
Abstract
There is a robust and growing literature base indicating that spanking is a common, but potentially problematic, discipline strategy.
Spanking is widely used as a discipline strategy in the United States. Investigators have found that 80–94% of parents with a 3- to -year-old report that they have spanked their child at least once (Gershoff et al., 2012; Straus & Stewart, 1999). Evidence compiled through decades of research indicates that spanking is associated with a subsequent increase in childhood aggression, greater risk of parental escalation to physical abuse, higher rates of substance use, anger, and marital conflict in adulthood, and other adverse outcomes (Afifi et al., 2017; Gershoff, 2002; Gershoff et al., 2018; Gershoff & Grogan-Kaylor, 2016; Lee et al., 2014; Grogan-Kaylor et al., 2018). Given the associated risks and prevalence of spanking, professional organizations such as the American Academy of Pediatrics, the Canadian Paediatric Society, and, most recently, the American Psychological Association have published statements indicating that physical punishment is not a recommended discipline strategy (American Academy of Pediatrics, Committee on Psychosocial Aspects of Child and Family Health, 1998, American Psychological Association, Committee on Children, Youth and Families, 2019, Canadian Paediatric Society, 2004). Moreover, although the United States has not ratified the treaty, the UN Convention on the Rights of a Child (McGoldrick, 1991) condemns the use of physical punishment.
Studies have identified characteristics of parents, children, and the family environment that are associated with the likelihood of using spanking. Regarding child characteristics, more children are spanked at ages four and five than any other age group, and rates of spanking decline with children’s age (Straus & Stewart, 1999). Studies have also consistently found that boys are more likely to be spanked than girls, at any age (Giles-Sims et al., 1995). With regard to parenting factors, mothers spank more frequently than do fathers (Wolfner & Gelles, 1993); however, this disparity might be due to mothers having more contact with children (Dietz, 2000; Straus & Donnelly, 1993). Other caregiver factors associated with a greater use of spanking include elevated frustration and poor emotional well-being (Regalado et al., 2004), lower income, lower overall socioeconomic status, and being an unmarried mother (Giles-Sims et al., 1995). A family’s racial/ethnic background is also related to reported use of spanking. Black mothers report spanking significantly more frequently than mothers in other racial groups, and some studies indicate that Hispanic mothers spank slightly more than do White and Asian parents (Gershoff et al., 2012; Regalado et al., 2004). Given these factors, some researchers have suggested that the associations between spanking and being a single parent, African American, and/or impoverished may indicate an underlying “stress theory.” In other words, experiences like discrimination and restricted economic opportunity present added stress to the inherently demanding role of being a parent, so higher rates of spanking among parents in these groups may be explained by the increased stress often associated with these experiences (Giles-Sims et al., 1995).
Given the negative outcomes associated with spanking, recent research has focused on evaluating interventions aimed at educating parents about more effective discipline strategies. Relatively intensive interventions (e.g., The Incredible Years, Parent-Child Interaction Therapy) that teach effective discipline techniques as alternatives to the use of corporal punishment have been shown to successfully reduce the likelihood of child maltreatment in high-risk families (Damashek & Chaffin, 2012). However, interventions such as these are time-intensive and only accessed by a small proportion of families, most of whom have a child with significant behavior problems or are considered at risk for maltreatment. Spanking is prevalent across family circumstances, so briefer, more universally accessible interventions are needed to reach a broader range of the population who may benefit from education on recommended discipline strategies.
Literature on interventions that specifically target spanking in caregivers is relatively sparse. Some research has found that the provision of brief summaries of research literature about the impacts of spanking on children resulted in decreased favorable attitudes toward spanking (ATS) among caregivers (Holden et al., 2014). Additionally, some researchers have successfully used Motivational Interviewing techniques during an educational intervention to decrease caregivers’ favorable ATS (Holland & Holden, 2016). Another study found that provision of educational baby books (books that mothers would read to their babies) about effective discipline strategies for mothers of infants reduced favorable attitudes toward spanking, particularly for African American mothers and those with lower levels of education (Reich et al., 2012). Research with conservative Christian college students (who were not parents) found that a combination of the presentation of research literature and progressive Biblical interpretations about spanking was more effective than providing information about research alone (Miller-Perrin & Perrin, 2017); however, as noted, these participants were not caregivers.
