
Abstract
Violence against women is a serious public health and human rights concern and can take many forms. Intimate partner violence (IPV) is the subject of the majority of research focused on violence against women around the world; yet the health consequences of non-partner violence (NPV) can be just as serious. There is a critical gap in literature focused on NPV and the co-occurrence of NPV and IPV in sub-Saharan Africa, particularly in informal settlements. The unique historical, political, social, geo-spatial, physical, and built environment in informal settlements—often characterized as places with high rates of crime and violence—may be important in understanding NPV and co-occurrence of NPV and IPV in these communities, but more research is needed. The purpose of this study was to explore NPV in a large informal settlement in Nairobi, Kenya including its relationship to IPV, correlates, and common perpetrators of NPV in this setting. Data from 552 household-level surveys collected from women in a large informal settlement in Nairobi in 2018 were used in this study. Descriptive statistics and penalized maximum likelihood logistic regressions were used to examine the association between IPV and NPV, correlates, and perpetrators of NPV. Findings showed a strong, positive association between past-year IPV and NPV—highlighting a critical area for future study in IPV, NPV, and poly-victimization research. Results corroborated some findings from existing NPV research, but yielded important new information about correlates and perpetrators of NPV in informal settlements. NPV and poly-victimization have serious health consequences for women in any context, but women in informal settlements also face a number of structural economic, social, political, and environmental challenges that affect their health and wellbeing and may exacerbate the health consequences of violence perpetrated against them. Thus, more research into NPV and poly-victimization in informal settlements is critical.
Introduction
Violence against women is a serious public health and human rights concern and can take many forms. Intimate partner violence (IPV) is defined as violence by an intimate partner, and may include control tactics such as physical, sexual, psychological, or economic abuse (World Health Organization, 2021). IPV is the subject of the majority of research focused on violence against women around the world (Abrahams et al., 2014; Devries et al., 2013; Ebrahim, 2021; World Health Organization & Pan American Health Organization, 2012). Non-partner violence (NPV), defined as violence perpetrated by someone other than an intimate partner, including strangers, acquaintances, friends, colleagues, peers, teachers, neighbors, family members, etc., has received less attention in the literature (Abrahams et al., 2014), particularly in sub-Saharan Africa (Barchi & Winter, 2019; Muluneh et al., 2020). Similar to IPV, NPV can include physical (e.g., simple or aggravated assault), sexual (e.g., unwanted sexual contact, forced sex), psychological (e.g., stalking, harassment), or economic violence (e.g., theft, fraud) (Mercy et al., 2017). While there are some forms of NPV that are distinct from IPV (e.g., officer-involved shootings; gang violence; and hate crimes), most often, it is the perpetrator that separates acts of NPV from acts of IPV. In some instances, even motivations for the violence can be similar. For example, gender-based violence encompasses both IPV and NPV shaped by gender norms and power dynamics (Russo & Pirlott, 2006). The focus of this study is the association between IPV and physical and sexual NPV.
Globally, over 26% of women aged 15 years and older have experienced physical and/or sexual IPV and about 6% have experienced NPV in their lifetime (World Health Organization, 2021), but prevalence rates of violence are not evenly distributed. In Eastern sub-Saharan Africa, 38% of women aged 15 years and older have experienced IPV, while 6% have experienced NPV (World Health Organization, 2021). Although there is still limited research, a few studies also suggest that violence rates may be even higher in urban informal settlements in sub-Saharan Africa (Mathur et al., 2018; Swart, 2012; Winter et al., 2020).
While prevalence rates for NPV seem to be lower than for IPV, globally, research suggests that the health consequences of NPV are serious and the risk factors associated with NPV and IPV have a number of similarities and key differences that make studying NPV critically important (Abrahams et al., 2014). Research suggests, for example, that sexual NPV may be more violent and/or more likely to involve a weapon (Abrahams et al., 2014). The purpose of this study, therefore, was to explore correlates (e.g., risk and protective factors) of NPV, in particular, the association between IPV and NPV and the common perpetrators of NPV in informal settlements in Nairobi, Kenya.
General Correlates of Non-Partner Violence
Although there is limited research focused on NPV in sub-Saharan Africa, a few studies have explored correlates of NPV in African contexts. Ebrahim (2021), for example, applied an ecological lens to explore correlates of NPV in Ethiopia using Demographic and Health Surveys—finding that household wealth and asset ownership were important correlates of physical NPV. Malihi et al. (2021) found higher rates of physical and sexual NPV among men and women with disabilities. Other demographic or individual-level variables associated with NPV in different contexts have included age, education, marital status, having witnessed family members abuse women in childhood, family size, living in a female-headed household, and employment (Barchi & Winter, 2019; Ellsberg et al., 2020).
Some studies suggest that there are also behavioral factors associated with NPV. For example, there are several studies demonstrating associations between respondent and partner alcohol use and NPV for women in sub-Saharan Africa (Barchi & Winter, 2019; Pitpitan et al., 2013). Other research suggests that circumstances in one’s environment may influence NPV. Snyder et al. (2021), for example, suggest that circumstances in a person’s everyday routines/activities may expose or protect them from criminogenic/high risk situations and environments. While Snyder’s research focuses largely on college campus environments in the United States, literature from sub-Saharan African contexts suggests factors such as lack of access to water and sanitation in the environment can impact women’s risk of violence (Sommer et al., 2014; Sorenson et al., 2011; Winter et al., 2020). Some studies suggest that women who have to travel long distances from their homes to fetch water may be at higher risk of sexual and physical violence (Massey, 2011; Sommer et al., 2014). Using firewood for fuel instead of charcoal has also been associated NPV in South Sudanese contexts because it requires that women travel further away from their homes to acquire firewood (Ellsberg et al., 2020). NPV can also vary by geographic or urban-rural differences (Barchi & Winter, 2019). Bars and alcohol distribution centers have been highlighted as higher risk environments for sexual NPV, particularly in urban contexts (Pitpitan et al., 2013). Factors in the social environment, such as restrictive marital practices, gender norms, and community conflict can also be drivers of NPV (Ellsberg et al., 2020).
