
Abstract
Domestic violence, broadly defined, includes violence among children, parents, siblings, intimate partners, and other relatives. Help-seeking behaviors for domestic violence, especially among sexual minority (gay, lesbian, bisexual, and others who are not heterosexual) victims, is not well understood. Using the National Crime Victimization Survey, the current study fills a gap in the literature regarding the relationship between sexual orientation and four types of formal help-seeking among victims of violence perpetrated by a relative or an intimate partner: reporting to the police, seeking psychological care, contacting a victim services agency, and seeking medical assistance. This study additionally examined whether individual and incident level variables are related to formal domestic violence help-seeking among sexual minority victims. Results indicate that sexual orientation was significantly related to seeking psychological care and help from a victim services agency, and the relationship between individual and incident level characteristics varies by type of help-seeking among victims of domestic violence. These results suggest that sexual minority victims’ decisions to access services is likely influenced by the availability of services and victims’ perceptions of how they would be treated within the various systems. Future research should continue to examine the help-seeking process among sexual minority victims of domestic violence in order to develop appropriate policy responses and provide services needed by this population.
Introduction
There has been a scholarly focus on domestic violence (DV) in the criminal justice system and research community since physicians and advocates brought the issue of child abuse to the forefront of social concern in the 1960s (Pleck, 1989). Feminists, activists, and advocates expanded this concern to violence against women in the 1970s. Today, the majority of DV state statutes address relationships between current or former intimate partners, boyfriend/girlfriends, household members, and other relatives. Most DV research regarding adults and teens in late adolescence conducted to date, however, has focused on violence between assumed heterosexual intimate partners with males as perpetrators and females as victims (Addington & Lauritsen, 2021). As a result, less is known about DV committed by other relatives and family members. Further, less is known about DV among sexual minority (SM) populations, which includes lesbian, gay, bisexual (LGB), and other non-heterosexual individuals (Edwards et al., 2015). This gap in research is especially concerning due to recent findings that SM individuals are at a heightened risk for DV victimization compared to heterosexual individuals. Some studies have documented high rates of injuries for intimate partner violence (IPV) among SM victims (Merrill & Wolfe, 2000). In addition to experiencing higher rates of DV, other studies have found that SM victims of DV may suffer enhanced mental and physical health consequences compared to heterosexual DV victims due to the combination of numerous systems of oppression faced by this population (Miller et al., 2016). Donovan and Barnes (2020) suggest that DV among this population is a social problem “exacerbated by cisgendered heteronormativity, heterosexism and LGB[Transgender] invisibility” (p. 567). Overall, research indicates that the potential for trauma is amplified among SM populations (Alessi et al., 2013).
The majority of research examining DV among SM victims has focused on the prevalence and correlates of violence with less attention directed at understanding help-seeking (HS) behaviors (Donovan & Barnes, 2019). HS is a broad term that refers to actions taken by victims to access informal and formal sources of support, including law enforcement, victim service providers, mental health professionals, medical providers, spiritual advisors, friends, and family. This gap in research on HS is concerning given that DV victims in general may be less likely to seek support and that SM victims of DV may be even more reticent to seek help. However, studies have shown that victims who engage in HS efforts are less likely to experience negative consequences from their victimization (Goodman et al., 2003).
It is important to understand the extent to which SM victims experience DV victimization and seek help from victim service providers and/or engage in other formal HS behaviors. It is additionally important to understand whether other characteristics of victims, such as race and age, and incidents, such as severity and victim offender relationship, impact the relationship between SM status and HS behaviors. Although many DV victims do not seek help, a careful study of the relationship between DV victimization, HS, and sexual orientation can provide insight for developing services that best support survivors. This study addresses limitations in the understanding of the impact of sexual orientation on formal HS for victims of DV.
Literature Review
Domestic Violence Victimization Among Sexual Minority Individuals
DV is a broad term that includes violence among children, parents, siblings, other family members and relatives, as well as IPV, a type of DV that specifically occurs between individuals who have an intimate relationship. DV perpetrators inflict physical, sexual, psychological/emotional, and/or economic harm that often intensifies over time. While the majority of research on DV among adults and adolescent/emerging adult dating partners has focused on IPV within assumed heterosexual relationships with males as perpetrators and females as victims (Addington & Lauritsen, 2021), there has been a recent shift in research to focus on DV among SM populations (Edwards et al., 2015). For example, to increase knowledge about IPV among SM populations, the National Intimate Partner and Sexual Violence Survey (NISVS) has inquired about respondents’ sexual orientation since 2010. Additionally, the National Crime Victimization Survey (NCVS) amended its survey questions in 2016 to ask about respondents’ sexual orientation. Addington and Lauritsen (2021) refer to these methodological changes as a step in “data innovation” among this line of research (p. 305). Now, national data can be used to estimate the rates at which SM individuals experience violence perpetrated by relatives and intimate partners compared to heterosexual individuals as well as assess victims’ efforts to reach out to formal sources of support, such as law enforcement (Bender & Lauritsen, 2021). Doing so challenges social norming of traditional heterosexual relationships within the research literature (Goldenberg et al., 2018).
