
Abstract
This study examined the efficacy of a short virtual case simulation for Korean American (KA) faith leaders, “Religious Leaders for Healthy Families.” The goal of the program is to increase knowledge about intimate partner violence (IPV) and healthy intimate partner relationships, enhance self-efficacy in IPV prevention and intervention, strengthen attitudes that support their roles on IPV prevention and intervention, increase positive outcome expectations of their actions, and increase behavioral intentions and behaviors on IPV prevention and intervention. KA faith leaders from two large metropolitan areas with a high concentration of KA immigrants were invited to participate in the study (N=102). Participants completed three online assessments: baseline, a 3-month, and a 6-month follow-up. After the baseline assessment, participants were randomized to either intervention (n = 53) or control (n = 49). The intervention consisted of four online simulation modules, each taking approximately 15–20 min to complete. At the 6-month follow-up, faith leaders in the intervention group significantly increased their knowledge and self-efficacy in IPV prevention and intervention compared to the control group. Mean scores for attitudes against IPV and prevention behaviors increased from baseline to the 6-month follow-up for the intervention group more than the control group, but the differences were not statistically significant. “Religious Leaders for Healthy Families” has the potential to reduce disparities in accessing resources and services for immigrant survivors of IPV. With its ease of use, this short, free online intervention has a high potential for uptake among faith leaders. Results are promising, but the COVID-19 pandemic negatively affected the study, with participants having scarce opportunities to practice the skills learned from the intervention. A larger follow-up study that combines “Religious Leaders for Healthy Families” with a community-wide intervention that targets all community members is warranted to reach more faith leaders and community members.
Keywords
Introduction
Immigrant women report more intimate partner violence (IPV) than the national average and less access to services (Klevens, 2007; Yoshihama & Dabby, 2015). Further, assessments of IPV tend to underestimate the actual prevalence (Breiding, Smith, et al., 2014), especially among immigrants with language and cultural barriers. Barriers that abused women face when seeking help are exacerbated in immigrant communities. Impediments unique to immigrants are limited English language skills, absence of culturally responsive services, lack of knowledge about existing resources, immigration status, financial dependency, community discrimination, and negative stereotypes of immigrants (Cho, 2012; Finfgeld-Connett & Johnson, 2013). In addition, cultural and religious values may also contribute to IPV and the shame of seeking help. These values are male-dominated family structure, rigid gender roles, ingrained patriarchal and hierarchal family systems, family honor and privacy, and group welfare over personal needs (Abugideiri, 2010; Roy, 2012). Due to these cultural and psychosocial barriers, abused immigrant women prefer to exhaust all informal resources, including faith leaders, before seeking help from formal service providers (Akutsu et al., 2007; Cuevas et al., 2014).
Various professionals, such as social service professionals (e.g., social workers, counselors, therapists, and child welfare workers), health care professionals (e.g., doctors, nurses, and midwives), criminal justice professionals (e.g., police officers, prosecutors, and judges), and faith leaders (e.g., ministers, priests, and imams), come into direct contact with survivors of IPV in their work (Breiding, Chen, et al., 2014). These professionals can play essential roles in screening and identifying IPV survivors, referring them to services, and conducting prevention activities (Choi & An, 2016). The World Health Organization (2013) published guidelines for training healthcare professionals on IPV. These guidelines focus on increasing knowledge of IPV and relevant laws, changing attitudes (e.g., victim-blaming), and teaching how to enquire and respond to potential survivors appropriately. Several intervention studies have worked with professionals to increase their knowledge of IPV and enhance IPV screening and assessment. However, these studies have been predominantly for healthcare professionals, with only 16 studies identified in non-healthcare settings (An & Choi, 2017; Sawyer et al., 2016). While half of the reviewed studies had a good or fair quality according to the U.S. Preventive Services Task Force guidelines (Choi & An, 2016), there is an urgent need to increase the methodological rigor (e.g., randomized control trials with valid and reliable measures).
Effective strategies to enhance access to IPV services and resources must incorporate the values and perspectives of the community from which survivors come. About 75% of Korean American immigrants in the United States are affiliated with Protestant churches (Kim et al., 2001). Immigrants turn to their church for various issues, such as mental health and family problems, including IPV (Lee et al., 2008). Coupled with the scarcity of formal social service agencies for Asian immigrants, Korean American immigrant clergy are essential to prevent and solve problems related to IPV in their community (Im, 2003; Moon, 2005). However, most faith leaders, including Korean American faith leaders, are not equipped to deal with IPV (Shaw et al., 2022; Tedder & Smith, 2018). Only 16% of KA immigrant clergy reported feeling well prepared to handle IPV in their congregations (Choi, 2015). On a positive note, the Korean American faith leaders in the same study recognized the need for IPV education and prevention activities in their community. In addition, they considered themselves valuable figures who are well-positioned, albeit often ill-prepared, to deal with IPV in the community. The large majority of respondents stated interest in attending a training on IPV.
Considering the Korean American immigrant community’s contexts and social norms that influence peer and community responses, or lack thereof, to IPV survivors, our study targeted the heart of immigrant communities, the religious leaders (Abu-Ras et al., 2008; Aloud & Rathur, 2009; Min, 2010). The cultural nature of the Korean American immigrant community grants religious leaders the strongest potential to assist IPV survivors in accessing the criminal justice system, getting necessary services, and changing attitudes that tolerate IPV.
Current Study
The present study describes the outcomes of a randomized clinical trial designed to evaluate the impact of an online simulation for Korean American faith leaders to increase their capacity to prevent IPV and assist survivors among Korean immigrants to the United States. The minimum contact control group participants received a 2-page brochure, “What every congregation needs to know about domestic violence,” from the Faith Trust Institute. It provides information on types of IPV and strategies for clergy for IPV intervention and prevention.
We hypothesized that faith leaders assigned to the online simulation, compared with the minimum contact control group, would report (1) more knowledge about IPV and healthy intimate partner relationships, (2) higher self-efficacy in IPV prevention and intervention, (3) stronger attitudes that support their roles on IPV prevention and intervention, (4) more positive outcome expectations of their actions, and (5) more frequent behavioral intentions and behaviors on IPV prevention and intervention.