Finally, there is some indication in the literature that IPV is associated with NPV (Krebs et al., 2011). When these two types of violence are experienced concurrently or recurrently over time, this can be considered poly-victimization.
Poly-victimization
A point of inquiry in this current study was to explore associations between past-year IPV and NPV in informal settlements, that is, to explore the co-occurrence of one or more types of IPV and at least one type of NPV within the same year as a form of poly-victimization. Definitions of poly-victimization (sometimes referred to as multi-victimization) differ throughout the literature—sometimes referring to recurrent incidents of the same type of violence committed by different perpetrators (re-victimization) and other times referring to experiences of different types of violence (psychological, physical, sexual, controlling, financial, family, and non-partner abuse) concurrently or recurrently over time (Chan et al., 2021). Poly-victimization is associated with poor physical and mental health, psychopathological and psychosomatic symptoms, trauma, and behavioral problems across the lifespan (Barnes et al., 2016; Chan, 2013; Charak et al., 2016; Finkelhor et al., 2007; Ford et al., 2010; Jackson-Hollis et al., 2017; Radatz & Wright, 2017; Richmond et al., 2009; Sabina & Straus, 2008; Turner et al., 2017; Wolfe, 2018). Despite the serious consequences of poly-victimization for women, literature focused on poly-victimization among adult women is scarce (Krebs et al., 2011), and no studies focus on poly-victimization of women in informal settlements.
Violence in Informal Settlements
While there is a paucity of research focused on poly-victimization in informal settlements, research suggests prevalence of violence against women is higher in these communities than in other contexts. Over 60% of Nairobi’s three million residents live in informal settlements (APHRC, 2014)—defined as residential areas lacking durable housing, sufficient living and public spaces, access to basic infrastructure and services, and secure tenancy (UN-Habitat, 2016). There is limited research documenting violence or crime rates in these communities; however, one study focused on gender-based violence in a large informal settlement in Nairobi reported that up to 85% of women may experience IPV in their lifetime (Swart, 2012). Another study found that about two-thirds of participants in a random sample of women in a large informal settlement in Nairobi experienced IPV in the last year (Winter et al., 2020)nter et al., 2020). Finally, findings from a study conducted in four large informal settlements in four cities across Kenya reported that 37.2% of residents had been the victims of theft, 23.3% were mugged, 16.2% were robbed, and 5% experienced gender-based violence or murder (Musoi et al., 2014). The unique economic, political, social, geo-spatial, physical, and built environment in informal settlements may factor into higher levels and co-occurrence of violence in these communities, but more research is needed to understand the prevalence of poly-victimization, key correlates of NPV, and perpetrators in these settlements.
The purpose of this paper is to help fill this gap by answering the following questions: (1) What are the correlates of past-year physical and sexual NPV in informal settlements in Nairobi? (2) To what extent, if at all, is past-year IPV associated with past-year physical and/or sexual NPV? and (3) Who are common perpetrators of physical and sexual NPV?
Methods
Study Site
Data for this study were collected in Mathare Valley (Mathare) informal settlement in Nairobi in 2018. Mathare is one of the largest and most densely populated settlements in Kenya. It is home to approximately 200,000 residents living on less than 3-square kilometers of land (Kenya National Bureau of Statistics, 2019a). Mathare is also one of the oldest informal settlements in Nairobi. Residents began settling there as early as the 1920s (Wanjiru & Matsubara, 2017). Although the population and physical boundaries of Mathare are contested, the settlement is divided into neighborhoods or “villages.” Data for this study were collected from the 11 villages that women in the study identified as comprising the Mathare informal settlement.
Estimates of Mathare’s population suggest there are approximately 106,522 males to 100,028 females in the settlement (Kenya National Bureau of Statistics, 2019a). Just over 47% of the residents are “working,” which includes individuals who are not full-time students, home-makers, retired, or incapacitated persons, and are not too young or too old to work; almost 13% are “seeking work,” but are unemployed (Kenya National Bureau of Statistics, 2019b).
Sample
A sample of 552 women was selected using a stratified, random sampling technique. Geographic information systems (GIS) was used to randomly select households—ensuring that at least 50 households were selected from each of Mathare’s 11 villages. Subsequently, Kish methodology (Kish, 1965) was used to randomly select one woman from each household to participate in the survey. To be included in this study, women had to be at least 18 years old, speak English or Swahili, and have resided in Mathare for a minimum of 6 months. Surveys were conducted in women’s homes when no one else was present or in a private room outside of their home. Surveys were conducted by a group of nine female residents in Mathare who were trained on the principles of ethical research and rigorous data collection. These women were also trained according to the World Health Organization’s (WHO) ethical and safety recommendations for research on violence against women and sensitive topics (Ellsberg et al., 2001; World Health Organization, 2001). Since this study asked questions about experiences of recent IPV and NPV, respondents who reported violence were covertly provided referral to relevant services. A local counselor was also contracted to be in the field throughout data collection to provide support to study participants as needed.
