
Abstract
Dealing with the outbreak of the new coronavirus has generated unprecedented challenges around the world, including in Israel. Women of childbearing age may be forced to live under particularly difficult circumstances during the pandemic. The current study among Israeli women of childbearing age has three main objectives related to the specific period of the COVID-19 pandemic: to study the prevalence and predictors of intimate partner violence (IPV); to investigate the prevalence and predictors of depression; to examine whether IPV mediates the association between general stress, fear of COVID-19 and depression as an outcome. In a cross-sectional study, 722 married women, Jewish and Arab residents of Israel, were recruited to answer an online self-completion questionnaire during the first wave of the COVID-19 pandemic. The questionnaire included an assessment of their degree of general stress and depression, fear of COVID-19, experiences of IPV and demographic variables. The results of the current study show that a high percentage of women reported IPV (with Muslim women reporting higher IPV than Jewish women), perceived stress (PSS), perceived COVID-19 stress and depression. The findings also show that IPV and its three dimensions mediate the relationship between COVID-19 stress and depression, such that higher stress was related to higher IPV, raising the odds for depression. Moreover, the total scores for IPV and emotional violence were found to mediate the relationship between stress and depression. That is, domestic violence explains part of the association between stress and depression during the COVID-19 pandemic. Indeed, the current pandemic has resulted in an increase in IPV and depression, and especially in the specific stress associated with the disease itself. Based on the findings of the current study, preventing violence will reduce stress-related depression. The Muslim population, and especially those who are more religious, is in particular need of intervention.
Keywords
Introduction
The outbreak of COVID-19 poses a physical and mental threat to public health and a challenge to health systems across the globe (WHO, 2020; Fiorillo & Gorwood, 2020). The uncertainty surrounding this disease, the inability to predict its consequences, evidence pointing to severe disease complications (Zandifar & Badrfam, 2020), high morbidity and mortality rates, and concerns about the future (Banerjee, 2020) all contribute significantly to stress and anxiety levels (Zandifar & Badrfam, 2020). Feelings of uncertainty have direct implications for the population’s daily life and mental health (Wang et al., 2020). Symptoms such as anxiety, depression, fear, stress, and sleep problems have been reported more frequently during the COVID-19pandemic (Torales et al., 2020). Depression is one of the most common mental health problems emerging in the context of natural disasters (Beaudoin, 2007; North & Pefefferbaum, 2013). The prevalence of depression symptoms was more than three times higher during the COVID-19 pandemic than before (Ettman et al., 2020; Thomas et al., 2021). Research shows that during outbreaks of infectious diseases people are liable to experience symptoms of psychosis, anxiety, trauma, suicidal thoughts, and panic (John et al., 2020; Tucci et al., 2017). Moreover, widespread social isolation, lockdown periods, and strict and long-term curfews imposed in some countries in an attempt to contain the global epidemic may also lead to a high level of mental distress (Rossi et al., 2020; Svoboda et al., 2004; Xiong et al., 2020). The COVID-19 pandemic conforms to key baseline conclusions emerging from disaster anthropology over past decades (Kelman, 2020; Ughulu & Igabor, 2021). The first is that natural disasters rarely exist because disasters are social and arise from a combination of hazard and vulnerability, with vulnerability as the causative factor. The second is that a disaster occurs at multiple levels simultaneously, with responses to a hazard exposing as many problems of vulnerability as the original hazard (Kelman, 2020). The COVID-19 pandemic has been described as the worst crisis to affect humanity since World War II (Chakraborty & Maity, 2020; Dohle et al., 2020).
Studies have found that when women are exposed to disasters such as hunger, war, and disease outbreaks they are more vulnerable to psychopathological outcomes (Bradshaw, 2015; Bradshaw & Fordham, 2015). Psychological disorders such as fear and stress (Hamama-Raz et al., 2015; Yokoyama et al., 2014), posttraumatic stress disorder (PTSD) (Cofini et al., 2015), and depression (Cénat & Derivois, 2014; Kun et al., 2013) are more prevalent among women.
At the onset of the COVID-19 pandemic, women were more anxious than men (Gao et al., 2020; Moghanibashi-Mansourieh, 2020) and experienced higher levels of stress, anxiety, and depression (Wang et al., 2020).
Previous studies have shown that post-disaster stress increases the prevalence of violence against women (Anastario et al., 2009; Yoshihama et al., 2013). Studies have found that intimate partner violence (IPV)is a significant factor associated with depression (Chandan et al., 2020; Refaeli et al., 2019). IPV is a serious and preventable public health problem that affects millions. Data accumulated about IPV incidences worldwide have led health authorities to address this issue by using known risk factors to raise awareness for prevention strategies (Berg, 2017; Blumling et al., 2018; Spivak et al., 2014; WHO, 2017). Indeed, across the globe almost one third (27%) of women aged 15–49 years old who have been in a relationship have experienced IPV (WHO, 2021).
Intimate partner violence (IPV), one of the most common forms of violence against women, includes physical, sexual, and emotional abuse and controlling behaviors by an intimate partner (WHO, 2021). These behaviors include threats, verbal and physical humiliation, surveillance, harassment, reduced means of support, social isolation, denying control over economic resources, coercive control, throwing objects, intimidation, rape or sexual assault, various physical injuries, and in extreme cases murder (WHO, 2020b).
During pandemics, IPV is linked to a variety of factors, among them economic stress, increased exposure to exploitative relationships, and reduced support options (Peterman et al., 2020). Due to the social isolation measures taken around the world to help reduce the spread of COVID-19, many people, including those in abusive relationships (IPV), were confined to their homes.
Social isolation exacerbates vulnerability to violence while limiting accessible and recognized support options (van Gelder et al., 2020). Yet social distancing and isolation are central to the public health strategy adopted by many countries to slow the spread of the virus (Campbell, 2020; van Gelder et al., 2020).
As in other countries, the government of Israel has issued many instructions and guidelines to deal with the consequences of the new COVID-19 virus and to prevent its spread (Ministry of Health, 2020). Guidelines dictating the closure of schools and workplaces have forced women to stay home with their abusers (in cases where the current spouse is an abuser), causing intense and unprotected contact in the absence of existing support networks, such as the extended family and social or community support networks for at-risk families (Ministry of Health, 2020).
