
Abstract
Intimate partner violence, including physical, psychological, and sexual violence, affects over one-third of Americans and is particularly common among college students. Previous work has found links between rejection sensitivity and aggressive or hostile behavior (i.e., perpetration) in intimate relationships, but this construct has only been tested as a predictor of violence in an all-male sample. A related body of work has found relationships between self-silencing and rejection sensitivity, and between self-silencing and both hostile and ingratiating behavior. The purpose of this study was to bridge these related literatures and examine the relationship between rejection sensitivity and intimate partner violence experiences and the role of self-silencing as a possible mediator. To test these relationships, we collected survey data from a sample of college students (N = 410) at a large university in the northeast United States. Using mediation analyses, we found that rejection sensitivity predicted intimate partner violence victimization (i.e., being the target of violence) through self-silencing. Similarly, rejection sensitivity predicted intimate partner violence perpetration (i.e., being violent toward one’s partner) through self-silencing. Neither gender nor race significantly moderated either path of the models. Implications of this study include incorporating individual difference variables in intimate partner violence research and programming.
In 2017, the #MeToo Movement brought sexual and physical violence between intimate partners, also called intimate partner violence (IPV), to the forefront of American consciousness (Bennett, 2018). Along with personal anecdotes of victimization, #MeToo highlighted decades of work from social scientists who have attempted to conceptualize IPV as a consequence of various individual, interpersonal, and cultural factors (see Capaldi et al., 2012 for a review). One such interpersonal factor, sensitivity to rejection, has been proposed as a potential predictor of IPV, but this association has only been tested in men and has not been revisited in recent years (Downey et al., 2000). There is some evidence supporting connections between rejection sensitivity (RS) and self-silencing behavior (e.g., Harper et al., 2006), and between self-silencing behavior and conflict in intimate relationships (e.g., Romero-Canyas et al., 2013), but these three concepts have not been assessed simultaneously in one model. The purpose of this study was to revisit the role of RS in self-reported IPV perpetration and victimization among college students, to investigate the role of self-silencing as a mediator in this hypothesized relationship, and to test this relationship in a diverse sample.
Intimate Partner Violence
The U.S. Centers for Disease Control defines IPV as “physical violence, sexual violence, stalking and psychological aggression (including coercive tactics) by a current or former intimate partner (i.e., spouse, boyfriend/girlfriend, dating partner, or ongoing sexual partner)” (Breiding et al., 2015). Although this article focuses specifically on IPV in the United States, it is important to note that rates of IPV vary widely across and within countries, and are shaped by levels of gender equality, health care and legal systems, and sociopolitical values (World Health Organization, 2013). A nationally representative survey of American adults, the National Intimate Partner and Sexual Violence Survey, has found that the lifetime prevalence of any physical, sexual, or stalking victimization is 36.4% among women and 33.6% among men, although women report higher levels of sexual violence and more severe physical violence than men (Smith et al., 2018). Moreover, 47% of women and men report any lifetime psychological violence from an intimate partner, including coercive behavior (Smith et al., 2017). More women than men endorse IPV-related consequences that impact well-being, including injury, posttraumatic stress disorder (PTSD) and emotional distress, and days of missed work (Breiding et al., 2011). Further, half of all female homicide victims in the United States are killed by a current or former intimate partner (Petrosky et al., 2017). National surveys also find that racial and sexual minority individuals experience IPV more frequently than white and heterosexual individuals, respectively (Black et al., 2011). Important differences also exist between certain sexual minority identities (e.g., higher rates of IPV experienced by bisexual individuals, compared to gay and lesbian individuals; Messinger, 2011). Similarly, gender nonconforming, nonbinary, and transgender individuals experience higher rates of IPV compared to cisgender individuals (Valentine et al., 2017). Across age groups, young adults (i.e., those 16–24 years old) are particularly affected by IPV and report the highest rates of victimization: 20% of American college students report experiencing some form of IPV (National Coalition against Domestic Violence, 2015).
Important questions have emerged among IPV researchers about the directionality of violent behavior; that is, whether and under what circumstances IPV might be bidirectional (both partners perpetrate and are victimized by violent behaviors) rather than unidirectional (one partner perpetrates violent behaviors and the other is the victim). Several review papers and meta-analyses conclude that male and female partners in heterosexual relationships perpetrate and are victimized by IPV at similar frequencies within those relationships (see: Archer, 2002; Chan, 2011; Langhinrichsen-Rohling et al., 2012). However, there are gender differences in the severity of behavior perpetrated, with men engaging in more severe and more violent behaviors (Archer, 2002). There are also reporting differences between heterosexual partners, such that rates of violence differ when collecting self-report from one partner versus requiring agreement between both partners, which can lead to skewed prevalence data depending on study methodology (Caetano et al., 2009). Further, one of the most widely used scales to measure IPV, the Conflict Tactics Scale (Straus et al., 1996), does not collect information about the context or motivation of behavior (e.g., self-defense). Among LGBTQ+ couples, rates and directionality (i.e., unidirectional vs bidirectional) of IPV are similar to heterosexual couples overall, but minority stress (e.g., discrimination, internalized homophobia) may create unique risk factors for both victimization and perpetration (Decker et al., 2018). These questions of directionality have not yet been resolved; however, they highlight critical nuances in IPV behavior and underscore the importance of determining whether factors associated with IPV victimization are unique to victimization or might be similarly associated with perpetration.