Methods
Intervention
In the first phase of this project, we developed and pilot-tested a four-module culturally responsive online simulation training for Korean American faith leaders called “Religious Leaders for Healthy Families” (Orpinas et al., 2021). We developed this intervention based on the authors’ extensive experience on this topic and the guidance of intervention mapping (Bartholomew Eldredge et al., 2016). We designed the online simulation to address the question, “What do participants in this training program need to do to prevent IPV and to handle IPV cases?” First, we identified four behavioral outcomes: (1) educate the congregation on healthy intimate partner relationships (primary prevention), (2) identify and respond to early warning signs of IPV (secondary prevention), (3) respond appropriately to disclosures of IPV (tertiary prevention), and (4) promote the safety of survivors and their children (tertiary prevention).
Second, we developed 23 performance objectives associated with the behavioral outcomes. A performance objective refers to what the clergy needs to do to achieve that outcome. For example, to educate the congregation about healthy relationships with their partner, the religious leaders must speak out against IPV from the pulpit and challenge the misuse of the Bible to justify the subordination of women.
Third, informed by social cognitive theory and theory of planned behavior (Bandura, 1986; Montaño & Kasprzyk, 2015) and the team’s research and practice experience for each performance objective, we identified four main determinants: knowledge, self-efficacy, attitudes, and outcome expectations.
Knowledge refers to facts and information not subject to opinions, with verifiable truth. Knowledge is a prerequisite to behavior change, although knowledge alone is insufficient for change (Bandura, 2004). Self-efficacy refers to the faith leaders’ confidence in their ability to educate their congregation on healthy intimate partner relationships, identify and respond to early warning signs of IPV, respond appropriately to IPV disclosures, and promote the safety of survivors and their children. Perceived self-efficacy is at the core of many health promotion interventions as believing in oneself impacts effort and persistence in the behaviors, despite barriers or setbacks (Bandura, 1997). Attitudes refer to the subjective evaluation of the expected behaviors to prevent IPV. The goal of the intervention is to strengthen attitudes against IPV and increase positive attitudes towards performing preventive behaviors. Outcome expectations refer to the pastors’ anticipated consequences of performing the preventive behaviors on parishioners. Perceiving that congregation members support their efforts to prevent IPV and intervene in cases of violence is valuable for pastors, particularly those serving small congregations (Orpinas et al., 2021).
The online training consisted of a tutorial and four virtual case simulation modules with varying degrees of complexity. Each module has a different scenario of the faith leader responding to a virtual parishioner’s questions about IPV. Each module includes several decision-making points and resources to increase faith leaders’ knowledge and self-efficacy related to each decision. For instance, in one module, the scenario introduced the background of the virtual parishioner, Inae, who is a Korean immigrant in an abusive relationship. As illustrated in Figure1, Inae starts the conversation by complaining about her husband’s bad temper, but she hesitates to reveal his violence. The faith leader needs to choose a dialogue option from the response box to comfort Inae and encourage her to share more details of her situation. After the faith leader submits the selection, Inae replies to the faith leader’s dialogue selection. In addition to the dialogue feedback from Inae, a feedback box will appear to explain why the faith leader’s decision leads to such a response from her. The scenario continues as the faith leader chooses the correct response; however, pastors are encouraged to select all answers as each provides valuable feedback. This dialogue pattern is consistent across all the modules where faith leaders can improve their knowledge of various IPV strategies. In several dialogue interactions, the system also provides related reading materials to help deepen faith leaders’ understanding. Decision-making point for faith leaders to respond to Inae’s experience.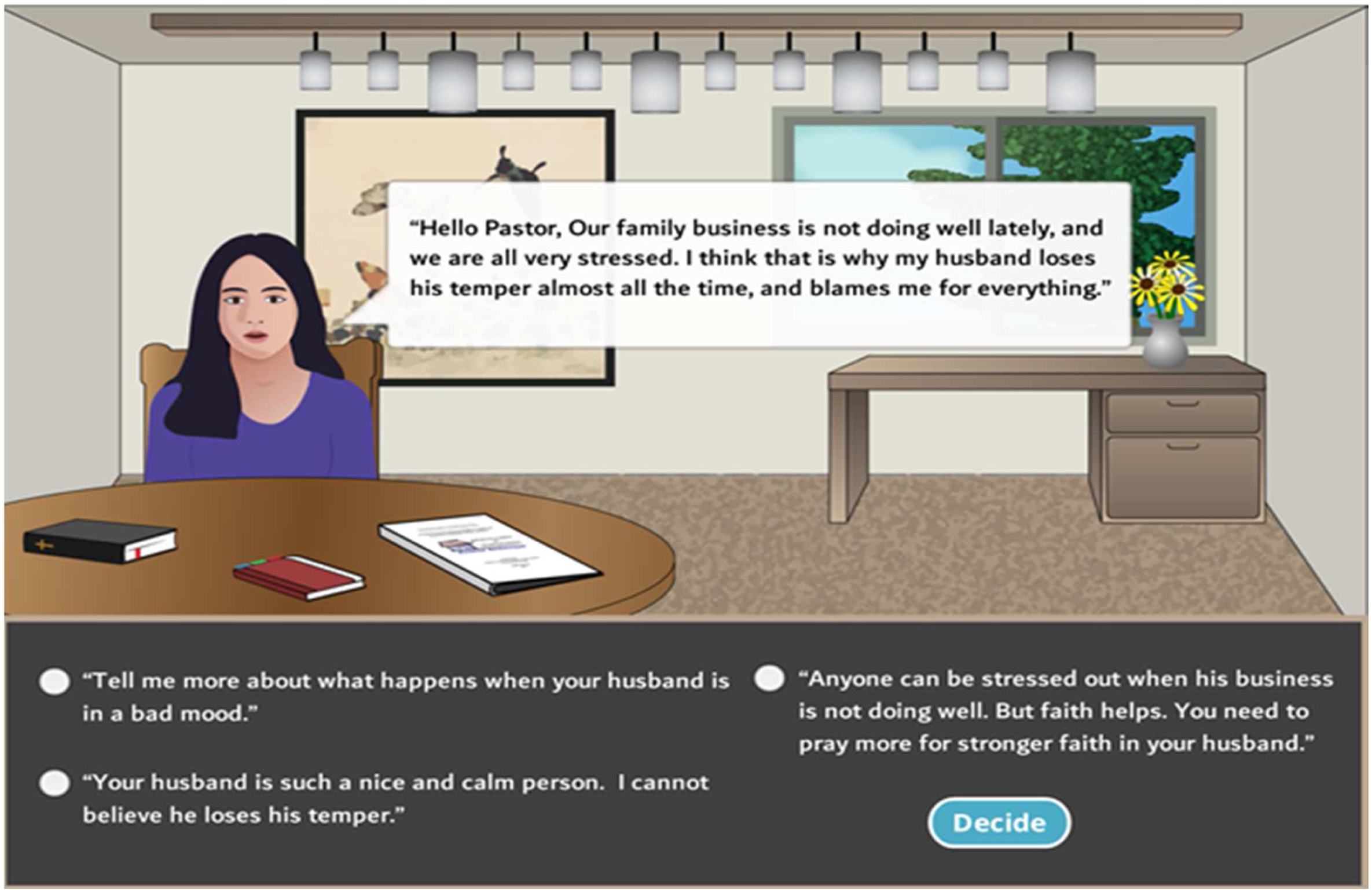
The culturally responsive design of the simulation focused on two types of Korean cultural values that contribute to IPV in Korean communities: support for traditional gender roles that view IPV as normal and acceptable to marital relationships (Raj & Silverman, 2002; Song, 1996), and sacrifice of personal needs to maintain family harmony that leads women to endure IPV and keep it a secret (Kim et al., 2018). The design of the dialogue narratives for the virtual parishioners incorporated these two values. For instance, one virtual victim blames herself for causing the violence and said, “But this (IPV) is all my fault. He would not have hit me if I had not acted so stupid, as he always says.” In another scenario, the victim asked the faith leader to hide IPV from being known by others, “Oh please, don’t. I don’t want anybody else to know about my family problem.” The faith leader needs to respond to those scenarios and change the virtual victims’ attitudes about IPV. We expect those value-based narratives to increase the cultural awareness of the faith leaders in preventing and responding to IPV in their congregation.
