
Abstract
Latinx immigrants bear a disproportionate burden associated with intimate partner violence (IPV); however, efforts to develop evidence-based IPV prevention strategies and address health disparities have been impeded by a lack of understanding of the unique cultural (i.e., acculturation and acculturative stress) and socio-environmental (i.e., adverse childhood experiences [ACEs]) factors that contribute to IPV in this historically marginalized population. Guided by a contextual framework for IPV and a life-course perspective viewed through a gendered lens, this study aims to (a) identify relationships among acculturation, acculturative stress, ACEs, and IPV victimization and perpetration; and (b) explore whether profiles of IPV risk factors differ by gender (women vs. men) among Latinx immigrants. This cross-sectional, descriptive, correlational study was a secondary analysis of data from the baseline assessment of 331 ever-partnered Latinx immigrants aged 18 to 44 in a longitudinal study named Salud (Health), Estrés (Stress), y Resilencia (Resilency) (SER) Hispano. Logistic regressions adjusting for individual characteristics and gender subgroup analyses were used to address study aims. The majority of the participants were women (71.30%). More than half of all participants had experienced IPV victimization (57.70%) or IPV perpetration (60.73%). Latinx immigrants with higher family stress (adjusted odds ratio [aOR] = 1.16; p < .001) had an elevated risk for IPV victimization; those with more ACEs (aOR = 1.08; p = .005) had an increased risk for IPV perpetration. Women had a lower risk of IPV victimization (aOR = 0.45; p = .03) and a higher risk for IPV perpetration (aOR = 3.26; p = .001) compared to men. Although further research is warranted, the profiles of risk factors for IPV perpetration were different for women than for men. Culturally tailored preventions focused on acculturative stress and ACEs are needed to help Latinx immigrant communities minimize exposure to life-course adversities, improve positive adaptation to the US, and eliminate IPV-relevant health disparities.
Keywords
Intimate partner violence (IPV), defined as any behavior of an intimate partner that causes physical, emotional, sexual harm (World Health Organization [WHO,], 2012), is a public health problem globally. Within the US, IPV disproportionately affects the mental and behavioral health of historically marginalized populations. Latinx (i.e., gender-inclusive term for Hispanic/Latino; Merriam-Webster, n.d.) immigrants are faced with an increased vulnerability to IPV due to unique cultural factors including acculturation and traditional gender roles (Cummings et al., 2013), and social-environmental factors such as discrimination and poverty (González-Guarda et al., 2011). Additionally, they experience more severe types of IPV (Clark et al., 2016) and suffer more serious health consequences compared to other racial and ethnic groups (Reyes et al., 2021).
According to a recent review (Gonzalez et al., 2020), IPV is the most prevalent type of interpersonal violence experienced by Latinx populations, with a range of 4% to 80% across samples. Latinx individuals exposed to IPV are more likely than those without exposure to suffer behavioral and mental health challenges including substance abuse, higher risk for HIV, and worse mental health outcomes (known as the SAVA syndemic; González-Guarda et al., 2011). Negative health effects of IPV can persist after leaving the abusive partners (Garcia-Moreno et al., 2006). National data show that Latinx victims of IPV-related homicide are more likely to be immigrants than their non-Hispanic White counterparts (Sabri et al., 2021), so efforts aimed at prevention, especially primary prevention, are urgently needed to address IPV in this group.
Failure to understand the unique contributing factors to IPV, especially those relevant to immigration (i.e., acculturation and acculturative stress) and adversity experienced in early life (i.e., adverse childhood experiences [ACEs]), from a life-course perspective has impeded efforts to develop evidence-based prevention strategies to address this urgent health issue among the Latinx immigrant community. Recent Latinx immigrants report less exposure to IPV than Latinx immigrants with longer residence in the US, and research suggests that acculturation to American culture is a driving risk factor for IPV in this population (Alvarez et al., 2020; Mancera et al., 2017). Nevertheless, little is known about the relative contribution of acculturation versus the stress associated with this process (i.e., acculturative stress). Additionally, research exploring the influence of acculturation on IPV risks has seldom considered the influence of life-course exposure to other stressful experiences, such as childhood and immigration-related adversity.
Background
Theoretical Framework
The current study was guided by the contextual framework for IPV (Bell & Naugle, 2008) and a life-course perspective (Elder, 1998) viewed through a gendered lens. The contextual framework for IPV highlights proximal risk factors related to IPV, such as stressors, which are modifiable and thus can serve as potential targets of prevention strategies. For Latinx immigrants, acculturation, a salient cultural stressor that captures adversity relevant to immigration, can give rise to stress in every aspect of life (Cervantes et al., 2016) and potentially increase conflicts in intimate relationships. IPV can be viewed as a maladaptive way to cope with stress. The life-course perspective (Elder, 1998) purports that the historical context of an individual’s life changes constantly across the life span, which led us to consider the extent to which early-life socio-environmental risks, indicated by childhood adversities, were significant contributors to IPV. The combination of these two guiding approaches led us to conceptualize that IPV stems from childhood adversities and develops under the chronic and intense stress of the acculturation process, cumulatively contributing to health disparities, especially for those living in a disadvantaged environment characterized by discrimination, poverty, and limited access to services, as is often the case for Latinx immigrants. We also considered that IPV victimization and IPV perpetration were likely to co-occur (Langhinrichsen-Rohling et al., 2012) due to relationship conflicts attributable to the immigration process and life-course adversities.
In acknowledgment that IPV is a gendered phenomenon, we conceptualized that the relationships described above could differ by gender. Traditional gender roles remain a shared contributor to IPV despite the great diversity across Latinx cultures. These gender roles, driven by gender inequality, tend to reinforce power imbalance within intimate relationships where women are often submissive to men and further are at risk of IPV victimization (Cummings et al., 2013; Mancera et al., 2017). Specifically, Latinx women primarily take care or even sacrifice for the family, whereas men take the role of decision-makers, as captured by terms describing gender roles for Latinx women (Marianismo) and men (Machismo). However, traditional gender roles are not always harmful. Machismo, for example, can prevent Latinx men from perpetrating IPV if its beneficial and positive attributes, such as responsibility and respect for partner and family, are embraced and practiced (Cummings et al., 2013; Mancera et al., 2017).