Survivors of IPV experience a range of consequences, including physical and mental health outcomes (e.g., physical injury, posttraumatic stress, unintended pregnancy), employment outcomes (e.g., quitting a job to avoid a violent partner), and increased mortality (Black et al., 2011). IPV also has broad economic impacts (Breiding et al., 2015), ranging from the individual (e.g., loss of income after quitting a job) to the societal level (e.g., increased health care spending). College students who have experienced IPV may face additional and unique challenges; for example, female students who had been assaulted in their first year of college reported lower average grades than their peers (Jordan et al., 2014) and poor academic outcomes reduce students’ access to scholarships, student employment, and student housing. In a sample of undergraduates, IPV, sexual violence, and stalking were associated with lower academic efficacy, academic conscientiousness, and institutional commitment and higher levels of college-related stress (Banyard et al., 2017). As these data demonstrate, IPV affects millions of Americans with implications for many aspects of health and well-being. These impacts underscore the importance of better understanding potential predictors of violent behavior.
Rejection Sensitivity
One factor that may be associated with IPV behavior is RS. RS is conceptualized as a cognitive-affective processing framework through which individuals “anxiously expect, readily perceive, and overreact to rejection” (Downey & Feldman, 1996 p. 1327). RS is rooted in attachment theory and develops through early experiences with one’s caregiver (Downey & Feldman, 1996); however, researchers have applied this construct to study intimate relationships in adolescence and adulthood (Downey et al., 1998; Downey et al., 2000). Broadly, RS has been associated with maladaptive behaviors and poor outcomes in intimate relationships. In samples of college students, Downey and Feldman found that students who were higher in RS were more likely than their low RS peers to attribute harmful intent to a partner’s ambiguously insensitive behavior, were less satisfied with their current relationship, and were more likely to engage in behavior that conveyed jealousy (by men) and hostility (by women). In a longitudinal study, higher RS levels predicted relationship breakup, even after controlling for participants’ partners’ RS levels, relationship satisfaction, and commitment (Downey et al., 1998). This line of work supports the theory that high levels of RS may initiate a “self-fulfilling prophecy” by which individuals who are high in RS and perceive rejection engage in avoidant or disagreeable behavior, which elicits the very rejection they hope to avoid (Downey et al., 1998; Meehan et al., 2018).
Beyond disagreeable behavior, high levels of RS have also been associated with aggression and violence in intimate relationships. Experimental priming studies with female samples have found that high RS participants were faster to pronounce hostility-related words after being primed with rejection related words, compared to neutral or negative primes, and these effects were not found in low RS participants (Ayduk et al., 1999). In a laboratory setting, male and female high RS participants gave a potential date who had rejected them more hot sauce (as a measure of hostility) than low RS participants, even after reading about the date’s aversion to spicy food (Ayduk et al., 2008). In a sample of male undergraduates, participants who reported high levels of RS and romantic investment were more likely to report physical aggression against a dating partner than participants who reported low levels of these constructs (Downey et al., 2000). And in a daily diary study among women, participants high in RS were more likely than participants low in RS to report conflict, including threats and insults, with their intimate partners on days immediately following a perceived rejection (Ayduk et al., 1999). Taken together, this evidence supports the hypothesis that individuals who are high in RS may be more likely to engage in IPV behavior.
Conversely, individuals who are high in RS may also be more likely to accept hostile or aggressive behavior from a partner to stave off rejection, which may leave them vulnerable to IPV victimization. In a series of experimental studies among undergraduates, Romero-Canyas et al. (2010) found that high RS individuals engaged in ingratiating behavior in certain contexts: among men, RS predicted willingness to spend money on a date with someone who had harshly rejected them and among women, RS predicted willingness to buy an expensive gift for someone who had read their profile and declined to meet them. In a study of middle school girls, high levels of RS were associated with a willingness to engage in potentially “wrong” behaviors to maintain a romantic relationship (Purdie & Downey, 2000). This may be pertinent to sexual health behaviors: in one study of college students, RS significantly predicted infrequent condom use only among participants who wanted to use condoms but thought that their partner did not (Edwards & Barber, 2010). Further, high RS individuals who perceived low approval of a romantic partner from their social network reported stronger relationship commitment, whereas the opposite pattern was observed for low RS individuals (Besikci et al., 2016). These findings suggest that high RS individuals may be willing to ingratiate themselves to a rejecting or hostile partner by sacrificing resources, engaging in undesirable behavior, reducing outside social ties, and otherwise minimizing their own needs to please their partner.