Several recent studies have also examined whether the interactive portion of a brief online parenting education program called Play Nicely can change caregivers’ attitudes toward spanking. Pediatric primary care settings have been targeted as research sites for these studies because they are frequented by families with varied parenting expertise and many parents seek discipline advice from pediatricians (Taylor et al., 2012). Play Nicely is a publicly available intervention that was originally designed to teach parents how to effectively manage childhood aggression by explaining why some discipline strategies (such as spanking) are not recommended and providing information on evidence-based alternative strategies (Scholer & Goad, 2003). Play Nicely is an attractive intervention for disseminating discipline recommendations because it is brief, free, engaging, easily accessible, and no training is required to administer or use it. Researchers have hypothesized that Play Nicely’s educational information about the problematic consequences associated with spanking, in combination with offering alternative discipline options via a nonjudgmental approach, may lead caregivers to question the utility of spanking.
One study that has evaluated Play Nicely’s influence on attitudes toward spanking, conducted by Chavis et al. (2013), recruited a sample of parents of 0.5- to 2-year-old children from a pediatric primary care clinic. Parents were randomly assigned to treatment or control conditions, such that control participants experienced a typical primary care appointment and treatment group participants were exposed to Play Nicely as “part of the clinic visit” (Chavis et al., 2013). Treatment group participants were instructed to engage with Play Nicely for 5–10 minutes. All participants (n = 258) were asked to complete the Attitude Toward Spanking (ATS; Holden et al., 1995) survey immediately following their clinic visit, and the treatment and control groups’ median scores were compared. Scores indicated that, following the intervention, the treatment group had significantly less favorable ATS than the control group. These findings are promising, given that research has indicated that ATS are significantly correlated with subsequent use of spanking (Vittrup et al., 2006). However, the study’s conclusions are limited by the narrow age criterion, brevity of exposure to the intervention, and lack of follow-up data. Additionally, because pre-test ATS scores were not collected, this finding may be confounded by a baseline difference between the treatment and control groups’ attitudes toward spanking.
An additional study conducted by Scholer et al. (2010) employed a randomized controlled trial design to evaluate the effects of Play Nicely on a sample of parents with a child younger than age 7, recruited from both a pediatric primary care clinic and a preschool. Parents in this study (n = 96) were randomized to the treatment or control condition, asked to complete the ATS survey at baseline, and those in the treatment group were instructed to view at least eight of the interactive options presented in the Play Nicely program (i.e., length of exposure to the intervention ranged from 8-20 minutes). Between 1 and8 months after intervention, a portion of the participants (66.6%) completed the ATS survey again over the telephone. The authors did not find a significant difference in post-test ATS scores between the treatment and control groups, but there was a significant decrease in favorable ATS from pre-to post-test within the treatment group (Scholer et al., 2010). Additionally, treatment group participants were surveyed immediately after the intervention about whether they planned to change anything about their parenting; about 89% of participants who viewed Play Nicely indicated plans to change how they respond to their child’s behavior, and 22% specifically indicated intention to spank less (Scholer et al., 2010). Some limitations of this study are that immediate intervention effects were not measured, and the timeframe for post-test data collection varied broadly across the sample. Overall, the design of this study provides more conclusive results, but less robust support for Play Nicely’s impact on parents’ attitudes toward spanking, given that a between-groups difference was not detected.
Existing research on Play Nicely has not adequately attended to cultural differences in attitudes toward spanking. To this author’s knowledge, one study has focused on this issue. Play Nicely was presented to an ethnically-diverse sample of parents (n = 197), and their perceptions of the program’s cultural sensitivity were compared (Smith et al., 2017). The authors concluded that parents across racial groups reported that Play Nicely “addressed their family needs” and “respected their family values and personal beliefs,” but this study did not evaluate the sample’s attitudes toward spanking. Additional research is needed to address previous studies’ limitations, including the degree of exposure to the intervention, rigor of methods employed, and exploration of the influence of relevant sociocultural factors (e.g., income level or racial/ethnic identity), in order to clarify Play Nicely’s impact on parents’ attitudes toward spanking.
Summary and Study Goals
The pervasiveness and negative outcomes associated with spanking call for an intervention that specifically targets this problem. Play Nicely shows promise for fulfilling this need due to its ease of dissemination and preliminary research findings that support its ability to decrease parents’ favorable attitudes toward spanking. However, there are some limitations to the current literature on Play Nicely. In addition, given that reported use of spanking is especially high among African American families, it is important to examine whether Play Nicely is equally effective for parents across racial groups.
