
Abstract
Childhood exposure to violence is a major public health issue. Effective treatment can reduce the impact of violence exposure on child outcomes. However, disparities in treatment engagement can interfere with effective treatment. This study reviews data collected from 2,546 children referred to community-based mental health services from 2001 to 2015 after exposure to violence. Children were categorized into three groups: those who attended intake but never started treatment, referred to as the Nonengager group; those who started but discontinued treatment prior to meeting treatment goals, referred to as the Attriter group; and those who completed treatment as rated by the treating therapist, referred to as the Completer group. The three groups were analyzed for differences in behavioral and emotional problems, racial identity, child social support, household income, number of people living in the home, parent stress, parent social support, community violence exposure, and neighborhood-level child opportunity. Analyses demonstrated that the Completer group were more likely to: live in neighborhoods with higher levels of childhood opportunity, identify as White, have an annual household income of $40,000 or greater, have significantly fewer people living in the home, report lower levels of parental stress, report higher levels of parental social support, report higher levels of child social support, and have significantly lower scores of emotional and behavioral problems after treatment. Overall, our study supports the importance of considering multiple ecological levels when targeting treatment engagement for children after exposure to violence. Results indicate that children from more advantaged environments are more likely to complete treatment, which leads to better outcomes. This can exacerbate existing disparities. Findings highlight the need for systems change and advocacy for children in less advantaged environments and meeting families in their specific context, to combat treatment disparities.
Keywords
Introduction
Children are exposed to violence at alarmingly high rates throughout the United States. Exposure to violence can occur within the home or community. Exposure to violence includes any type of aggression that is directed toward the child or aggression between others that the child witnesses. Throughout this paper, exposure to violence refers to domestic violence, sexual victimization, physical assault, community violence, child abuse (including child physical, sexual, or emotional abuse), or neglect. In a nationally representative sample of children from birth to age 17, 61% of children reported direct exposure to violence in the past year (Finkelhor et al., 2015). Children exposed to violence (CEV) can exhibit deficits across a variety of domains including: (1) behavioral and emotional responses, (2) relationships and attachment, (3) learning and school performance, (4) peer relationships, and (5) civic engagement (Delaney-Black et al., 2002; Fowler et al., 2009; Jackson et al., 2019; Lynch, 2003; Perkins & Graham-Bermann, 2012). Nonetheless, providing children with early access to mental health treatment after violence exposure can minimize deleterious effects on child functioning (Berkowitz, 2003; Schewe et al., 2013; Wethington et al., 2008). While effective treatment is critical to mitigate the effects of violence exposure on socioemotional and behavioral development, up to 80% of youth who require mental health treatment do not receive it (Kataoka et al., 2002). Many factors can influence whether a family engages in or completes treatment following a child’s exposure to violence. While previous research studies have considered individual child and family factors that may impact treatment engagement, researchers have acknowledged the need to consider system-level factors as well (Morris et al., 2019; Shaw et al., 2016). To best support the well-being and development of children after exposure to violence, it is critical that we develop a more robust understanding of the relationship between both individual and system-level factors that impact treatment engagement and effectiveness.
The Exosystem—The Neighborhood Environment
Bronfenbrenner’s (1977) Ecological Systems Theory provides a guiding framework through which we can consider the many levels of factors that influence a child’s development. This theory demonstrates how social and place-based factors, although distal to the child, still impact their health and development (Bronfenbrenner, 1977). These social and place-based factors that comprise the exosystem in Bronfenbrenner’s model are often referred to as social determinants of health. These social determinants consist of the systems and environments in which the child is embedded. Despite the distal representation of these factors in the model, they influence all aspects of the child’s environment.