Our theoretical framework (a) provides additional insights into the health disparities and marginalization of Latinx immigrants by providing a life-course picture of their adversities, and (b) informs future development of culturally tailored IPV prevention strategies by addressing the unique cultural and socio-environmental risks specific to this group. We reviewed relevant literature on acculturation, acculturative stress, ACEs, and IPV below. Given the limited evidence specific to Latinx immigrants, we included research more inclusive of Latinx individuals, both immigrants and US-born, but we are aware that these groups can be distinct in their IPV prevalence and risk (Gonzalez et al., 2020; Sabina et al., 2015).
Acculturation and IPV
There is considerable interest in acculturation and its impact on the health domains of Latinx populations, yet evidence concerning their relationships (including that specific to IPV) generally remains contradictory. Acculturation is defined as a multidimensional process by which individuals change in their “practices, values, and identifications” when they contact a new culture while maintaining their culture of origin (Schwartz et al., 2010, p. 237). Research focused on the role acculturation plays in IPV among Latinx immigrants is inconclusive and underrepresented in the current literature. Some evidence suggests that acculturation to U.S. culture (hereafter acculturation to the US) protects Latinx immigrant women from IPV victimization (Frías & Angel, 2012), yet other research argues that retaining Hispanic culture (hereafter Hispanicism/enculturation) is protective, especially for immigrant women (Sabina et al., 2015). Acculturation adds to the risk for IPV victimization among Latinx individuals, although the magnitude of the association differs by gender as indicated in a recent meta-analysis (Alvarez et al., 2020). A review focused on Latinx men identified acculturation as a risk factor for IPV perpetration (Mancera et al., 2017); however, the scant evidence among Latinx women was not consistent. Some evidence suggests that acculturation is not associated with IPV perpetration among women (Cunradi, 2009; Grest et al., 2018); other research supports an association (Caetano et al., 2007). Several limitations concerning the conceptualization and measurement of acculturation might have contributed to these inconsistencies. The complex process of acculturation is often simplified to a unidimensional concept that captures only acculturation to the US, leaving Hispanicism/enculturation unexamined. Proxies of acculturation, such as time in the US and language proficiency, are often used rather than validated instruments (Alvarez et al., 2020). These limitations must be addressed in order to advance our understanding of the role of acculturation in relation to IPV.
Acculturative Stress and IPV
Acculturative stress refers to the stress that individuals experience as they respond to stressors during the acculturation process (Gonzalez-Guarda et al., 2021) and is less appreciated in IPV literature compared to acculturation. Acculturative stress is a construct related to acculturation, but one should not assume that it is an expected outcome of acculturation (Rudmin, 2009); it can have distinct and independent effects on IPV, separate from those caused by acculturation. Furthermore, acculturative stress offers a plausible explanation for the inconsistent evidence on acculturation and health outcomes including IPV; the level of stress is deterministic to poor health and exposes Latinx individuals to high risk for IPV (Alvarez et al., 2020). Latinx immigrants are commonly faced with chronic stress arising from conflicts in cultural expectations and discrimination in all aspects of their lives, including relationships, work, and health, as they navigate the U.S. context (Cervantes et al., 2016) despite significant diversity in their culture and acculturation. In addition, different types of acculturative stress are likely to co-occur and further deteriorate the health of Latinx immigrants (Cervantes et al., 2016; Salas-Wright et al., 2015), which highlights the need to capture a comprehensive picture of acculturative stress to clarify its impact on IPV.
Current evidence generally supports that acculturative stress contributes to an elevated risk for IPV victimization and perpetration among the Latinx population. A review focused on IPV perpetration among Latinx men identified acculturative stress as a risk factor (Mancera et al., 2017), and empirical studies have revealed that acculturative stress adds to the risk for IPV perpetration and victimization across gender groups among Latinx individuals (Caetano et al., 2007; Gonzalez-Guarda et al., 2013). Nevertheless, apart from the impact of acculturation, the contribution of acculturative stress to IPV and the specific types of acculturative stress that are most predictive for IPV remain unclear.
ACEs and IPV
ACEs are a well-established risk factor for IPV victimization and perpetration cross-culturally (Smith-Marek et al., 2015), including in the general U.S. population (Capaldi et al., 2012) and the Latinx population (Cummings et al., 2013). ACEs are defined as intensive and stressful life events experienced before 18 years of age, including child maltreatment, household dysfunction, and violence in the living environment (e.g., peer, community, or collective violence) (WHO, 2018). Latinx individuals experience higher rates of ACEs compared to non-Hispanic White individuals (Llabre et al., 2017), with rates of childhood maltreatment ranging from 16% to 69% and of sexual abuse ranging from 16% to 79% in this group (Gonzalez et al., 2020). Most previous studies have relied on ACEs measures that only capture aspects of child maltreatment and household dysfunction. Missing from the conceptualization and measurement of ACEs in these studies is adversity at the level of community or experienced collectively. This aspect of ACEs is particularly relevant to Latinx immigrants, as escaping violence at their country of origin has been cited as a major reason for their immigration to the US (Keller et al., 2017), where they may be subjected to further violence upon arrival (Simmons et al., 2015). The broader socio-environmental context during childhood is a crucial factor known to affect IPV in adulthood (Davis et al., 2021; Sabina, 2013). Additionally, our current sample resided in U.S. South and was heavily affected by regional anti-immigration sentiment that can contribute to an elevated level of environmental violence. Future research should account for environmental violence to ensure a comprehensive appreciation of the relationship between ACEs and IPV in this historically marginalized group.
Current Study
Informed by the contextual framework for IPV (Bell & Naugle, 2008) and a life-course perspective (Elder, 1998) viewed through a gendered lens, the current study fills gaps in the literature by expanding knowledge of the relative contributions of acculturation and its associated stress (i.e., acculturative stress) as well as of the influence of life-course exposure to other stressful experiences (i.e., ACEs) on IPV risks. Specifically, the aims of our study were to (a) identify relationships among acculturation, acculturative stress, ACEs, and IPV victimization and perpetration, and (b) explore whether the profile of factors associated with IPV victimization and perpetration differs by gender (women vs. men) among Latinx immigrants.