Recent research suggests that rates of DV among couples in same-gender relationships are just as high or higher than rates among couples in different-gender relationships (Edwards et al., 2015). Based on data from the NISVS, 44% of lesbian, 61% of bisexual, and 35% of straight women reported experiencing IPV (measured as rape, physical violence, or stalking) by an intimate partner at some point in their lifetime (Walters et al., 2013). Twenty-six percent of gay, 37% of bisexual, and 29% of straight men experienced IPV by an intimate partner (Walters et al., 2013).
According to Morgan and Truman (2020), the rate of DV committed by intimate partners or other family members was 4.2 violent victimizations per 1,000 persons age 12 or older in the population, based on the 2019 NCVS survey. One of the first studies to examine the relationship between gender identity, sexual orientation, and victimization using the revised NCVS found that rates of violent victimization by a person well known to the victim, including intimate partners, relatives, or other persons, were significantly higher among sexual and gender minority (SGM; i.e., LGB and transgender people) individuals than non-SGM individuals. Specifically, rates were 71.1, 16.2, and 14.7 (per 1,000 people) for overall violence, IPV, and violence by a relative, respectively, among SGM respondents compared to 19.2, 2.4, and 2.0 for non-SGM individuals (Flores et al., 2020). Similarly, Bender and Lauritsen (2021) report that SM individuals are significantly more likely than heterosexual individuals to experience a violent victimization committed by a known person other than an intimate partner, and bisexual females, specifically, experience IPV at a rate that is 7.6 times higher than straight females.
In addition to an increased research focus on DV among SM victims, changes to the Violence Against Women Act (VAWA) have also begun to address the concern that this population is “largely invisible in DV[Abuse] policy and practice” (Donovan & Barnes, 2020, p. 554). Protections for same-gender couples were included in the 2013 reauthorization of VAWA. The controversial and contentious reauthorization addressed the needs of several marginalized groups, including lesbian, gay, bisexual, and transgender (LGBT) individuals. Specifically, a provision was added to the Act that prohibits the denial of services based on sexual orientation by programs funded by VAWA (Gover & Moore, 2021). It is important to note that even though the reauthorization provided the enabling legislation, this did not ensure equitable delivery, access, and provision of services for all victims.
Help-Seeking Behaviors Among Sexual Minority Individuals
Despite these legislative changes, little is known about the extent to which SM DV victims seek assistance from victim service providers or other formal sources of help or about factors that contribute to the likelihood of formal HS. Given that the majority of SM DV research focuses on violence between intimate partners, less is known about DV perpetrated by other family members specifically or about HS after such incidents. Existing research suggests that SM youth experience more parental abuse and rejection as well as violence from siblings than heterosexual youth, while older LGBT adults face additional types of elder abuse related to their identity, such as ostracism from family, and are hesitant to seek help due to prior experiences of discrimination during the life course (Bloemen et al., 2019; Friedman et al., 2011; Martinez & McDonald, 2021; Richter et al., 2017). More research is needed on these groups, as well as on adults who experience DV from parents and siblings and their HS behaviors.
Additionally, many studies that examine the relationship between sexual orientation and DV, especially within the IPV literature, compare same-gender violence to different-gender violence, which can mask the experiences of those who identify as bisexual within the SM population. Regardless of sexual orientation, the limited available studies suggest that victims of DV by an intimate partner are more likely to engage in informal HS (i.e., support from friends, family members, or co-workers) rather than formal HS (i.e., police, mental health, legal, housing, medical, and advocacy services) (Santoniccolo et al., 2021). Although most of the existing studies are based on nonrepresentative convenience samples, such as survivors working with a victim services agency, they provide a foundation for developing research questions around the HS behaviors of SM individuals. For example, these studies suggest that the majority of SM individuals who experience IPV do not seek help from formal sources of support such as the police or service-delivering agencies (Barnes & Donovan, 2018). According to Barnes and Donovan (2018), among those who do seek formal help, SM victims tend to do so from private service providers such as therapists. This is supported by Hardesty et al. (2011), who reported that SM IPV victims are more likely to seek discrete formal services, such as mental health counseling, rather than IPV-specific services from a DV shelter. Finally, a recent systematic review of DV HS for violence committed by same-gender intimate partners found that counselors were the most commonly sought formal source of support, which included psychologists, psychiatrists, social workers, and therapists (Santoniccolo et al., 2021). Again, it is important to note that most of the studies assessed are not generalizable due to methodological and sampling limitations and focus almost exclusively on DV committed by intimate partners.
In addition to the suggestion that SM IPV victims are more likely to seek help from private service providers, there is limited research to suggest that the experiences SM DV victims have when they seek help from a provider may differ from those of straight victims. Previous research has found that mental health service providers do not view violence among same-gender partners to be as serious as violence between different-gender partners (Blasko et al., 2007; Wise & Bowman, 1997). Additionally, according to a national survey, practitioners from DV shelters were less likely to perceive women in same-gender relationships as victims compared to women in different-gender relationships (Basow & Thompson, 2012). Studies have also found that some DV hotline workers subscribe to the traditional view of an IPV victim being female and the perpetrator being male which further marginalizes SM IPV victims (Turell & Herrmann, 2008). Further, shelter services for SM victims do not exist in most jurisdictions which leaves gay and lesbian victims without residential services (Hammond, 1989; Pattavina et al., 2007).