Since social isolation and quarantine measures were introduced across the world, reports of domestic abuse and IPVhave increased. For example, France (Reuters News Agency, 2020), the United States (Wagers, 2020), and the United Kingdom (Bradbury-Jones & Isham, 2020; Kelly & Morgan, 2020) have reported increased rates of IPV. Since the beginning of the COVID-19 crisis (March to October 2020), there were three times more complaints of domestic violence in Israel than during the corresponding period in 2019 (Ministry of Social Affairs, 2020).
Dealing with the outbreak of the new coronavirus has created unprecedented challenges around the world, including in Israel. For example, in the US women of childbearing age may be forced to live under particularly difficult circumstances during the pandemic due to job loss, constrained access to contraception and other sexual and reproductive health services, and exposure to IPV (Guttmacher, 2020). Thus, it is very important to examine the experiences of these women in order to understand how the exceptional circumstances of this period have affected various aspects of their lives.
To the best of our knowledge, very few studies have examined the health implications of COVID-19 on various health aspects of Israeli women of childbearing age. Therefore, the current study conducted among Israeli women of childbearing age has three main objectives related to the specific period of the COVID-19 pandemic: (1) to study the prevalence and predictors of IPV; (2) to investigate the prevalence and predictors of depression; and (3) to test whether IPVis a mediator of the association between general stress, fear of COVID-19 and consequent depression. Identifying the health challenges facing women of childbearing age during the COVID-19 pandemic can help in understanding how to reduce such negative effects and improve women’s quality of life during and after this pandemic and during disasters in general. The State of Israel has a very diverse and multicultural population, especially in the Northern District. People came to Israel from different countries from all over the world and created a human mosaic made up of different ethnicities, different religions, and different cultures. The present study presents the rate of stress, anxiety, and violence among women in a multicultural population.
Material and Methods
In this cross-sectional study, Jewish and Arab women of childbearing age residing in Israel were recruited through Facebook, and participants were asked to forward the link of the questionnaire to other relevant individuals, thereby creating a snowball sample. Participation in the study was voluntary and no inducements were offered.
Participants were asked to answer an online self-completion questionnaire during the first wave of the COVID-19 pandemic. The questionnaire included an assessment of their degree of general stress and depression, as well as specific questions pertaining to participants’ fear of COVID-19, experiences of IPV, and other obstetric and demographic variables. The depression (PHQ-2) and stress (PSS) questionnaires were originally written in English and were translated in two stages: first from English into Hebrew and Arabic, and then back-translated by other translators from Hebrew and Arabic into English. The reliability of each part of the questionnaire was tested separately using the Cronbach’s alpha statistic. The other questionnaires were originally written in Hebrew and Arabic.
Data collection was completed during the period from April 22 to May 2, 2020, corresponding to the lockdown imposed by the Ministry of Health to contain the COVID-19 pandemic (Public Health Order, 2020). The inclusion criteria were Israeli women between the ages of 18 and 45 years old who were married or in a relationship. Data collection was done mainly through internet forums that were intended for women in an intimate relationship. In the Arab society, the meaning of an intimate relationship is engagement, preceding marriage. Thus, in order to make the two ethnic groups as comparable as possible, we turned to married Jewish women only.
Participants
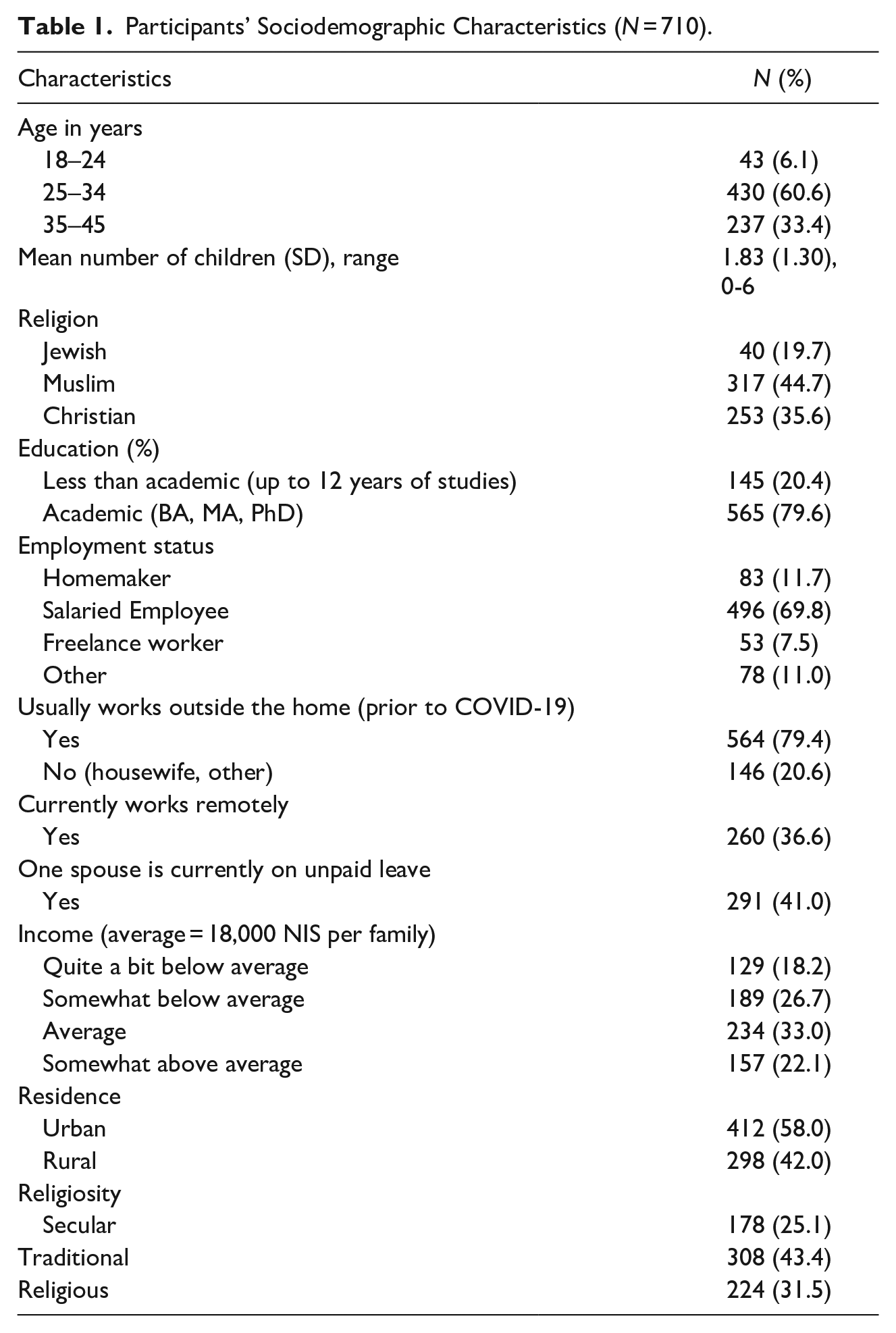
The majority of the 710 participants (Table 1) were between the ages of 25 and 34(61%) and most of the others were between 35 and 45 years (33%). The definition of three age groups was according to known pregnancy risks: younger women (18–24), older women (35–45), and the main group of childbearing women (25–34), follows other studies that used the same age cutoff points (Aolymat, 2021). Participants had up to six children, with a mean of 1.83 children (SD = 1.30). Most of the Arab women participants were Muslim (45%) or Christian (35%). Jewish participants comprised around 20% of the sample. About 80% of the participants had an academic education. Under normal circumstances (prior to COVID-19) about 79% of the participants usually worked outside the home, while at the time of the study about 37% were working remotely from home. In about 41% of the families, at least one spouse was on unpaid leave from work. About 45% of the women reported that their income was below average, about 33% reported an average income, and an additional 22% reported that their income was above average. About 58% of the women lived in urban localities, 25% were secular, 43% were traditional (somewhat religious) and 32% were religious.
