
Abstract
Study Questions: People who identify as same-sex attracted (SSA) face significantly greater risk for victimization than their non-SSA counterparts. However, little distinction is made between single versus recurring victimization among the SSA population. There are no national prevalence estimates, and we do not know the extent to which disproportionate risk of victimization among SSA populations applies to recurring victimization versus single occurrences. Subjects: We analyze data from 483 survey respondents who reported same-sex attraction and 8544 respondents who do not report SSA. Methods: The current study utilizes a nationally representative sample to estimate the prevalence of single and recurring victimization among SSA populations, and compare these estimates with those found in the non-SSA population. We further investigate some possible mediating processes that may explain differences between these groups in risk for recurring victimization, drawing upon lifestyles, self-control, and minority stress frameworks. Findings indicate that SSA groups have significantly greater risk for both single and recurring physical assault victimization. Much of the disproportionate recurring victimization risk can be explained by differences in both risky lifestyles and low self-control, as well as minority stress. Implications: Recurring victimization is an important problem for SSA individuals. Prevention efforts may focus on school contexts, including the addition of Gay-Straight alliances, creating supporting peer groups, and providing supportive adult role models.
Introduction
Research indicates that same-sex attracted (SSA) individuals faced increased risk of victimization (Balsam et al., 2005; Russell et al., 2001). Among youth, Russell et al. (2001) found that sexual minorities had significantly higher odds of requiring medical care as a result of violence, experiencing a violent attack, and being jumped. Similarly, a meta-analysis reported that sexual minorities were on average 1.2 to 3.8 times more likely than heterosexuals to experience victimization, including sexual abuse, parental physical abuse, assault at school, and missing school through fear (Friedman et al., 2011). In a systematic review of 32 empirical studies, McGeough and Sterzing (2018) concluded that rates of childhood physical, sexual, and emotional abuse were consistently higher for sexual minority youth than among heterosexual peers 1 .
The consistency of such findings across studies raises important questions for scholarly inquiry. First, while SSA status seems to be a risk factor for victimization, we do not know if and how sexuality may be related to recurrent physical assault victimization risk. That is, we have yet to determine nationwide prevalence estimates of recurring physical assault victimization among SSA youth in the U.S. Second, although studies have found high rates of victimization among sexual minorities, we have yet to explain the mechanisms through which SSA leads to differential victimization rates, particularly with regard to potential recurrent victimization patterns.
The current study empirically examines these questions using a nationally representative sample of SSA and non-SSA attracted individuals drawn from the National Longitudinal Study of Adolescent to Adult Health (Add Health). Drawing on two popular victimization frameworks, lifestyles and self-control, and informed by minority stress theory, we consider some possible ways in which SSA may be related to both single and recurring physical assault victimization. We examine if the prevalence of risky lifestyle characteristics differs between SSA and non-SSA youth, and how lifestyle characteristics may repeatedly place same-sex attracted individuals at higher victimization risk. We also examine the extent to which higher rates of victimization and recurring victimization among same-sex attracted youth can be explained by differences in self-control and experiences of minority stress.
Literature Review
Studies consistently report that sexual minorities have higher rates of victimization compared to their peers. For example, Balsam et al. (2005) found that the risk of childhood sexual assault, intimate partner violence, and rape were all significantly higher for Gay, Lesbian, and Bisexual (GLB) individuals than heterosexuals. Hughes et al. (2010) determined that lesbian/bisexual women had twice the prevalence of lifetime victimization compared with heterosexual women. Similarly, gay men had almost twice the lifetime prevalence of victimization compared with heterosexual men (Hughes et al., 2010). Much of the existing work has focused on single-event victimization among sexual minority-identified persons. Less is known about recurring victimization, especially among those who are same-sex attracted but not necessarily identified as gay, lesbian, or bisexual.