Each simulation took 15–20 minutes to complete. Participants could log into the online training site at any time during the intervention period. Our research team sent bi-weekly emails or made phone calls to participants to encourage them to complete the training. In addition, participants received a companion resource booklet (67 pages in the English version) that consisted of information about the prevalence, types, and signs of IPV; strategies to respond to IPV; and pastoral and community resources. At various points, the simulations encouraged participants to review specific sections of the booklet.
Setting and Participants
Korean American faith leaders from two large metropolitan areas (mid-Atlantic, mid-West) with a high concentration of Korean American immigrants were invited to participate in the study (October 2019 – May 2020). Inclusion criteria were: (1) is a current clergy of a Korean American church (a Protestant church that serves Korean Americans exclusively and conducts services in Korean) in one of the two metropolitan areas, (2) self-identifies as Korean or Korean American, (3) is 18 years old or older, and (4) has access to a computer. The present study was conducted collaboratively between our research team and two social service organizations that provide services to Asian immigrant survivors in the selected cities. Each agency hired a part-time project coordinator for this project.
Design and Procedures
We used two recruitment strategies. First, the coordinator from each domestic violence program attended a Korean Church Association meeting in each region for in-person recruitment. Second, coordinators contacted Korean American churches listed on the Korean Yellow Page by phone and invited ministers to participate. Korean Yellow pages list all Korean American churches, their contact information, and the clergy’s names. As of March 2018, each participating metropolitan area had over 180 Korean American churches listed.
Participants completed an online survey three times: baseline, 3-month, and 6-month follow-up. Demographic information was collected at baseline. We measured participants’ knowledge, self-efficacy, attitudes, outcome expectations, and prevention and intervention behaviors each time. The baseline assessment consisted of a 15-minute online survey emailed to all Korean American faith leaders who consented to participate. After baseline assessment, we used block randomization to randomly assign half of the participants from each region to the intervention and half to the control group. Block randomization was chosen over individual randomization to reduce the time between recruitment and randomization. In our previous intervention study with faith leaders, it took about 4 months to recruit 55 participants (Choi et al., 2019). This meant that the first participant would have had to wait for 4 months to be assigned to a group, and this long delay in randomization could have resulted in the loss of participants. Therefore, modeled after the National Institute on Drug Abuse’s Clinical Trials Network multisite trial, instead of recruiting all study participants and then randomizing them to either group all at once, as we recruited participants, each cohort of 4–6 participants was randomized as a block to either the online simulation or the control group using a random numbers table (Choi et al., 2019; Langhorst et al., 2012; Tross et al., 2008).
After the initial email with the survey link, we sent participants two more emails with the same survey link. To increase retention, we called participants 2 weeks before each assessment to remind them of the upcoming survey and encouraged them to complete it (Choi et al., 2015; Farabee et al., 2011). In addition, all study participants received $25 for completing the baseline assessment, $50 for completing the 3-month follow-up, and another $50 for completing the 6-month follow-up.
The university’s Institutional Review Board approved all study procedures. All participants signed an informed consent form before participating in the study. Participants could select Korean or English for the consent form, surveys, and intervention.
Measures
All measures were adapted from Choi et al. (2019) to match the intervention content.
Knowledge about facts related to IPV in the Korean community and in general was measured with 15 items. Response categories were yes, no, and uncertain. Correct responses were added (1 point each); thus, higher scores indicate more knowledge.
Self-efficacy to educate about IPV and respond to disclosures of partner violence was measured with 15 items (alpha = 0.91). Response categories ranged from not at all confident to very confident on a 4-point scale. Responses were averaged with higher scores indicating stronger self-efficacy.