Although Kuehnle and Sullivan (2003) reported that those in same-gender relationships engage in formal HS by reporting victimization to the police at similar rates as those in different-gender relationships, identifying as a SM could present additional barriers to receiving help from the criminal justice system. SM victims’ reporting rates are impacted by victims’ fears of being treated in a biased, discriminatory, and insensitive manner by police due to underlying homophobic attitudes (Hardesty et al., 2011; Scheer et al., 2020). Additionally, some SM victims do not report because they are afraid their experience will not be considered as serious as heterosexual IPV, and instead viewed as mutual violence resulting in dual arrest (Hirschel & McCormack, 2021; Turell & Herrmann, 2008). These findings suggest that HS rates from formal sources, like counselors, victim service providers, and the police, may be different for SM populations when examined in a nationally representative sample.
While some DV HS research has found that the relationship between the victim and offender impacts HS, factors related to HS, and specifically those among SM victims, are still not well understood (Barnes & Donovan, 2018; Mookerjee et al., 2015). DV victims of violence by a same-gender intimate partner have reported feeling “doubly closeted” because of the social stigma related to their SM status as well as the stigma surrounding violence among intimate partners. Due to these feelings, SM victims of DV may have different experiences when seeking informal and formal sources of support (Santoniccolo et al., 2021). As such, it is necessary to understand the extent to which demographic and incident characteristics condition the likelihood of HS among DV victims while accounting for sexual orientation.
The Current Study
Sexual orientation has recently been found to have an impact on several crucial stages of the HS process (Rollè et al., 2021). Despite the increase in research focusing on DV by intimate partners among SM individuals, there are gaps in the literature in terms of understanding DV victimization perpetrated by other relatives and HS among this population. Recent research indicates that rates of DV, and specifically, IPV, among SM individuals are as high or higher than rates among straight couples. Additionally, much of the research on formal HS behaviors is limited methodologically. Given that SM DV victims face additional barriers when seeking formal help, such as heteronormative biases and systemic heterosexism, the extent to which LGB individuals seek help is not well understood. Finally, while the literature has identified individual and offense level factors that are related to formal HS among straight intimate partners, questions remain regarding factors that influence formal HS for DV among SM individuals.
The current study uses recent data from the NCVS to address these gaps in the literature. Specifically, to understand the relationship between sexual orientation and formal HS among victims of DV, this study answers the following three research questions: 1) Do rates and characteristics of DV victimization perpetrated by intimate partners and other relatives vary according to sexual orientation? 2) Is there a relationship between DV HS behaviors and sexual orientation among victims of violence perpetrated by intimate partners and other relatives? 3) Is there a relationship between individual and incident level factors and HS among SM and heterosexual victims of violence perpetrated by intimate partners and other relatives?
Methodology
Data Source and Sample
Data are from the NCVS, a nationally representative, household-based survey, sponsored by the Bureau of Justice Statistics (BJS), that collects information on self-reported experiences with criminal victimization (BJS, 2020). The NCVS is one of the two principal measures of crime in the U.S. In addition to capturing incident level information on victimizations both reported and not reported to police, the survey also collects data on the characteristics of victims and victims’ socio-emotional responses and HS behaviors. The survey is in the field on a continuous basis with data collected by representatives from the U.S. Census Bureau through in-person and telephone interviews with all persons age 12 or older living in sampled households. Households are in the sample for 3 years and interviewed every 6 months about experiences with criminal victimization during the prior 6 months. The BJS releases annual public-use files available through the National Archive of Criminal Justice Data and an annual report containing additional methodological information about the survey (Morgan & Truman, 2020).
In 2016, the NCVS became the first federal household-based survey to collect data on the sexual orientation and gender identity of respondents age 16 or older. The current analysis uses pooled NCVS data from 2017 through 2019, which are the three publicly available years of data that include the sexual orientation variable. The sample was restricted to persons age 16 or older who experienced one or more incidents of DV, defined as rape or sexual assault, robbery, aggravated assault, or simple assault (including threats of harm or abuse), perpetrated by a relative or an intimate partner (current or former romantic partner or spouse). 1 The unweighted sample size for 2017–2019 was 1,308 victims, with 1,211 identifying as straight, 32 as lesbian or gay, and 65 identifying as bisexual. Survey weights were applied to account for nonresponse and to weight the sample to known U.S. population totals from the American Community Survey.
The BJS changed survey procedures in the second half of 2019 to only ask the sexual orientation question of victims rather than all respondents. Thus, to calculate rates of DV victimization, data from 2017, 2018, and the first half of 2019 (weighted to reflect the full population of the U.S.) were used to estimate the population of persons identifying as lesbian or gay, bisexual, or straight. Based on weighted data, 94.9% of the population from 2017 through the first half of 2019 identified as straight, 1.3% as lesbian or gay, 0.7% as bisexual, and 3.0% had an unknown sexual orientation. The full years of data for 2017 through 2019 were used for calculating the numerator for rates and for all analyses focusing on victimization, victim characteristics, and HS behaviors.