A handful of peer-reviewed studies examine recurring victimization among GLB groups; these works provide insight regarding what one may expect among SSA versus non-SSA comparisons. For example, using a non-probability sample, Heidt et al. (2005) found that 40% of GLB individuals reported sexual revictimization. In addition, Hughes et al. (2010) found that 38.2% of lesbians and 27.1% of gay men reported two or more victimizations over their lifetime, using data from a nationally representative sample of adults. This compares to 10.7% of heterosexual women and 8.7% of heterosexual men. Such findings suggest that SSA individuals would not only face higher risk of single-event victimization, but may be more likely to experience recurring victimization as well. However, currently we know of no published national prevalence estimates that specifically compare SSA/non-SSA populations with regard to single and recurring victimization. Thus, we do not know the extent to which patterns revealed in prior studies hold amongst those who report SSA, but may not identify as gay or lesbian. Moreover, to date no published work has tested criminological explanations for differences in both single and recurring victimization risk across SSA-status. Should national prevalence provide evidence that SSA populations are at higher risk for both single and recurring victimization, how might criminologists explain such disparities, and would such theories bear out via empirical investigation?
Lifestyles Theory
Lifestyles theory suggests that the patterns of behavior that make up a person’s lifestyle differentially expose some people and not others to risks for victimization (Hindelang et al., 1978). A number of empirical studies have supported the impact of risky lifestyles on victimization (Cohen & Cantor, 1980; 1981; Cohen et al., 1981; Hough, 1987; Messner & Blau, 1987; Miethe et al., 1987). Miethe et al. (1990), for example, find a significant relationship between changes in nighttime activities, household guardians, limiting activities, and avoiding dangerous places and both personal and property victimization. Miethe and Meier (1990) find that engaging in dangerous activities significantly increased the odds of both violent and burglary victimization, while taking safety precautions significantly decreased the odds of burglary victimization.
Hindelang et al. (1978) argue that both ascribed and achieved statuses are important indicators of victimization risk, because they may lead to different consistent behavioral patterns, or lifestyles. In the context of the current study, this means that same-sex attracted individuals may routinely engage in different behavioral patterns than their non-SSA peers. This difference in lifestyle may confer more risk for recurring victimization for same-sex attracted individuals. Indeed, they acknowledge structural constraints (economic, familial, etc.) as causal players in the creation of individual and subcultural adaptations that lead to lifestyles. Putting this into the context of the current study, the economic and familial challenges of being a same-sex attracted youth may differentially expose these youth to riskier lifestyles, such as prostitution, running away from home, and substance abuse. These risky lifestyles, in turn, may increase the risks for victimization and recurring victimization.
Self-Control Theory
Originally used to explain differences in offending behavior, Gottfredson and Hirschi’s (1990) self-control theory has since also been conceptualized as a theory of vulnerability (Schreck, 1999). That is, over the last two decades, victimization researchers have paid increasing attention to the idea that people with low self-control self-select into risky lifestyles; these various risky behaviors, in turn, increase their risk of victimization. Self-control theory is helpful for explaining the “victim-offender overlap.” Research consistently finds a correlation between offending and victimization, in that victims and offenders frequently share social and personal characteristics (Gottfredson & Hirschi, 1990; although this is not always the case, see Bachman, 1994; Jennings et al., 2012; McHugh & Frieze, 2006; Widom, 1989).
Numerous studies test whether low self-control increases one’s risk of property and violent victimization (for some examples, see: Holtfreter et al., 2008; Piquero et al., 2005; Schreck et al., 2012; Schreck et al., 2006). In a recent meta-analysis of 66 empirical studies from 1995 to 2013, Pratt et al. (2014) found that self-control is a “modest, yet consistent” predictor of victimization (2014; 87). However, the effect of self-control was significantly smaller among studies that control directly the risky behaviors assumed to mediate the self-control victimization link. Placing this into the context of SSA, it is possible that due to the struggles SSA youth have with their families of origin, they may develop lower levels of self-control (on average) or higher involvement in risky behaviors than non-SSA youth, due to differential socialization practices in families.