Participants’ Sociodemographic Characteristics (N = 710).
Diversity Statement
The population of Israel is multicultural and diverse. This study examined women of childbearing age, such that only one gender was included in the research population. Within this group, the participants reflected differences in socioeconomic status, ethnicity, language, religion, residential region, education, age, and culture.
Research Tools
Stress: The ten-item version of the Perceived Stress Scale (PSS) was used to assess individual stress levels (Cohen & Williamson, 1988). The internal consistency (Cronbach’s α) for the full 10-item scale was 0.86. The scale measures perceptions and feelings related to recent levels of general stress on a scale ranging from 0 = never to 4 = often. The overall score ranges from 0 to 40, with higher scores indicating higher levels of perceived stress. Scores between 0 and 13 were considered to indicate a low stress level, scores between 14 and 26 a moderate stress level, and scores between 27 and 40 a high stress level.
Fear of COVID-19: For the purposes of this study, the researchers designed a questionnaire consisting of five statements examining women's concerns about COVID-19 (Cronbach’s α = .74). The questionnaire included items such as: “I am afraid of getting COVID-19”; “I am afraid someone in my family will get COVID-19”; “I am afraid someone close to me will die from COVID-19”.Participants answered on a 5-point Likert scale ranging from 1 = totally disagree to 5 = strongly agree. The mean of all answers was considered to indicate the level of fear specific to the pandemic, such that the higher the score, the higher the woman’s perceived fear of COVID-19.
Depression: The Patient Health Questionnaire–2 (PHQ-2) developed by Kroenke, Spitzer, Williams (2003) was used to measure depression. This questionnaire consists of the first two items of a larger questionnaire, the PHQ-9. Both items measure depressed mood and loss of interest (anhedonia). A participant must give a positive answer to at least one item to be screened positive for any depressive disorder according to the DSM-IV. PHQ-2 scores can range from 0 to 6, and a cutoff point ≥3 indicates significant depression. The cutoff point was used to define the dependent variable, which was thus dichotomous (0, 1). The correlation between the two items in the current study was r = .72 (p < .001).
IPV Questionnaire: IPVwas assessed using a questionnaire consisting of ten items about violence perpetrated by the participant's spouse (categories: 1 = never, 2 = rarely, 3 = often, 4 = always). The questions were based on the US IPV Prevention Services Task Force (2004) and have been used by the Israeli Ministry of Health and in a study conducted in Israel (Daoud et al., 2017). A woman is defined as a victim of violence if she gives an affirmative answer to at least one of the ten questions (i.e., at least “rarely” for at least one question). The Cronbach’s α for the entire scale was .80. Types of violence were defined as physical or sexual violence—Items 6, 9, 10 (Cronbach’s α = .70); emotional or verbal violence—Items 1, 2, 7, 8 (Cronbach’s α = .53); and social or economic violence—Items 3, 4, 5 (Cronbach’s α = .64).Total scores were computed using item means.
Questionnaire examining women’s demographic variables: Age, level of education, employment, religion (Jewish, Muslim, Druze or Christian), degree of religiousness (secular, traditional, religious), and income. At the time the study was conducted, the average family income in Israel was about NIS 18,000 per month. Participants were asked whether their family income was below average (considerably or slightly), average, or above average (considerably or slightly).
Procedure
Ethical Considerations: This study was conducted in accordance with the Helsinki Declaration and was approved by the Helsinki Committee of Nazareth Hospital, as well as by the Ethics Committee of the academic institution where the researchers work. The questionnaire included a request for each participant to provide informed consent before filling it out. Participants were informed they could withdraw from the study at any time without any consequences.
Statistical methods: Data were analyzed with SPSS version 27 (SPSS, Chicago, IL, USA). Depression was dichotomized, with a cutoff point ≥3 signifying the clinical range for depression. Odds ratios (OR) and 95% confidence intervals (CI) were calculated to assess the relationships between the demographic variables and depression/IPV (yes/no).