The goals of the current pilot study were to use a randomized controlled trial design to 1) rigorously test the effects of the Play Nicely program on attitudes toward spanking, specifically among low-income caregivers of young children (ages 1–5); 2) compare changes in ATS between White caregivers and caregivers of color; and 3) assess for a difference in caregivers’ perceptions of Play Nicely’s cultural acceptability between White participants and POC. This project served as a pilot study of the intervention with this low-income, racially diverse sample.
In an effort to clarify Play Nicely’s impact on attitudes toward spanking, this study included the collection of pre-test and immediate post-test data, a more significant exposure to the intervention than previous studies, and the examination of a variable that may impact participants’ treatment response (i.e., perception of the program’s cultural sensitivity). We hypothesized that, consistent with the outcomes presented by Scholer et al. (2010), favorable ATS would be lower for the treatment group than the control group at post-test. Analyses comparing changes in ATS and perceptions of Play Nicely’s cultural sensitivity between White participants and POC were exploratory.
Methods
Participants
Sample Demographic Characteristics Reported at Baseline.

aResponse not provided by two participants (3.8%).
bResponse not provided by five participants (9.6%).
Procedures
Subject recruitment and participation took place at a university-affiliated pediatric primary care clinic that provides services to a high volume of low-income and racially/ethnically-diverse patients. Approximately 80% of this clinic’s patients are insured through Medicaid. Given the ubiquity of parental use of corporal punishment (Gershoff et al., 2012), recruitment was open to any caregiver who brought their child to the clinic, regardless of the reason for their appointment (i.e., well child visit or sick child) and regardless of whether they were seeking information about discipline techniques. Upon checking in for their child’s physician appointment, caregivers were given a flyer describing the study and explaining that study participation could occur directly after their child’s appointment or at a later date if preferred. If interested, caregivers provided their contact information on the flyer and returned it to a research assistant (RA) in the waiting room. At the end of their child’s appointment, these individuals were intercepted in the clinic’s waiting area and led to an examination room (reserved for research activities) where they provided written informed consent and verbally confirmed their eligibility. A total of eight individuals (out of 117) were determined to be ineligible for the study. In the event that a caregiver was interested in participating but unable to do so on the same day as their child’s doctor appointment, they were scheduled to return to the clinic to participate on a subsequent day. Of the 117 individuals who indicated interest, 65 people did not participate and the remaining 52 people were enrolled in the study. See Figure 1 for participant flow. Participant flow.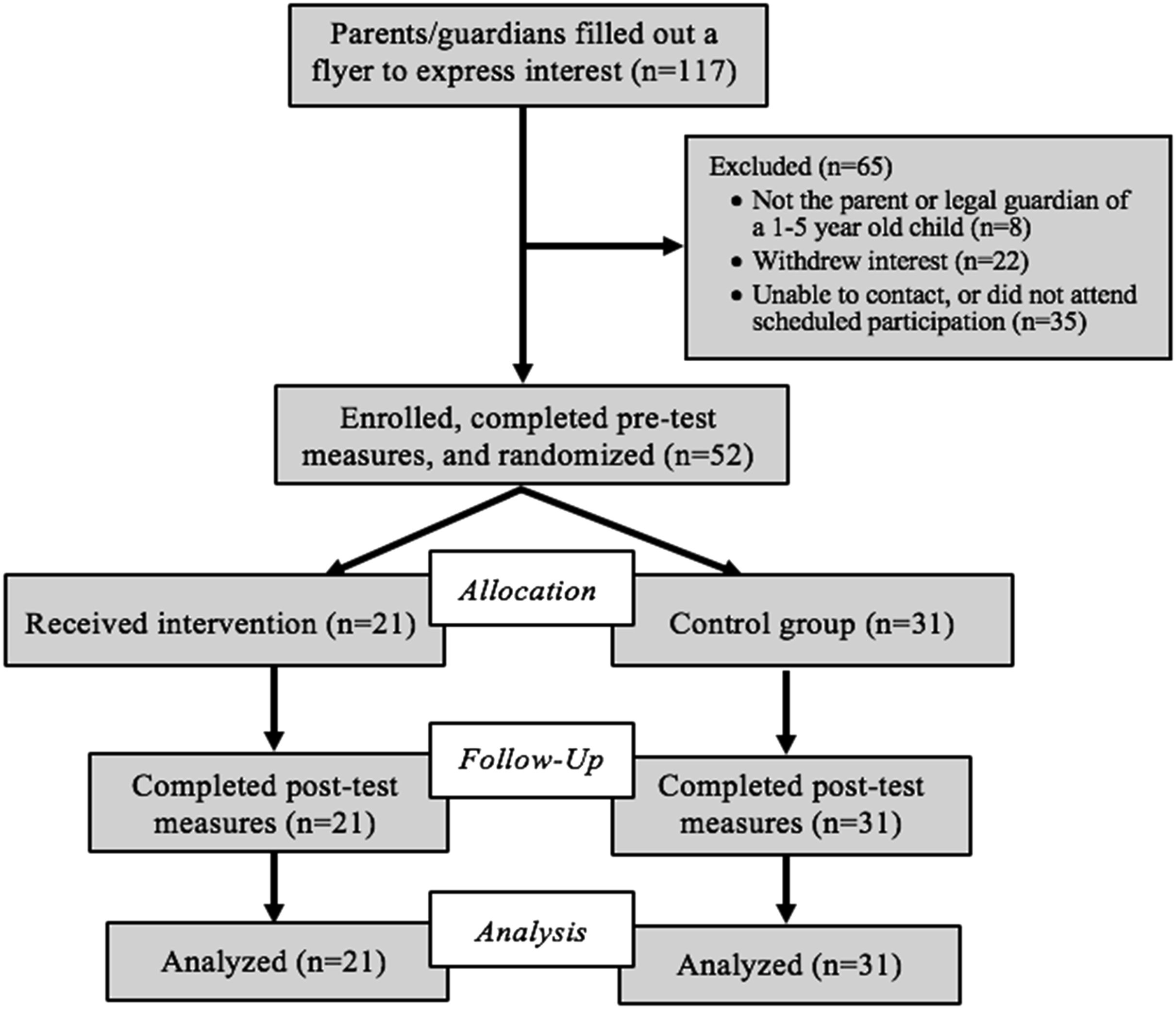