Measures
Non-partner violence
Past-year physical NPV was measured with a single item on the survey that asked, “In the last 12 months has anyone other than your husband/partner hit, slapped, kicked, or done anything else to physically hurt you?” Women who responded “yes” to the question were given a score of “1” = experienced past-year physical NPV. Those who responded “no” were given a score of “0.” Similarly, past-year sexual NPV was measured with a single item on the survey that asked, “In the last 12 months has anyone other than your husband/partner forced you to have sex or perform sexual acts when you did not want to?” Women who responded “yes” were given a score of “1” = experienced past-year sexual NPV, and those who responded “no” were given a score of “0.”
Perpetrators of non-partner violence
Women who reported having experienced past-year physical NPV or sexual NPV were asked a follow-up, verbatim question pertaining to each type of NPV: “what was your relationship to this person?” Two researchers reviewed the responses and came up with general categories of perpetrators. If one researcher identified a type of perpetrator that did not match any of the categories, both the researchers discussed the unmatched response. As a team, it was determined whether a new category of perpetrators should be added or an existing category should be expanded to include the unmatched response. After the coding, all responses could be grouped into eight categories of perpetrators: authority figures, boyfriend/partner other than primary husband/partner, family member, child, neighbor or friend, stranger, acquaintance, or multiple people across different categories.
Intimate partner violence
We used a modified version of the domestic violence module in the Demographic and Health Surveys (DHS) to develop an IPV measure (2014). IPV scores are based on women’s experiences of three types of violence (psychological, physical, and sexual) within the past 12 months. Psychological IPV was measured with three items (e.g., partner humiliated, threatened to hurt someone close, or insulted participant), physical IPV was measured with eight (e.g., partner pushed, shook or threw something at participant; slapped; twisted arm or pulled hair; punched; kicked, dragged, or beat up participant; tried to strangle or burn participant; threatened with a weapon; or attacked with a weapon), and sexual IPV was measured with three (e.g., partner used physical violence to force sexual intercourse, physical violence to force participant to perform other sexual acts they did not want to, or threatened to use physical violence to have sexual intercourse or perform sexual acts). Responses to individual questions were binary. Separate dichotomous variables for emotional, physical, and sexual IPV were included in analyses exploring associations between different types of IPV and past-year NPV. To test associations between IPV poly-victimization, that is, the experience of more than one type of IPV (emotional, sexual, or physical) in the same one-year period, and NPV, we created a four-category past-year IPV poly-victimization variable. The four categories include: 0 = “did not experience any form of IPV,” 1 = “experienced only one form of IPV,” 2 = “experienced two forms of IPV,” and 3 = “experienced all three forms of IPV.”
Other potential social, economic, mental health, and demographic correlates of NPV
A number of sociodemographic variables including household income (measured as a respondent’s estimate of monthly income in Kenyan shillings [KES] (less than 10,000, between 10,000 and 15,000, and more than 15,000), level of education (less than primary, completed primary, and at least some secondary), age (continuous), women’s relationships status (married; regular partner, but not married; and single), number of children (none, one or two children, and three or more children), had employment, had a business, had access to a toilet for all sanitation needs throughout the day and night, and had access to water inside her home/building/housing plot were included in the statistical models. Women’s self-reported health status was also included. The self-reported health variable, originally measured on a five-point scale ranging from 1 (poor) to 5 (excellent), was dichotomized. Women who reported having good/very good/excellent health were given a score of “1”; those who reported having poor/very poor health were given a score of “0.” Additionally, measures of whether the participant drinks alcohol or whether her husband/partner drinks alcohol were also included.
Women in this study were asked whether, in the last 2 weeks, they had experienced each of the following problems every day or nearly every day: (1) money problems, (2) health problems, (3) conflict with family or friends, and (4) problems with authorities (such as employers, bar owners, police, or government officials). If a respondent answered “yes” to having these issues, they were given a score of “1” = reports frequent problems on that item. A score of “0” on one of the “frequent problems” items reflects that the participant did not report experiencing that issue frequently (every day or nearly every day) in the 2 weeks leading up to the survey.
Finally, we included two mental health measures in the analyses. A Swahili version of the Patient Health Questionnaire-9 Depression Scale (PHQ-9) was used as a screening tool to assess whether respondents’ self-reported depression symptoms met the criteria for possible major depressive disorder (Manea et al., 2015; Omoro et al., 2006). Respondents were provided with a list of nine symptoms that correspond with diagnostic criteria for major depression and were asked to indicate how often each symptom bothered them over the last 2 weeks from 0 (not at all) to 3 (nearly every day). A standard cutoff score of 10 or above (i.e., respondent reported experiencing at least five symptoms more than half of the days) was used, which has been shown to be an accurate cutoff for screening for possible major depression across multiple studies (Levis et al., 2019).
Respondents were also asked questions about whether they had, in the last 2 weeks, experienced suicide ideation or had ever attempted suicide. Responses to these variables were combined into a single “suicidality” variable for which participants were given a score of “1=has had suicidal thoughts in the past 2 weeks and/or has ever attempted suicide” or “0 = had never attempted suicide nor had suicidal ideation in the past 2 weeks.”