Previous studies have found that many social determinants of health are associated with a child’s exposure to violence and their likelihood of accessing treatment after such exposures (Hunter & Flores, 2020; Morris et al., 2019). Within violence exposure research, the neighborhood in which a child is raised is often conceptualized as an influential factor that goes beyond frequency of exposure to community violence. In fact, the neighborhood environment is recognized as an integral part of a child’s development that influences differences in a child’s rates of mental and physical health and access to healthcare (Bronfenbrenner, 1977; Jackson et al., 2019; Lynch, 2003; Morris et al., 2019). The neighborhood and overall exosystem of a child can present as both a risk and a protective factor in a child’s development. A neighborhood may promote or hinder a child’s access to resources and other instances of opportunity by impacting factors such as the types of after-school activities, public transportation, and the quality of food they have access to. For example, if a child lives in a neighborhood with high levels of opportunity, the child may have increased access to safe outdoor play spaces and local community activities, such as team sports. The increased availability of outdoor play spaces and community activities could contribute to increased physical activity, mental well-being, and improved overall health. In contrast, living in a neighborhood with low levels of opportunity could indicate children are without safe outdoor play spaces, which could result in them spending time in areas that increase their risk of exposure to violence. In addition, the opportunity level of the neighborhood could impact the number of relationships the child makes outside the home, potentially limiting their ability to form robust support systems. All these factors influence how a child develops and their opportunities for support and treatment after exposure to violence. The indirect influence of the exosystem is therefore important to account for, when assessing how children engage and respond to treatment following exposure to violence.
The Mesosystem—Interaction Between the Systems
The mesosystem is made up of the interactions between the various components of the child’s microsystem but that do not directly involve the child (Bronfenbrenner, 1977). For many children, this is most often the interaction between their teachers (school microsystem) and their parents/primary caregivers (family microsystem). Because it is based on interactions that occur while the child is not present, the impact of the mesosystem on the child can be hard to operationalize within research. However, one way it can be partially measured is by looking at the parent/primary caregiver’s (henceforth referred to as “parent”) levels of social support and stress. Parents’ levels of social support and stress are likely dependent on the other systems in which they interact (their workplace, their relationships with their community, etc.), and could include individuals that also belong to another of the child’s microsystems.
Measures of parent stress and social support are also important to consider when looking at treatment engagement as they can help to conceptualize how the parent may be coping with the child’s exposure to violence. This can provide insight into the family system’s capacity to respond to and support the child. For instance, if a parent has a robust support system that can assist them with childcare, they are likely better equipped to bring a child to appointments than a single parent who does not have other childcare options. In addition, a parent who has a high level of stress from their job might find it harder to cope with the added stress of their child’s emotional and behavioral problems as compared to a parent with lower stress levels.
The Microsystem—Individual and Family Factors
The majority of a child’s microsystem is their family environment. Although peer relationships and school are also included in the microsystem, previous research has indicated that the family has a relatively influential role in determining a child’s response to and subsequent functioning after exposure to violence (Lynch, 2003). A child’s immediate familial surroundings impacts their coping strategies and how they make sense of an event. In addition, many children can experience violence within the family, making the family not only a critical vehicle through which they receive treatment but also a possible additional source of risk. For this reason, it is important to study both characteristics of the individual child as well as the family to better understand what factors enhance or hinder treatment engagement after exposure to violence.
Family income and the number of people supported by that income, is also a crucial aspect of the microsystem that can impact both exposure to violence and treatment engagement. Previous studies have indicated that children from low-income families or those with low social capital, experience higher rates of exposure to violence and are less likely to have access to treatment (Hanson et al., 2006; Jackson et al., 2019, Kim & Drake, 2018). In fact, one of the most significant barriers to mental health treatment can be cost. However, even when services are offered at no-cost, the income level of a family can still present barriers to treatment engagement as it may impact a family’s ability to travel to the appointment, find appointment times that are outside their work schedule, etc. In addition, a family’s income level can impact the effectiveness of treatment after exposure to violence as it often determines the type of access children have to resources that promote resilience.
Racial Disparities—A Factor That Cuts Across System Levels
It is critical that the impact of race is accounted for when taking a systems-level approach to understanding treatment engagement and effectiveness after exposure to violence. Black, Latinx, Asian, and Indigenous children have lower rates of mental health treatment engagement in comparison to White children (Atdjian & Vega, 2005; Burns et al., 2004; Costello, et al., 2014; Fraynt et al., 2014; Pumariega et al., 2013; Risser & Schewe, 2013). These differences are likely due to racial disparities in access to mental health resources, historic and systemic racism, as well as internalized stigma surrounding the use of mental health resources. In addition, many studies have found increased rates of lifetime violence exposure among Black children (Collins, et al., 2010; Kilpatrick et al., 2003). The combined influence of facing increased incidence of violence exposure and lower rates of treatment engagement can further exacerbate disparities among racial groups.