Attitudes towards preventing IPV and intervening in cases of partner violence were measured with 18 items (alpha = 0.89). Response categories ranged from strongly disagree to strongly agree on a 5-point scale. Responses were averaged with higher scores indicating stronger attitudes against IPV.
Outcome expectations of the anticipated consequences of their actions on the parishioners were measured with 9 items (alpha = 0.74). Response categories ranged from most parishioners will strongly dislike it to most parishioners will strongly like it on a 5-point scale. Responses were averaged with higher scores indicating stronger expectations that parishioners would like their actions to prevent IPV.
Eleven questions measured behavior and intentions for IPV primary prevention (Cronbach’s alpha = 0.87). The questions covered speaking against IPV (e.g., preaching about healthy marital relationships, using Biblical references to speak out against domestic violence) and displaying educational materials about healthy relationships and local community services. The response categories are based on the Transtheoretical Model of Change: (1) I did not do it in the past 3 months; (2) I did not do it but intend to do it in the next 3 months; (3) I did not do it but intend to do it in the next 30 days; (4) I did it in the past 3 months; (5) I did it in the past 3 months and plan to continue to do it (Prochaska et al., 2015). Responses were averaged with higher scores indicating more frequent behaviors to prevent IPV.
For IPV intervention, the leading question was whether a parishioner had disclosed IPV. Those who indicated that a parishioner had disclosed IPV completed 11 questions about their behavior. The response categories were Yes/No (Kuder-Richardson 20 = 0.68). Those who indicated that a parishioner had not disclosed IPV completed 11 questions about their intentions if confronted with the situation that a parishioner discloses IPV. The response categories ranged from very unlikely to very likely on a 5-point scale (Cronbach’s alpha = 0.91).
Demographic data included gender, age, years living in the USA, marital status, denomination, church location (mid-West or mid-Atlantic), seminary training received and country of the training, and primary language (Korean, English, both Korean and English).
When the first stay-at-home order was issued in mid-March 2020 due to COVID-19, the majority (95%) of the study participants had finished the baseline survey. However, 53% of the intervention group was still completing the intervention with others at various study stages. Anticipating the impact of COVID-19 on the study participants’ ministry and ease of participation in the study, we included questions about the effects of COVID-19 in the 6-month survey. The questions asked about the impact of COVID-19 on conducting religious services, meeting with parishioners, their lives, and participating in the study. We also asked the intervention group participants whether COVID-19 affected their intention to ask community organizations to provide education on IPV for their congregation and their opportunities to use the knowledge and skills they learned from the intervention. Finally, the intervention group participants reported the ease of using the modules and their usefulness for their work as religious leaders.