Most variables did not deviate from a normal distribution (skewness = −0.52 to 0.07, SE = 0.09), except for the measures of violence (skewness = 1.61 to 4.57, SE = 0.09). These measures therefore underwent log transformation. Pearson correlations were calculated between the study variables. Multiple hierarchical logistic regressions were calculated for depression as the dependent variable. The control variables of income level, Muslim religion, and level of religiosity were entered in the first step; the independent variables of COVID-19 stress and PSS stress were entered in the second step; and the mediating variables of IPV and its dimensions were entered in the third step. The mediating role of IPV in the relationship between PSS stress and depression was assessed using the Process procedure (Hayes, 2018), Model 4, with 5000 bootstrap samples and 95% CI. This procedure was chosen due to the binary scale of the dependent variable. Significance level was set at p < 0.05.
Findings
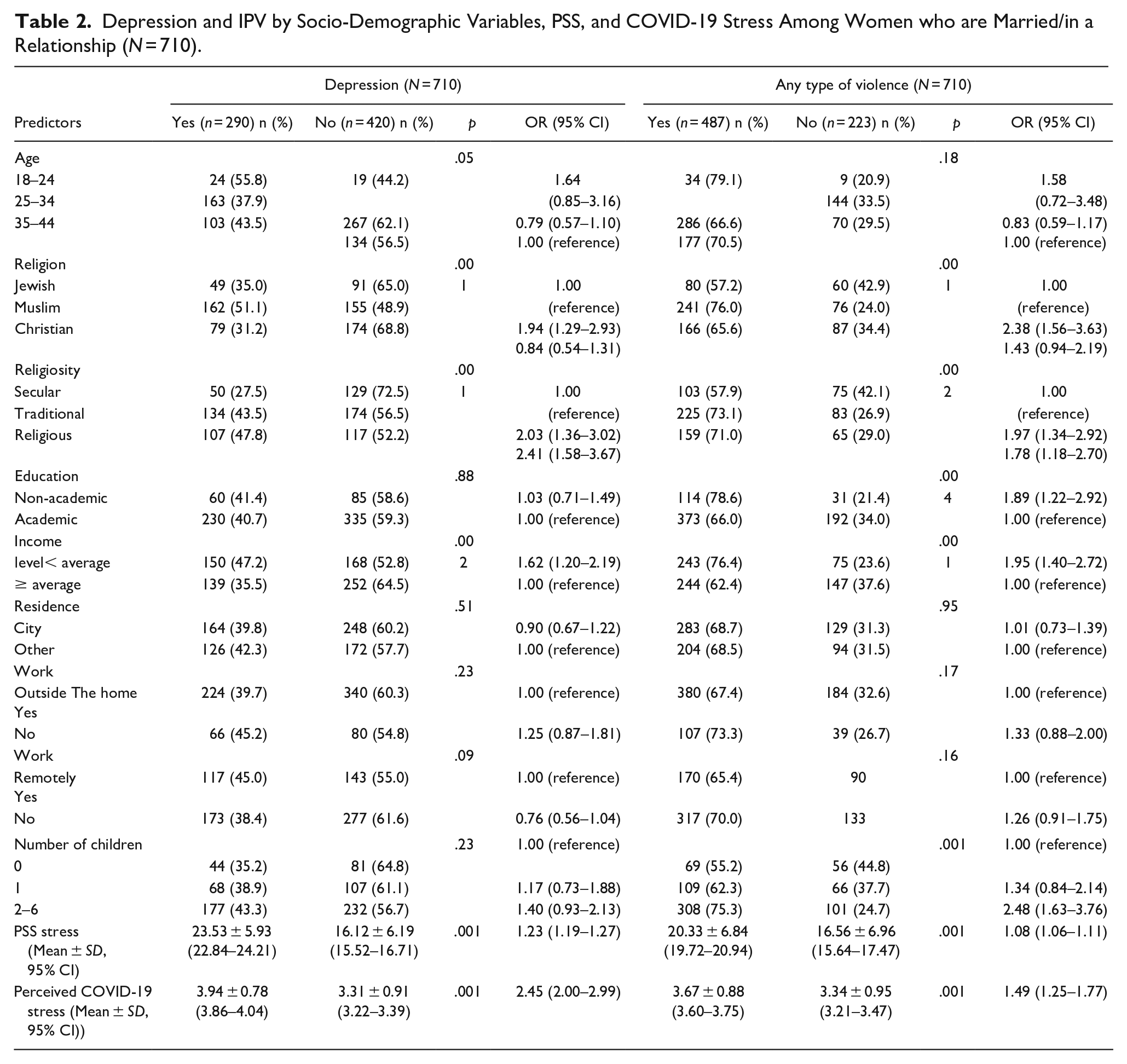
Of the 710 married women participants, 290 (40.8%) were classified within the clinical range for depression and about two-thirds (N = 487, 68.6%) reported IPV. About one-third of the participants (N = 242, 34.1%) exhibited IPV and also fell within the clinical range for depression. Several demographic/socioeconomic variables were found to be related with the dichotomous definitions of depression and IPV (Table 2). Both depression and IPV were significantly higher among Muslim women than among Jewish women and were also higher among women who were traditional/somewhat and veryreligious than among secular women. Further, both depression and IPV were higher among women who reported a below average income than among women who reported an average or above average income. In addition, IPV was higher among women with non-academic education than among those with academic education as well as higher among women raising at least two children than among women raising one or no children. Finally, PSS stress and perceived COVID-19 stress were both found to be related to depression and IPV, such that higher levels of stress increased the odds of being classified within the clinical range for depression and of reporting the existence of IPV.
Depression and IPV by Socio-Demographic Variables, PSS, and COVID-19 Stress Among Women who are Married/in a Relationship (N = 710).
About half the women who reported IPV (the dichotomous definition) were classified in the clinical range for depression (N = 242, 49.7%), compared with about one-fifth of the women who did not report IPV (N = 48, 21.5%), a significant difference (p < .001). Likewise, over half the women who reported physical/sexual violence, emotional/verbal violence, or social/economic violence were classified within the clinical range for depression, compared with about a quarter to a third of the women who did not report IPV, with all differences significant (Table 3).
Relationship between IPV and Depression (N = 710).