Self-silencing
Censoring and devaluing one’s own needs to please a partner is conceptualized as self-silencing (Jack, 1991). Self-silencing originated as a hypothesized explanation for higher rates of depression among women compared to men (Jack, 1991). Jack (1991) theorized that women experience tension between their self-interest and their intimate relationships, leading them to repress their opinions, desires, and feelings to maintain the peace in their relationships, and therefore women are more likely than men to become depressed. Although self-silencing was originally theorized as a behavior common in women, subsequent studies have found that men report self-silencing at rates equal to or higher than women (Duarte & Thompson, 1999; Gratch et al., 1995). Hypothesized reasons for this unexpected gender parity include gender differences in interpreting the questionnaire (i.e., gender differences in conception of “voice” and agency; Smolak, 2010) and gendered socialization patterns (i.e., men may be silencing emotional responses to avoid them, not as self-sacrifice; Remen et al., 2002). For men and women, self-silencing is an important variable to the functioning of individual and dyadic interactions (e.g., Harper et al., 2006; Thomas & Bowker, 2015).
Previous work has found associations between self-silencing and various measures of relationship function and satisfaction, particularly in younger populations. In a study of heterosexual adolescent couples, partners who reported higher levels of self-silencing also reported poorer communication, and girls who reported higher self-silencing reported lower relationship satisfaction (Harper & Welsh, 2007). Also in heterosexual adolescent couples, self-silencing significantly mediated the effect of RS on depression symptoms for both partners (Harper et al., 2006). In a longitudinal study, Little et al. (2011) found that frequency of sexual intercourse among heterosexual adolescents moderated the effect of self-silencing on depression, such that self-silencing predicted depressive symptoms only among participants engaging in more frequent sexual intercourse. Self-silencing also significantly mediated the effect of conflict on depressive symptoms for both partners in a study of heterosexual married couples (Whiffen et al., 2007). Outside romantic contexts, self-silencing has been shown to significantly mediate the effect of RS on friendship support in male and female adolescents (Thomas & Bowker, 2015). This evidence supports the role of self-silencing as an important factor in relationship function and well-being, particularly in young adults.
There is also evidence to suggest that self-silencing behavior and aggressive behavior are related. In a sample of college students, self-silencing behavior significantly positively mediated the effect of RS on post-rejection hostility among women, but not men (Romero-Canyas et al., 2013). In a daily diary study, high RS individuals who reported high levels of prevention pride (i.e., pride in avoiding negative interpersonal outcomes) reported higher levels of self-silencing to avoid conflict and higher levels of hostility in the days following self-reported conflict, compared to low RS and low prevention pride participants (Ayduk et al., 2003). Given the effects of RS on various interpersonal outcomes through self-silencing, and the associations between self-silencing behavior and hostile behavior, it is reasonable to hypothesize that RS may predict IPV perpetration and/or victimization through self-silencing.
Present Study
The present study uses a cross-sectional survey design in a college student population to test the role of self-silencing as a mediator in the hypothesized relationship between RS and IPV experiences. Given the theorized bidirectional nature of IPV and evidence to support RS as a predictor of both aggression and ingratiation, we hypothesized that there would be a significant positive effect of RS on IPV perpetration and of RS on IPV victimization across individuals, and that self-silencing would be a significant mediator of both relationships. As an exploratory hypothesis, we included race and gender as potential moderators of these relationships.
Methods
Participants
Participant Demographics.