It must be recognized that an individual’s race does not put them at increased risk for violence. Rather, racial disparities in CEV likely result from macrosystem-level social forces such as structural racism and systemic oppression that have led to segregation and an increased likelihood of Black, Latinx, and Native American families living in neighborhoods with lower income levels and decreased resources (Collins et al., 2010; Halfon et al., 2020; Kim & Drake, 2018; Slopen & Heard-Garris, 2022). Unfortunately, the effects of these inequities may manifest at every level of a child’s ecological system. For the purposes of this study, we will operationalize the impact of race at the macrosystem level. Although racial identity is collected at the individual level, we make this distinction to highlight that the impact of race results from societal influences rather than individual characteristics.
Statement of the Problem
To combat disparities in treatment engagement and completion, it is important that we understand how risk and protective factors at the individual, family, and neighborhood level interact to impact treatment engagement and effectiveness. Many studies of children’s exposure to violence focus solely on individual and family risk and protective factors that contribute to treatment engagement and outcomes (Kolko et al., 2003; Koverola et al., 2007; Lynch, 2003; Risser & Schewe, 2013). In addition, previous research has also often limited the types of violence that are studied in a given sample, focusing either solely at the microsystem level by studying child maltreatment (Hunter & Flores, 2020), or solely at the exosystem level by looking at community violence (Fowler et al., 2009; Jackson et al., 2019; Lynch, 2003). Given the interaction between these systems, it is important that multiple levels and types of violence exposure are considered within the same sample to understand the relative contribution of each system level on treatment engagement and effectiveness. In addition, while many studies focus on identifying risk factors for violence exposure, very few studies have examined what factors impact whether children exposed to multiple types of violence engage in treatment. While identifying risk factors to direct prevention efforts is undoubtedly important, it is also imperative that we begin to understand what factors contribute to treatment engagement in pediatric populations with exposure to violence.
This study aims to compare factors at the child (individual system), family (microsystem), and neighborhood/societal (exosystem) levels to understand the combined influence these factors may have on child treatment engagement and effectiveness.
Hypotheses
We predict that children who complete treatment relative to those who do not will: (1) live in neighborhoods with higher levels of child opportunity; (2) report lower levels of exposure to community violence; (3) report higher levels of parental social support; (4) report lower levels of parental stress; (5) report a higher annual household income; (6) have fewer people living in the home; and (7) report higher levels of child social support. We also predict that the percentage of children who identify as White will be higher in the group that completes treatment. We posit that there will be no differences in clinical symptoms related to behavioral and emotional problems across the engagement groups, as we expect that all children by virtue of being exposed to violence will present with similar clinical symptom levels.
However, we hypothesize that the children who complete treatment will show higher rates of improvement across the treatment period. We also predict that children that live in areas with higher rates of child opportunity will report increased treatment effectiveness.
Method
This study reviews data collected from children who were referred to mental health services at 12 community-based sites in Illinois from 2001 to 2015 after exposure to violence.
Participants
Participants included 2,546 CEV and the individual serving in the primary parental role (referred to as parent throughout the rest of this manuscript). Children were referred to services for a range of violence types. A majority (64%) of the children were referred for witnessing domestic violence, 8% had experienced child abuse, 3% had experienced community violence, 24% experienced some combination of the three violence types, and 1% reported experiencing violence classified as “other.” The sample was diverse in age and race/ethnicity but largely of lower socioeconomic status. Children were aged 1–17 years (M = 4.9, SD = 3.1) and identified as 40% White, 26% Black, 20% Latinx, 11% Biracial, 1% Asian, and 1% Other. Most families (79%) reported an annual household income below $40,000. Most of the children’s parents were not in an ongoing relationship at the time of intake (71%) and 42% of children were currently living in single-parent homes.
Children were categorized into three groups based on their treatment engagement, Nonengagers, Attriters, and Completers. Children who attended an intake session but never started treatment were categorized as Nonengagers. Children who started treatment but discontinued prior to reaching treatment goals were categorized as Attriters. Children who completed treatment as rated by the treating therapist, were categorized as Completers. These categories are consistent with previous research (Koverola et al., 2007; Risser & Schewe, 2013). The “Nonengager” group was made up of 813 children (32%), the “Attriter” group, made up the largest portion of the sample (n = 974, 38%) and the “Completer” group included 759 children (30%). The number of sessions a child attended varied depending on their presenting needs, ranged from 1 to 146 sessions (M = 11.71 sessions, SD = 12.84; for Attriters and Completers).