Once enrolled, each participant completed a demographic questionnaire. An RA then provided instructions for the pre-test Attitude Toward Spanking survey (Holden et al., 1995) and left the room while it was completed so as to reduce response bias. During this time, the participant was randomly assigned to either the treatment or control condition. Group assignment was determined through a stratified randomization procedure using two randomly generated lists of 0’s and 1’s. One randomization list was for participants who selected “White” for the race/ethnicity item on the demographic measure, and the other randomization list was for participants who selected any race/ethnicity other than “White.” The purpose of stratifying the randomization process was to increase the likelihood that the treatment and control groups were equally racially diverse.
Intervention
Participants were given a laptop displaying the website associated with the condition to which they were assigned. An RA delivered verbal instructions for the appropriate condition, provided a physical copy of the relevant instructions, and left the room while the participant completed intervention procedures.
Treatment Group
Participants randomly assigned to the treatment group engaged in the Play Nicely intervention. Consistent with previous studies, participants in the present sample engaged in the portion of Play Nicely that describes a hypothetical scenario in which their child hits another child. The user is shown 20 options for responding to the situation (e.g., say “no,” time-out, give a warning, take away a privilege). Upon selecting an option, the user is told if they chose “a great option,” “a good option after others have failed,” or if “there are better options,” through an approximately 1-minute long explanation as to why each response is effective or ineffective. Participants were asked to select and read/listen to the explanation of all 10 options in the left column of the menu, to ensure that they were exposed to the information about spanking, and any six of the options in the right column of the menu. This resulted in viewing 16 options total, which took approximately 20 minutes.
Control group
Participants in the control group were instructed to view a website about child safety for 20 minutes. This website includes 21 categories of safety information for kids ages 1–4. Users can click on each of these categories to read tips about various safety recommendations (e.g., choking prevention, fire safety, playground safety, sports safety) for young children. Participants in this group were asked to read the information from as many categories as possible within 20 minutes.
Immediately after a participant finished using either the Play Nicely program or the child safety website for 20 minutes, they completed an adapted version of the Multicultural Therapy Competency Inventory (MTCI) measure to assess their perception of the intervention’s cultural sensitivity. Participants then repeated the Attitude Toward Spanking (ATS) questionnaire as a post-test measure. Participants were given a $20 gift card for completing the study.