Minority Stress
Minority stress theory posits that marginalized people experience more chronic stressors including stigma, prejudice, isolation, discrimination, and internalized homophobia. Toxic home or school environments undermine the critical social support, guidance, and protection required for healthy development. If SSA on average does have more experiences of discrimination and stress and these experiences are linked to victimization and recurring victimization, then SSA may be more at risk for recurring victimization than non-SSA youth due to these differences in stressful experiences. It is also important to note that rejection and exclusion could force SSA youth into dangerous situations, increasing their participation in risky lifestyles in their efforts to survive. Disproportionate exposure to such chronic stresses may not only lead to differences in self-control and risky lifestyles, but make them particularly vulnerable targets for victimization.
The Current Study
In this study, we examine the rates of single and recurring victimization for both SSA and non-SSA youth in a nationally representative sample. We test whether rates of single and recurring victimization differ significantly across these two groups and whether variables measuring minority stress, risky lifestyles and low self-control mediate any group-based differences in the experience of victimization. Specifically, we hypothesize that SSA will have higher rates of recurring victimization relative to their non-SSA peers. Furthermore, we expect that this association will be at least partially explained by risky lifestyles, self-control, and minority stress. To our knowledge, this is the first study to present national prevalence estimates of recurring victimization for SSA youth and to provide an empirical examination of why SSA might have higher rates of single and recurring victimization drawing on two prominent theories of victimization and minority stress theory. We do so by analyzing data from the National Longitudinal Study of Adolescent to Adult Health (Add Health).
Data and Methods
The data for this project come from the National Longitudinal Study of Adolescent to Adult Health (Add Health). Add Health is a nationally representative, longitudinal study of adolescents in middle and high school as they transition into adulthood. The first wave of data was collected in 1995, when the respondents were in 7th through 12th grades. Wave 4, the final wave used in this project was collected in 2008, approximately 13 years after the initial data collection.
The sample was collected utilizing a clustered probability sampling strategy, where schools were first stratified by region and then selected for inclusion. Approximately 80 high schools and 52 middle schools from the U.S. were selected. After that, students were stratified by year in school, and sex, and a random sample within each stratum was conducted so that approximately 200 adolescents were selected from each middle school—high school pair. This resulted in approximately 12,000 adolescents in the core in-home sample. In addition to this, special oversamples were conducted for well-educated black families, Chinese, Cuban, and Puerto Rican students. Sixteen schools were selected for the saturated schools sample, which included all students in those schools, for the purpose of social network analysis. Twin pairs were included for genetic studies. All of this resulted in an in-home wave 1 sample of over 20,000 respondents. For this project, we utilize, the 8937 respondents who provided data on the outcome variable, which encompassed all fours waves, as well as all of the independent variables, which were measured at wave 1.
Measures
The dependent variable for our analyses is a multi-category nominal variable which represents physical assault victimization over time. Respondents were classified as non-victims if they reported no victimization at any wave. They were classified as single-victims if they reported victimization in only one of the four waves, and as recurring victims if they reported victimization in more than one of the waves. Victimization was defined by questions in the waves 1–4 surveys, which asked “During the past 12 months, how often did each of the following things happen?” This included “Someone pulled a knife or gun on you,” “Someone shot you,” “Someone cut or stabbed you,” and “You were jumped.” Responses were collapsed so that an affirmative response to any item represented victimization for that wave.
Our key independent variable was any same-sex romantic attraction (SSA). Consistent with prior research (for example, see Teasdale & Bradley-Engen, 2010), SSA was measured at Wave 1 based on two items which asked “Have you ever had a romantic attraction to a female?” and “Have you ever had a romantic attraction to a male?.” Female respondents who said yes to the female question and male respondents who said yes to the male question were coded as 1 = SSA. Male respondents who said no to the male attraction item and female respondents who said no to the female attraction item were coded as 0. Respondents who said yes to both items were also coded 1. 2
In order to test our mediation model, we examine a series of variables derived from the lifestyles perspective. Those include risky sex (including sexual trade/services and number of sexual partners), running away from home, drug use, and alcohol use. In addition, we examine low self-control and minority stress covariates as rival mediational processes.