Analysis Strategy
Descriptive statistics provided information about the study sample and the prevalence rates of NPV in Mathare. In order to explore correlates of past-year physical and sexual NPV (research question 1: RQ1), chi-square tests (for categorical variables) and bivariate logistic regressions (for continuous variables) were used to test bivariate associations between various social, economic, demographic, health, and mental health items and past-year physical and sexual NPV. Additionally, multivariate penalized maximum likelihood logistic regressions were run in Stata statistical software (version 15; StataCorp, 2017) to explore key correlates of past-year physical and sexual NPV. Since NPV is a relatively rare event, we used penalized maximum likelihood logistic regressions to reduce the risk of small sample bias or “separation” in the models (Allison, 2012; King & Zeng, 2001). We followed the guidance of Hosmer et al. (2013) for purposeful selection of covariates to build our penalized maximum likelihood logistic regression models. In order to explore potential associations between past-year IPV and past-year physical and sexual NPV (research question 2: RQ2), we included different types of past-year IPV (emotional, physical, and sexual) in the multivariate penalized maximum likelihood logistic regressions from RQ1 as independent variables (Model 1: Physical NPV as dependent variable; Model 2: Sexual NPV as dependent variable). In two separate models (Models 2 and 4) we included a past-year poly-victimization count variable instead of the different types of IPV to explore whether IPV poly-victimization was associated with past-year physical and/or sexual NPV. Variance inflation factors (VIFs) were used to assess multicollinearity of all independent variables included in the multivariate logistic regressions. All VIFs were less than 2.5—well below the acceptable value of 4.0 (Hair et al., 2010). In order to explore common perpetrators of physical and sexual NPV (research question 3: RQ3), we looked at frequencies of the eight categories of perpetrators of past-year physical and sexual NPV in this sample.
Ethics Approval
The study was approved by ethics committees at Rutgers, The State University of New Jersey, and the National Commission on Science, Technology, and Innovation in Nairobi Kenya.
Results
Participant Characteristics
Descriptive and Bivariate Statistics.
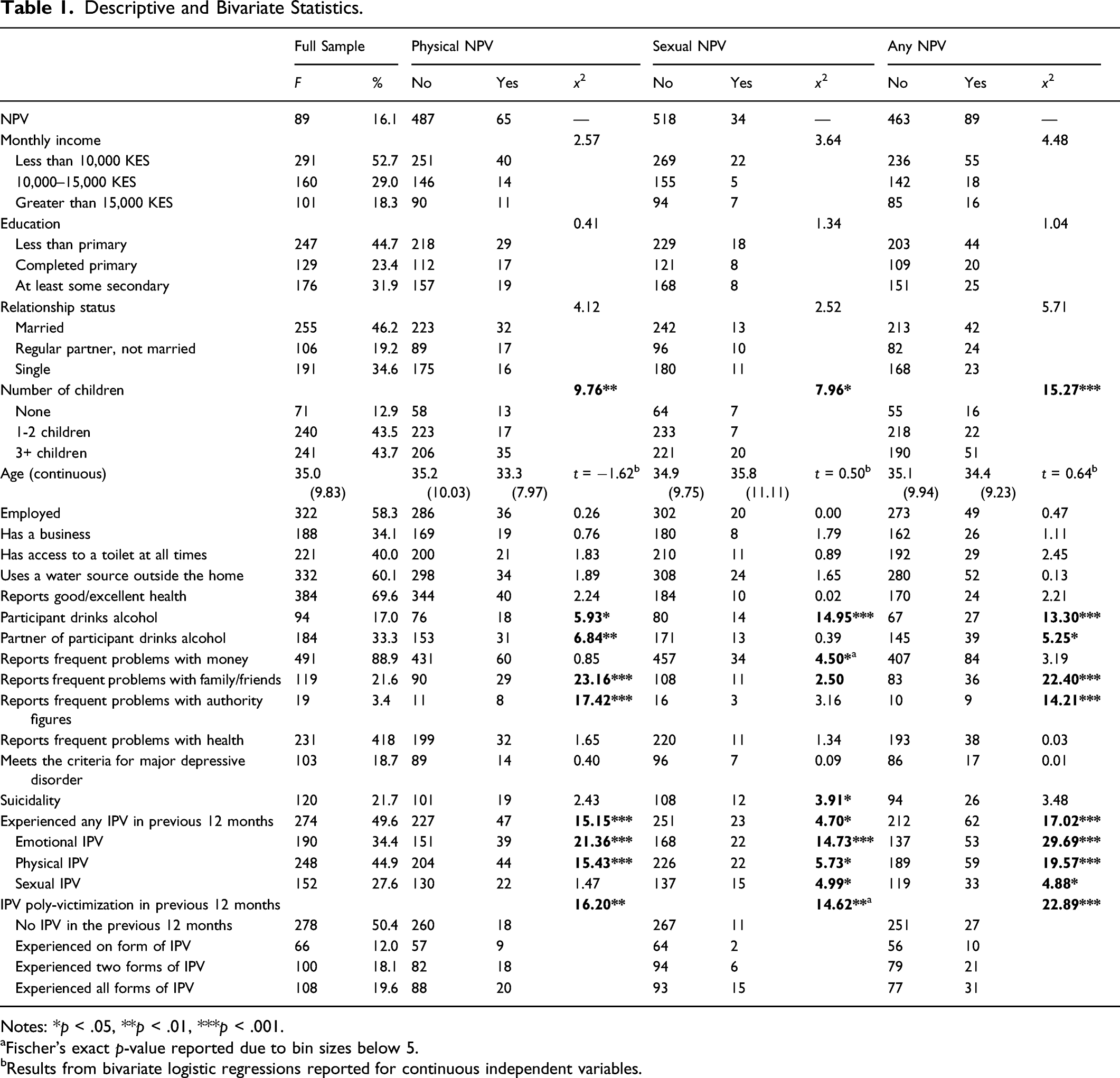
Notes: *p < .05, **p < .01, ***p < .001.
aFischer’s exact p-value reported due to bin sizes below 5.
bResults from bivariate logistic regressions reported for continuous independent variables.
Bivariate Tests
Results from chi-squared tests between categorical independent variables and NPV and from bivariate logistic regressions between continuous independent variables and NPV are presented in Table 1.