Data Analyses
To examine whether participants in the intervention and the control groups differed at baseline, we used independent samples t-tests (age, years living in the USA, years in ministering, seven outcome variables) and chi-square tests (gender, marital status, denomination, seminary training received, primary language) (Dumville et al., 2006). To examine the intervention effect across the three time points (baseline, 3-month, and 6-month follow-up) for the two groups with respect to increasing knowledge, self-efficacy, attitude, outcome expectations, and prevention and intervention behaviors, we used a repeated measure mixed model ANCOVA, controlling for the church locations (McCoy, 2017; Stevens, 1996).
Results
Participant Flow
Figure 2 details the participant flow through the course of the study. Of the 110 participants who consented to participate, eight people dropped out before completing the baseline assessment. The remaining participants (N= 102) completed the baseline assessment and were randomized to either intervention (n = 53) or the control (n = 49). Of the 53 participants assigned to the intervention, 50 completed the 3-month follow-up assessment, and 49 completed the 6-month follow-up assessment (attrition rate of 7.5%). Of the 49 participants assigned to the control group, 48 completed the 3-month follow-up assessment, and 48 completed the 6-month follow-up assessment (attrition rate of 2%). Loss to follow-up of 5% or lower is considered of little concern, whereas a loss of 20% or greater can mean a potential bias (Dumville et al., 2006). We compared baseline demographic and outcome data of participants with complete and incomplete assessments; we found no significant differences between the two groups. Religious Leaders for Healthy Families: Consort Diagram.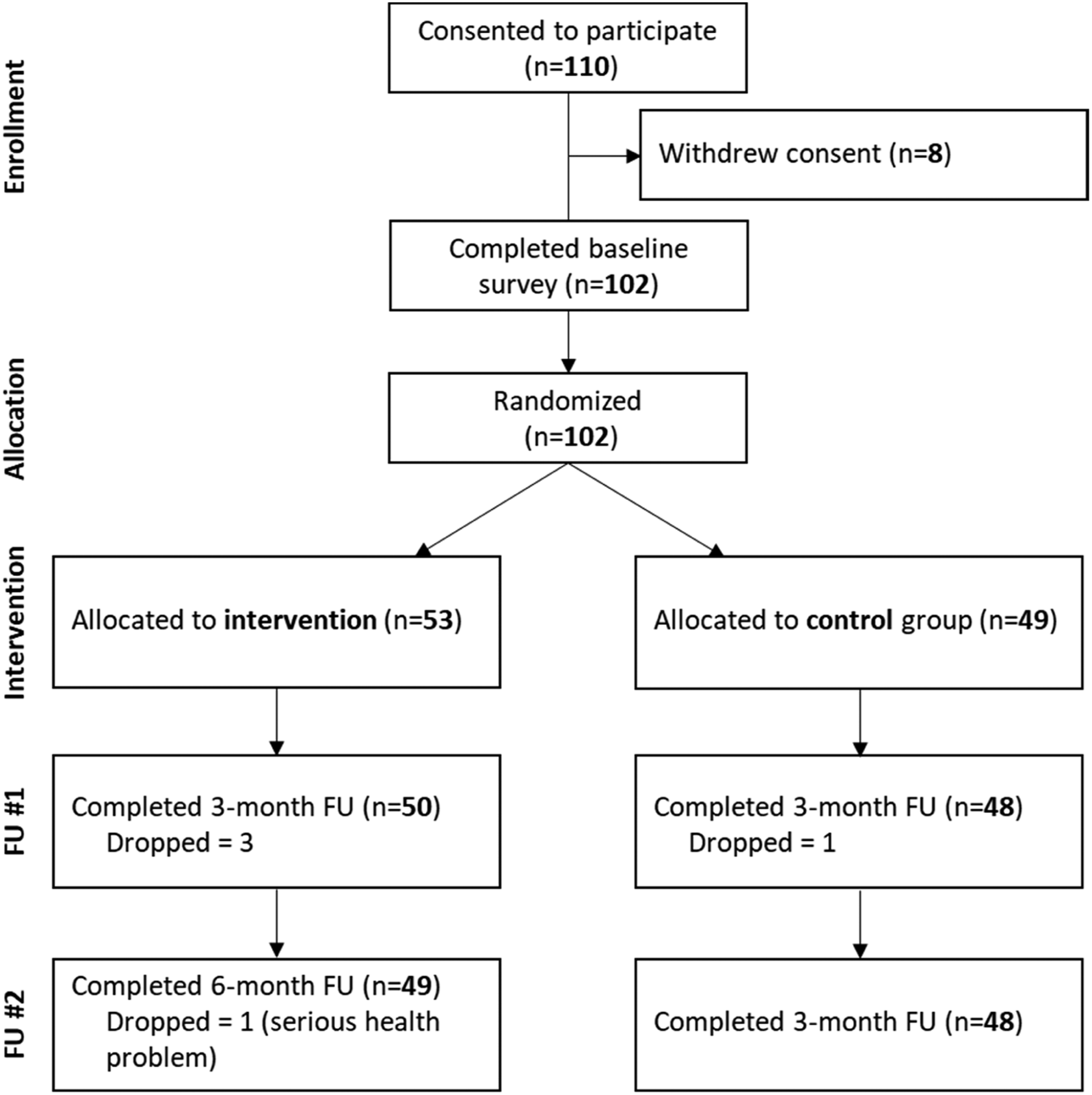
The study findings were based on an intent-to-treat approach that included all participants who completed the baseline assessment (n = 102). We conducted power analyses using G*Power (Faul et al., 2007). We can detect a small (.15) effect with 80% power (α < .05) with 74 participants. Given that the total sample size for this study will be 102, we are confident our analyses will be sufficiently powered.
Participant Demographic Characteristics
Most participants were male (93%), married (94%), and foreign-born (99%), with a mean of 21.4 years living in the USA. They received the seminary training (99%), and a majority of them noted that their primary language was Korean (65.7%), followed by both Korean and English (34.3%); all but one of them completed the surveys in Korean. Their mean age was 53 years. Fewer than half of the participants were Presbyterian (45.2%), followed by Baptist (22.6%) and Methodist (15.7%). The intervention and control groups did not differ significantly on demographic characteristics or the seven outcome variables at baseline.
Effects of Intervention on Outcome Measures
Means and Standard Deviations on Seven Outcome Variables at Baseline, 3-month, and 6-month Follow-up by Intervention Group.
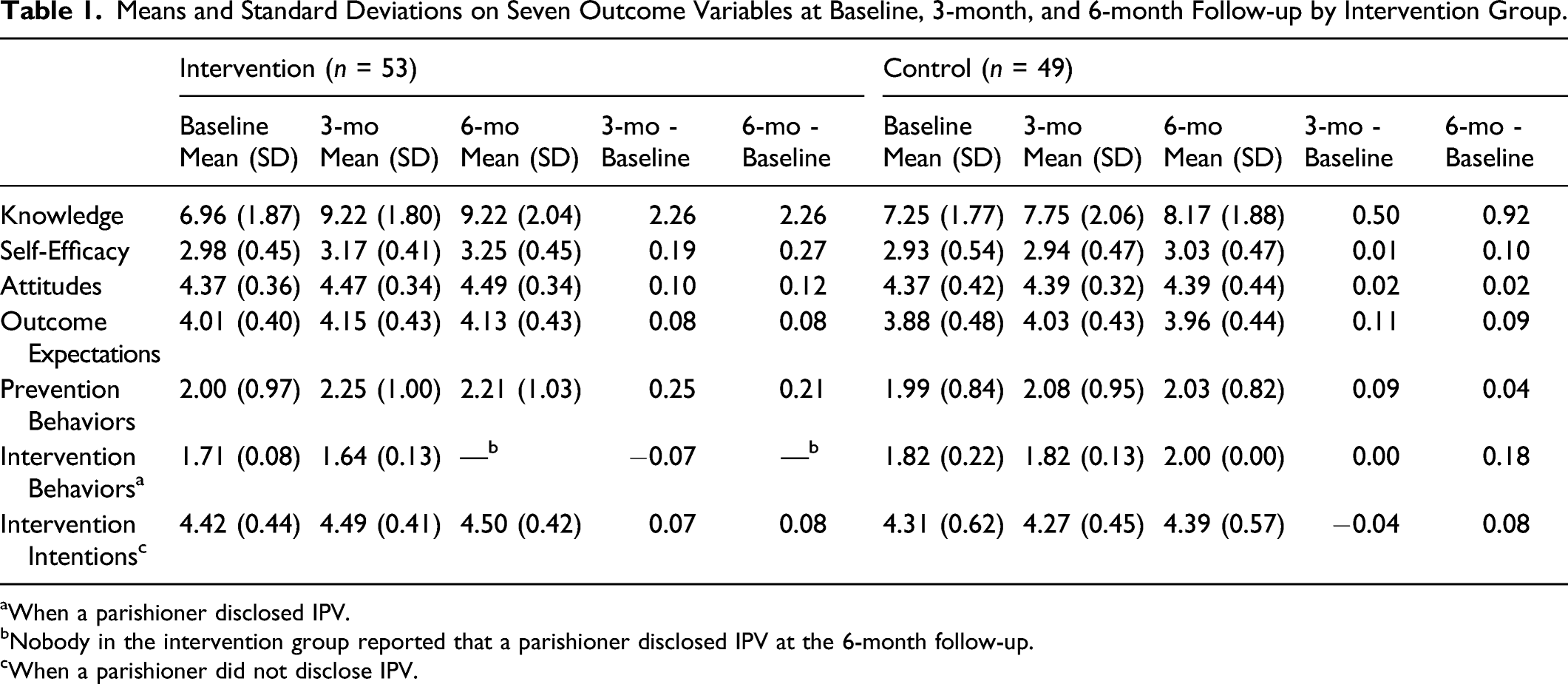
aWhen a parishioner disclosed IPV.
bNobody in the intervention group reported that a parishioner disclosed IPV at the 6-month follow-up.
cWhen a parishioner did not disclose IPV.