Variables
Dependent Variables
The NCVS includes several measures that tap into different dimensions of victim HS. Dependent variables for the analysis include whether the victim sought psychological care, got medical care, reported the victimization to police, or got help from a victim services agency or organization. Psychological care was measured through a question asking victims whether they sought professional or medical help for the feelings they experienced because of the crime. Victims were only asked this question if they reported experiencing negative feelings following the victimization for a month or more. Victims who skipped out of the question because they did not experience negative feelings for an extended period were coded as a “no” for seeking psychological care. Medical care was recoded as a yes/no variable reflecting whether the victim received care at the scene, a first aid station, a doctor’s office or health clinic, an emergency room, a hospital, or other locations. Victims who were not injured or received explicitly informal treatment for injuries (e.g., self-care at home, treatment from a friend or neighbor) were coded as a “no.” The police notification variable focused on whether the victim, specifically, reported the victimization to the police. If the victimization came to the attention of police through other means (e.g., reported by someone else, police were already at the scene), the variable was coded as a “no” for the purpose of these analyses. Finally, victim services were measured by a question asking whether the victim received “help or advice from an office or agency—other than the police—that deals with victims of crime.”
Independent Variables
Sexual orientation, the primary variable of interest, was measured through a question asking respondents age 16 or older how they think of themselves. Response categories were “[lesbian or] gay; ” “straight, that is, not [lesbian or] gay; ” “bisexual; ” “something else; ” and “I don’t know the answer.” 2 Persons who responded with “something else,” “I don’t know the answer,” or who chose not to answer the question were excluded from the analysis. 3
Control Variables
Based on the literature, the models also included controls for incident characteristics and other demographic characteristics. These variables may condition one’s likelihood of engaging in HS behaviors, regardless of SM status, but are not of primary focus for the current analysis. Incident characteristics included whether the offender was a current or former intimate partner or a relative, whether the offender had a weapon, whether the victim was physically injured, whether there were bystanders present, and whether the victim believed the incident was a hate crime motivated by sexual orientation bias (Briones-Robinson et al., 2016; Felson et al., 1999; Felson & Pare, 2005; Langton et al., 2012). Demographic characteristics included sex, age, race/Hispanic origin, household income, urbanicity, marital status, education, and citizenship (Ackerman & Love, 2014; Baumer & Lauritsen, 2010; Bosick et al., 2012; Cho et al., 2021).
Analysis
Population and victimization weights were applied for all analyses to ensure that the sample reflected the age, gender, and racial composition of the U.S. population and to compensate for survey nonresponse and the NCVS’ address-based, stratified cluster sample design. Analyses were conducted using complex sample procedures to account for the sample design. Prior to computing estimates for this paper, the analytic approach and weights were used to produce estimates that replicated those generated by BJS. After first examining rates of DV per 1,000 people, the characteristics of DV victims, and rates of HS, Student’s t-tests were used to determine whether these rates and characteristics differed by sexual orientation. Next, separate multivariate logistic regression models were run for each of the HS behaviors. Each form of HS was regressed on sexual orientation, controlling for the demographic and incident characteristics. Standard errors and confidence intervals for rates of victimization and HS were generated using the NCVS generalized variance function parameters supplied by BJS, while confidence intervals for multivariate models were generated using direct variance estimation using Taylor series linearization.
Results
Domestic Violence Victimization Among Sexual Minority Individuals
Victimization rates per 1,000 people, 2017–2019.
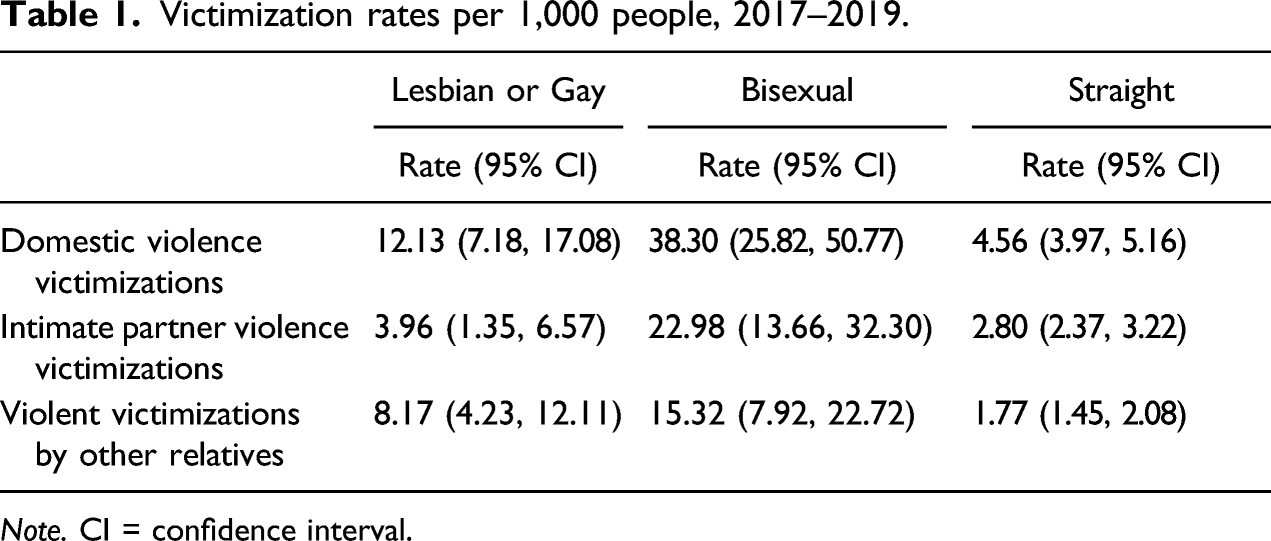
Note. CI = confidence interval.