Measures
Demographics
Participants completed a questionnaire on socio-demographic characteristics at pre-test.
Attitude Toward Spanking
The ATS survey uses a 7-point Likert scale to measure the extent to which participants agree or disagree with 10 statements about spanking (Holden et al., 1995; Holden & Zambarano, 1992). Each item is scored on a scale of 1–7 points, where 1 indicates strong agreement and 7 indicates strong disagreement. Four items are reverse-scored, then the points for each item are summed to produce a total score with a possible range of 10–70 (Vittrup et al., 2006). High scores indicate more positive attitudes toward spanking, while low scores indicate less approval of spanking. This measure has high internal reliability (ranging from .88 to .90) and test-retest reliability over a 2-week period (r = .76; Holden et al., 1995). Moreover, parents’ scores on this measure have been found to be significantly correlated with their subsequent spanking behavior (Vittrup et al., 2006). Participants completed this measure at pre- and post-test.
Multicultural Therapy Competency Inventory
The MTCI is a 32-item instrument used to assess clients’ perceptions of their therapists’ cultural competence. Each item is answered by checking a box in one of three columns labeled “does this very well,” “does this adequately,” or “does this poorly,” which are scored as 2, 1, and 0, respectively. Research indicates that the MTCI is reliable and valid, and predicts client satisfaction with treatment (Cole et al., 2014). For the present study, relevant items were adapted to refer to an “online training” rather than a therapist (e.g., “The training explains things in a way that demonstrates familiarity with my family’s culture.”), resulting in a 15-item adapted measure with a possible score range of 0–30. Higher scores indicate more positive perceptions of an intervention’s cultural sensitivity. Participants completed this measure at post-test.
Analysis Plan
Preliminary analyses employed chi-square tests and independent samples t-tests to examine whether there were differences between the treatment and control groups on demographic characteristics or baseline ATS scores. Bivariate analyses were also conducted to examine the relations between pre-test ATS scores and demographic variables. Boxplot representations of the treatment group identified two extreme values among ATS pre–post change scores; these two participants’ scores were not included in analyses of the treatment group’s ATS change scores. Shapiro–Wilk tests of normality indicated that scores on all measures were normally distributed across groups, so parametric tests were used. Due to sample limitations, subgroup comparisons of racial/ethnic outcomes were conducted using two groups: all participants who did not identify as White (i.e., the “participants of color” (POC) group) and White participants.
To examine the first study goal, a one-way ANCOVA was used to compare the treatment and control groups’ post-test ATS scores. For the second study goal, paired samples t-tests were used to examine changes in ATS scores for White participants and for POC within the treatment group only. In addition, an independent samples t-test was used to assess for a difference in the pre-to post-test change scores in ATS between the treatment group’s White participants and POC. Finally, for the third study goal, an independent samples t-test was used to assess for a difference in perceptions of the intervention’s cultural sensitivity between White participants and POC in the treatment group.
Results
Descriptive statistics
Attitudes toward spanking
For the present study, mean ATS scores at baseline were 29.70 for the control group (SD = 12.16) and 28.14 for the treatment group (SD = 12.32), with a possible score range of 10–70 points. Thus, baseline ATS scores were on the low end of the possible range, indicating a moderately low endorsement of favorable ATS among the overall sample.
Perceptions of the intervention’s cultural sensitivity
The MTCI mean score for the treatment group was 23.17 (SD = 5.53) out of a possible 30 points. This mean score falls in the high end of the range, demonstrating an overall positive perception of Play Nicely’s cultural appropriateness.
Preliminary analyses
There were no statistically significant baseline differences between treatment (n = 21) and control (n = 31) groups in terms of pre-test ATS scores (t (50) = −0.45, p = 0.66), participant race (χ(4) = 3.52, p = 0.48), age (χ(20) = 12.91, p = 0.88), marital status (χ(4) = 4.49, p = 0.34), education level (χ(4) = 2.35, p = 0.67), or household income (χ(11) = 7.16, p = 0.79). Similarly, no statistically significant baseline differences were detected between POC and White participants on demographic variables within the treatment group. See Table 1 for a summary of overall sample demographics, as well as demographic breakdowns for treatment and control groups.