Methods
Study Design
This cross-sectional, descriptive, correlational study was a secondary analysis of data from the baseline assessment of adult Latinx immigrants participating in a longitudinal, observational study named Salud (Health), Estrés (Stress), y Resilencia (Resilency) (SER) Hispano. Baseline data were collected from May 2018 to January 2020. Variables, including IPV, acculturation, acculturative stress, ACEs, and individual characteristics (i.e., gender, sociodemographic, relationship, and immigration-relevant variables) were used to address the study aims. This study was approved by Duke Health Institutional Review Board. After obtaining informed consent, trained bilingual research team members conducted the data collection in Spanish or English according to each participant’s preference.
Sample
The SER sample consisted of 391 community-dwelling Latinx immigrants. Participants were recruited in partnership with Hispanic community organizations using community-based recruitment strategies, including attending cultural events or other programs and disseminating recruitment flyers via culturally relevant media such as Latinx-targeted local newspapers, listservs, and social media. Participants were included in the SER study if they (a) self-identified as Latino/a or Hispanic; (b) had migrated from Latin America/Caribbean to the US; (c) had lived in the US for at least 1 year; and (d) were between 18 and 44 years of age when enrolled. Participants were excluded if they planned to move to another geographic area within the next 2 years. The current analysis sample, however, includes only those participants who were ever partnered in the past 6 months at baseline (N = 331). Researchers either read the questions and options to participants or let them self-administer the survey on a tablet based on their preference. Other details of data collection are published elsewhere (González-Guarda et al., under review).
Measures
Each measure matched the definition of respective concept and was culturally and linguistically adapted for Latinx immigrants. Adaptation details are published (Nagy et al., 2021).
IPV victimization and IPV perpetration
The adapted version of Short Form Revised Conflict Tactics Scale for Latinx populations (CTS2S; McCabe et al., 2016; Straus & Douglas, 2004) was used to measure physical (14 items), emotional (8 items), and sexual violence (2 items). Participants were asked to rate the frequency of violent behaviors by their partners toward them (victimization), and by them toward their partners (perpetration) in the past 6 months on a 4-point Likert scale (0 = never to 4 = three or more times). Example items included “[Your partner] slapped, kicked, bit, or hit you”; “You sulked or refused to talk about an issue”; and “You forced him/her to have sex.” The scale demonstrated great reliability among Latinx immigrants, with an internal consistency of 0.87 (González-Guarda et al., under review). The primary outcomes were derived using one scoring method suggested by scale developers (Straus & Douglas, 2004). Each of the 24 items was recoded as 0 = never or 1 = one or more times. Binary IPV victimization and IPV perpetration outcomes, each coded as 0 = no exposure and 1 = exposure to any type of IPV, were derived from the 12 victimization and 12 perpetration items, respectively.
Acculturation
The Bidimensional Acculturation Scale for Hispanics (Marin & Gamba, 1996) was used, which enabled us to measure degree of acculturation based on two cultural dimensions: Hispanicism/enculturation (12 items) and Americanism/acculturation to the US (12 items). Items were focused on language use, linguistic proficiency, and electronic media use in Spanish and English, respectively, for each domain. Example items included: “How often do you speak in Spanish/English with your friends?” “How well do you speak Spanish/English?” and “How often do you listen to music in Spanish/English?” Participants were asked to rate each item on a 4-point Likert scale (1 = almost never/very poorly, 4 = almost always/very well). Mean scores for Hispanicism and Americanism were calculated, with each having a possible range from 1 to 4. This instrument has excellent performance in validity and reliability among Latinx individuals (Marin & Gamba, 1996). The scale demonstrated good internal consistency in current sample, as indicated by a Cronbach’s alpha of 0.70 for Hispanicism and 0.95 for Americanism.
Acculturative stress
The Hispanic Stress Inventory 2 Immigrant Version (Cervantes et al., 2016) was used. It measures 10 domains of psychosocial stress associated with the acculturation process comprehensively and shows high reliability and construct validity among diverse Hispanic groups. Specifically, this 90-item scale was used to measure: parental stress (13 items), occupation and economic stress (12 items), marital stress (12 items), discrimination stress (11 items), immigration stress (9 items), marital acculturation gap stress (9 items), health stress (8 items), language-related stress (6 items), premigration stress (6 items), and family stress (5 items). Example items included “My spouse has expected me to be more traditional in our relationship,” “I was treated ‘less than’ other Americans because I am Hispanic/Latino,” and “I have felt as though I would never see some family members ever again.” Participants were first asked to indicate whether they had experienced the stressor described in each item in the past 6 months, and if so, to rate their level of concern on a 5-point Likert scale (1 = not at all worried to 5 = extremely worried). If they had not experienced a stressor, the score for that item was coded as 1. We derived a subscale score for each domain by summing the items comprising the subscale, with higher scores indicating a greater degree of stress. The internal consistency of the domains was satisfactory in our sample, with Cronbach’s alphas ranging from 0.69 to 0.88.
Adverse childhood experiences
The Adverse Childhood Experience International Questionnaire (ACE-IQ; WHO, 2018), developed to allow cross-country usage, was adapted. The adapted ACE-IQ used 31 items to assess experiences beyond child maltreatment (e.g., physical, emotional, and sexual abuse, and neglect) and household dysfunction (e.g., incarcerated household members, household violence, parental death, or separation); it also captured peer, community, and collective violence. Exemplary items included: “Did someone actually have oral, anal, or vaginal intercourse with you when you did not want them to?” “Did you see or hear someone being stabbed or shot in real life?” and “Were you beaten up by soldiers, police, militia, or gangs?” Three response formats were used across the 31 items, including dichotomous responses (0 = no, 1 = yes), 4-point Likert scale (0 = never to 4 = many times), and 5-point Likert scale (0 = never to 5 = always). From these, a binary score per item was derived, with 0 = no exposure and 1 = exposure. These binary scores were summed to determine the total number of ACEs, ranging from 0 to 31. The Cronbach’s alpha for the total score was 0.88 in our sample, indicating excellent reliability.
Individual characteristics
Sociodemographic, relationship, and immigration relevant variables were used. Candidate covariates were decided based on empirical evidence on risk factors for IPV among the U.S. population (Capaldi et al., 2012) and specific to Latinx groups (Cummings et al., 2013; Gonzalez-Guarda et al., 2013), including sociodemographic (i.e., age, sexual preferences, number of children, education, current employment, and monthly household income) and relationship variables (i.e., marital status and multiple partners). In addition, immigration-relevant variables (i.e., age of immigration and years in the US) were chosen a priori as covariates as they capture unique aspects of immigration with potential impact on IPV (Alvarez et al., 2020). Gender was also selected a priori as we conceptualize IPV to be gendered. Of note, we aim to be inclusive for gender diverse individuals by offering numerous options for gender (man/woman/transgender man/transgender woman/gender nonconforming/other).