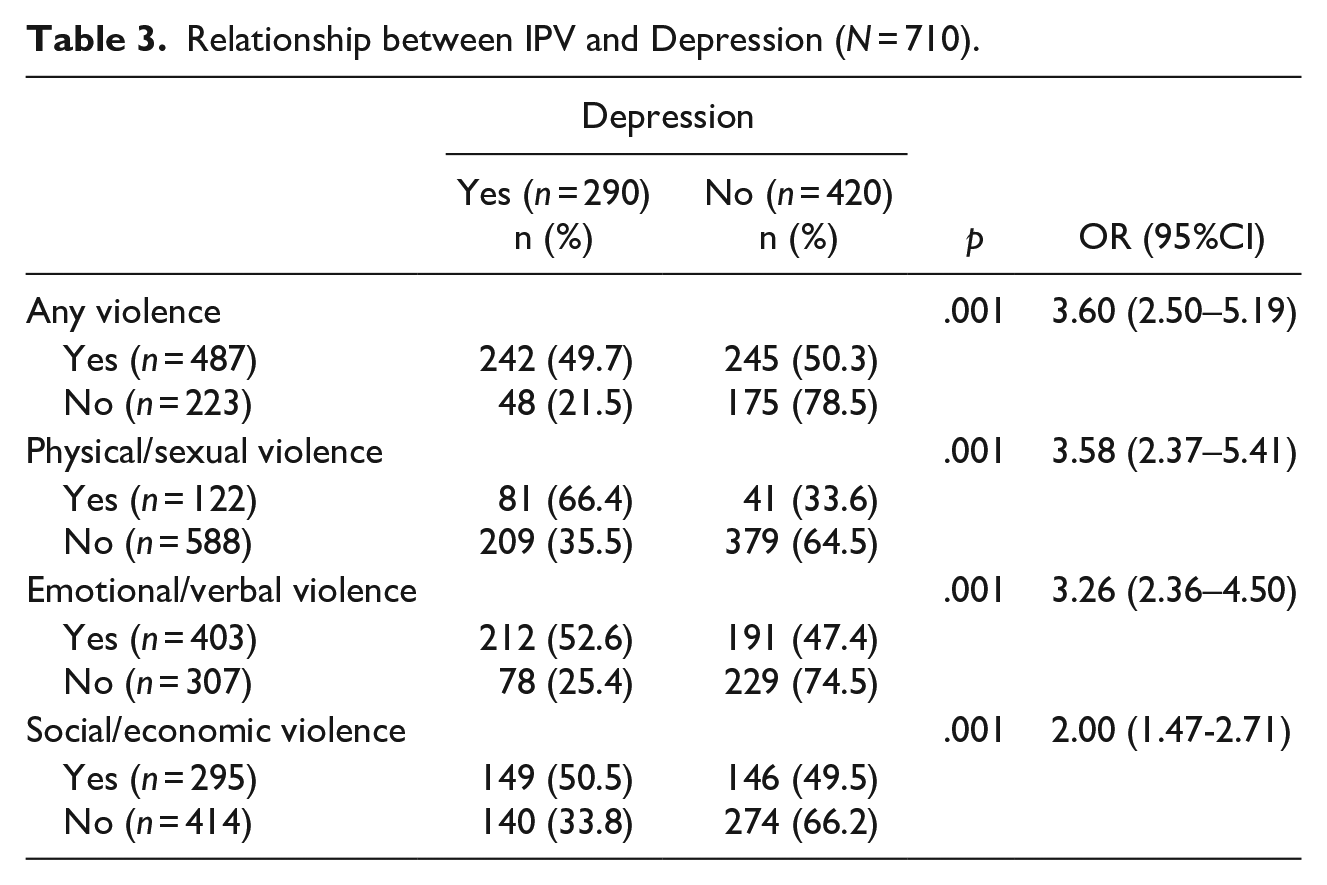
Table 4 shows the distribution of the study variables and the intercorrelations among them. Means in the table reveal that both COVID-19 stress, and PSS stress were moderate. IPV (the continuous score) was low, and about 41% of the women were classified in the clinical range for depression. Positive and significant correlations were found among all variables. That is, the independent variables—COVID-19 stress and PSS stress—exhibited a positive interrelationship and were both positively associated with IPV. All variables were positively associated with depression.
Means, Standard Deviations, and Intercorrelations Among the Study Variables (N = 710).
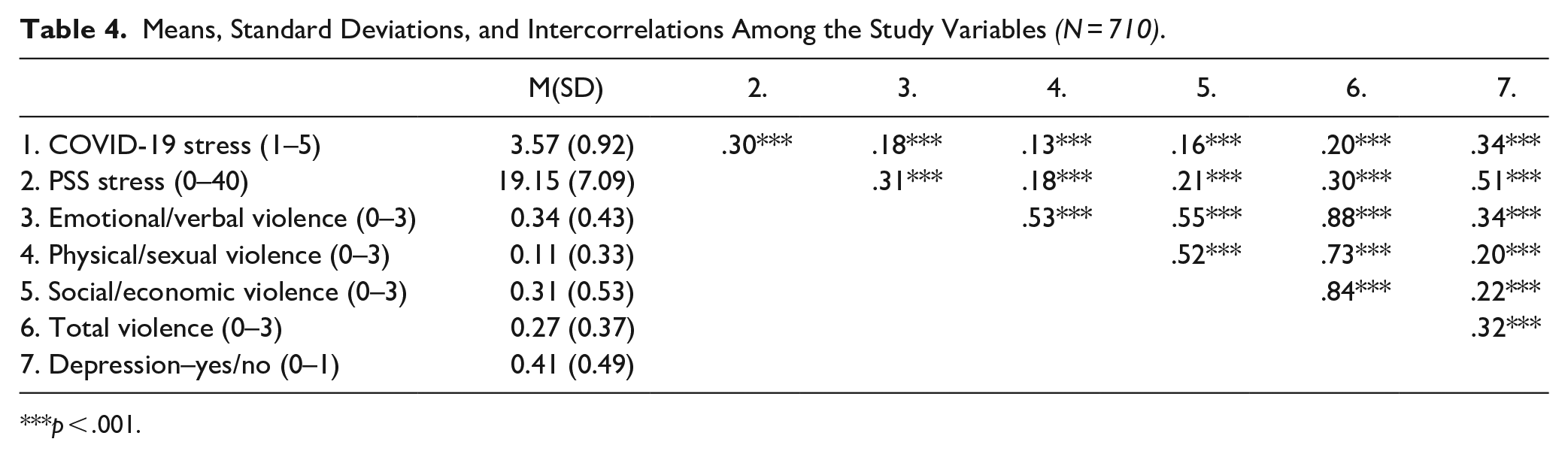
p < .001.