Descriptive statistics for victimizations.

Notes. CI = confidence interval.
aPercentage should be interpreted with caution because the coefficient of variation is greater than 50%.
bPeople categorized as non-Hispanic other include American Indian and Alaska Natives; Asian, Native Hawaiian, and Other Pacific Islanders; and people of two or more races.
The vast majority of bisexual and straight victims were female rather than male. In contrast the distribution of males and females among lesbian and gay victims was not statistically significant. A larger percentage of lesbian and gay victims were victimized by relatives other than intimate partners, while bisexual and straight victims were more likely to be victimized by intimate partners. Bisexual victimizations were less likely to involve weapons and more likely to have a third party present compared to victimizations against straight victims. Lesbian and gay and bisexual victims were more likely than straight victims to believe the crime was motivated by bias because of their sexual orientation.
Formal Domestic Violence Help-Seeking Among Sexual Minority Individuals
Help-seeking behaviors.
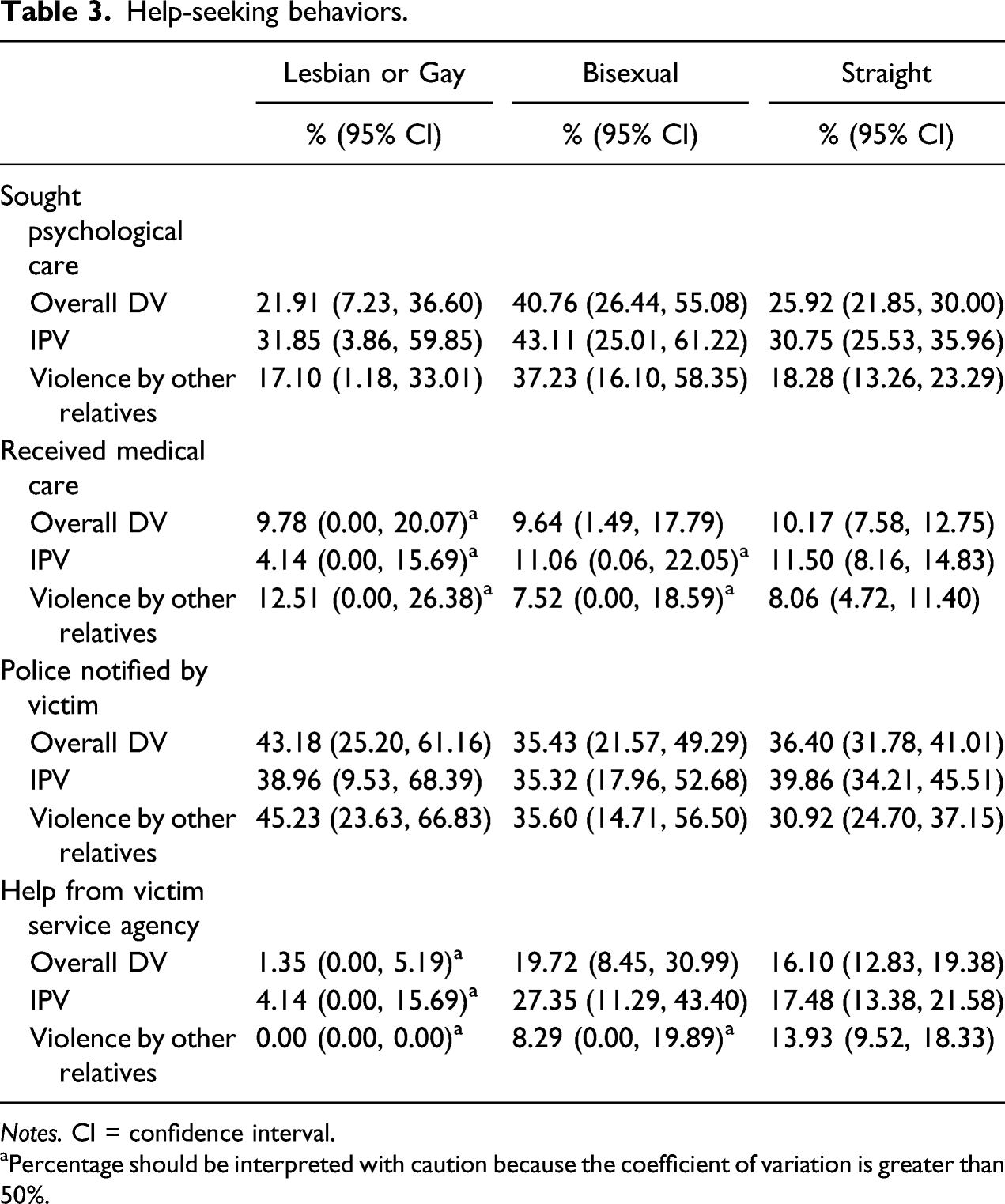
Notes. CI = confidence interval.
aPercentage should be interpreted with caution because the coefficient of variation is greater than 50%.