Risky sexual activities are measured using two variables. The first measures sold/traded sexual services. This is captured by a single item that asks “Have you ever given someone sex in exchange for drugs or money?” The responses are coded 1 for yes and 0 for no. We also measure number of sexual partners. This is captured by responses to the following question: “With how many people, in total, including romantic relationship partners, have you ever had a sexual relationship?” Responses were open-ended and ranged from 1 to 187 people.
Running away from home was a single item that asked respondents “Over the past 12 months, how often did you run away from home?” Response options were collapsed so that 0 is never and 1 is at least once in the past year.
Drug use was captured by a dichotomous indicator (1 = yes) of any past month drug use. This was based on any affirmative response to questions about past month use of marijuana, cocaine, inhalants (such as glue or solvents), illegal drugs (such as LSD, PCP, ecstasy, mushrooms, speed, ice, heroine, or pills without a doctor’s prescription).
Alcohol use was measured based on responses to the question “During the past 12 months, on how many days did you drink alcohol?” Response options included Never (0), 1 or 2 days in the past year (1), once a month or less (2), 2 or 3 days a month (3), 1 or 2 days a week (4), 3–5 days a week (5), and every day or almost every day (6).
Our self-control measure is consistent with those commonly identified in the existing literature. This specific measure has been utilized in prior studies, capturing possible behavioral, attitudinal, and/or cognitive elements of low self-control (see Perrone et al., 2004). Specifically we relied on responses to four questionnaire items. Respondents were asked “Since school started this year, how often have you had trouble: (1) getting along with your teachers?; (2) paying attention in school; and (3) getting your homework done?)” Response options were coded as 0 = never, 1 = just a few times, 2 = about once a week, 3 = almost everyday, and 4 = everyday. We included an additional item that asked: “How often the following things were true during the past week: You had trouble keeping your mind on what you were doing?” Response options were coded as 0=never or rarely, 1 = sometimes, 2 = a lot of the time, and 3 = most of the time or all of the time. Cronbach’s alpha indicated acceptable reliability (alpha = .68). Thus, the four items were summed to create the indicator of low self-control. 3
Minority stress was operationalized using two items. The first question asked respondents “Before your 18th birthday, how often did a parent or other adult caregiver say things that really hurt your feelings or made you feel like you were not wanted or loved?” Response options ranged from “this has never happened” (0) to more than 10 times (5). In addition, respondents were asked “In your day-to-day life, how often do you feel you have been treated with less respect or courtesy than other people?” Response options ranged from “never” (0) to “often” (3).
Finally, we include control variables for respondents’ sex (1 = female), age at wave 1 (years since birth), and race/ethnicity, which is a series of dummy variables Black, Latino, and Other versus the omitted reference category of White.
Data Analysis
Since the Add Health sampling plan involves a clustered sampling strategy with unequal probabilities of selection, we conduct design-adjusted analyses using the svyset commands in Stata (version 15.0) and for the indirect effects calculations in Mplus, correcting for weights, clustering, and stratification. The analyses are conducted via design-adjusted multinomial logistic regressions to take into account the multi-category nominal nature of our dependent variable. In addition, Mplus uses the delta method of standard error computation for the indirect effects.
Results
Descriptive Statistics (n = 8937).

Bivariate Association between Recurring Victimization and Same-sex attraction (n = 8937).
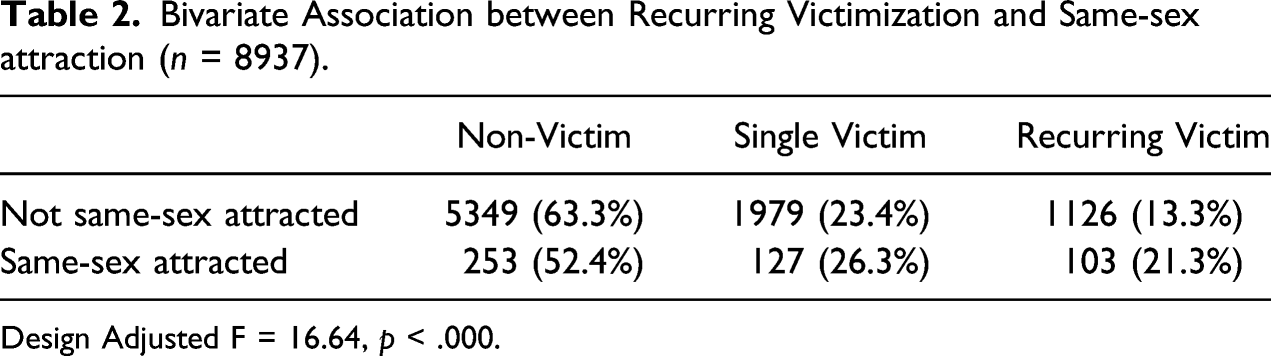
Design Adjusted F = 16.64, p < .000.