Fixed-Effect Tests for Model Terms.
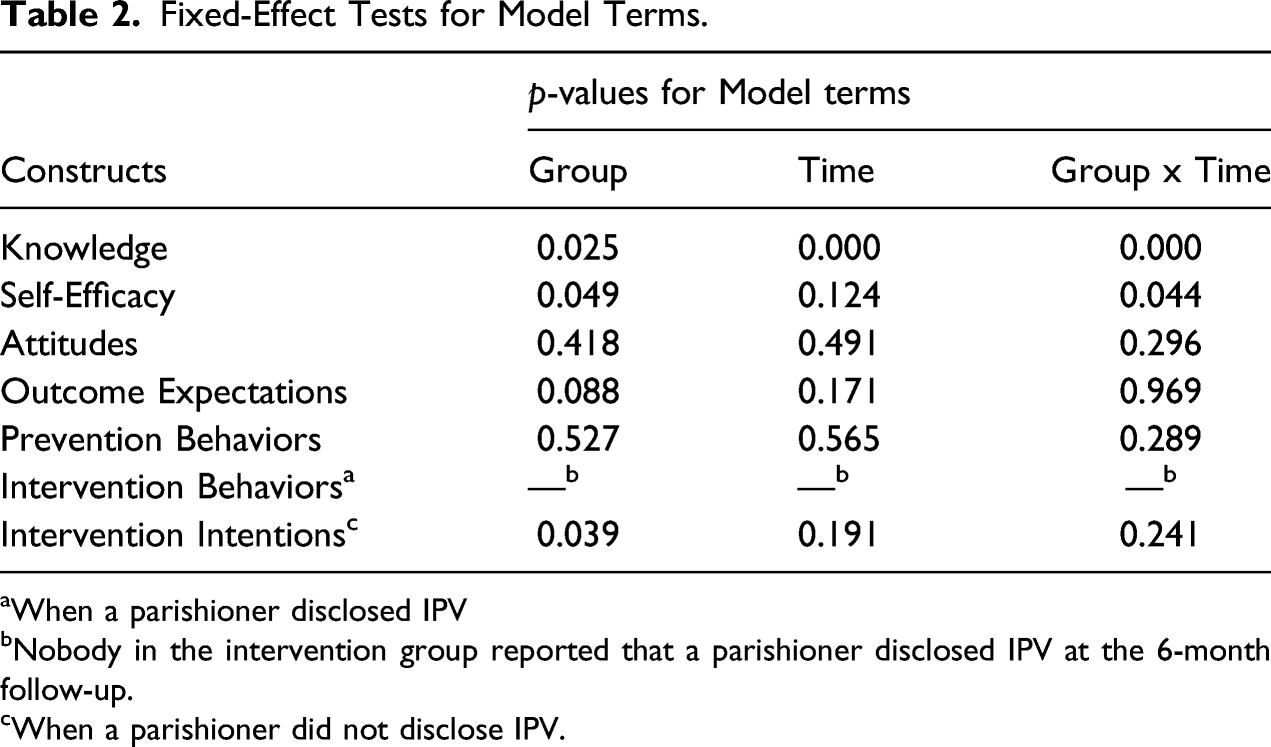
aWhen a parishioner disclosed IPV
bNobody in the intervention group reported that a parishioner disclosed IPV at the 6-month follow-up.
cWhen a parishioner did not disclose IPV.
Most importantly, the interaction term between group and time was significant for knowledge (p < .001) with small to medium effect size (η
p
2
= 0.09), and self-efficacy (p = .044) with small effect size (η
p
2
= 0.03). The mean for knowledge level for the intervention group was lower than that of the control group at baseline, but it was significantly higher than the control group at the 3-month and the 6-month follow-ups. Even though the mean of self-efficacy for the intervention group was comparable to that of the control group at baseline, it significantly improved over time; it was significantly higher than the control group at the 3-month and the 6-month follow-ups. In other words, the intervention group significantly improved their knowledge and enhanced self-efficacy more than the control group, as shown in Figure 3. For attitudes against IPV and prevention behavior, mean changes from baseline to the 3-month or the 6-month follow-up for the intervention group were higher than the control group (Table 1), but the differences were not statistically significant. The groups did not differ in outcome expectations at baseline, both groups increased their score at the 3-month assessment, and the difference widened at the 6-month assessment due to a slight drop in scores of the control group. An exploratory analysis between baseline and 6-month showed a significant increase in the intervention group. Group × time interaction plots for knowledge and self-efficacy. Note. Graphs use estimated marginal means controlling for the location of the church.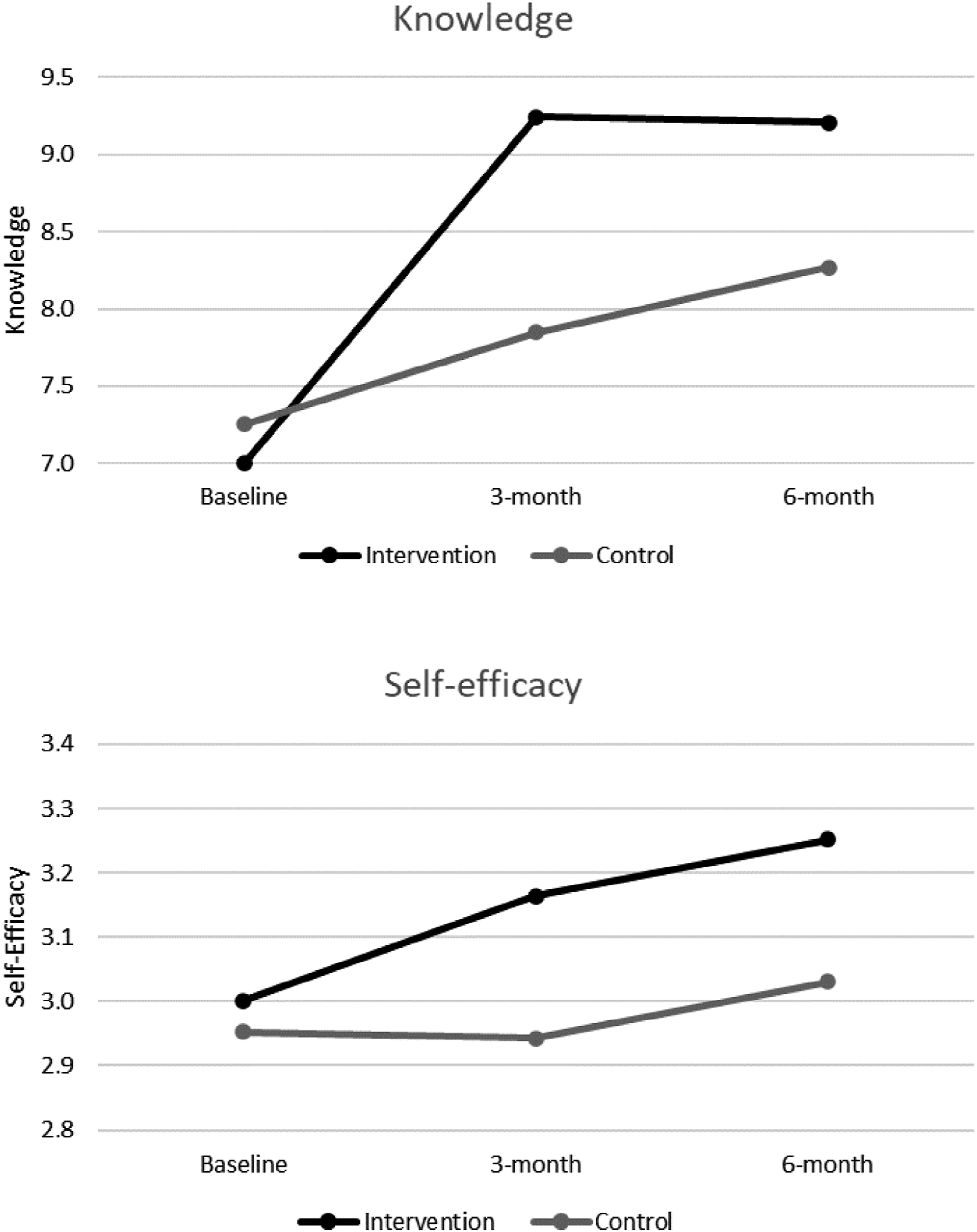
Impact of Covid-19
The majority of participants (85%) conducted their services online and met their parishioners via diverse methods: in-person (57%), email and text (63%), phone (73%), and video chat (60%). Ten participants (10%) reported not meeting their parishioners in person at all. The online survey and intervention facilitated participation in the study (53%), and some participants had extra time to participate because church services were closed (27%). However, COVID-19 had numerous adverse effects on study participation and the emotional functioning of the participants: fear of catching COVID-19 for self and family (51%), uncertainty about the future direction of their church (49%), financial strain (30%), burned out with the increased workload (26%), and overwhelmed with the need to respond to new situations (22%). In addition, due to COVID-19, it was difficult for the participants to answer some survey questions because they could not interact with parishioners in person (33%), and some were too busy to participate in the study fully (10%) and felt too stressed to concentrate on the study (6%).