Statistical Analysis
Descriptive statistics were used to detail individual characteristics, risk factors (acculturation, acculturative stress, and ACEs), and IPV outcomes (victimization and perpetration). Nondirectional statistical tests were performed with significance set at 0.05, with one exception: significance was set at 0.10 to identify individual characteristics to be included as covariates in the initial multivariable logistic regression examining the relationship of the risk factors with each IPV outcome. All analyses were conducted using SAS 9.4.1 (Cary, NC).
Bivariate logistic regression was conducted to examine the relationship of each individual characteristic with each IPV outcome and to determine covariates for subsequent models. Of note, gender and the two immigration-relevant variables were incorporated as covariates regardless of their statistical significance to assess their impact on IPV outcomes. Further, we controlled for IPV perpetration when examining IPV victimization as an outcome and vice versa because these are likely to co-occur due to relationship conflicts. We also examined the differences in IPV outcomes by documentation status using bivariate logistic regressions. This was conducted and reported solely to provide additional context for our study findings in acknowledgment of the potential influence of documentation status on IPV disclosure among Latinx immigrants.
We applied bivariate logistic regression to examine the simple relationship of each risk factor with each IPV outcome. Odds ratios (ORs) and their 95% confidence intervals (CIs) were used to address effect size. To screen for multicollinearity among risk factors, we conducted Spearman correlations with a correlation coefficient of ±0.70 or higher indicating collinearity.
The next step was an initial multivariable logistic regression analysis to examine the relationship of each risk factor with each IPV outcome, after controlling for the effects of the other risk factors and covariates. The initial model for each outcome was then reduced to a final parsimonious model using an iterative backward elimination method with a stay criterion of 0.05. Adjusted odds ratios (aORs) and their 95% CIs were derived.
We conducted gender subgroup analyses to explore the relationships of 13 risk factors for each IPV outcome to identify risk factors unique to women and men. For each gender subgroup, covariates were identified using bivariate logistic regression between individual characteristics and each IPV outcome. We also controlled for the two immigration-relevant variables and the other IPV outcome described above. The initial multivariable logistic regression model for each IPV outcome was conducted for women and men separately. Later, each initial model was reduced to final parsimonious model using the backward elimination method as described earlier.
Results
Individual Characteristics
The majority of participants self-identified as women (71.30%; 234 cisgender and 2 transgender women) and heterosexual (92.00%) with at least one child (74.92%). The mean age was 34.47 years (SD = 6.52, range = 18.00–45.00). Nearly half were from a relatively low-socioeconomic background; specifically: 41.39% had an education of less than high school, and 42.27% had a monthly household income of less than $1,999. Furthermore, approximately one-fourth were unemployed (25.98%). Most were in a relationship (80.24%) and had only one partner in the prior 6 months (92.42%). On average, they were 20.50 years old at the time of immigration (SD = 8.20, range =0–42.00) and had been in the US for 13.55 years (SD = 7.05, range = 1.00–38.00). Over one-third were undocumented (36.30%). More than half were from Mexico (54.98%), followed by Honduras (10.57%) and EI Salvador (6.95%). They immigrated to be with family (31.12%) or for financial prospects (28.70%). See Supplemental Appendix A Table S1 for details.
IPV Victimization and Perpetration
Among the 331 participants, 191 (57.70%) had experienced IPV victimization, and 201 (60.73%) reported IPV perpetration in the prior 6 months: specifically, victimization only (n = 24, 7.25%), perpetration only (n = 34, 10.27%), both victimization and perpetration (n = 167, 50.45%), and no victimization or perpetration (n = 106, 32.02%). Documentation status was associated with IPV victimization (p = .04), but it did not influence IPV perpetration (p = .15).
Covariates
We identified education, monthly household income, and marital status as covariates in the initial multivariable regression model for IPV victimization based on bivariate logistic regression results (all p ≤ .10) along with the covariates chosen a priori (i.e., gender, age of immigration, years in the US) and IPV perpetration. Marital status was the only other covariate incorporated in the initial model for IPV perpetration (p ≤ .10) besides those covariates identified a priori and IPV victimization. See Supplemental Appendix A Table S1 for details.
Risk Factors and IPV
The mean ACEs total score was 10.04 (range =0–30.00), and the respective means for Hispanicism (range = 2.08–4.00) and Americanism (range = 1.00–4.00) were 3.43 and 2.48, respectively. Because the acculturative stress scores were skewed, we presented the median, 25th, and 75th percentile scores for each of the 10 domains (see Table 1).
Factors Associated with IPV Victimization and IPV Perpetration: Bivariate Logistic Regression Results.