Multinomial Logistic Regression (n = 8937).
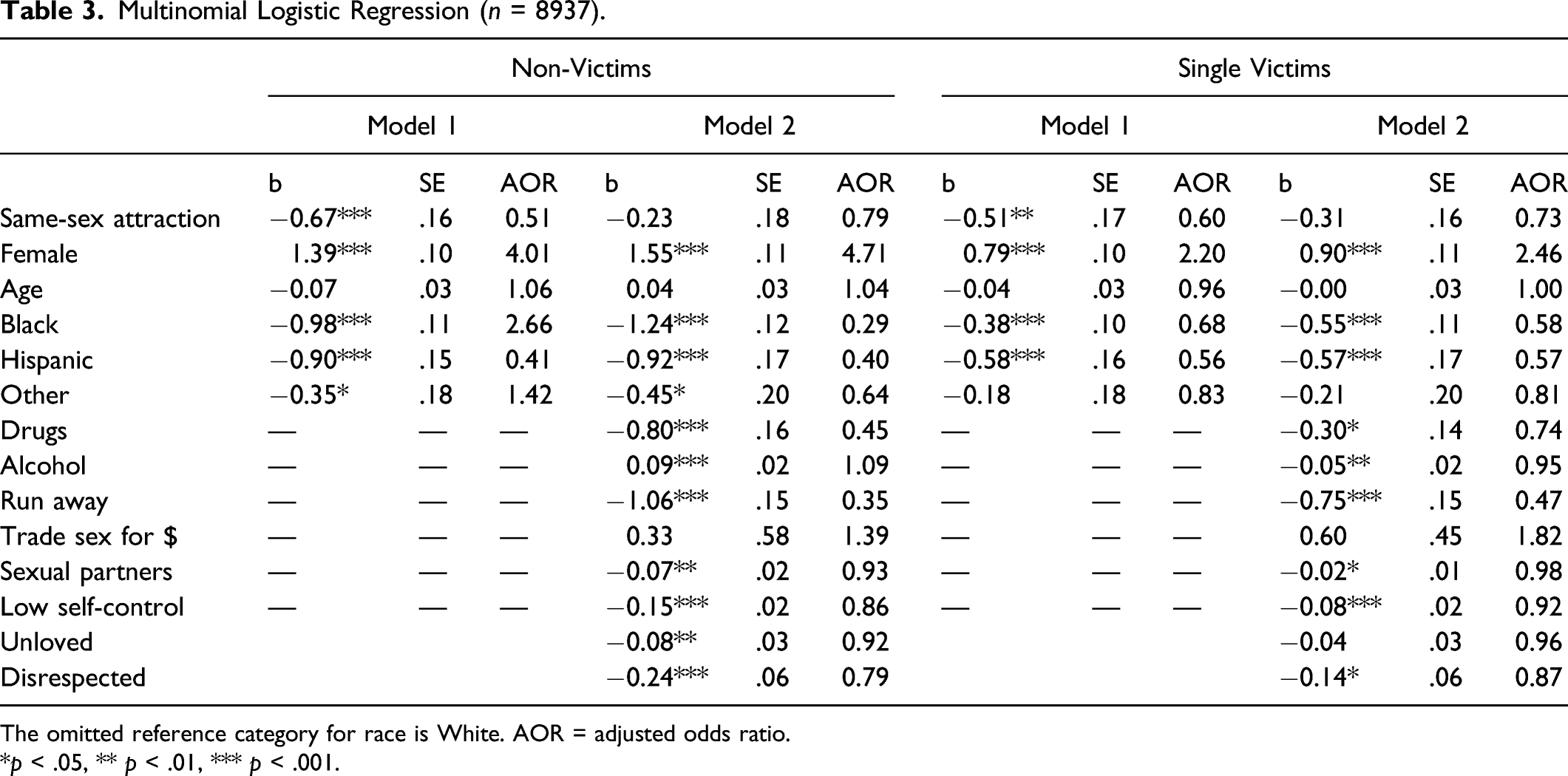
The omitted reference category for race is White. AOR = adjusted odds ratio.