For the intervention group participants, 65% were unable to invite community organizations to educate the congregation on IPV, and 39% reported that COVID-19 reduced their opportunities to use the knowledge and skills they had learned from the intervention.
Program Satisfaction
The intervention group participants found it easy to navigate the modules (96%) and thought the messages for interacting with potential survivors of domestic violence in the modules were clear (86%). Furthermore, they considered the modules (94%) and the accompanying Resource Booklet (94%) useful for their work as a religious leader.
Discussion
Our project aimed to increase scientific understanding by developing culturally responsive and technology-informed strategies to assist immigrant survivors of IPV in accessing justice and getting valuable services. This study examined the efficacy of an online simulation training for Korean American faith leaders—“Religious Leaders for Healthy Families”—designed to increase knowledge about IPV and healthy intimate partner relationships, enhance self-efficacy in IPV prevention and intervention, strengthen attitudes that support their roles on IPV prevention and intervention, increase positive outcome expectations of their actions, and increase behavioral intentions and behaviors on IPV prevention and intervention. In this randomized clinical trial, 102 Korean American faith leaders were randomly assigned to intervention or control groups. At the 6-month follow-up, faith leaders in the intervention group significantly increased their knowledge and self-efficacy in IPV prevention and intervention.
The online case simulation provided the foundation for increasing knowledge and confidence to prevent IPV and respond to survivors. Knowledge by itself will not change behaviors, but it is a precondition for change (Bandura, 2004). Perceived self-efficacy or confidence in adopting new behaviors is central to change (Bandura, 1977). The increase in self-efficacy attests to the development of the simulation, which provided immediate personalized feedback based on a participant’s choice (e.g., how specific responses may be harmful to the survivors), positive acknowledgment of failed attempts, modeling of ideal responses, and engaging pathways to additional resources. The four modules are short (about 15–20 minutes each) and easy to complete. In focus groups after the intervention, participants indicated that the modules were the start of the process of developing these skills. They asked for more in-person training and appreciated their connections with the domestic violence agency in their area.