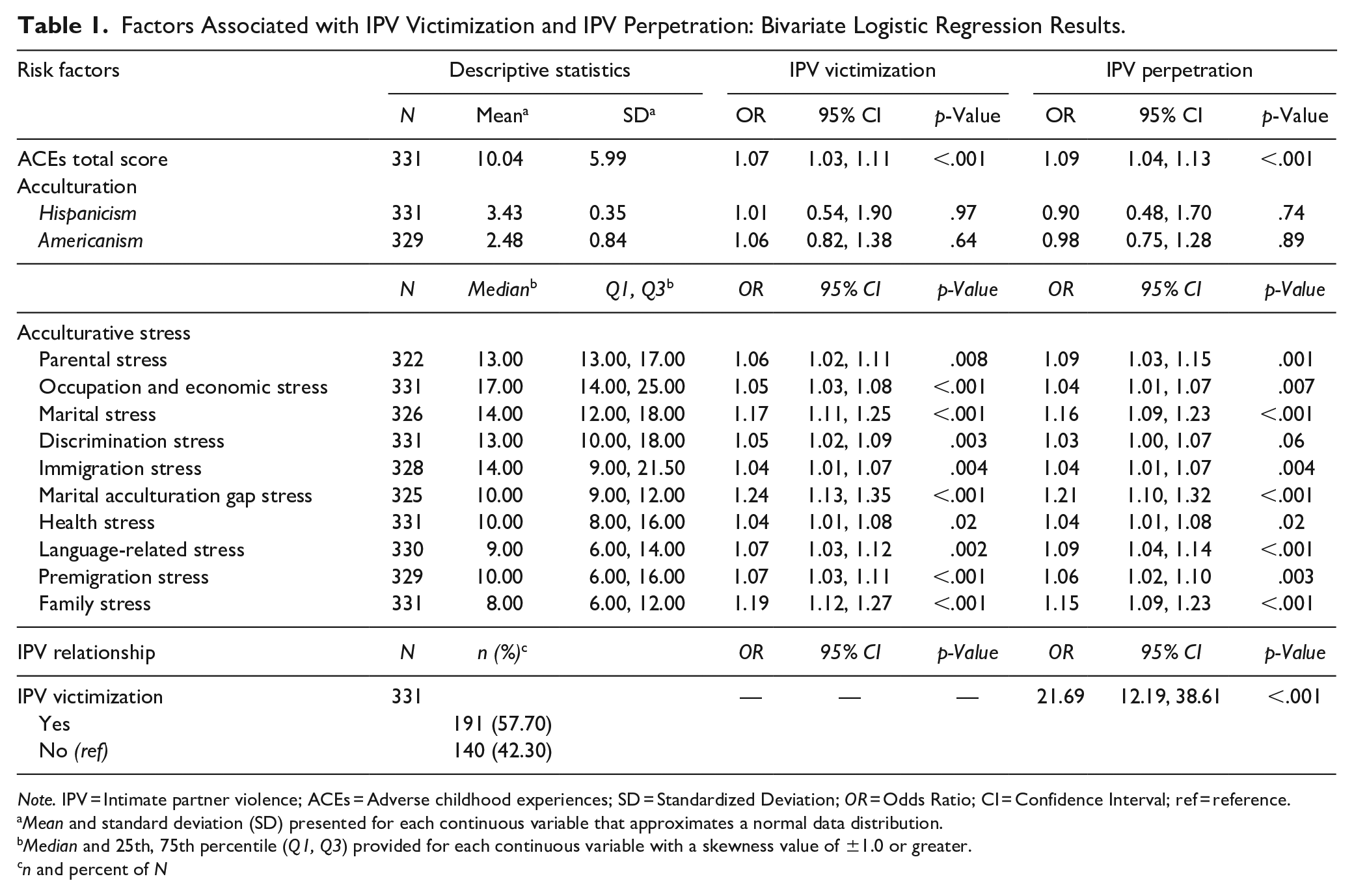
Note. IPV = Intimate partner violence; ACEs = Adverse childhood experiences; SD = Standardized Deviation; OR = Odds Ratio; CI = Confidence Interval; ref = reference.
Mean and standard deviation (SD) presented for each continuous variable that approximates a normal data distribution.
Median and 25th, 75th percentile (Q1, Q3) provided for each continuous variable with a skewness value of ±1.0 or greater.
n and percent of N
Bivariate logistic regression indicated that the profile of significant risk factors was the same for both IPV victimization and perpetration (all p < .05; see Table 1). Increased risk for each IPV outcome was associated with a greater number of ACEs and greater acculturative stress in all 10 domains. Acculturation (Hispanicism and Americanism) scores were not associated with either IPV outcome. All 13 risk factors were retained for inclusion in the initial multivariable logistic regression models because multicollinearity was not deemed a concern as no Spearman correlation coefficients were ±.70 or higher (Supplemental Appendix B Table S2).
The initial multivariable model included the 13 risk factors and covariates detailed earlier (Supplemental Appendix C Table S3). The IPV victimization model included seven covariates, and the IPV perpetration incorporated five. The initial model indicated that individuals who had increased family stress, identified as men, and those who reported IPV perpetration were at significantly higher risk for IPV victimization after controlling for other factors and covariates (all p < .05). In contrast, the risk for IPV perpetration was significantly greater for women and those who had experienced IPV victimization (all p < .05).
The results from the final parsimonious models (Table 2) further demonstrated that increased risk for IPV victimization was associated with greater family stress (aOR = 1.16; p < .001) and that women had a lower risk of IPV victimization compared to men (aOR = 0.45; p = .03). Men were 2.2 times more likely to experience victimization than woman. The parsimonious models for IPV perpetration (Table 2) further supported that those with more ACEs (aOR = 1.08; p = .005) had an elevated risk for perpetration. Interestingly, women had a higher risk of perpetrating IPV compared to men (aOR = 3.26; p = .001). IPV victimization was the strongest predictor for IPV perpetration (aOR = 26.05; p < .001).
Final Parsimonious Logistic Regression Models for IPV Victimization and IPV Perpetration.