Several of the relationships between the background variables and being classified within the clinical range for depression (yes/no) were found significant (Table 2). Income level was an ordinal variable that did not deviate from the normal distribution (skewness = −0.14, SE = 0.09) and was thus used as a continuous variable that was negatively related to depression (OR = 0.75, 95%CI = 0.64, 0.87; p < .001). Muslim religion (yes/no) was positively related to depression (OR = 2.16, 95%CI = 1.59, 2.93; p < .001). Further, level of religiosity was an ordinal variable that did not deviate from the normal distribution (skewness = −0.11, SE = 0.09) and was thus used as a continuous variable that was positively related to depression (OR = 1.51, 95%CI = 1.23, 1.86; p < .001). The other background variables were not found to be associated with classification within the clinical range for depression. Due to these relationships, the variables of income level, Muslim religion, and level of religiosity were controlled for in further analyses.
A multiple hierarchical logistic regression was calculated, with depression as the dependent variable (yes/no), as shown in Table 5. The control variables of income level, Muslim religion, and level of religiosity were entered in the first step; the independent variables of COVID-19 stress, and PSS stress were entered in the second step; and the mediating variable of IPV (the continuous score) was entered in the third step. The results show that all three demographic variables were significant in the first step, but after the independent variables were entered, only Muslim religion retained its significance in further steps. COVID-19 stress and PSS stress were significant predictors of depression, such that higher levels of both these variables increase the odds for depression. Moreover, the total IPV score made a significant positive contribution to depression, thus increasing the odds for depression.
Multiple Hierarchical Logistic Regression for Depression (N = 710).
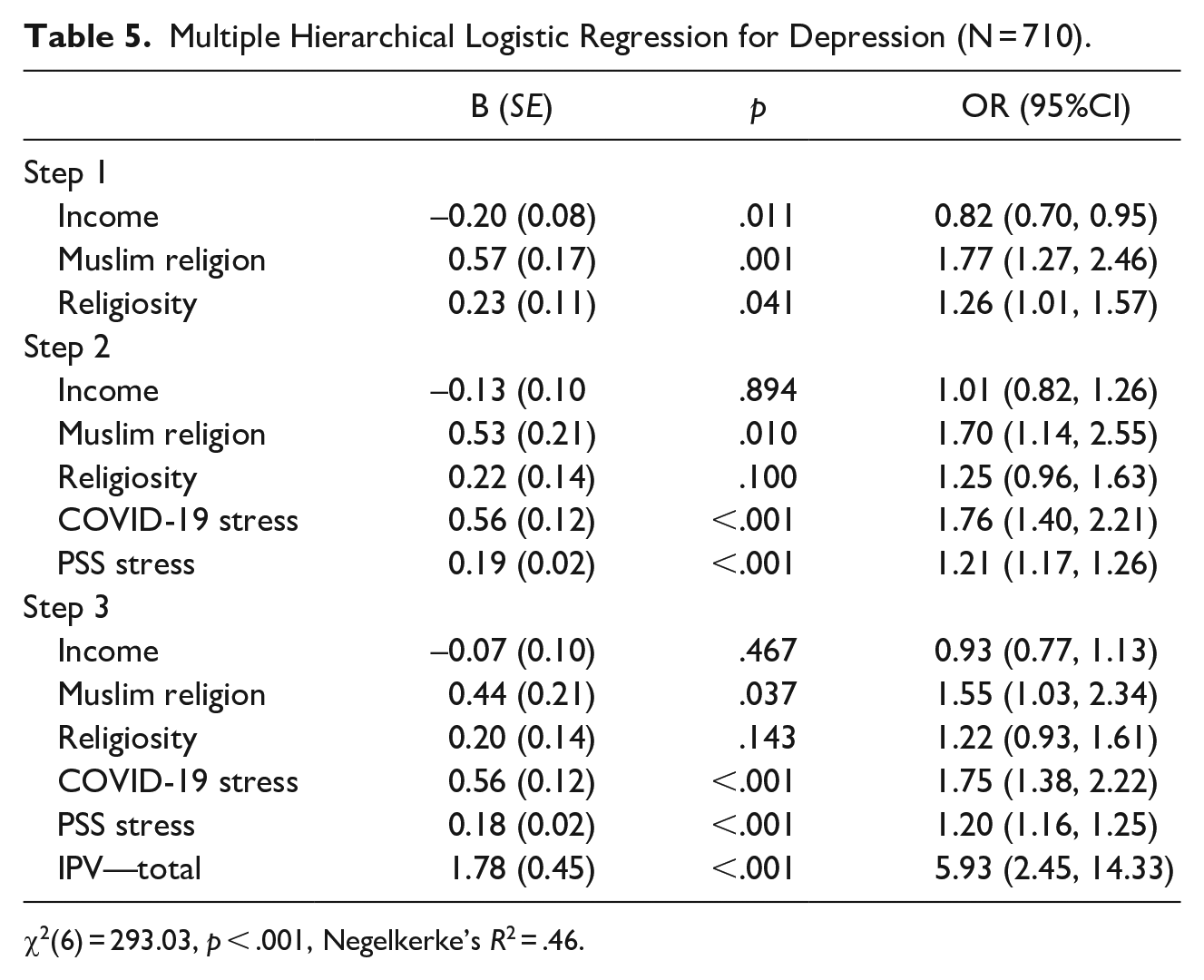
χ2(6) = 293.03, p < .001, Negelkerke’s R2 = .46.
In addition to the logistic regression analysis with the total IPV score, we tested another model with the three dimensions of emotional violence, physical violence, and social violence. Yet due to the marginally high IPV values (up to 1.71) and the rather high correlations between the three dimensions of IPV (r = .52 to r = .55, p < .001), each dimension was examined in a separate regression model.