Attitudes against IPV and intentions to intervene if a parishioner discloses IPV were very high at baseline (M = 4.3 out of 5 for attitudes and M = 4.4 out of 5 for intentions), which may have led to the ceiling effect; thus, they were difficult to increase. Past research shows problematic attitudes of faith leaders. Some Latino clergies believe that women could avoid being beaten if they change their behavior and advise abused women to submit to and remain with partners to preserve family unity (Ames et al., 2011; Behnke et al., 2012; Fuchsel, 2012). Muslim faith leaders consider abused women’s formal and external help-seeking behaviors as disloyal to the husband and the family (Kulwicki et al., 2010). Korean American faith leaders lack awareness of many barriers that IPV survivors, especially immigrant survivors, encounter if they decide to leave the abusive relationship. Pastors believe that addressing the needs of abused women is the responsibility of counselors and social workers, not clergy (Choi, 2015). Therefore, our study participants’ strong attitudes against IPV and beliefs in their active role in promoting the safety of IPV survivors and preventing IPV at the baseline is a welcome finding. This finding may indicate attitudinal changes among faith leaders over the past 10 years since the above-referenced studies.
The study findings on behavioral changes are inconclusive due to a lack of associated data from the closure of churches during the pandemic. This lack of behavioral effect stems from the complicated situation that most churches lived in during the COVID-19 pandemic. Pastors completed the online intervention in its entirety. However, the religious leaders had to close their church and pivot to online religious services with little to no training. The survey asked for two types of preventive behaviors. The first was communication with the parishioners about healthy relationships and their religious position against partner violence, and the second was to display information about the services of the domestic violence prevention agency. Both behaviors were challenging as they closed their church and juggled with technology. The intervention behaviors were also challenging when faith leaders were not interacting with parishioners in person. Thus, more research is needed to understand the impact of the intervention on behaviors.
Limitations
This study had some limitations. The sample size was relatively small, especially for certain variables. On every outcome variable, except the intervention behavior when parishioners disclosed IPV, mean changes from baseline to the 6-month follow-up for the intervention group were larger than the control group suggesting that we would have detected additional effects with a larger sample. The COVID-19 pandemic affected the study negatively, with study participants not having opportunities to practice the skills learned from the intervention. The study did not include external measures to cross-validate outcomes; all the measures were assessed by self-reports, and social desirability may have influenced participants’ responses. Lastly, a potential selection bias (pastors who agreed to participate may have been more open-minded and interested in this topic) and response bias is possible due to the lack of blinding of study participants; blinding would be impossible due to the nature of the intervention. While we addressed this potential problem by providing equal incentives for intervention and control groups, this problem remains a possible limitation.
Implications
Despite the limitations, the study results have four primary implications. First, “Religious Leaders for Healthy Families” has the potential to reduce disparities in accessing resources and services for immigrant survivors of IPV. Revealing IPV outside the family is considered a sign of personal failure that would shame the entire family for Korean American survivors. Therefore, Korean American immigrant women who suffer violence from their partners severely underutilize formal services such as women’s shelters, hotlines, police, and legal aid (Lee & Bell-Scott, 2009; Leung & Cheung, 2008). Faith leaders who feel confident to help survivors and implement IPV prevention activities can bring about real transformation in creating an environment that does not condone IPV and supports IPV survivors who report abuse (Choi et al., 2018). Faith leaders knowledgeable about barriers immigrant survivors of IPV face and available resources and services can be the bridge between survivors and service providers (Choi et al., 2018).
Second, with ease of use, this short, free online intervention has a high probability of uptake among faith leaders. “Religious Leaders for Healthy Families” is a brief online intervention with four easy to complete modules. Cost and distance have been identified as barriers to intervention uptakes (Pell et al., 2011), and online intervention eliminates these barriers to participation. Short interventions are cost-effective and have the potential to improve health promotion outcomes (Gc et al., 2016; Searight, 2009). For faith leaders who are busy with multiple issues vying for their attention, a modulized intervention that they can complete at a convenient time and location is likely more appealing than an all-day community education many IPV programs. For example, faith leaders can take only one module in one sitting for 15–20 minutes. The cost for providing the intervention is none, so IPV service providers can easily integrate it into their community education training. Further, “Religious Leaders for Healthy Families” can provide an excellent starting point for conversations with other faith leaders and a foundation to connect with other community organizations that work with IPV survivors.
Third, “Religious Leaders for Healthy Families” is the only culturally responsive intervention targeting Korean American community. We developed it in partnership with Korean American victim service organizations and extensive inputs from Korean American faith leaders via several studies conducted by us, making it relevant to Korean American faith leaders. It addresses cultural values that contribute to tolerating IPV, such as the priority of family interests over individual interests and the cultural expectation for women to endure hardship to preserve the family. Stigma and shame are attached to Korean American victims’ reluctance to seek help for IPV. The intervention helps faith leaders enhance their skills to engage in IPV prevention activities—for example, condemning IPV, sending supportive messages to victims during sermons, and inviting Korean American victim service organizations for IPV education. These behaviors would encourage Korean American victims to seek help from faith leaders.
Lastly, while “Religious Leaders for Healthy Families” increased the knowledge and self-efficacy of Korean American faith leaders, the program’s impact on the pastors’ behaviors and Korean American community members is currently unknown. Suppose we increase the capacity of Korean American faith leaders for IPV intervention and prevention. Would it strengthen Korean American community members’ attitudes that condemn IPV and decrease the stigma of seeking help for IPV? In addition, while a high proportion of Korean American immigrants in the United States are affiliated with Christian churches (Kim et al., 2001), those who are not cannot benefit from the program. Therefore, a more extensive follow-up study that combines “Religious Leaders for Healthy Families” with a community-wide intervention for all community members is warranted.
Footnotes
Acknowledgments
Our community partners have provided valuable feedback in every step of the intervention development, particularly Anna Bang and Jieun Han from KAN-WIN in Chicago and Ji-Young Cho, SooJinKim, and SuJung Park from KCSC in Greater Washington. Our thanks to Dool Soon Kim from the Korean Women’s Development Institute and to pastors for their feedback of the final modules.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institute of Justice, Office of Violence Against Women (Grant #: 2018-SI-AX-0003).