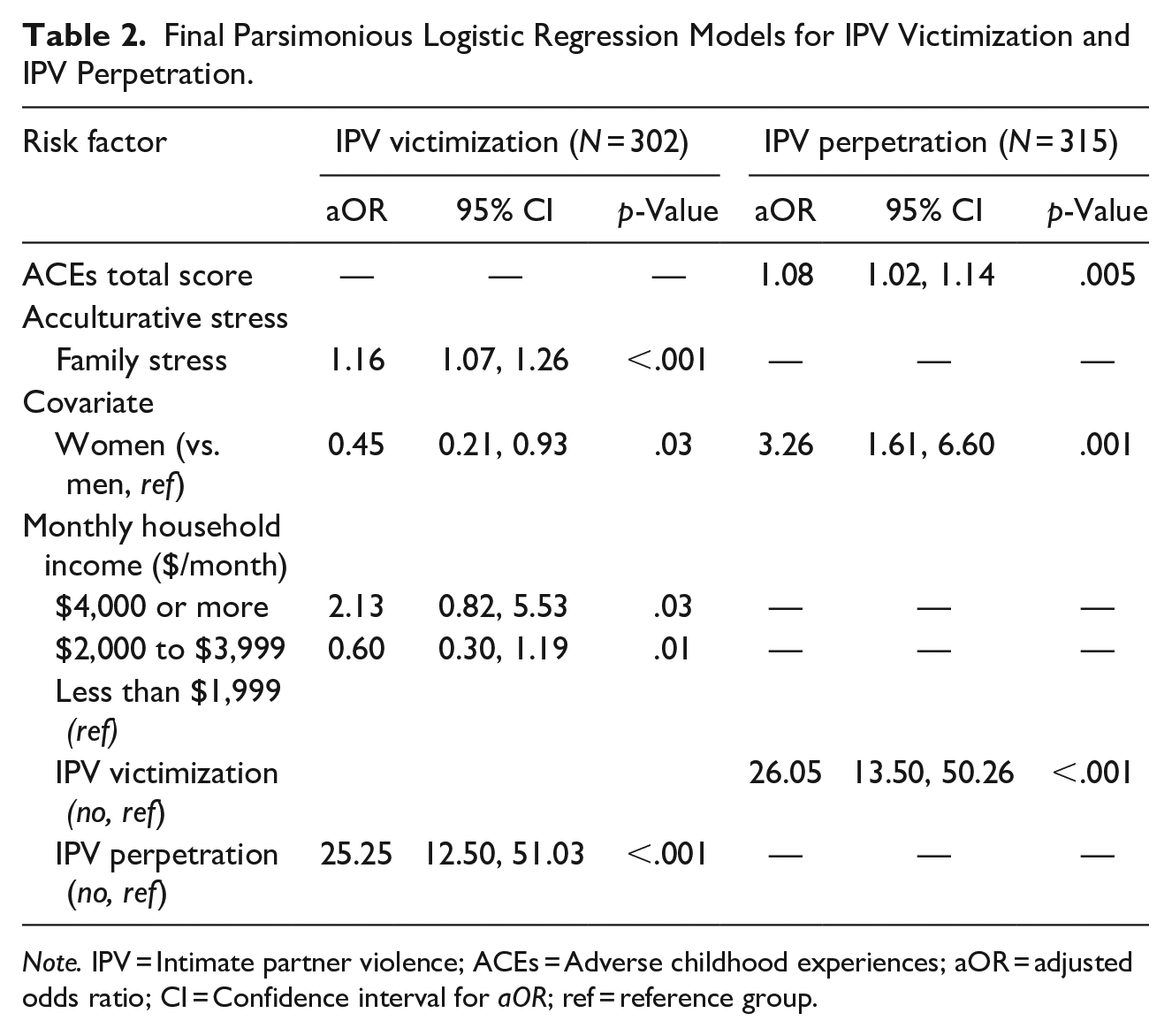
Note. IPV = Intimate partner violence; ACEs = Adverse childhood experiences; aOR = adjusted odds ratio; CI = Confidence interval for aOR; ref = reference group.
Subgroup Analysis by Gender
We did not conduct analyses on the moderating effects of gender on the relationships between the 13 risk factors and IPV outcomes due to the lack of hypotheses regarding moderation, the number of risk factors of interest, small sample size per gender group, and insufficient statistical power. However, we did explore whether the profile of factors associated with IPV outcomes differed by gender with a focus on reporting effect sizes. The initial logistic regression for IPV victimization included marital status as a covariate for women (p < .10) and none for men; models for IPV perpetration included education and marital status for women and monthly household income for men (all p < .10). Table 3 presents the final parsimonious model for each IPV outcome. Increased risk for IPV victimization was significantly associated with marital stress and IPV perpetration in both women and men (all p < .03). The profile for IPV perpetration was different for women and men, with the exception that the risk for perpetration was 25 (women) to 50 (men) times greater for those who had experienced IPV victimization relative to those who had not. IPV perpetration risk for women was higher among those with greater level of acculturation to the US, marital stress, and language stress (all p < .04). Women with greater discrimination stress were less likely to report IPV perpetration (p = .02). In contrast, IPV perpetration risk in men was significantly reduced among those with higher Hispanicism but was elevated among men with greater premigration stress (all p < .02).
Subgroup Analysis: Final Parsimonious Models for IPV Victimization and IPV Perpetration.
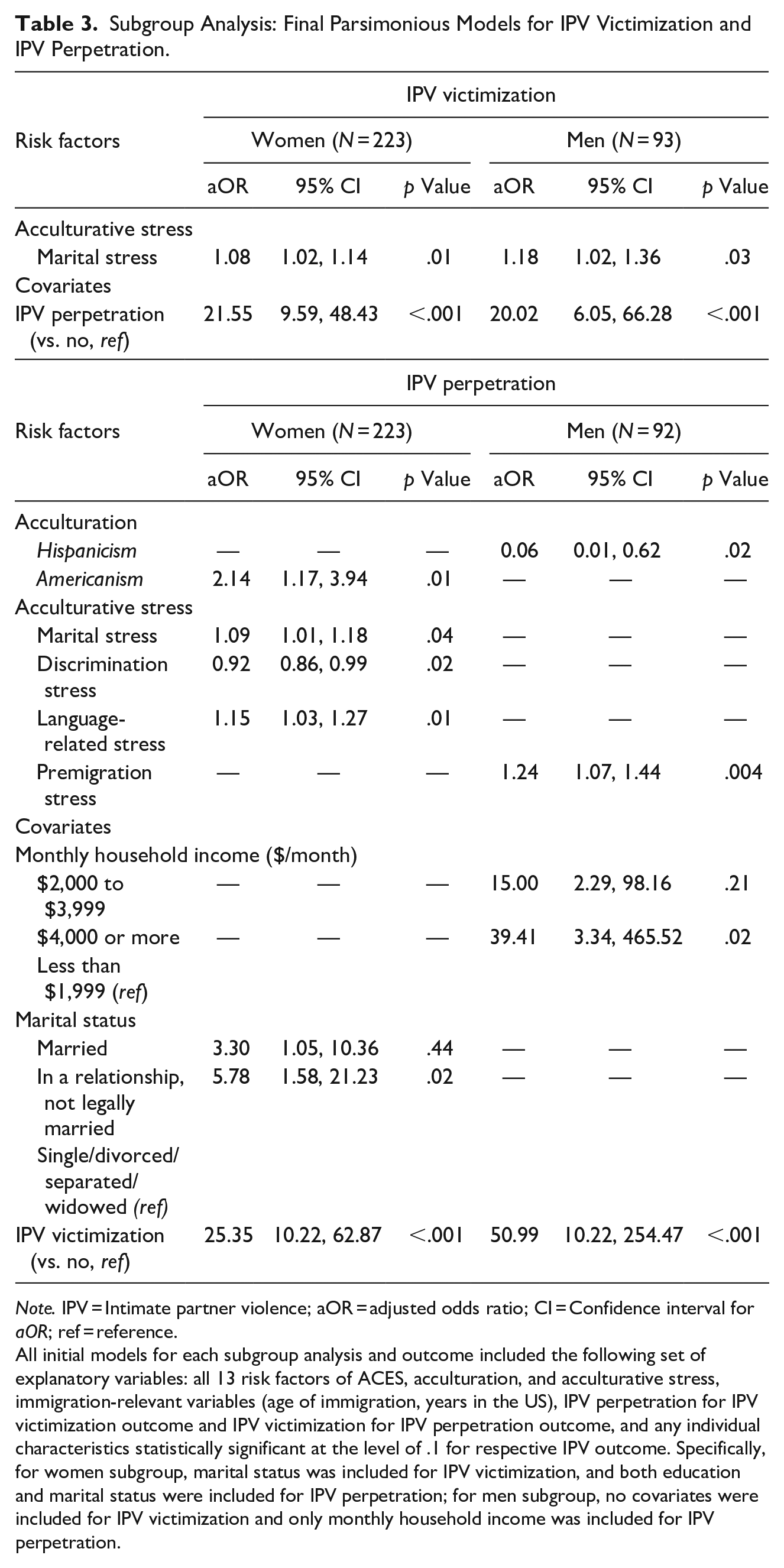
Note. IPV = Intimate partner violence; aOR = adjusted odds ratio; CI = Confidence interval for aOR; ref = reference.