Factors Related to Formal Domestic Violence Help-Seeking
Logistic regression models predicting help-seeking behaviors.
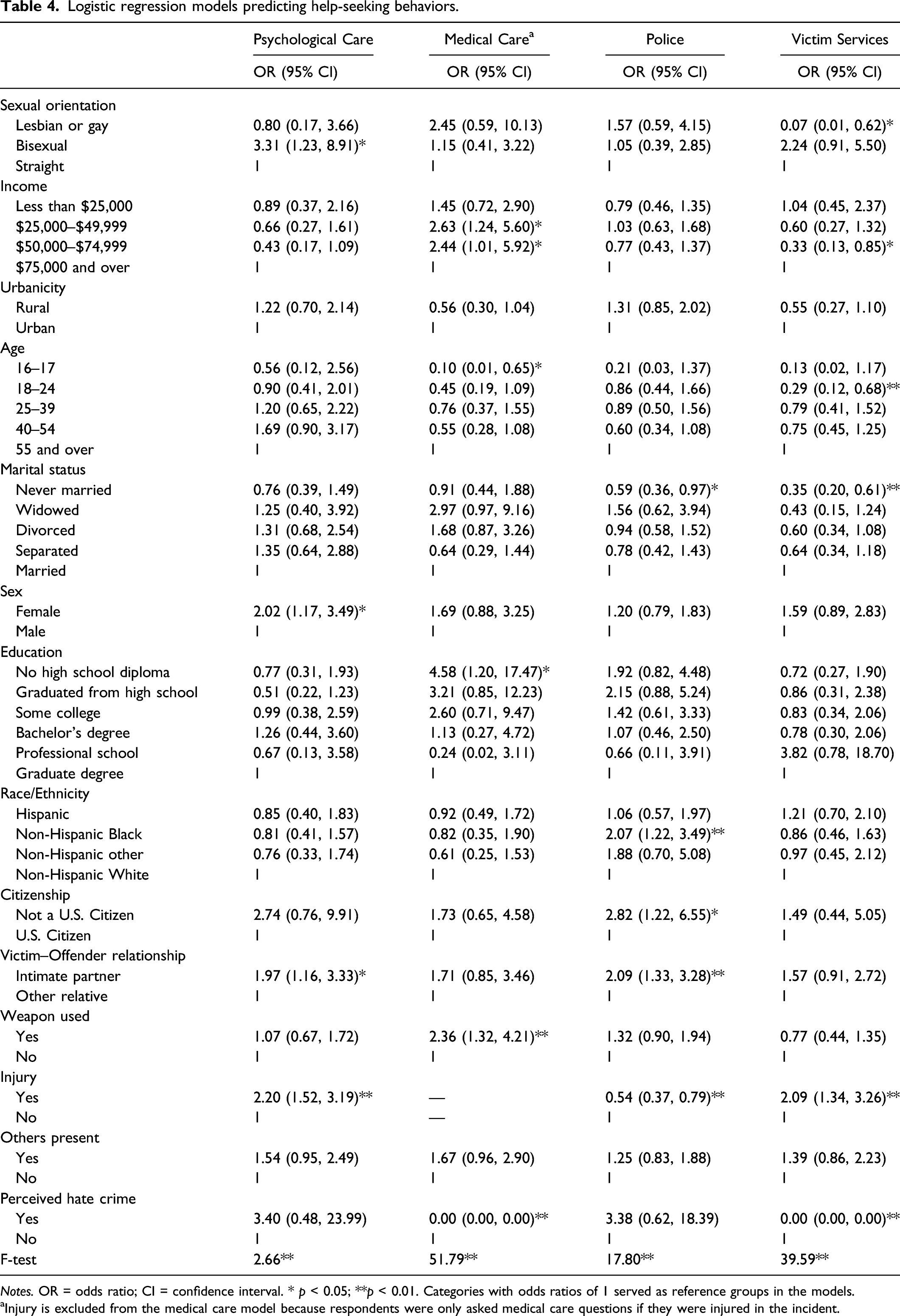
Notes. OR = odds ratio; CI = confidence interval. * p < 0.05; **p < 0.01. Categories with odds ratios of 1 served as reference groups in the models.
aInjury is excluded from the medical care model because respondents were only asked medical care questions if they were injured in the incident.