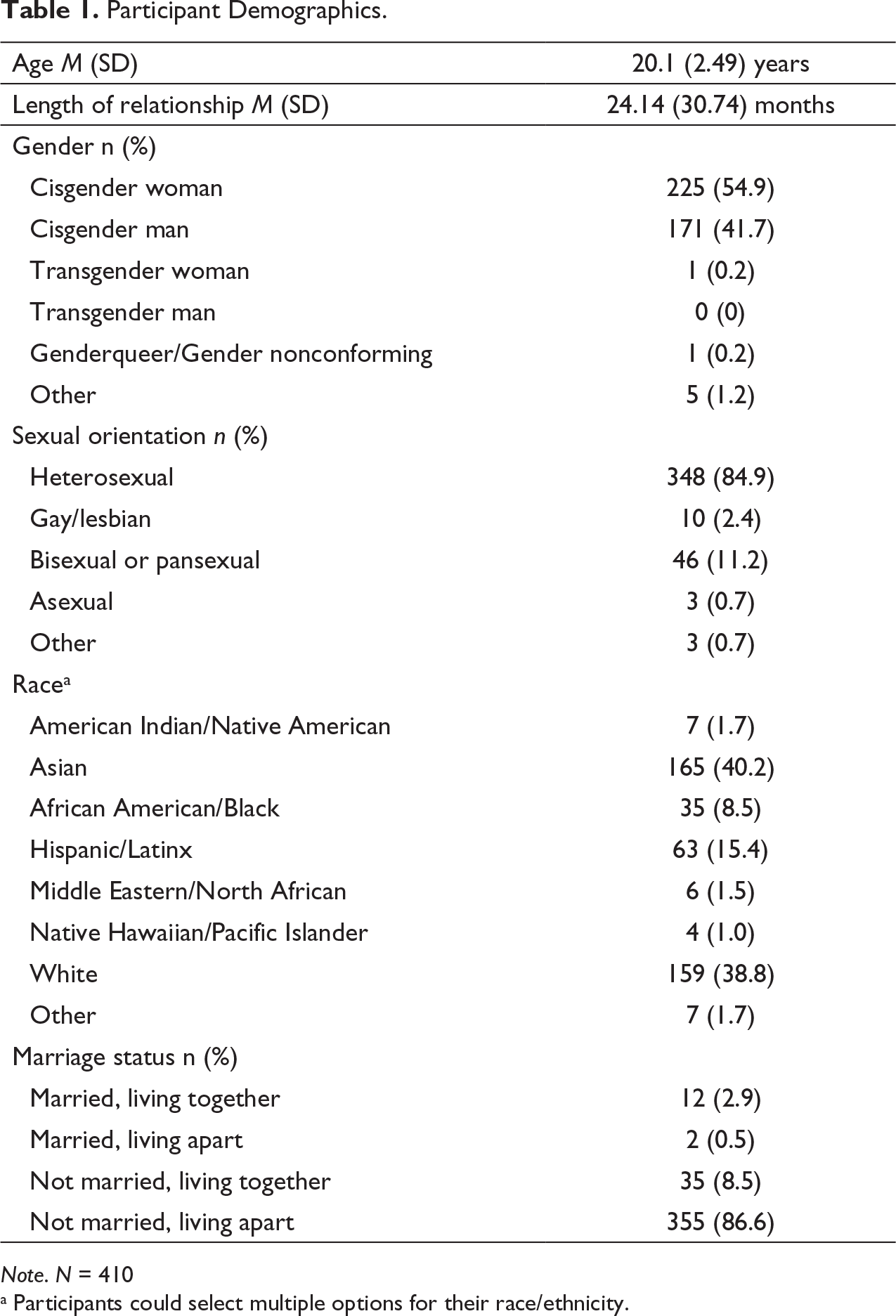
Note. N = 410
a Participants could select multiple options for their race/ethnicity.
Procedure
This study was approved by the University Institutional Review Board. Participants were eligible to participate if they were 18 years or older, able to read and understand English, and in a self-defined intimate relationship. After reading a brief recruitment slide, participants were directed to the consent form. The consent form advised participants to complete the study in a private space and on a personal computer in order to maintain privacy and confidentiality. After survey completion, participants received debriefing information and were compensated with course credit (i.e., participants received points toward their final grade in their psychology courses for participating in university research studies). Participants also received information about available counseling resources, including the campus counseling center and a national IPV hotline. Data collection occurred between April and December, 2019.
Measures
Rejection sensitivity. Rejection sensitivity was measured using the Rejection Sensitivity Questionnaire (RSQ; Downey & Feldman, 1996) which contains eight potential rejection scenarios (e.g., “Imagine you call your partner after a bitter argument and tell them you want to see them”). After each scenario, participants rate their concern/anxiety (e.g., “How concerned or anxious would you be over whether or not your partner would want to see you?”) on a scale of 1 (“Very unconcerned”) to 6 (“Very concerned”) and their expectations for the event (e.g., “I would expect that they would want to see me”) on a scale of 1 (“Very unlikely”) to 6 (“Very likely”). Items are scored by multiplying the response to the first question (anxiety) by the reverse of the response to the second question (expectations) and then averaging across the eight scores. Higher scores indicate higher levels of RS. Reliability of the eight-item measure in the current study was acceptable (α = .67), though lower than the reliability found in previous studies (α = .77; Romero-Canyas et al., 2010).
Intimate partner violence. IPV was assessed with items taken from the Conflict Tactics Scale (CTS; Straus et al., 1996). This 78-item measure presents 39 behaviors an individual may have perpetrated against or experienced from an intimate partner in the past year. Sample items include “I threw something at my partner that could hurt” and “I had a sprain, bruise, or small cut because of a fight with my partner.” Consistent with established scoring guidelines (Straus et al., 1996) participants indicated the frequency of these behaviors in their relationship on a scale of 0 (“Not in the past year/Never”) to 25 (“More than 20 times in the past year”). Responses were summed to create a perpetration (α = .88) and a victimization (α = .90) score for each participant.