Emotional/verbal violence was positively associated with depression (B = 1.70, SE = 0.36, p < .001, OR = 5.50, 95%CI = 2.69, 11.25), such that a higher level of emotional violence increases the odds for depression. Likewise, physical/sexual violence was positively related to depression (B = 1.06, SE = 0.48, p = .029, OR = 2.88, 95%CI = 1.11, 7.45), as was social/economic violence (B = 0.66, SE = 0.32, p = .038, OR = 1.93, 95%CI = 1.04, 3.59), such that higher levels of both physical and social violence increase the odds for depression.
Finally, an attempt was made to assess the mediating role of IPV in the relationship between stress and depression. The Process procedure (Hayes, 2018), Model 4, was used for that purpose, with 5,000 bootstrap samples and 95% confidence interval, as shown in Table 6.
Path Coefficients and Indirect Effects for IPV as a Mediator Between Stress (COVID-19 and PSS) and Depression (N = 710).
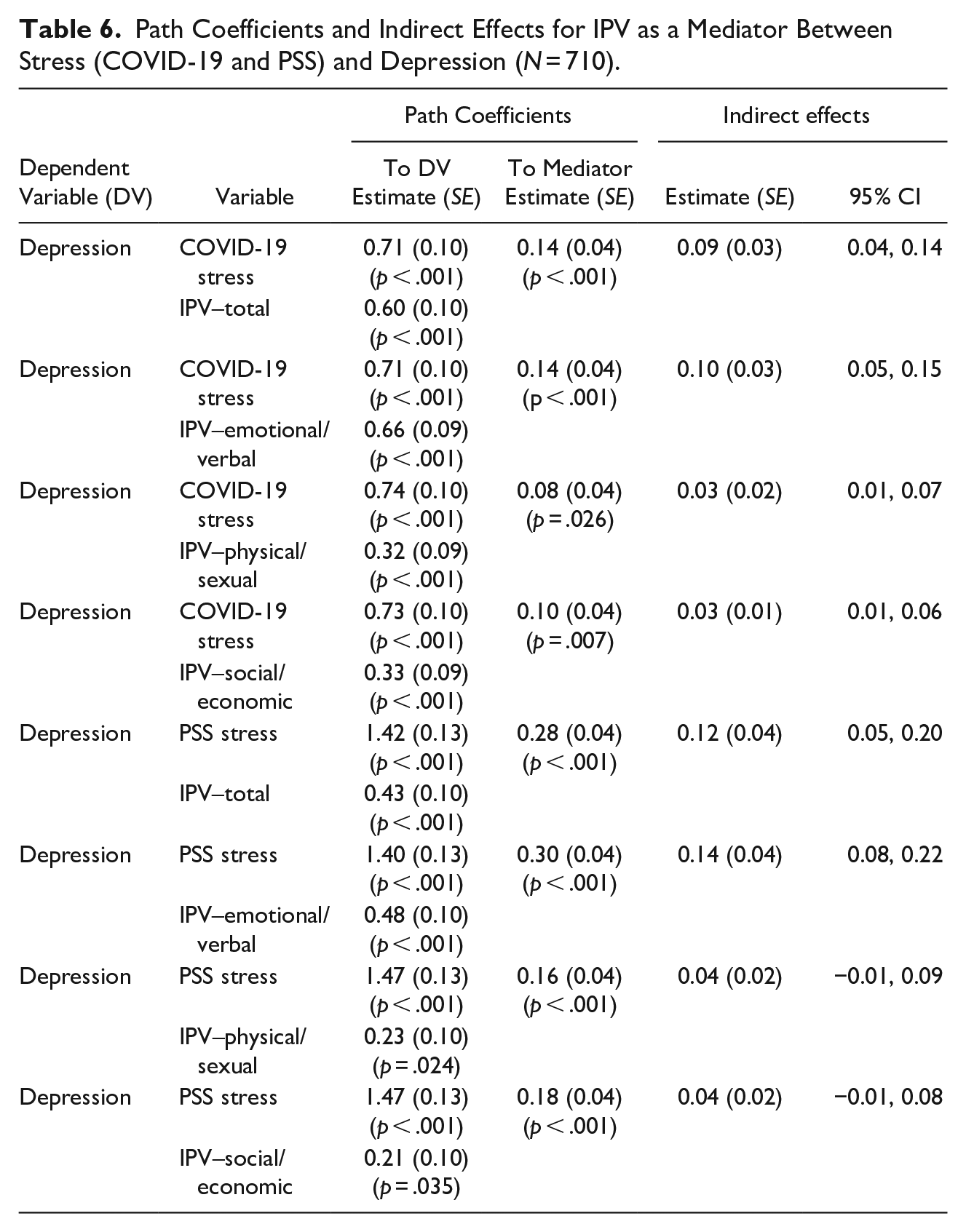
The results reveal significant relationships. IPV and its three dimensions (the continuous score) were found to mediate the relationship between COVID-19 stress and depression, such that higher stress was associated with higher IPV, increasing the odds for depression. Further, the total scores for IPV and emotional violence were found to mediate the relationship between PSS stress and depression, such that higher stress was associated with higher total and emotional IPV, increasing the odds for depression. In this case, physical and social violence did not serve as significant mediators.
Discussion
The results of the current study show that a high percentage of the participants reported IPV, PSS stress, perceived COVID-19 stress, and depression. The current study also found that IPV and its three dimensions mediate the relationship between COVID-19 stress and depression, such that higher stress is associated with higher IPV, raising the odds for depression. Moreover, the total scores for IPV and for emotional violence were found to mediate the relationship between stress and depression. That is, IPV explains part of the association between stress and depression during the COVID-19 pandemic. The findings of the present study are in line with many studies, as noted in the introduction section.