The odds of receiving medical care after a victimization did not differ significantly by sexual orientation. Victim characteristics significantly associated with getting medical care included income, age, and education. People with household incomes between $25,000 and $74,999 were more likely to get medical care than those with incomes of $75,000 and over, people under 18 were less likely to get medical care than people 55 and over, and people without a high school diploma were more likely to get medical care than those with graduate degrees. Regarding incident characteristics, when a weapon was used the victim was more likely to receive medical care. In contrast, when the victim perceived the attack as a hate crime, they were less likely to receive medical care.
Sexual orientation was also not a significant predictor of whether the victim notified the police. NH Black victims were more likely to notify the police than NH White victims, with the odds for reporting to the police for Black victims being 2.07 times higher than for White victims. Victims who had never been married were less likely to contact the police than married victims. Surprisingly, non-citizens were more likely to notify the police than citizens. Regardless of sexual orientation, the odds of a victim notifying the police were 2.09 times higher when the offender was an intimate partner compared to when the offender was a relative. Injured victims were less likely to notify the police themselves than those who did not suffer an injury.
The multivariate model predicting receiving help from a victim services agency revealed that lesbian and gay victims were less likely to receive help than bisexual and straight victims. This is consistent with the t-tests comparing help received by victim services agencies across sexual orientation groups. Victims with household incomes between $50,000 and $74,999 were less likely to receive help from a victim services agency than those with incomes of $75,000 and over. Younger victims in the 18–24 age group were less likely to receive help from a victim service agency than victims 55 and older. Victims who had never been married were also less likely to receive help from a victim services agency than married victims. Victims who suffered an injury were more likely to receive help from a victim services agency than those who did not, while victims who perceived the attack as a hate crime were less likely to receive help than those who did not.
Discussion and Conclusion
Despite the fact that more attention has been paid to rates and correlates of DV victimization among SM victims in recent years, this population continues to remain overlooked in DV policy and practice (Donovan & Barnes, 2020). The results from the current study provide new insight about rates and characteristics of DV among gay, lesbian, bisexual, and straight individuals, as well as factors related to DV HS among SM victims.
The first research question inquired as to whether rates and characteristics of DV victimization vary according to sexual orientation. The findings revealed that rates of DV are higher among SM victims compared to straight victims. Of particular importance, bisexual victims had a dramatically higher rate of DV that was three times higher than that of lesbian and gay victims and eight times higher than that of straight victims. Bisexual rates of victimization by other relatives, specifically, were also the highest, although a larger percentage of lesbian and gay DV victimizations were committed by other relatives than intimate partners compared to the other two groups. These results are consistent with findings reported by Walters et al. (2013) and Bender and Lauritsen (2021), who found that rates of DV were highest among male and female bisexual victims compared to male and female gay, lesbian, and straight victims. Our findings reinforce the notion that studies looking at victimization among sexual minorities should seek to understand the unique experiences of bisexual victims rather than grouping all SM victims into a single category.
The second research question focused on whether there is a relationship between DV HS behaviors and sexual orientation. Based on the findings from this study, bisexual victims were more likely to seek psychological care after a victimization, while lesbian and gay victims were less likely to receive help from a victim services agency. These findings are consistent with results from previous research indicating that when SM victims seek formal sources of support, they are more likely to pursue discrete, private HS sources such as mental health professionals (Hardesty et al., 2011; Santoniccolo et al., 2021). The findings could be attributed to the fact that a larger percentage of lesbian and gay DV victims were male, and males traditionally have fewer options for accessing victim services. Lesbian and gay victims may also be less likely to seek help from a victim services agency due to heteronormativity, real or perceived, in those spaces (Turell & Herrmann, 2008). This suggests that victim service providers continue to have work to do to ensure that services are inclusive and that outreach efforts target SM communities that experience high rates of victimization but are less likely to seek formal sources of help.
Significant differences were not found across groups regarding notifying the police or seeking medical care, which supports previous findings reported by Kuehnle and Sullivan (2003) and Flores et al. (2020). Medical providers and law enforcement officers can be important conduits for information and access to community resources for victims, and these findings suggest that this role is particularly important for SM DV victims who may be hesitant to independently seek other formal sources of help.
The final research question examined whether individual or incident level factors explain HS behaviors among straight and LGB DV victims. While sexual orientation was significantly related to seeking psychological care and help from a victim services agency net of other factors, there were no factors that consistently predicted behavior across the different types of formal HS. For example, the offender being an intimate partner increased the likelihood that the victim sought psychological care and reported to the police, but it was not related to seeking medical care or victim services. Consistent with prior research, being injured during the victimization increased the likelihood of HS through medical care and victim services (Santoniccolo et al., 2021). Injuries, however, decreased the likelihood of reporting to the police, which may be due to the injury preventing them from contacting the police or medical professionals contacting the police for them if they received medical care. Consistent with previous NCVS research on police notification of domestic and intimate partner violence, NH Black victims were more likely to notify the police than NH White victims (Ackerman & Love, 2014; Baumer & Lauritsen, 2010), which again suggests that law enforcement officers have an important role to play in helping to connect DV victims with other sources of help. However, race/ethnicity was not related to the other types of HS.