One-way ANOVAs indicated that there were no significant relationships between ATS pre-test scores and participants’ marital status (F (4, 47) = 1.65, p = 0.18), race (F (4, 47) = 1.10, p = 0.37), education level (F (4, 47) = 0.45, p = 0.77), or gross annual household income (F (11, 40) = 0.70, p = 0.73). Pearson product-moment correlations did not identify significant relationships between ATS pre-test scores and participant age (r = −0.12, p = 0.41) or number of children in the home (r = −0.06, p = 0.68). Similarly, a point-biserial correlation indicated that there was not a significant relationship between ATS pre-test scores and participant gender (rpb = 0.13, p = 0.34).
Comparing Treatment and Control Groups’ Post-Intervention Attitudes Toward Spanking
Group and subgroup means (and standard deviations) on ATS and MTCI measures.
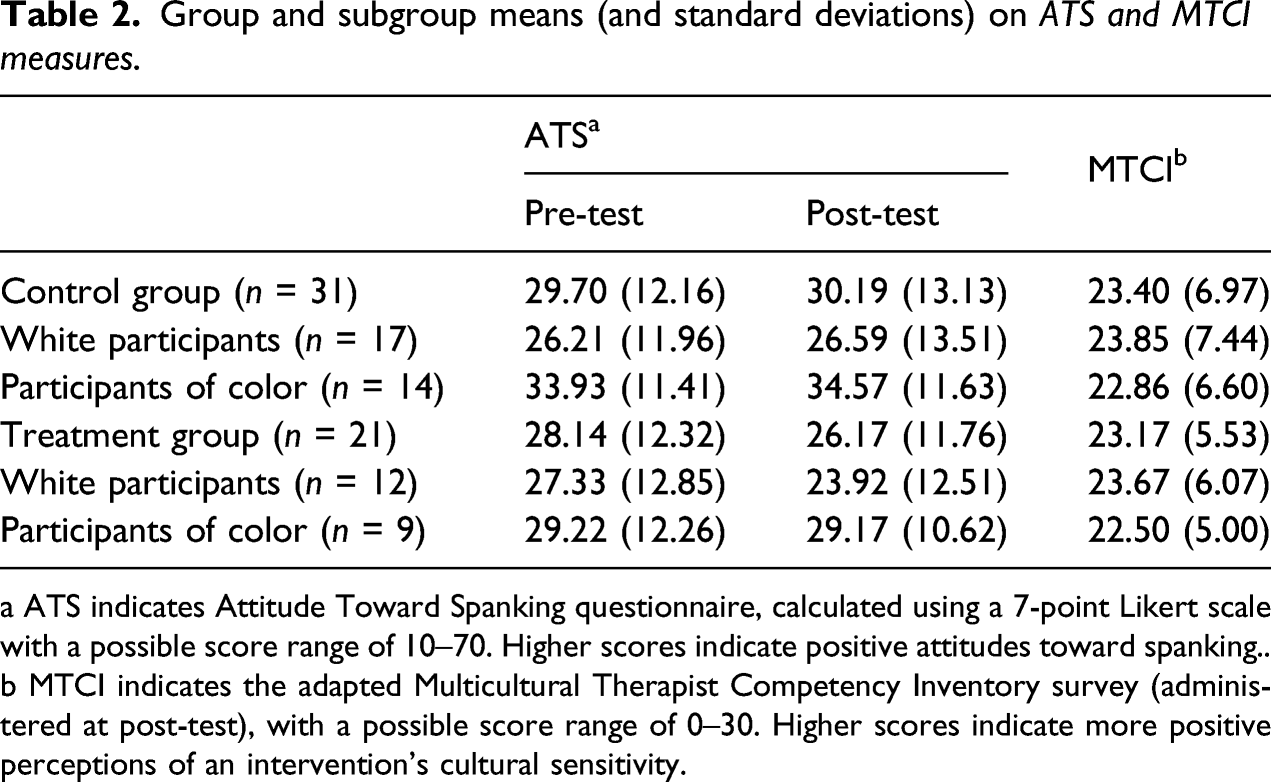
a ATS indicates Attitude Toward Spanking questionnaire, calculated using a 7-point Likert scale with a possible score range of 10–70. Higher scores indicate positive attitudes toward spanking..
b MTCI indicates the adapted Multicultural Therapist Competency Inventory survey (administered at post-test), with a possible score range of 0–30. Higher scores indicate more positive perceptions of an intervention’s cultural sensitivity.