Self-silencing. Self-silencing was measured with the Silencing the Self Scale (STSS; Jack & Dill, 1992), which asks participants to indicate their agreement on a scale from 1 (“Strongly disagree”) to 5 (“Strongly agree”) with 31 items about self-silencing, ingratiating, or accommodating behaviors in an intimate relationship. Example items include “Caring means choosing to do what the other person wants, even when I want to do something different” and “I think it is best to put myself first because no one else will look out for me” (reverse scored). Items are summed such that higher scores reflect higher levels of self-silencing. The STSS has been considered to have four subscales: Self-Silencing, Divided Self, External Self-Perception, and Care as Self Sacrifice (Jack & Dill, 1992). However, there is evidence to suggest the four-factor model is a poor-fitting model (Cramer & Thoms, 2003; Remen et al., 2002). Overall sum scores have also been used in place of subscale scores in other recent studies on self-silencing and sexist behavior (e.g., Hurst & Beesley, 2013; Watson & Grotewiel, 2016). Therefore, in the present study, only the overall sum score was considered. Internal reliability for the 31-item scale was strong (α = .90).
In addition to the aforementioned scales, participants completed demographic measures (e.g., age, race, gender, sexual orientation), questions about the relationship with their intimate partner (e.g., length of relationship, marital status, children, level of financial interdependence), and questions about their perceived levels of support from their partner, adherence to traditional gender roles, and psychological wellbeing (e.g., anxiety, depression).
Data Analysis
Descriptive statistics and bivariate correlations were conducted in IBM SPSS Statistics 26. Mediation analyses were conducted in Mplus version 8.3 (Muthén & Muthén, 2017). IPV victimization and perpetration variables were count data with nonnormal distributions, therefore negative binomial regression was used to model these outcomes (Swartout et al., 2015). Both models tested the effect of RS on past-year IPV (victimization and perpetration) through self-silencing. In each model, we tested gender and race as moderators of both paths. We did not control for participant gender or race, or any other variable.
Results
Descriptive Statistics
Descriptive Statistics and Variable Intercorrelations.
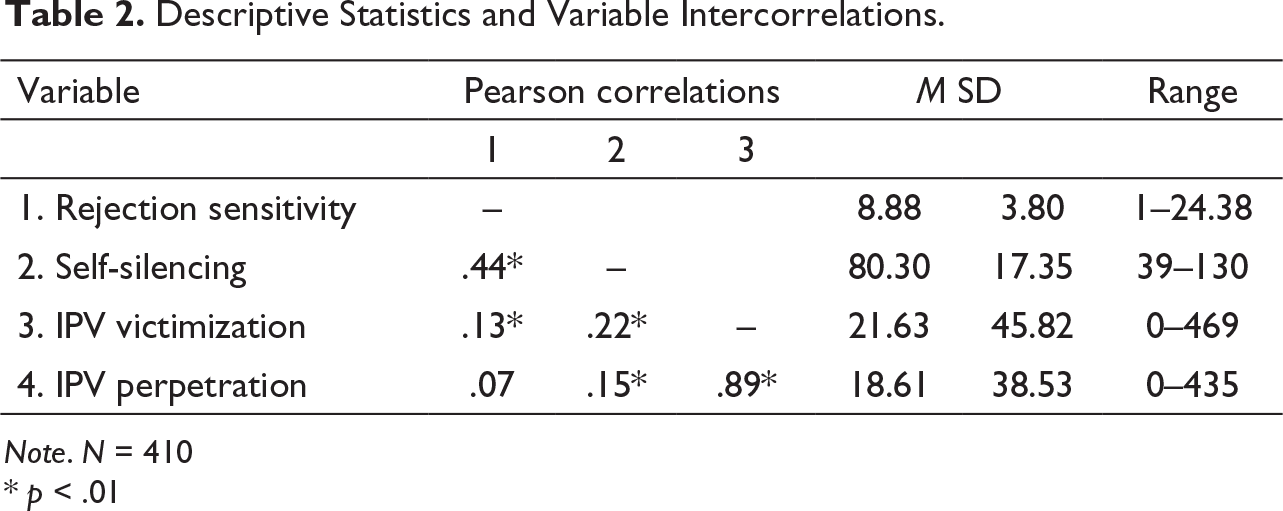
Note. N = 410
* p < .01
We also checked for possible racial differences in the variables of interest. A series of one-way ANOVAs revealed a significant effect of race on RS, F(6, 403) = 3.03, p < .01 and on self-silencing, F(6, 403) = 5.15, p < .01. Tukey-Kramer post-hoc tests revealed no significant mean differences between racial groups on RS, but found significant mean differences in self-silencing between Asian participants (N = 152; M = 85.22, SD = 15.20) and White participants (N = 137; M = 76.62, SD = 18.12), p < .01 and between Asian participants and Latinx participants (N = 46; M = 77.40 SD = 18.90), p < .05. There was no significant effect of race on IPV victimization or perpetration. Previous studies have similarly found higher scores on RS and self-silencing for Asian individuals compared to White, Latinx, and Black individuals (Gratch et al., 1995; see also Chan & Mendoza-Denton, 2008; London et al., 2007).