Measures
Background information form
The Background Information Form (BIF) was created specifically for this study to collect demographic information, child’s current symptom levels, the type and severity of violence exposure, child’s developmental history, and family characteristics such as annual household income, number of people living in the home, and current zip code at intake. In addition, each parent rated whether their child had positive experiences or support in five different areas of their life; these items were summed to provide an overall score of the child’s social support on a 0 to 5 scale with higher scores indicating more social support. It should be noted that in some families more than one child received treatment and in these cases each measure was completed individually for each child. The BIF was administered in a semi-structured interview format and included ratings by the therapist of both the child’s and parent’s functioning.
As part of the BIF, the parent who was present at intake completed a self-report rating of their own social support from family and friends or community members on a 3-point Likert scale where 0 was “No support” and 3 was “High level of support.” The two items were summed to give a total rating of parent social support ranging from 0 to 6. Finally, both the parent and the therapist rated the parent’s stress level on a 10-point Likert scale, where 10 was the highest level of stress.
Child emotional and behavioral problems
Each child’s level of behavioral and emotional problems was assessed using the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2000) at intake, during treatment, and at the end of treatment. Two versions of the caregiver-report CBCL were used. One version was designed to be used with children aged 1.5–5 years and contains 99 items. The second version was designed to be used with children aged 6–18 years and contains 112 items. The items on the CBCL can be combined to generate seven syndrome scales (Aggressive Behavior, Anxious/Depressed, Attention Problems, Emotionally Reactive, Sleep Problems, Somatic Complaints, and Withdrawn), two subscales (Internalizing and Externalizing), and a total score. The Internalizing subscale is intended to capture problems pertaining to the self and includes the Anxious/Depressed, Emotionally Reactive, Somatic Complaints, and Withdrawn scales. The Externalizing subscale assesses problems related to dealing with others and includes the Aggressive Behavior and Attention Problems scales. The CBCL is well researched and widely used, scores are provided as t-scores with scores from 60 to 63 indicating the borderline clinical range and scores of 64 or greater indicating clinical range (Achenbach & Rescorla, 2000). The CBCL was administered to all children at intake (referred to as Time 1) and again around the eighth session or at termination (referred to as Time 2). Nonengagers were mailed CBCL forms to complete and mail back for Time 2 assessments.
Child exposure to community violence
At intake parents also completed a 19-item measure, that was an adapted version of the Childhood Exposure to Community Violence (Amaya-Jackson, 1998). This parent-report checklist was used to measure the child’s exposure to community violence. Parents responded to items such as “Has the child been threatened with serious physical harm by someone in the community?” The parent rated 12 items on a Likert-type scale, 0 (“Never”) to 3 (“4 or more times”), and 7 items were scored, Yes (scored 1) or No (scored 0). There was also an option for the parent to select that they “don’t know” for each item. The child then received a total score ranging from 0 to 43 with higher scores indicating a higher exposure to community violence.
Child opportunity at the neighborhood level
The Child Opportunity Index (COI) 2.0 (diversitydatakids.org, 2021) is a measure of opportunity for children across the U.S. that is calculated at the neighborhood level based on data from 72,000 neighborhoods across the nation. The COI 2.0 provides both nationally normed and state-normed scores of the total opportunity as well as neighborhood opportunity across three domains (health and environmental, social and economic, and education). The overall opportunity score is calculated using 29 indicators within these domains, such as rates of housing vacancy, poverty and employment, and air quality. Each neighborhood is also assigned an opportunity score that is normed at the national level and ranges from 0 to 100, where 100 is very high opportunity. Neighborhoods also received opportunity level scores (very low, low, moderate, high, or very high) for the total opportunity as normed at the national, state, and metro-level. For the purposes of this study, we will focus on national and state normed scores.
GIS overview
Mapping was completed using ArcGIS Pro 2.5.0 software. All zip codes within Illinois were geocoded according to the zip code tabulation areas (ZCTA) from the 2010 Census. Children were mapped according to the zip code they provided at intake. Choropleth maps were created from the various COI 2.0 measures, generating two thematic maps that displayed the gradient of child opportunity across the state (see Figures 1 and 2). Children were matched based on zip code location to their subsequent scores of neighborhood opportunity. Scores were extracted from the map and added to the database for analysis along with self-report data.