All initial models for each subgroup analysis and outcome included the following set of explanatory variables: all 13 risk factors of ACES, acculturation, and acculturative stress, immigration-relevant variables (age of immigration, years in the US), IPV perpetration for IPV victimization outcome and IPV victimization for IPV perpetration outcome, and any individual characteristics statistically significant at the level of .1 for respective IPV outcome. Specifically, for women subgroup, marital status was included for IPV victimization, and both education and marital status were included for IPV perpetration; for men subgroup, no covariates were included for IPV victimization and only monthly household income was included for IPV perpetration.
Discussion
Guided by the contextual framework for IPV (Bell & Naugle, 2008) and a life-course perspective (Elder, 1998) viewed through a gendered lens, this study contributes to knowledge of health disparities faced by Latinx immigrants by articulating how unique cultural (i.e., acculturation and acculturative stress) and socio-environmental risks (i.e., ACEs) influence IPV victimization and perpetration. To the best of our knowledge, this study is among the first to undertake a comprehensive examination of acculturative stress, identifying specific types with meaningful contribution to IPV. The findings can inform culturally tailored IPV prevention strategies to promote health in this historically marginalized population.
This study sheds light on the distinct roles of acculturation and acculturative stress in relation to IPV, indicated by victimization. Acculturative stress rather than acculturation was predictive of IPV victimization in our study. This finding supports stress theory, which proposes that the stress associated with acculturation, rather than acculturation itself, influences risk for IPV for Latinx individuals (Alvarez et al., 2020), and explains the inconsistency underlying the relationships between acculturation and IPV in prior literature. The current study also extends our knowledge of specific types of acculturative stress most influential to IPV. Family stress emerged as a critical risk factor associated with IPV victimization and offers a potential target for future prevention efforts; however, it is important to recognize the complexity underlying the intersection of family stress resulting from acculturation and from IPV to ensure that prevention strategies are effective. One stress-reduction program that focused on work and family stress among Latinx young adults was successful except for those with exposure to IPV (Torregosa et al., 2021). Family stress captures stress related to disagreement among family members, isolation/loneliness, and inability to center family needs. This can reflect Latinx immigrants’ inability to practice the cultural value of familism (i.e., emphasizing family needs over members’ individual interests) and thus are unable to benefit from its protective effects against adverse health outcomes (Gallo et al., 2009) and sequentially risk for IPV victimization. Policies need to be in place to secure funding to develop, test, and implement culturally tailored resources for Latinx immigrants as well as to grant them access to these resources to further prevent IPV.
Surprisingly, neither acculturation nor acculturative stress was found to be associated with IPV perpetration in our study, inconsistent with existing evidence (Caetano et al., 2007; Gonzalez-Guarda et al., 2013; Mancera et al., 2017). However, the contribution of acculturation and acculturative stress toward IPV perpetration in Latinx immigrants diverged depending on gender. The significance of gender is evidenced by gender subgroup analysis results, supporting some prior literature on gender differences (Frías & Angel, 2012; Sabina et al., 2015). When women and men were examined together, the impact of acculturation and acculturative stress was masked or diluted and thus resulted in null relationships. Further examination of the role of gender is needed to appropriately inform prevention strategies among Latinx immigrants.
This study provides unique insights into the contribution of life-course adversity to IPV among Latinx immigrants; by including community and collective adversity, it expands prior knowledge beyond immigration-relevant adversity and captures the impact of crucial socio-environmental context. ACEs was a stable predictor for IPV perpetration in our study, validating the well-established ACEs–IPV link across populations (Capaldi et al., 2012; Cummings et al., 2013; Smith-Marek et al., 2015). Interestingly, when considered together with acculturation and its associated stress, ACEs did not seem to link to IPV victimization, contrary to prior evidence, possibly due to the cumulative approach used in current ACEs scoring. Consistent with the scoring method in the seminal CDC-Kaiser ACEs study (Felitti et al., 1998), the cumulative approach assumes the occurrence of ACEs, regardless of specific type and level of exposure; total counts of ACEs are summed, and all carry the same weight in predicting IPV victimization. This assumption, however, is challenged by emerging evidence; in a study using a prospective longitudinal design, community violence remained the only ACE significant in predicting IPV victimization in a U.S. sample (Thulin et al., 2021), and a meta-analysis on the ACEs–IPV link suggested further examination of the strengths of relationships between two common categories of ACEs (witnessing IPV and experiencing child abuse) to IPV (Smith-Marek et al., 2015). The field can benefit from future research that goes beyond the cumulative approach of ACEs; for example, a person-centered approach using latent class models or group-based trajectory models to capture the heterogeneity of ACEs patterns and their impact on specific IPV outcomes among the diverse Latinx immigrant population and pinpoint tailored prevention based on these patterns. The conceptualization of our ACEs measure presents another possibility. Despite including community- and collective-level adversity, crucial aspects of ACEs were not fully appreciated. The current conceptualization of ACEs might have missed other adversities unique to Latinx immigrants; for example, adverse experiences related to anti-immigration sentiment and immigration policies (Barajas-Gonzalez et al., 2021). Future research on the impact of ACEs to health should be reflective and inclusive of adversities relevant to Latinx immigrants, include the ACEs–IPV link, and specify the types of ACEs meaningful to IPV.