Mediation Model
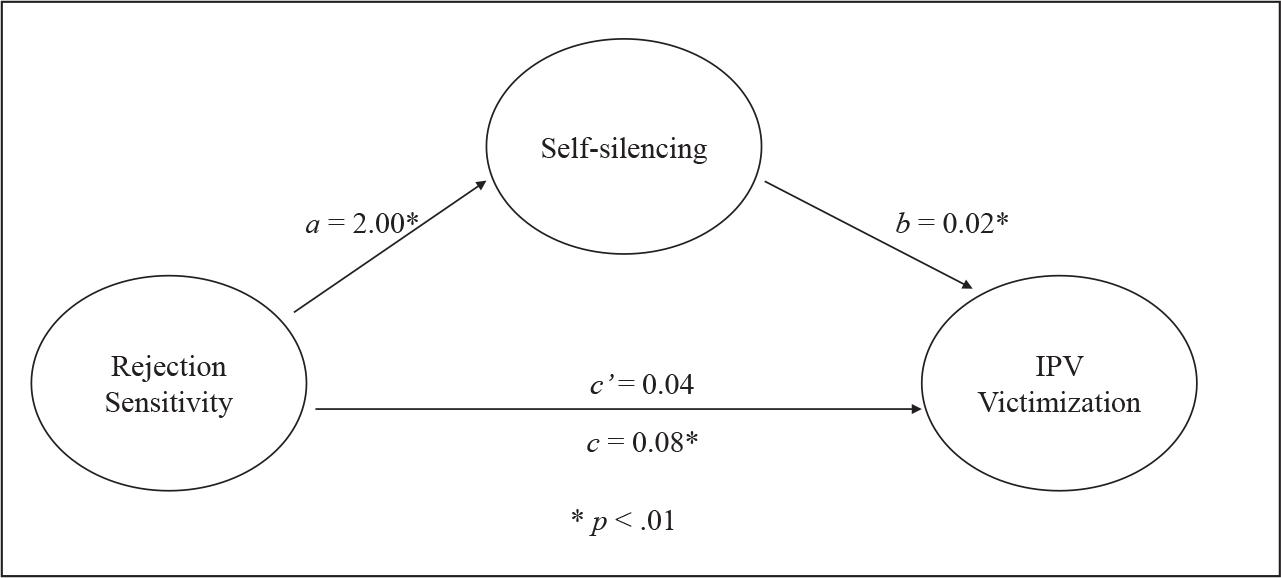
RS indirectly predicted IPV victimization through its association with self-silencing (see Table 3 and Figure 1). Participants who reported higher levels of RS also reported higher levels of self-silencing (b = 2.00; 95% CI [1.59, 2.41]) and participants who reported higher levels of self-silencing reported higher counts of IPV victimization in the past year (b = 0.02; 95% CI [0.01, 0.03]). There was a significant indirect effect of RS on victimization (b = 0.04; 95% CI [0.02, 0.07]), but no significant direct effect (b = 0.04; 95% CI [−0.01, 0.09]). Despite the gender differences in self-silencing and the racial differences in RS and self-silencing, neither gender nor race was a significant moderator of either path in the model.
Mediation model: Victimization as outcome.
Model Coefficients.