Comparing Changes in Attitudes Toward Spanking Between White Participants and Participants of Color
Within the treatment group, the mean ATS score for White participants (n = 12) decreased by 3.42 points from baseline (M = 27.33, SD = 12.85) to post-intervention (M = 23.92, SD = 12.51), whereas the mean ATS score for POC (n = 9) decreased by only 0.05 points from baseline (M = 29.22, SD = 12.26) to post-intervention (M = 29.17, SD = 10.62). Paired samples t-tests showed that ATS scores did not significantly change from pre-to post-test among White participants (t (11) = 1.786, p = 0.102) or POC (t (8) = 0.010, p = 0.992). However, a significant difference was detected in ATS change scores between White participants and POC in the treatment group (t (17) = −2.125, p = 0.049). Thus, while neither subgroup’s ATS scores reflect a statistically significant change from pre-to post-test, White participants’ favorable ATS decreased significantly more after engaging with Play Nicely than did the attitudes of POC.
Comparing Perceptions of Play Nicely’s Cultural Sensitivity Between White Participants and Participants of Color
There was not a significant difference in MTCI scores between White participants (M = 23.67, SD = 6.07) and POC (M = 22.50, SD = 5.00) in the treatment group (t (19) = 0.469, p = 0.644), indicating that there was not a substantial discrepancy in perceptions of the cultural sensitivity of Play Nicely between POC and White participants in the treatment group.
Discussion
Previous studies have indicated preliminary support for using the brief, interactive Play Nicely program to decrease parents’ favorable attitudes toward spanking, but the limitations of these studies warranted further investigation. This randomized controlled trial aimed to: (1) replicate previous studies’ examinations of the impact of Play Nicely on ATS among caregivers of children aged 1–5 (with a specific focus on low-income families), (2) examine whether changes in ATS differed between White participants and POC in the treatment group, and (3) assess for a difference in perceptions of Play Nicely’s cultural sensitivity between White caregivers and caregivers of color.
Analyses indicated that, contrary to our primary hypothesis, ATS were not less favorable in the treatment group compared to the control group at post-test. This outcome is not consistent with findings reported in the existing literature, which may be explained by differences in study design. The study by Chavis et al. (2013) found a difference between the treatment and control groups’ ATS scores immediately following intervention, despite having participants view only four of the options presented by Play Nicely; the current study asked intervention participants to view 16 options and did not detect a difference between groups. This discrepancy may have occurred because the current study’s sample size provided insufficient power for detecting an existing treatment effect, whereas the study by Chavis et al. (2013) had a much larger sample (n = 258). Given that a small effect size was detected (d = 0.20), it is possible that a significant difference would have emerged between groups if this study had enrolled a larger sample. Another explanation may be the lack of baseline data collected in the previous study, as possible existing group differences could not be controlled.
Scholer et al. (2010) did not detect a difference between groups; however, the study did demonstrate a significant change in the treatment group’s ATS scores from pre-to post-test (between 1 and 8 months after intervention), which was not reflected in the current study. The pre-test scores in our study were similar to those in Scholer et al. (2010) indicating some similarity in our samples in terms of parental attitudes toward spanking; however, the amount of change from pre- to post-test that we observed was slightly smaller than in the study by Scholer et al. (2010). Scholer et al. (2010) reported a change of −2.7 points for the treatment group, whereas we observed a change of −1.97 points for the treatment group. Moreover, Scholer et al. (2010) included a larger sample size (n = 96) than the present study.
Another possible explanation for the present study’s nonsignificant outcomes may be that individuals’ ATS do not shift until they have a chance to employ alternative discipline strategies (such as those recommended by Play Nicely), so the immediate post-test scores may not capture Play Nicely’s effect on attitudes toward spanking. Alternatively, given the lengthy range of time during which post-test ATS scores were collected by Scholer et al. (2010), and in light of research showing that rates of spanking decline substantially with a child’s age (Straus & Stewart, 1999), it could be the case that their results reflected an effect that was at least partially inflated by the sample’s naturally occurring decrease in favorable ATS over time.