Physical non-partner violence
Number of children [χ2 (2, N = 550) = 9.76, p = 0.008], participant drinks alcohol [χ2 (1, N = 551) = 5.93, p = 0.015], participant’s partner drinks alcohol [ χ2 (1, N = 551) = 6.84, p = 0.009], frequent problems with family or friends [ χ2 (1, N = 551) = 23.16, p = 0.000], and frequent problems with authority figures [χ2 (1, N = 551) = 17.42, p = 0.000] were significantly associated with past-year physical NPV. Any past-year IPV [χ2 (1, N = 551) = 15.15, p = 0.000], but specifically emotional and physical IPV, and past-year IPV poly-victimization [χ2 (1, N = 551) = 16.20, p = 0.001] were significantly associated with past-year physical NPV.
Sexual non-partner violence
Number of children [χ2 (2, N = 550) = 7.96, p = 0.019], participant drinks alcohol [χ2 (1, N = 551) = 14.95, p = 0.000], frequent problems with money [ χ2 (1, N = 551) = 4.50, p = 0.034], and suicidality [χ2 (1, N = 551) = 3.91, p = 0.030] were significantly associated with past-year sexual NPV. Any past-year IPV [χ2 (1, N = 551) = 4.70, p = 0.030], including emotional, physical, and sexual IPV, and past-year IPV poly-victimization [χ2 (1, N = 551) = 14.62, p = 0.005] were significantly associated with past-year sexual NPV.
Multivariate Regressions
Multivariate Logistic Regressions.

Notes: *p < 0.05, **p < 0.01, ***p < 0.001.
aDue to small bin sizes, results presented are from model with collapsed three-category IPV poly-victimization variable (1 = less than two forms of IPV, 2 = 2 forms of IPV, 3 = all three forms of IPV).
Physical non-partner violence
Findings from Model 1, looking at associations between different types of IPV and past-year physical NPV, suggest that past-year emotional and physical IPV were associated with three times the odds of experiencing past-year physical NPV (ORemotional = 3.0, 95% CI [1.30, 6.86]; ORphysical = 3.0, 95% CI [1.24, 7.21]). Also in Model 1, being single, as compared to being married, was associated with 2.6 times the odds of experiencing past-year physical NPV (OR = 2.6, 95% CI [1.03, 6.70]). Having 1–2 children, compared to having no children, was associated with 72% lower odds of experiencing past-year physical NPV (OR = 0.3, 95% CI [0.12, 0.68]). Relying on a water source outside the home was associated with 50% lower odds of experiencing past-year physical NPV (OR = .5, 95% CI [0.28, 0.91]). Participant drinking alcohol was also associated with about 2 times the odds of experiencing past-year physical NPV (OR = 2.1, 95% CI [1.06, 3.97]). Finally, frequent problems with family or friends (OR = 2.6, 95% CI [1.38, 4.70]) and frequent problems with authority figures (OR = 3.2, 95% CI [1.09, 9.12]) were both associated with increased odds of past-year physical NPV. Findings from Model 2, looking at associations between past-year IPV poly-victimization and past-year physical NPV, suggest that past-year IPV poly-victimization increase the odds of experiencing physical NPV in the same year (ORone form of IPV = 3.1, 95% CI [1.13, 8.30]; ORtwo forms of IPV = 5.9, 95% CI [2.28, 15.44]; ORthree forms of IPV = 4.0, 95% CI [1.55, 10.49]).
Sexual non-partner violence
Findings from Model 3, looking at associations between different types of IPV and past-year sexual NPV, suggest that past-year emotional IPV was associated with about six times the odds of experiencing past-year physical NPV (OR = 6.1, 95% CI [1.81, 20.58]). Also in Model 3, being single, compared to being married, was associated with 5.3 times the odds of experiencing past-year physical NPV (OR = 5.3, 95% CI [1.6, 17.02]). Having 1-2 children, compared to having no children, was associated with over 80% lower odds of experiencing past-year physical NPV (OR = 0.2, 95% CI [0.06, 0.57]). Participant drinks alcohol (OR = 3.9, 95% CI [1.81, 8.57]) was associated with increased odds of past-year sexual NPV, and reporting frequent health problems (OR = 0.4, 95% CI [0.17, 0.87]) was associated with decreased odds of past-year sexual NPV. Findings from Model 4, looking at associations between past-year IPV poly-victimization and past-year sexual NPV, suggest that past-year IPV poly-victimization increased the odds of experiencing physical NPV in the same year (ORtwo forms of IPV = 4.9, 95% CI [1.40, 17.46]; ORthree forms of IPV = 8.8, 95% CI [3.10, 25.09]).
Perpetrators of Non-Partner Violence
Common Perpetrators of NPV.

Physical non-partner violence
Findings suggest that about a quarter of past-year physical NPV was perpetrated by a neighbor or friend, 22% by a family member (mostly in-laws or cousins), and 15% by an authority figure (including an employer, government official, police, or water point manager). About 12% of past-year physical NPV incidents were perpetrated by strangers and an additional 9% by acquaintances (e.g., a fellow drinking buddy at a bar or a friend of a friend).
Sexual non-partner violence
About a quarter of past-year sexual NPV was perpetrated by a neighbor or friend. About 17% was perpetrated by a family member, 15% by a boyfriend or partner other than the participants’ primary partner, and 12% by an authority figure. An additional 12% of past-year sexual NPV incidents were perpetrated by acquaintances and 8% by strangers.
Discussion
The purpose of this study was to explore correlates of past-year NPV, associations between past-year IPV and NPV, and common perpetrators of NPV in a large informal settlement in Nairobi. One of the key findings of this study was the clear association between past-year IPV and NPV—suggesting a high probability of poly-victimization, that is, the co-occurrence of at least one type of IPV and NPV in the past year in informal settlements. The strong association between past-year IPV poly-victimization, that is, a woman experiencing multiple forms of IPV (emotional, physical, and/or sexual) with past-year NPV suggests that poly-victimization may be a serious issue for some women both within and outside the home.