Choropleth map of child opportunity by state normed opportunity levels.

Choropleth map of nationally normed child opportunity score.
Data Analytic Plan
Analyses were conducted in SPSS Version 26. First, a series of one-way analysis of variance (ANOVA) tests were used to examine differences across the three treatment engagement groups on all continuous clinical, child-level, family-level, and neighborhood-level factors. Post hoc analyses were examined for significant results to determine which groups differed. Cross-tabulations (using χ2 statistic) were used to examine differences across the treatment engagement groups on categorical variables. A one-way analysis of covariance (ANCOVA) test was used to test for differences in treatment outcomes when controlling for clinical symptomology at intake. Finally, multiple regression models were used to test the impact of neighborhood opportunity scores on treatment outcomes. For any variables that exhibited a non-normal distribution, sensitivity analyses were run to ensure that the selected statistical test was robust enough to detect effects without a transformation of the variable. Based on the sensitivity analyses, all results were found to withstand any skewness in the data, therefore all normalized results are reported.
Results
Descriptive statistics for the sample are provided in Table 1, demographic information is provided for the total sample as well as by engagement group.
Sample Demographics by Engagement Group.
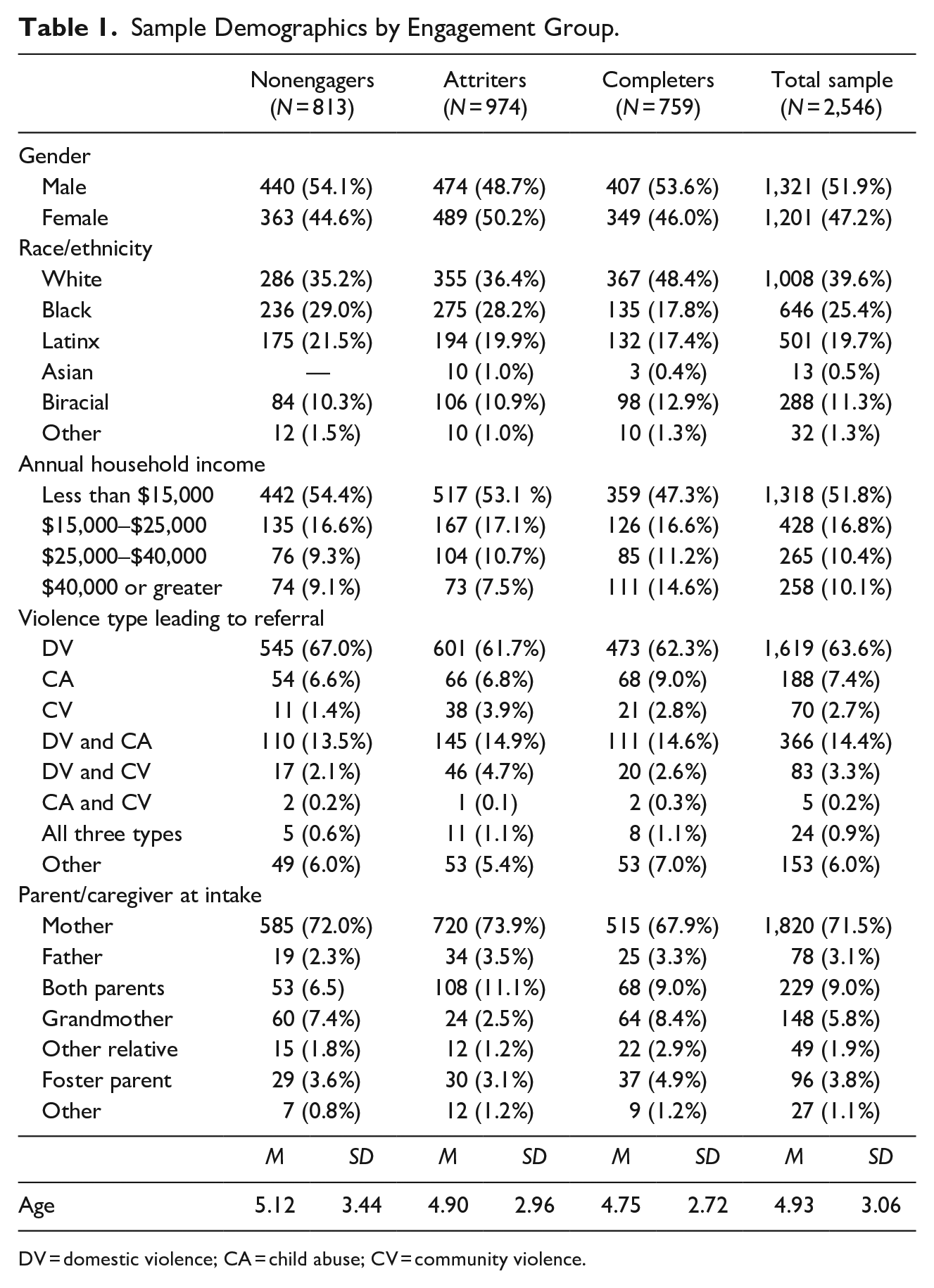
DV = domestic violence; CA = child abuse; CV = community violence.