A novel finding presented by the current study is that favorable ATS declined significantly more among White caregivers than among POC in the treatment group. This finding is of particular interest given that participants in these subgroups reported statistically equivalent perceptions of Play Nicely’s cultural sensitivity, with mean scores indicating strong endorsement. Thus, while Play Nicely had a less substantial impact on ATS for POC, results indicate that this discrepancy is not explained by a perceived deficit in the program’s cultural competence. It is important to note, however, that due to the small sample size of this study, particularly when examining the treatment group only, this result should be considered preliminary. Studies with larger sample sizes should examine whether this finding is replicated. Moreover, further investigation is needed to identify factors that may moderate the effects of Play Nicely or other spanking interventions for families across racial and ethnic backgrounds.
This study has limitations that should be taken into consideration. As previously noted, interpretations of these findings are limited by the study’s small sample size. Results may not accurately reflect the effects of Play Nicely because analyses were not sufficiently powered. Moreover, the small sample size necessitated compiling participants who endorsed any racial/ethnic identity other than “White” into one subgroup for analyses (i.e., the “POC” subgroup), rather than examining outcomes across the distinct racial/ethnic identities represented in the sample. This study was conducted at one medical clinic, so the geographic generalizability of the results may also be limited. However, the sample did consist of a significant proportion of POC and represented lower than average income and education levels, which were desirable demographic characteristics for this study. Studies with significantly larger samples are needed to illuminate potential differences in outcomes among racial groups for POC.
In terms of methodological limitations, longitudinal data may be useful for capturing potential latent and/or sustained effects of Play Nicely, but this study only reported the program’s immediate effects on attitudes toward spanking. Additionally, potential selection bias could have impacted the study, as caregivers who use harsh discipline strategies may have been less likely to participate so as to avoid potential risks to disclosing this information (e.g., negative judgment from others or reports to child protective services). We attempted to recruit anyone who had an appointment at the clinic, but it is possible that those who were attending due to a specific child health concern were less likely to participate in the study than those who were attending for a well child visit. We did not collect data on the reasons for participants’ visits to the clinic. Finally, research in this area is complicated by practical barriers to obtaining an accurate, objective measurement of spanking frequency, and thus often rely on parents’ self-reported use of spanking or proxy measures such as attitudes toward spanking. While parents’ ATS are correlated with their subsequent use of spanking (Vittrup et al., 2006), the ATS measure does not provide data on the frequency of caregivers’ actual spanking behavior. Thus, future studies should explore more direct methods for ascertaining parents’ use of spanking.
Conclusions
While findings on the use and outcomes of spanking are complex, many experts suggest that other discipline strategies are equally effective and safer, and thus should be promoted in place of spanking (Gershoff et al., 2012, 2018; Graziano, 1989; Graziano et al., 1996). Spanking remains a very common practice, and a majority of parents cannot easily access existing interventions that provide empirically supported recommendations for discipline. Furthermore, in light of the known influence of socio-demographic factors on the use of spanking, cultural competence should be a primary focus of the development and evaluation of relevant interventions.
Programs like Play Nicely offer great promise in terms of ease of access and low-effort engagement. Exploring the potential applications of Play Nicely may advance the field’s understanding of novel approaches to broadly educating parents on effective child management strategies. To improve upon the existing literature base in this area, future research should pursue larger samples to further clarify Play Nicely’s effect on caregivers’ attitudes toward spanking, incorporate measures that can more directly indicate whether Play Nicely changes parents’ actual use of spanking, and explore cultural factors that may moderate the degree to which a parent will benefit from the Play Nicely program. From a public health perspective, the small effect size that was detected in this study may indicate that Play Nicely can produce desirable outcomes for a portion of the people who use it. Thus, despite the lack of significant findings in this study, further research on Play Nicely and comparable interventions should be conducted to identify and establish empirical support for an intervention for spanking reduction.
Footnotes
Acknowledgment
The authors thank Dr Seth J. Scholer for providing permission to evaluate the Play Nicely intervention and advice for project development. Thanks also to Dr Dilip Patel and Jessica Good for invaluable support throughout data collection. Results of this study were presented in an oral session at the Society for Advancement of Violence and Injury Research conference in Cincinnati, Ohio on April 2, 2019. This research was supported by grants from the Blue Cross and Blue Shield of Michigan Foundation (2476. SAP) and the Western Michigan University Graduate College.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was supported by grants from the Western Michigan University Graduate College and Blue Cross Blue Shield of Michigan Foundation.