*p < .05, ** p < .01, *** p < .001.
As shown in Model 2 of Table 3, several of our lifestyles and minority stress measures were significantly associated with recurring victimization. Those who used drugs, drank alcohol more frequently, ran away from home, or had a higher number of sexual partners had significantly higher odds of being in the recurring victims category than either the non- or single-victim categories. In addition, those with lower levels of self-control had significantly higher odds of being in the recurring victims category than either the non-victims or the single-victims category. Minority stress also significantly correlated with being a non-victim and a single victim. Feeling disrespected significantly increased the odds of being in the recurring victims category compared to both non-victims and single victims. Feeling unloved also significantly increased the odds of being in the recurring victims category, compared to the non-victims category. Finally, the effects of being same-sex attracted on non-victim and single-victim were both reduced in magnitude and to non-significance, once we entered mediators into the model. Specifically, the effect of same-sex attraction on non-victim reduced by 66% and the effect of same-sex attraction on single-victim reduced by 40%. This indicates substantial mediation by the included variables for both levels of the outcome, as opposed to recurring victimization, the reference category.
Next, we tested for indirect effects in Mplus. In the non-victim versus recurring model, significant indirect effects of same-sex attraction were found through: self-control (IE = .037, p < .000), alcohol use (IE = .013, p = .002), number of sexual partners (IE = .018, p < .000), running away from home (IE = .047, p < .000), drug use (IE = .043, p < .000), exchanging sex for money or drugs (IE = .033, p = .032), and feeling unloved (IE = .008, p = .002). The above reported indirect effects are standardized. Thus, the largest indirect effects were through running away from home and drug use. In the single-victim versus recurring model, significant indirect effects of same-sex attraction were found through: self-control (IE = .021, p < .000), running away from home (IE = .037, p = .001), and drug use (IE = .028, p = .001). Here too, we find that the largest standardized indirect effects are through running away from home and drug use.
Conclusions
To our knowledge, this study provides one of the first prevalence estimates for recurring victimization across SSA versus Non-SSA individuals based on nationally representative data. We find that risk for recurring victimization is twice as high among same-sex attracted individuals than for those reporting opposite-sex attraction. This disparity is alarming. In a relatively short period of the life-course, using a conservative measure of recurring victimization, we project that one in four same-sex attracted individuals will experience recurring victimization. Our findings suggest that it is critical for social scientists to find ways to prevent and address victimization among this highly vulnerable population.
Victimological theory previously used to explain differences in victimization rates among other groups was applicable for this group as well. That we can explain differences in risk for victimization utilizing traditional victimology theory is promising. Specifically, we find that much of the increased risk among SSA populations is rooted in differences in risky lifestyles. We identify key features that are more common amongst same-sex attracted individuals, such as running away from home, risky sexual activities, and substance use that disproportionately place sexual minorities at risk for recurring victimization, compared to their non-SSA peers. These risk factors require intervention, if we are to reduce the recurring victimization burden of this population.