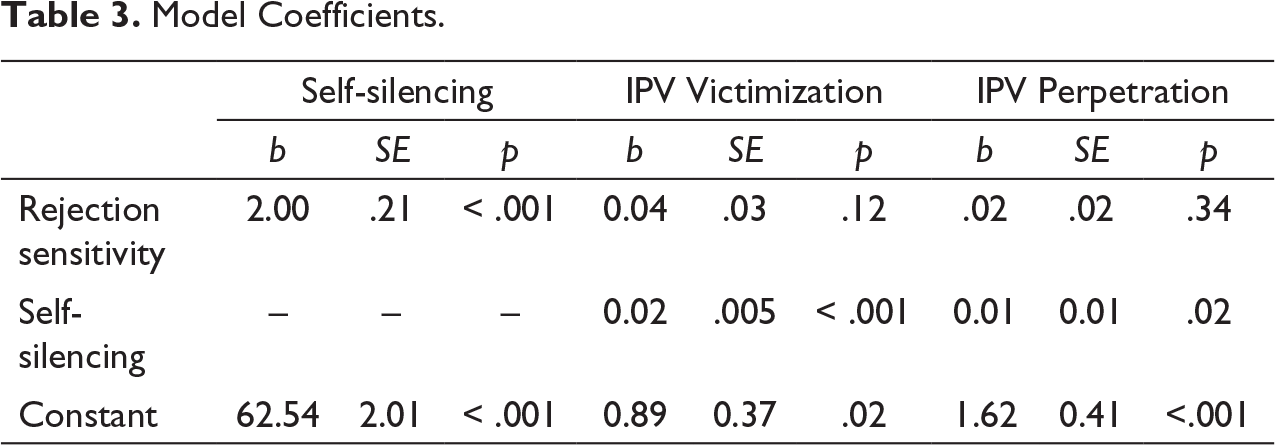
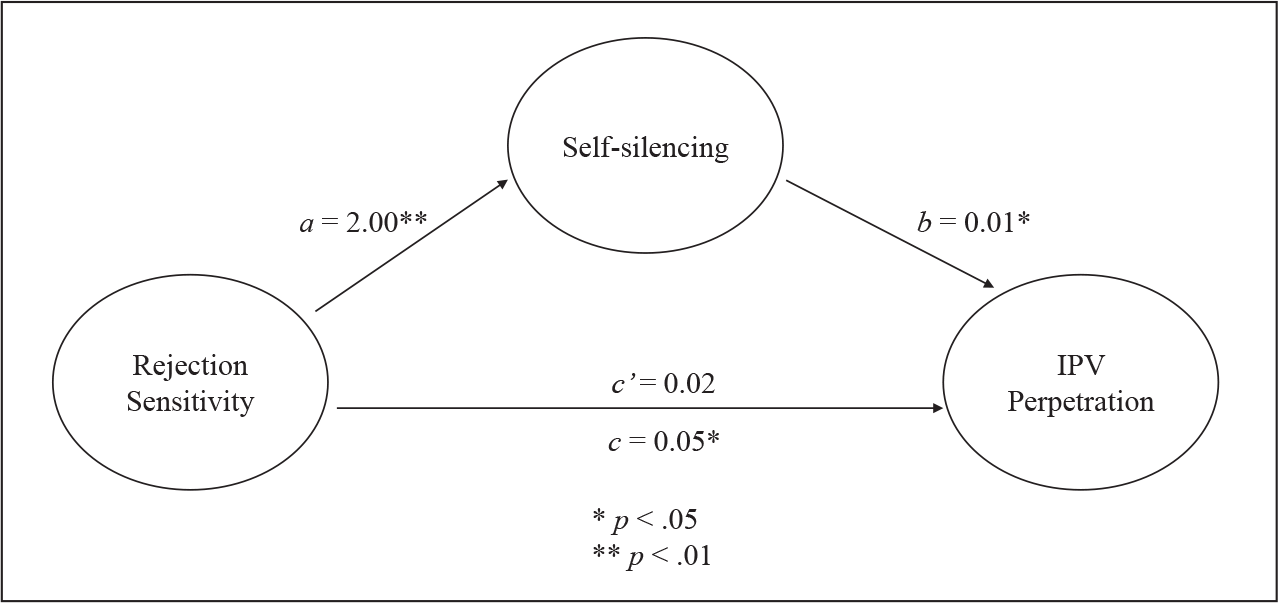
RS indirectly predicted IPV perpetration through self-silencing (see Table 3 and Figure 2). Participants who reported higher levels of RS reported higher levels of self-silencing (b = 2.00; 95% CI [1.59, 2.41]) and participants who reported higher levels of self-silencing reported higher counts of IPV perpetration in the past year (b = 0.01; 95% CI [0.002, 0.02]). There was a significant indirect effect (b = 0.03; 95% CI [0.004, 0.05]) of RS on IPV perpetration, but no direct effect (b = 0.02; 95% CI [−0.02, 0.06]). Neither gender nor race was a significant moderator of either path in the model.
Mediation model: Perpetration as outcome.
Discussion
The purpose of this study was to revisit rejection sensitivity as a predictor of IPV perpetration and victimization, to test self-silencing as a potential mediator of these relationships, and to examine these models in a diverse sample of college students. We found that RS was a significant predictor of IPV victimization and IPV perpetration and self-silencing fully mediated both of these relationships. RS as a predictor of IPV perpetration extends previous work supporting a relationship between RS and aggression/hostility in interpersonal relationships (e.g., Ayduk et al., 2008; Downey et al., 2000) to include IPV behavior. Although previous research has identified self-silencing as a mediator between RS and hostility in women (Romero-Canyas et al., 2013), we found here that self-silencing mediated the RS-IPV perpetration link in a mixed-gender sample.