These results speak to the fact that the formal types of HS studied here are not the same. Decisions to seek psychological or medical care are likely influenced by financial resources and health insurance coverage, while decisions to access victim services are likely influenced by the availability of services and the victim’s perception of how they would be treated by representatives of the criminal justice system and other service-providing agencies. Although the current study was limited in its ability to do so due to small sample sizes when subsetting the data, examining DV HS behaviors among SM victims from an intersectional framework would consider power dynamics among partners and propensities towards violence that may be impacted by the intersection of sexual orientation, gender identity, ethnicity, race, socioeconomic status, and relationship status (see Parry & O'Neal, 2015). Transgender victims of DV, in particular, may have unique HS experiences given additional barriers they face compared to cisgender victims of DV. For example, transgender DV victims often face barriers related to transphobia and are less likely to seek help from formal sources of support that can provide them with the most beneficial resources and services (Kurdyla et al., 2019; Messinger et al., 2022). Additionally, for SM victims who are also members of marginalized racial and ethnic minority communities, the physical and mental health consequences of DV by an intimate partner can be particularly dire due to the intersections of homophobia, transphobia, racism, and sexism (Miller et al., 2016). Recognizing one’s many facets of identity contributes to an understanding of an individual’s multiple circumstances (Crenshaw, 1991).
The small unweighted sample sizes in the current study meant that it was not possible to sufficiently examine specific types of DV individually perpetrated by a relative or intimate partner. Prior research suggests that consequences of DV vary according to the type of victimization experienced (e.g., Basile et al., 2004), which can subsequently impact HS behavior (Flicker et al., 2011). Although the current study was unable to fully examine unique relationships between sexual orientation, specific types of DV victimization, and HS behavior due to methodological limitations, future research should examine whether the victim–offender relationship moderates the association between HS and sexual orientation in a multivariate analysis. Additionally, the current study was limited by measures of DV captured through the NCVS items. For example, the NCVS’s measure of psychological abuse is limited and primarily captures threats of physical harm or damage to property and not other types of coercive control, like name-calling and forcing financial dependence and isolation (Stark, 2013). A unique type of psychological abuse experienced by SM victims is referred to as “identity abuse.” Identity abuse involves “targeting, discrediting, belittling, and devaluing of a partner’s already-stigmatized identity” (Scheer et al., 2020, p. 142). For example, a common form of identity abuse includes threats made to “out” their partner to friends, family, and employers. The NCVS, however, does not specifically capture this aspect of psychological abuse.
Another limitation of this study is the measure of psychological care, which was only asked if the victim experienced distress for a month after the victimization. Psychological care could potentially be underestimated as a result. Additionally, this study was limited in its ability to generalize to the population on certain measures of HS. A strength of the NCVS is that it is nationally representative, allowing researchers to generalize their results. However, cell sizes quickly shrink when examining specific domains of victimization given that crime is already a relatively rare event, which can make generalization harder. For example, when looking at unweighted sample sizes, one lesbian or gay victim sought help from a victim services agency. While it is difficult to generalize that finding to all lesbian and gay DV victims in the population despite the sampling design, this seems to be a meaningful finding within the NCVS sample as the remaining 31 lesbian and gay victims did not seek help from a victim services agency.
Despite these limitations, findings from this study fill a gap in existing research regarding the impact of sexual orientation on formal HS among DV victims in several ways. First, these results use data from a large, nationally representative survey to enhance existing research suggesting that DV among SM populations is higher than DV experienced by non-SM populations. Next, this study contributes to the literature by operationalizing DV broadly to include violence between all family members in addition to intimate partners, since the majority of research examining HS among SM populations focuses on DV among intimate partners only. Additionally, the current results add to the literature by highlighting different experiences with DV and HS between those identifying as lesbian or gay versus bisexual. Finally, these results contribute to knowledge about four types of formal HS among SM populations while utilizing a nationally representative sample.
Directions for future research should include a focus on DV that occurs between family members in addition to intimate partners. While other relatives are often considered in rates of DV and as a comparison to intimate partners (e.g., Felson & Pare, 2005; Morgan & Truman, 2020), research on the theoretical mechanisms influencing violence between adult siblings and parental abuse of adult children is rare. This area of research may be particularly salient for adult SM DV victims given previous findings that SM individuals experience more sibling violence, child abuse, and parental rejection due to their sexual orientation (Friedman et al., 2011; Martinez & McDonald, 2021; Richter et al., 2017). Future studies should also consider whether the specific type of violence (i.e., sexual violence vs. other physical violence) experienced influences SM HS behaviors, as the type may vary by sexual orientation and HS can vary based on the type (Morgan & Truman, 2020). While the NCVS cannot fully capture the experiences of people with sexual identities outside of those studied here, future research should explore DV and HS behaviors among other non-heterosexual identities. It is important to continue examining the HS process among SM victims of DV in order to develop appropriate policy responses and provide services needed by this population. Understanding factors that are related to all survivors’ decisions to seek help is important for community-level service-providing agencies, medical and health providers, and practitioners in the criminal justice system for the provision of accessible services that encourage HS among victims.
Footnotes
Acknowledgments
The authors would like to thank the anonymous reviewers for their constructive and thoughtful feedback.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.