance, and inflexibility in when post-assessments were conducted precluded us from examining the relationship between level of mandate and pre-post change. Improving uptake for post-measures (e.g., mailing them out if the participant misses the final group) is an area for future development.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by: University Medical Research Fund (University of Ottawa Institute of Mental Health Research).