Similarly, this study found that RS significantly predicted IPV victimization. Previous work has found that high-RS individuals are more likely to ingratiate themselves to a partner, pursue relationships that their support networks disapprove of, and engage in undesired unprotected sex to avoid rejection (Besikci et al., 2016; Edwards & Barber, 2010; Purdie & Downey, 2000). Our findings suggest that high RS individuals may also engage in self-silencing or ingratiating behaviors when the threat of rejection is in the form of violence or aggression. Although self-silencing has been identified as a key mediator in the relationship between RS and outcomes including depression and perceived support (Harper et al., 2006; Thomas & Bowker, 2015), this is the first study to identify self-silencing as a mediator between RS and victimization.
These findings do not indicate that high RS individuals cause their intimate partners to become violent, or that engaging in self-silencing is a form of “asking for” violence. In fact, RS may be better conceptualized as a risk factor than a causal factor. Nor do our findings suggest that high RS individuals who engage in violence should not be held accountable. It is possible that individuals who perpetrate IPV behaviors seek out partners who appear sensitive to rejection or willing to ingratiate themselves. RS and IPV have common risk factors stemming from negative childhood experiences: past experiences of child abuse and adolescent IPV are predictive of IPV victimization and perpetration in adulthood (Manchikanti Gómez, 2011) and childhood experiences with parental rejection and maltreatment are predictors of RS later in life (Downey et al., 1997; see also Araiza et al., 2019). Additionally, experiencing peer rejection early in life may lead to both increased peer victimization (due to a lack of social support) and increased endorsement of aggression as a legitimate response (Dill et al., 2004). Longitudinal work, in the form of prospective designs or daily diary studies, is necessary to untangle these relationships.
It is important to note the very high correlation between IPV perpetration and victimization in this sample (r = .89), in concordance with previous work on IPV bidirectionality (e.g., Langhinrichsen-Rohling et al., 2012). A survey of college students across 32 nations found that bidirectional violence is the most commonly reported type of IPV (Straus, 2008). Additionally, one’s partner’s use of aggression has been identified as a significant predictor of aggression in intimate relationships among adolescent and young adult couples (Capaldi et al., 2007; Baker & Stith, 2008). Although a great deal of work has focused on gender differences in directionality (e.g., Archer, 2002), future research should investigate the role of other potentially informative variables, including motivation (e.g., self-defense or retaliation) and individual difference variables (e.g., RS-adjacent constructs like attachment style).
One strength of this study was the college student sample. Early adulthood is a particularly vulnerable time for IPV victimization: the majority of individuals who report lifetime IPV victimization first experience victimization before the age of 25 (Smith et al., 2018). We were therefore able to test the hypothesized RS-IPV relationship during this period in which IPV, and intimate relationships more generally, are particularly salient. This study was also strengthened by the racial diversity of the sample, which had roughly equal numbers of Asian and White students, reflecting the population of the university where the sample was recruited. Despite racial differences in levels of RS and self-silencing in this sample, particularly for Asian participants, race did not moderate either path in the models. The generalizability of these models across races is important given the increasing racial and ethnic diversity in higher education in the United States (Espinosa et al., 2019). Specifically, the percentage of young adults pursuing an undergraduate degree is higher among Asian individuals than any other race/ethnic group (Espinosa et al., 2019). Given the prevalence of IPV among young adults and the focus on IPV prevention programming for undergraduates, determining which processes generalize across races is just as important as determining which processes are moderated by racial group or other social identity.
Despite these strengths, there are a few limitations to this work. First, this study used a cross-sectional design. Despite theoretical evidence to suggest RS develops in childhood (Araiza et al., 2019; Downey et al., 1997), before dating and intimate relationships begin, the cross-sectional design limits our ability to make causal conclusions. Future work should test the proposed mediation models using longitudinal methods. Additionally, despite instructions to complete the questionnaire honestly and in a private space, it is possible that participants underreported their own behaviors and experiences with IPV (Follingstad & Rogers, 2013). Collecting data from both partners would allow for a better understanding of behavior frequency and directionality.
In conclusion, the current study found that RS is a significant predictor of self-reported IPV victimization and IPV perpetration, and that self-silencing is a significant mediator in both of these paths. Over one-third of Americans report experiencing some form of physical, sexual, or psychological IPV during their lives and these experiences adversely impact physical and psychological health, as well as academic, professional, and economic outcomes (Smith et al., 2018). This work has implications for IPV research and IPV prevention programming. Future work on IPV prevention should further investigate RS and similar cognitive affective processes, as well as self-silencing or other ingratiating behaviors, as potential risk factors for victimization and violence. IPV prevention programming, which is popular on college campuses, typically focuses on interpersonal and community-level constructs, including the bystander effect and social norms (e.g., rape myths; Dills et al., 2016). These programs should consider addressing individual-level factors, which could include information about individual differences in rejection sensitivity and self-silencing or additional support systems for students for whom these factors increase their vulnerability to engaging in or being victimized by violent behavior.
Footnotes
Acknowledgments
We would like to acknowledge Dr Marci Lobel for her constructive feedback on an earlier version of this article and Dr Christina Dyar for her advice on analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.