Intimate partner violence and Non-Partner Violence are Prevalent in Informal Settlements in Nairobi
Overall, about 16% of women in this study reported experiencing physical and/or sexual NPV in the past year, close to 50% reported experiencing psychological, physical, and/or sexual IPV, and more than 11% reported experiencing both IPV and NPV in the past year. Although there are no existent studies focused on poly-victimization among adult women in Kenya or in informal settlements, specifically, findings from a study by the Kenyan National Crime Research Centre (National Crime Research Centre, 2014) suggest prevalence rates of 19.1% for women experiencing past-year NPV and 37.7% for women experiencing past-year IPV. Comparatively, rates of past-year NPV in this study are slightly lower than national estimates and rates of past-year IPV are slightly higher; however, it is difficult to make cross-country or even cross-contextual comparisons of prevalence because definitions of poly-victimization and the measurement of IPV, NPV, and poly-victimization vary drastically between different studies (Chan et al., 2021).
In general, the lack of prevalence rates of poly-victimization in sub-Saharan Africa, particularly in informal settlements, is disconcerting considering the health implications of poly-victimization for women. The high rates of poly-victimization in this study coupled with the paucity of research focused on poly-victimization in informal settlements, where violence rates are thought to be much higher than in other contexts (Izugbara & Egesa, 2019; Ruteere et al., 2013; Swart, 2012; UN-Habitat, 2015; Winter et al., 2020; Ziraba et al., 2011), highlight the importance of more research exploring causes, correlates, and associated outcomes for poly-victimization and points for response, support, and prevention in these settlements.
Intimate Partner Violence and Non-Partner Violence are Strongly Correlated, Suggesting Poly-Victimization
Findings from this study corroborate evidence from other research that suggests IPV and NPV are strongly associated (Krebs et al., 2011). In this study, 70% of women who reported experiencing past-year NPV also reported experiencing past-year IPV and women who reported experiencing past-year emotional IPV or physical IPV had three times the odds of also experiencing physical NPV in the same year. Those who reported experiencing past-year emotional IPV had six times the odds of also experiencing sexual NPV in the same year. Perhaps an even more striking finding from this study is the strong association found between past-year IPV poly-victimization, that is, when women are experiencing more than one form of IPV (emotional, physical, and/or sexual), and experiences of physical and sexual NPV in the same year. These findings suggest that in addition to experiences of IPV, in general, IPV poly-victimization may be an important predictor of NPV in this setting, and/or NPV may be a strong predictor of IPV, as has been shown in other studies (Capaldi et al., 2012; Stöckl et al., 2014; World Health Organization & Pan American Health Organization, 2012).
Although literature focused on poly-victimization among adult women is scarce (Krebs et al., 2011), research focused on poly-victimization in other populations may provide some insights into why exposure to past-year IPV might increase a woman’s odds of also experiencing NPV in informal settlements. Finkelhor et al. (2009), for example, found that living in a dangerous area, having a dangerous or problematic family, or having emotional problems are associated with poly-victimization among children. This finding has, to some extent, been reflected in other research focused on violence and crime in informal settlements. For example, Winter, Obara, et al. (2021) found that residents perceive safety and security as serious issues in informal settlements in Nairobi, and they associated this lack of safety/security with high rates of crime and violence in these communities.
Lifestyles routine activities and target congruence theories have also been used in literature to help explain the occurrence of poly-victimization in several contexts (e.g., Snyder et al., 2021). Target congruence theory considers individual characteristics that may make a person more vulnerable to victimization. Lifestyles routine activities theory posits that victimization risk is associated with circumstances in a person’s everyday routines/activities that either expose or protect them from criminogenic/high-risk situations and environments (Felson, 1998; Hindelang et al., 1978; Hope et al., 2001). While no research has specifically applied target congruence or lifestyles routine activities theories to study violence in informal settlements, there may be a number of factors specific to or exacerbated by living in informal settlements that increase women’s risk of experiencing poly-victimization (e.g., being part of a targeted tribal/ethnic minority in a section of the settlement that is dominated by a different tribal/ethnic group or having a disability or mental health issue). There may also be circumstances specific to residents’ everyday routines/activities in informal settlements that either expose or protect them from high-risk situations and environments for poly-victimization. For example, lack of access to water and sanitation, a common reality for many households in informal settlements, can impact women’s risk of violence (Sommer et al., 2014; Sorenson et al., 2011; Winter et al., 2020).
Research has also shown that harmful social and community norms that normalize or condone violence as a response to certain behaviors and actions that violate gender or other social roles can contribute to poly-victimization (Chan et al., 2021; Salter, 2014). The unique economic, political, and social context in informal settlements may factor into poly-victimization in these communities. For example, findings from research focused on young men and masculinities in informal settlements in sub-Saharan Africa (Gibbs et al., 2014; Izugbara et al., 2014; Izugbara & Egesa, 2019; Mariano et al., 2018; Moncada, 2013) and studies focused on residents’ perceptions of the causes of violence in informal settlements in Nairobi (Winter, Obara, et al., 2021) suggest that social, political, and economic exclusion of residents of these settlements inhibits men from conforming to traditional ideas of masculinity, such as financially providing for their family—pushing them into petty crime and involvement in gangs. As a result, men in these communities may, in an effort to exercise some power or control in the face of many day-to-day challenges, perpetrate violence against women (Mariano et al., 2018)—leading, perhaps, to higher poly-victimization levels in these settlements.