Child-Level Factors
Clinical symptoms across treatment groups at intake
One-way Welch ANOVAs demonstrated a significant main effect of treatment engagement group on CBCL T-scores. Results demonstrated significant differences by treatment engagement group membership on CBCL Total Score, Welch’s F(2, 908.86) = 3.17, p = .043, partial η2 = .005; CBCL Externalizing Score, Welch’s F(2, 908.31) = 3.11, p = .045, partial η2 = .005; and CBCL Internalizing Score, Welch’s F(2, 909.05) = 4.24, p = .015, partial η2 = .006. See Table 2 for the average T-scores by group. Games-Howell post hoc analysis revealed that Nonengagers demonstrated significantly lower mean CBCL Total Scores than Attriters, with a mean difference of 2.23 (95% CI [0.08, 4.38], p = .040). Nonengagers demonstrated significantly lower mean Externalizing Scores than Attriters, with a mean difference of 2.35 (95% CI [0.12, 4.58], p = .037). Nonengagers also had a significantly lower mean Internalizing Score than Attriters (mean difference of 2.19, 95% CI [0.20, 4.18], p = .027) and Completers (mean difference of 2.18, 95% CI [0.24, 4.12], p = .023).
CBCL Mean Scores by Engagement Group at Time 1 and Time 2.

CBCL = Child Behavior Checklist.
Additional child-level factors
No significant differences were found by engagement group on the parent-reported risk factor of community violence exposure F(2, 2556) = 1.90, p = .15. There were significant group differences found in the protective factor of Child Social Support Welch’s F(2, 1604.73) = 10.21, p < .001, partial η2 = .008. Specifically, Games-Howell post hoc analyses determined that the Completer group had significantly higher average scores of Child Social Support (M = 4.11; SD = 1.02) than Attriters (mean difference: 0.23, 95% CI [0.06, 0.32], p < .001) and Nonengagers (mean difference: 0.19, 95% CI [0.10, 0.36], p = .001). There were no significant differences between the Attriters and Nonengagers on ratings of Child Social Support.
Family-Level Factors
A one-way Welch ANOVA determined that there were statistically significant differences in the number of people living in the home across engagement group membership Welch’s F(2, 1528.28) = 9.49, p < .001, partial η2 = .008. Games-Howell post hoc analysis revealed that children in the Completer group had significantly fewer people living in the home than the two other groups (Completers vs. Attriters, −0.29, 95% CI [−0.49, −0.10], p = .001; Completers vs. Nonengagers, −0.34, 95% CI [−0.54, −0.14], p < .001). There were no significant differences in number of people living in the home between the Attriter and Nonengager groups. Cross-tabulation determined that there was a significant association between treatment engagement and Annual Household Income χ2(6) = 28.30, p < .001, Cramer’s V = 0.08, such that Completers were more likely to have an Annual Household Income of $40,000 or greater (43%) than to have an Annual Household Income of less than $40,000 (range: 27%–32%). Attriters were more likely to have an Annual Household Income of less than $40,000 (39%).