Our finding that Latinx immigrant women were more likely to be perpetrators compared to men is inconsistent with both sides of the ongoing debate in IPV research on whether rates, types, and motives of IPV perpetration among men and women are similar (i.e., gender symmetry; IPV is bidirectional) or different (i.e., gender asymmetry; IPV is not bidirectional, and IPV perpetrated by women is a self-defensive response to violence perpetrated by their male partners) (Hamby, 2017). One potential explanation for this is that we retained only one item to measure sexual violence in our revised measure (i.e., “You forced him/her to have sex”), which likely led to an underestimation of IPV perpetration among men in a systematic manner (Hamby, 2017). We also used a dichotomous outcome for IPV perpetration without accounting for the severity of the violent behaviors included in the CTS2S. The severity of IPV perpetrated by women versus men is likely to differ fundamentally; for example, women have reportedly been subject to severe or lethal types of IPV yet directed less severe violence toward their partners in self-defense (Dobash et al., 1992). Discordant reporting of IPV among intimate partners may also be a factor. It is well-recognized in the research community that low-to-moderate agreement is typically observed between partners in IPV reporting across studies (Chan, 2011); although the direction of its impact requires further clarification, gender remains a key factor underlying this discordance. A study using a probability sample of U.S. couples, including Latinx couples, indicated that men tended to underreport IPV perpetration, whereas women were more likely to report their perpetration of IPV (Caetano et al., 2002). Moreover, Latinx couples were more likely to disagree on male-to-female violence compared to non-Hispanic White couples (Caetano et al., 2002). The trusting relationships enabled by our community-engaged approach may have created a safe and comfortable environment that further encouraged disclosure of IPV perpetration, particularly for Latinx women. Lastly, selection bias might have played a role. Latinx men were less likely to participate in research studies (Sullivan et al., 2007); those willing to engage tended to be healthier compared to those who did not, leading us to a healthier Latinx men subsample characterized by less IPV perpetration. Future studies should use couple-level data and mixed methods design to allow a contextual picture and nuanced understanding of how gender affects IPV among Latinx immigrants. Results should be interpreted cautiously to avoid any unintended consequences of falsely concluding that women were more violent than men.
The findings of the gender subgroup analysis suggest a gendered risk profile for IPV, particularly for IPV perpetration. This is generally aligned with prior evidence on associations between acculturation/acculturative stress and IPV (Alvarez et al., 2020; Caetano et al., 2007; Gonzalez-Guarda et al., 2013; Mancera et al., 2017). The protective effects of Hispanicism against IPV perpetration for men are noteworthy, which might reflect their retaining of the positive attributes of Machismo (e.g., respect/responsibility for partner and family; Cummings et al., 2013; Mancera et al., 2017). However, great caution must be exercised due to the exploratory nature of the subgroup analysis. The analysis may have missed risk factors and covariates besides those identified due to small sample sizes, especially for men, and insufficient statistical power to detect important small-to-medium effects. Future studies with sufficient statistical power are needed to validate the suggested gendered risk profiles for IPV.
Several limitations should be noted. First, none of relationships discussed in the current study were causal in nature due to its cross-sectional design. The self-reported measure by one partner on IPV might be a threat to validity, as underreporting of IPV perpetration seems more likely for men compared to women; therefore, future couple-level studies are needed. In addition, our study is retrospective and thus subject to recall bias. Although our sample generally reflected the heritage among Latinx immigrants in the US, we acknowledge that a majority of our sample are women, heterosexual, documented, and recruited from a single region in U.S. South, limiting the generalizability of the study findings. Despite the use of culturally and linguistically adapted measures (Nagy et al., 2021), the dichotomous nature of ACEs and IPV scoring did not account for the severity of each exposure and assumed the same weights of all incidents, which can limit our ability to distinguish among exposures that were most meaningful for Latinx immigrants. Another limitation concerns potential overlap in information (e.g., divorced parents and family members with health challenges were captured by both ACEs and pre-migration stress), although statistically, collinearity was not a concern between these variables.
Conclusion
Despite limitations, our study significantly enhances knowledge from a life-course perspective of unique factors contributing to IPV among Latinx immigrants. It (a) links acculturative stress (vs. acculturation) to elevated risk for IPV victimization, and ACEs to increased risk for IPV perpetration among Latinx immigrants; and (b) extends current evidence by specifying the type of acculturative stress most predictive of IPV (family stress for IPV victimization). Gendered differences in the risk profiles (i.e., acculturation and acculturative stress) for IPV perpetration are also suggested, although further research is warranted. Culturally tailored preventions focused on acculturative stress and ACEs hold promise for minimizing exposure to life-course adversities and improving positive adaptation to the US, further eliminating health disparities relevant to IPV in this historically marginalized population.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605221109905 – Supplemental material for Acculturation, Acculturative Stress, Adverse Childhood Experiences, and Intimate Partner Violence Among Latinx Immigrants in the US
Supplemental material, sj-docx-1-jiv-10.1177_08862605221109905 for Acculturation, Acculturative Stress, Adverse Childhood Experiences, and Intimate Partner Violence Among Latinx Immigrants in the US by Jiepin Cao, Susan G. Silva, Miriam Quizhpilema Rodriguez, Qing Li, Allison M. Stafford, Richard C. Cervantes and Rosa M. Gonzalez-Guarda in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We would like to acknowledge Janice Humphreys, PhD, RN, FAAN, and Yan Guo, PhD, for their thoughtful feedback on earlier drafts of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Number R01MD012249: SER Hispano: Salud/Health, Estres/Stress, y/and Resiliencia/Resilience among Young Adult Hispanic Immigrants (PI: R. Gonzalez-Guarda). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Qing Li received partial financial support from University of Colorado Anschutz Medical Campus School of Medicine 2021 and 2022 Slay Community Scholars.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.