The unique geo-spatial, physical, and built environment in informal settlements may also intersect with social environments in these communities, contributing to women’s poly-victimization risk. For example, informal settlements are extremely densely populated with most houses being constructed side-by-side. If a woman in this context is experiencing violence at the hand of their partners at home or in public, others, including neighbors and other family members, may easily hear or witness violent incidents. Additionally, research suggests that residents of informal settlements frequently share stories about violence that may contribute to a normalization of violence against women (Winter, Aguilar, et al., 2021) even if there are no general community or social norms that condone violence. This aligns with theories of violence, for example, social learning theory, that suggest violence is learned and reinforced primarily through association with or exposure to others (Akers, 1998). To some extent, findings from this study about the common perpetrators of NPV seem to corroborate the idea that the social and physical environment in informal settlements may influence NPV. For example, 25% of physical and sexual NPV is perpetrated by a neighbor or friend and an additional 22% of physical NPV and 17% of sexual NPV is perpetrated by a family member. Thus, for both physical and sexual NPV, close to half of the incidents are perpetrated by individuals who are the most likely to also witness or hear about IPV being perpetrated against the respondent.
Correlates of Non-Partner Violence
Findings from this study also provided helpful information about correlates of NPV in informal settlements. Results from the multivariate regressions, for example, suggest that women who relied on a water source outside of their home, building complex, or housing plot had lower odds of experiencing past-year physical NPV. This finding is inconsistent with previous research that suggests lacking access to water and sanitation in the home is associated with higher risk of NPV (Sommer et al., 2014; Sorenson et al., 2011). Some studies have suggested that women having to travel long distances away from their homes to fetch water or relieve themselves may be at higher risk of violence (Massey, 2011; Sommer et al., 2014). In a community with higher levels of violence, in general, having to fetch water or access a site/facility for sanitation outside the home, especially at great distances, can simply increase the time of exposure to potential violence; however, this explanation is likely too simplistic. Another explanation to consider is the effect lack of access to water and sanitation has on women’s exposure to different physical and social environments. Literature suggests, for example, that, depending on the location of available water sources or sanitation, women may have to travel outside of their communities; into forested, dangerous, or poorly lit areas; or through/past areas with higher crime and violence rates such as alcohol outlets (Truelove, 2011). This may increase women’s risk of NPV.
While our findings contradict evidence that women who have to travel outside their homes for water are at greater risk of NPV, some research suggests the direction of the relationship between access to water and NPV may vary across different contexts (Barchi & Winter, 2019). There is limited explanation in the literature about why this variation exists. In this study, however, our exploration of the most common perpetrators of NPV may shed some light on our findings. Most women in this informal settlement are experiencing NPV at the hands of family members, neighbors, and friends. Since water is a necessity and women are usually responsible for collecting it, fetching water outside the home may provide women with an acceptable opportunity to get away from home on daily or near daily basis and, in doing so, to put space between themselves and these perpetrators of violence Also, a lot of the research suggesting water access is associated with higher risk of violence is focused on settings other than informal settlements, for example, rural contexts, which could explain some of the difference in findings between this study and others. Depending on the time of year and water availability in informal settlements, women in these communities may not have to travel as far to fetch water or may have more than one point outside the home from which they can collect water—giving them the option to avoid areas of high crime, forests, poorly lit areas, etc. This may not be the case for women in other communities, for example, in dry rural areas where there may only be one water source. Additionally, women’s water options are contingent upon water availability both within and external to their communities. Even in informal settlements such as Mathare, governments often ration water during the dry seasons, in times of drought, or during infrastructure changes (Ledant, 2013; Njoroge et al., 2018), that is, they turn on water taps only during certain hours on specific days of the week. So, we want to be careful about assuming women living in informal settlements always have different options for water collection.
Women in this study who reported frequent problems with friends or family and authority figures also had higher odds of experiencing past-year physical NPV. This aligns with findings from this study that suggest NPV is often perpetrated by friends, neighbors, and family. This finding also highlights a limitation of the study data. Since this is a cross-sectional study and we did not measure frequency and timing of NPV, we cannot make claims about whether or how often problems with family and friends or authority figures causes NPV or vice versa.
Frequent problems with health were also associated with past-year physical NPV in this study. Again, the cross-sectional nature of the data makes it hard to know whether NPV is causing health problems or frequent health problems are a risk factor for NPV. In the latter case, frequent health problems could be a proxy for a chronic health condition or disability. Disability and chronic diseases, such as diabetes, have been associated with NPV (Malihi et al., 2021), IPV (Mason et al., 2013; Weitzman & Goosby, 2021), and poly-victimization (Codina et al., 2022; Lev et al., 2021; Snyder et al., 2021) in previous studies. While chronic disease and disability are often thought of as potential consequences of violence, they may also be risk factors for NPV. For example, frequent and chronic health problems may make it difficult for women in informal settlements to carry out expected tasks in the home or in difficult-to-navigate, challenging physical and built environments, thus increasing their vulnerability to violence.
Participants who reported that they drink alcohol had higher odds of experiencing past-year physical and sexual NPV in this study. There are several studies that have found associations between both respondent and partner alcohol use and IPV in sub-Saharan Africa (Barchi et al., 2018; Greene et al., 2017) or abuse by a sexual partner, more broadly (Pitpitan et al., 2013). In specific verbatim responses in this study, some women reported that they had experienced sexual and/or physical NPV at the hands of strangers, acquaintances, and/or friends they met or knew from a bar/drinking context. While these women did not represent the majority of women who experienced past-year NPV, alcohol consumption may be a risk factor for NPV. This finding may also be in-line with Snyder et al.’s (2021) suggestion that circumstances in a person’s everyday routines/activities may expose or protect them from criminogenic/high-risk situations and environments. Bars or alcohol distribution centers could, for example, be higher risk environments for NPV as has been seen in some previous studies (Pitpitan et al., 2013). However, it is important to emphasize that these women are not at all to blame for their experiences. Rather, identifying spaces where women experience increased levels of risk is critical, as it provides opportunities for prevention and intervention.