A one-way ANOVA demonstrated a main effect of group for Parent Social Support F(2, 2370) = 14.61, p < .001, partial η2 = .012. Parent Social Support was significantly higher in the Completers group than the Attriter group (0.44, 95% CI [0.24, 0.65], p < .001) and Nonengager group (0.39, 95% CI [0.18, 0.61], p < .001). However, no group differences in Parent Social Support were found between Attriters and Nonengagers. Significant differences were also found across engagement group for Self-reported Parent Stress F(2, 1476.89) = 3.59, p = .028, partial η2 = .003. Parent Stress increased from Completers (M = 6.36, SD = 2.42), to the Nonengagers (M = 6.40, SD = 2.58), and then again to Attriters (M = 6.68, SD = 2.62). Post hoc analyses determined that Attriters had significantly higher reports of stress than Completers (0.32, 95% CI [0.02, 0.62], p = .04). However, there were no significant differences found between Nonengagers and Completers or Nonengagers and Attriters. In addition, no significant differences were found between the groups on Therapist-rated Parent Stress Welch’s F(2, 1385.72) = 2.60, p = .075.
Neighborhood-Level Factors Across Treatment Groups
A one-way ANOVA of the overall Neighborhood Childhood Opportunity (nationally normed) showed statistically significantly group differences, F(2, 2543) = 10.83, p < .001, partial η2 = .008. Neighborhood Child Opportunity Scores increased from the Nonengagers (n = 813, M = 32.10, SD = 27.28), to Attriters (n = 974, M = 35.42, SD = 28.87), to Completers (n = 759, M = 38.67, SD = 27.47). Tukey-Kramer post hoc analyses revealed significant differences between all groups. The average increase in Child Opportunity Score from Nonengagers to Attriters was 3.32 (95% CI [0.20, 6.43], p = .033), the increase from Attriters to Completers was 3.25 (95% CI [0.07, 6.42], p = .04), leading to a mean increase of Neighborhood Childhood Opportunity Score from the Nonengagers to Completers of 6.56 (95% CI [3.26, 9.87], p < .001).
Cross-tabulation was used to analyze treatment engagement group differences in Neighborhood Opportunity Level. All four measures were run twice, once based on national norms and again based on state-level norms. Model results are shown in Table 3. There were significant differences between treatment engagement groups across all measures of childhood opportunity at the neighborhood level except for neighborhood educational opportunity based on state norms.
Chi-Square Values for Neighborhood Child Opportunity Level Scores by Treatment Engagement Group.

Additionally, the total Neighborhood Opportunity Level was mapped across the state of Illinois and visualized based on state norms (Figure 1) and national norms (Figure 2).
Treatment Outcome by Engagement Group and Neighborhood Opportunity
A one-way ANCOVA was used to test for differences in CBCL Total Score at Time 2 while controlling for scores at Time 1. There was a statistically significant main effect of group for the Time 2 CBCL Total Score after controlling for pre-treatment CBCL scores, F(2, 617) = 11.54, p < .001, partial η2 = .033. Adjusted means are presented, unless otherwise stated. Total CBCL Score at Time 2 was significantly lower in the Completer group (M = 48.45, SE = 0.52) compared to the Attriter group (M = 52.04, SE = 0.79) by 3.59 points (95% CI [1.32, 5.86], p < .001) and the Nonengager group (M = 52.79, SE = 1.02) by 4.34 points (95% CI [1.60, 7.08], p < .001). There were no significant differences between the Nonengager and Attriter groups on the CBCL Total Score.
Multiple regression models were conducted to examine the impact of neighborhood child opportunity score on treatment outcomes. While there was a significant effect of neighborhood opportunity on behavioral and emotional symptoms at intake F(1, 1453) = 11.15, p = .001 with the CBCL Total Score increasing by about 0.04 points for every 1-point increase in child opportunity, no significant differences were found by neighborhood opportunity in the change in CBCL Total Score from Time 1 to Time 2 F(1, 673) = 1.50, p = .22.
Racial Differences in Treatment Engagement
Cross-tabulation determined that there was a significant association between treatment engagement and race χ2(8) = 52.52, p < .001, Cramer’s V = 0.11.1 Children who completed treatment were more likely to be identified as White (49%) than other racial identities. Children who identified as Black were more likely to be Attriters (43%) and Nonengagers (37%) than Completers (21%).