The longer people stay at home and the more time families spend in close contact, particularly in crowded conditions, the more stress there is inside the home and the greater the likelihood of IPV (Buller et al., 2018). In fact, for women facing IPV, the home is not safe and may even be the place where the physical and mental abuse occurs. Violence may escalate during humanitarian crises because women remain isolated at home with their abuser and without proper support. Studies from around the world (Boserup et al., 2020; Campbell, 2020) have reported an increase in IPV during the COVID-19 era. Indeed, a significant increase in IPV has been reported in the past following various natural disasters such as tsunamis, hurricanes, fires, earthquakes, and other devastating events (Parkinson, 2019; Parkinson & Zara, 2013; Weitzman & Behrman, 2016).
In the current study, Muslim women reported a higher degree of marital violence compared to Jewish women. This finding corresponds with previous studies conducted in Israel that found more severe IPV among Arab women than among Jewish women (Daoud et al., 2017; Eisikovits et al., 2004). Shoham (2013) also documented that IPV against women pervades all cultures in Israel and is prevalent mainly among immigrants and minorities. In traditional cultures, norms and social attitudes that emphasize the sanctity of family life may also make it more difficult for women to report or complain about violence.
In the current study, low income was also found to be a variable related to IPV. Economic pressures arising during the COVID-19 pandemic generated by business slowdowns, declining incomes and high unemployment rates may have been related with a sense of stress and uncertainty, thus being related with IPV as well. Previous studies have found that low income is associated with the cycle of IPV (Daoud et al., 2020; Campbell, 2020; Eisikovits et al., 2004). Having many children was also found to be a variable associated with IPV. For many women, quarantine and social isolation increase the burden of household chores and caring for children at home, especially because the children do not regularly attend kindergartens and school. Moreover, a large number of children increases overcrowding in families with low socioeconomic status, which may lead to increased stress and subsequently to IPV (Peek-Asa et al., 2017).
In the current study, the COVID-19 pandemic was marked by high levels of stress, a sense of being threatened by the virus, and depression. We also found that the perceived threat of the disease was high among the study population. Our findings are similar to those of other studies suggesting that women are vulnerable to heightened psychological distress such as depression and stress (Mazza et al., 2020; Qiu et al., 2020; Wang et al., 2020). Symptoms such as depression, fear, and stress were seen more frequently during the COVID-19 pandemic (Özdin & BayrakÖzdin, 2020; Torales et al., 2020), with various studies finding that more than a quarter of their participants experienced moderate to severe levels of stress and depression (Wang et al., 2020). The duration of lockdown periods during pandemics increases the risk of serious psychological consequences (Brooks et al., 2020). In addition, people are more concerned about their health and family (Li et al., 2020).
The psychological consequences of dealing with the COVID-19 pandemic are quite complex. Mental illness and negative emotions were found to increase during this period, while positive emotions such as feelings of happiness and life satisfaction decreased (Li et al., 2020). In addition, the lack of information about the disease and its treatment, uncertainty about its ultimate consequences, exposure to various and contradictory sources of information about the disease and its health and economic consequences, and social distancing measures designed to treat the outbreak while diminishing social ties may all have health and social consequences.
In our study, Arab women reported higher levels of mental health problems. Various studies conducted among traditional minority groups have suggested that one of the factors associated with depression is a patriarchal culture that considers men to be superior and women to be inferior (Bargai et al., 2007; Pineles et al., 2008).
The findings of the current study revealed a positive relationship between IPV and depression. Stress and perceived threat of the disease were found to be predictors of depression. Moreover, mental IPV was found to mediate between stress and depression. Violence is a serious risk factor for women’s health during emergencies and tends to increase during pandemics (WHO, 2020b). The current pandemic—in particular the specific stress associated with the disease itself—was related with IPV and depression. The findings of the current study showing that mental violence mediates stress and depression indicate that preventing violence may help reduce stress-related depression. After logistic regression, the association between Muslim religion and depression remained. Therefore, intervention is especially important for the Muslim population and especially for the more religious among them.
This study has several limitations due to the sampling technique. Relying on Facebook for voluntary recruitment and sharing may have introduced a bias of choice, such that the sample does not include people who are not active on Facebook, do not have internet access, and do not use smartphones or email. Self-report may have also led to bias, especially since the study was conducted at the very beginning of the pandemic when fear and uncertainty may have been at the highest. Another limitation is the current study’s cross-sectional design, which does not allow for causal inference between research variables. Our findings suggest high prevalence of IPV during the pandemic, however we cannot conclusively say that the prevalence was solely due to the pandemic and not other stressors that were not controlled for in the study.
Conclusions
Dealing with the outbreak of the new coronavirus disease (COVID-19) has generated unprecedented challenges around the world, including in Israel. While lockdowns are designed to protect people from the disease, for some women the lockdowns resulted in changes in their living circumstances that were associated with negative social and psychological consequences during this period.
IPV is a national epidemic that became very clear during the COVID-19 crisis. The sharp rise in the number of women referred for protection against IPV (WHO, 2020b) indicates the magnitude of the challenge facing health systems.
The present study examined mental aspects such as depression, stress, and perceived threat of the disease, as well as the prevalence of IPV and the relationship between these variables among a diverse population of women of childbearing age in the State of Israel, including a comparison of minority groups (Muslims and Christians Arabs). These findings may be of great importance in devising intervention programs to reduce IPV and to encourage a mental health intervention strategy as a follow-up to COVID-19.
Recommendations
IPV is on the rise (WHO, 2020b). Only by handling this problem properly can the authorities deal with the many psychological consequences among women in our society. Governments must address the escalating issue of violence against women during the COVID-19 pandemic. The needs of women facing complex challenges during this period should be addressed. In this regard, programs should be designed that will empower women to reveal their problems, and financial and professional resources should be allocated to treat groups at-risk for violence and mental health problems, with special emphasis on minority groups who are more vulnerable to the consequences of these problems. In conclusion, these results provide important information for identifying factors related to the mental health of women of childbearing age, the prevalence of IPV, and the relationship between these factors. The findings may also be useful in tailoring mental health interventions aimed at treating the posttraumatic nature of distress and at training health professionals.
Footnotes
Acknowledgements
we would like to thank Doctor Jawad KarramMD- Nazareth Hospital, for his help in requiting participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Max Stern Yezreel Valley College Ethical Committee, number YVC EMEK2020-91.