Interestingly, the only demographic variables associated with women’s experiences of past-year NPV were having 1-2 children, as compared to having none and being single or having a regular partner who is not a spouse, as compared to being married. Women in this study who reported they had 1-2 children, as opposed to no children, had lower odds of experiencing past-year physical and sexual NPV. While this is a challenging factor to explain, we, again, turn to women’s reports of the common perpetrators of NPV. About 17% of perpetrators of sexual NPV in this study were family members, including in-laws and blood relatives. The finding that women who do not have children have higher odds of experiencing past-year sexual NPV may reflect social and community norms about women’s roles in society. There may be social, community, or family norms about the acceptability of violence in certain circumstances or among certain women (Chan et al., 2021; Salter, 2014). In this case, for example, sexual NPV may be more normalized or accepted among women who do not yet have children. It is, however, not possible to make any definite conclusions without further research investigating norms and expectations around NPV in these contexts. A small percentage of the perpetrators of physical IPV (6.2%) were also children of the participant; however, this small proportion is unlikely to explain significant associations between having children and past-year physical NPV.
Women who were single, compared to women who were married, had significantly higher odds of having experienced past-year physical and/or sexual IPV. Women who reported having a regular partner, but who were not married also had significantly higher odds of past-year sexual IPV compared to married women. These findings corroborate evidence from previous literature that suggests being married may be a protective factor against NPV in some contexts. Barchi and Winter (2019), for example, found that being married was associated with lower odds of experiencing past-year NPV in 17 out of 20 countries in an analysis of Demographic and Health Surveys from Sub-Saharan Africa.
Limitations
Although the findings from this study provide important information about the relationship between IPV and NPV, correlates of NPV, and common perpetrators of NPV in a large informal settlement context in sub-Saharan Africa, the study had limitations. First, data are cross-sectional; thus, we cannot make any claims about the direction of associations between IPV and NPV or between specific correlates and NPV. Given the high prevalence rates of NPV and poly-victimization in this sample, it is clear that there is a need for longitudinal research focused on these critical issues in informal settlements in sub-Saharan Africa and other global contexts. Another potential limitation to these data is under- or over-reporting of violence. Almost all research focused on violence against women acknowledges that, given the stigma and sensitivity associated with violence, many women may not feel comfortable talking about it. While we did our best to ensure that all women who assisted in the data collection were trained extensively in the importance of maintaining anonymity of surveys, confidentiality of participant information, and the ethics of conducting research focused on sensitive topics, some of the participants may not have been comfortable sharing their experiences of violence, particularly with fellow community members (data collectors). Finally, because NPV is a relatively rare event, we had to dichotomize several variables or collapse the number of response categories for others to ensure there was an adequate distribution of NPV frequencies across all categories of the independent variables. For some variables, the use of indicator variables also helped clarify relationships between potential correlates and NPV. Number of children, for example, was measured as a continuous variable in the original surveys; however, findings from models with the continuous form of this variable versus a categorical transformation of the variable suggest that, in this context, increasing numbers of children are not associated with a significant difference in odds of experiencing NPV, but having children and, specifically, having 1-2 children, is. While dichotomizing continuous, ordinal, or nominal variables and collapsing response categories of multi-category nominal variables can lead to a loss of information and power, it was necessary for some variables in these rare-event analyses. Future studies with larger samples of women and more continuous variable options may limit loss of information and power; however, our hope is that NPV becomes an increasingly rare event regardless of the sample size; so, this statistical limitation may continue to be an issue even in larger sample sizes with more continuous variables.
Conclusion
The purpose of this study was to explore NPV in a large informal settlement in Nairobi, including investigating correlates and common perpetrators of NPV in this setting. Findings from this study showed a strong, positive association between past-year IPV and NPV—highlighting a critical area for future study in IPV and NPV research and reconsideration of violence theories that separate IPV and NPV without acknowledging potential links between the two. Results corroborated some findings from research focused on factors associated with NPV, but yielded important new associations in the informal settlement context. Women in this study who reported accessing water outside the home, for example, had lower odds of experiencing past-year physical NPV. While this finding contradicts existing research, women’s reports about common perpetrators of NPV in this study may provide important context for exploring the theoretical and practical implications of the finding. For example, given that most women in this study reported experiencing NPV at the hands of family members, neighbors, and friends, accessing water outside the home may provide women with an acceptable reason to leave the home and have space from a potential perpetrator. This study marks an important first step in documenting prevalence of NPV and poly-victimization and correlates and common perpetrators of NPV in informal settlement contexts; however, it also highlights the serious lack of existent literature that focuses specifically on NPV and poly-victimization. NPV and poly-victimization have serious health consequences for women in any context, but women in informal settlements are also facing a number of structural economic, social, political, and environmental challenges that affect their health and wellbeing and may exacerbate the health consequences of violence perpetrated against them. Thus, more research into NPV and poly-victimization in informal settlements in sub-Saharan Africa and globally is critical. Longitudinal data as well as qualitative studies exploring the reason for significant associations and correlates of NPV would help to clarify causes of NPV and poly-victimization and points for intervention and policy change.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data on which this study is based were originally collected as part of a pilot project supported by a grant from the Rutgers Global Health Institute and were collected by the author Dr. Winter as part of a postdoctoral research fellowship at Rutgers, The State University of New Jersey.