To be clear, our empirical explanation is in no way meant to victim-blame. Rather, we argue that the adverse experiences and conditions to which SSA youth are subjected may be the real culprit here. Researchers should explore how the circumstances in which populations are situated directly and indirectly increase their vulnerability. For example, a negative school environment may lead people to engage in antisocial behavior (Teasdale & Bradley, 2020), which subsequently places people at increased risk for victimization. Expanding victimological explorations to include minority stress and other theoretical frameworks can provide valuable insight. Our minority stress measures, particularly feeling unloved, were important influences victimization risk. Future studies should explore the possibility that the association between minority stress and victimization may be mediated by risky lifestyles and low-self-control. This could shed light on how structural constraints of LGBT life and culture may be responses to exclusion, rejection, and discrimination, and how these responses may increase risk for on-going victimization. We suggest that SSA adolescents may be more likely to engage in risk-taking behavior due to the adverse circumstances in which they live (i.e., they are more likely to run away because their homes are more likely to be places people want to run away from). It is a precarious situation, to flee or be rejected from conventional family, school, and peer groups, only to turn to risky behavior to survive.
Thus, it is critical that schools and communities create appropriate interventions and alternative solutions to the adverse structural conditions that have given rise to this risk-taking. Pro-social peer support networks, adult mentoring, student groups, sensitivity training and education and other programs and activities targeting SSA and LGBTQIA groups could provide effective, safe alternatives to prevent the adoption of lifestyle behaviors that put SSA youth at risk for recurring victimization. Improving the school environment and fairness of school policies and practices, anti-bullying policies, and other efforts to reduce the pains of LGBTQIA youth and other stigmatized groups may directly reduce their need to seek out risky coping strategies.
There is empirical support for these approaches. Specifically, Kosciw et al. (2013) provide evidence that supportive school environments can buffer the negative experiences that LGBT students have at school. They found that supportive staff members and Gay-Straight alliances both reduced the harmful effects of victimization on missed school days. They also found LGBT inclusive curriculum can buffer the harmful effects of victimization on self-esteem. Moreover, supportive staff members and a comprehensive anti-bullying/harassment policy both have independent main effects, promoting higher self-esteem amongst LGBT identified youth. Supportive staff members and LGBT inclusive curriculum both increase GPA and reduce missed school days. Finally, they found that a comprehensive anti-bulling/harassment policy significantly increases GPA and reduces missed school days for LGBT students.
Research consistently finds that the routine activities of those with low self-control often place them in close proximity to motivated offenders, and decreases their willingness to utilize appropriate guardianship strategies (for a review, see Pratt et al., 2014). Positive social support and school engagement may also reduce victimization risk among those with low-self-control by increasing their exposure to capable guardianship and decreasing their time spent with motivated offenders. Belonging and associating with prosocial peers and supportive others may also indirectly protect those with low self-control by discouraging or prohibiting risky behaviors and encouraging those with low self-control to self-regulate behavior that put them at risk for victimization.
Although there is the possibility of reverse causal ordering, we do not believe this is a central risk in our study. Same-sex attraction was measured prior to the onset of victimization, as were potential mediating mechanisms. The mediating mechanisms also likely occurred after individuals identified as same-sex attracted. Just as with all survey research, spuriousness is a potential concern; we cannot capture offender-related variables. Thus, we do not know if recurring victimization involves the same perpetrator over time or if the recurring victims are repeatedly encountering new offenders throughout life. This is not a trivial omission, since prevention implications may hinge on whether it is victim behavior or perpetrator behavior that is the driver of recurring victimization. This is a common shortcoming within much of the recurring victimization literature. In addition, there may be other mediators that might further explain the link between same-sex attraction and recurring victimization. Future studies should explore other potential mechanism through which SSA youth are disproportionately at risk for both singular and recurring victimization.
In spite of limitations, this study furthers our understanding of the recurring victimization experiences of same-sex attracted young people. We theorize and empirically investigate the processes that disproportionately lead same-sex attracted young people to recurring physical assault victimization, over time. It is our hope that this project stimulates additional research into the recurring victimization experiences of same-sex attracted youth.
Footnotes
Acknowledgments
Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. No direct support was received from grant P01-HD31921 for this analysis.
Data Availability
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill. Information on how to obtain the Add Health data files is available on the Add Health website (![]() ).
).