Supplemental Analyses
To account for families where more than one child was receiving care, supplemental analyses were run using only one child per family (n = 1,528). The majority of the analyses were replicated within the one child sample with little change in p-value and effect size; exceptions are presented here. A one-way Welch ANOVA determined that the number of people living in the home did not differ significantly across the engagement groups Welch’s F(2, 906.50) = 2.76, p = .064, partial η2 = .004. Instead, the effect was seen as trending toward significance, with no significant group differences in the number of people living in the home between the Completers and Attriters (p = .15) or Nonengagers (p = .09). In addition, although there were not statistically significant differences between engagement groups on Therapist-rated Levels of Parent Stress in the full sample, a one-way ANOVA found that there were significant differences in the one-child sample F(2, 1254) = 3.30, p = .037. Post hoc analyses determined that Attriters had significantly higher reports of stress than Completers (0.37, 95% CI [0.02, 0.72], p = .04).
Discussion
The purpose of this study was to examine how different levels of a child’s ecological system affected treatment engagement and treatment outcomes after exposure to violence. Overall, we found mixed support for the hypotheses. Our findings indicate that children who completed treatment were more likely to identify as White and had lower levels of parental stress, higher incomes, fewer people living in the home, and higher levels of social support for both the parent and child. In addition, those that completed treatment showed higher rates of symptom improvement across the treatment period. We also found that those children who completed treatment were more likely to live in neighborhoods with higher levels of child opportunity, however the level of child opportunity in which a child lived did not impact treatment effectiveness. We did not find support for our hypothesis that children would present with similar initial levels of emotional and behavioral problems following exposure to violence and prior to treatment. Rather, Nonengagers had significantly lower CBCL Total Scores, CBCL Externalizing Scores, and CBCL Internalizing Scores than Attriters. In addition, Nonengagers had significantly lower CBCL Internalizing Scores than Completers. Our findings also did not support our hypothesis that children who completed treatment would have lower levels of exposure to community violence.
Given that the CBCL used in this study was based on parent-report, it is possible that the parents of the children in the Nonengager group felt as though their children were coping well enough after their exposure to violence, such that they did not need treatment. It is also possible that the treatment barriers faced by the family outweighed the family’s perception of the child’s need for treatment. If this is the case, it may be a contributing factor as to why they did not attend any treatment sessions. Although children that dropped out of treatment (Attriters) presented with the highest levels of emotional and behavioral problems as measured by the CBCL Total Score, Externalizing and Internalizing Scores, there were no significant differences found at intake between the presenting symptomology of Completers and Attriters. This lack of difference between the two groups suggests that their different engagement behaviors—successfully completing treatment versus dropping before completion—were likely related to factors other than the parents’ perception of the child’s emotional and behavioral problems.
There were, however, significant differences in treatment outcomes between those who completed treatment and those who did not. Children who completed treatment exhibited greater improvements in behavioral and emotional functioning than those who did not engage in treatment (Nonengagers) or started treatment but did not successfully complete (Attriters). This indicates that Completers benefitted from their increased engagement in treatment. This finding is significant because it supports previous research that one of the most important protective factors for children that have been exposed to violence is receiving treatment (Berkowitz, 2003; Schewe et al., 2013; Wethington et al., 2008). Thus, we can reasonably expect that efforts aimed at increasing treatment engagement could also improve treatment outcomes and overall functioning in CEV.
We found that Completers had significantly more social support and their parents had higher levels of social support than other engagement groups. These findings highlight the influence of protective factors in both the microsystem (the child and the family) and the mesosystem (interaction between the systems) have on the child’s treatment engagement. These results also suggest that using a strengths-based approach when screening and assessing children post-violence exposure may aid providers in identifying additional treatment targets related to finding and building social support that can facilitate treatment engagement. The Completer group also had lower scores of self-reported parent stress; however, there were no differences found between the engagement groups in therapist-rated parent stress. These results indicate that therapists in the study may not be accurately gauging the level of stress a parent is experiencing; this may lead them to miss signs that the parent may not be able to support their child through completing treatment. This highlights the need for providers to include a parent’s self-reported level of stress in treatment planning. Future studies should aim to build on these findings by including additional measures of mesosystem level factors that impact social support such as the parent’s relationships with others in the child’s life like teachers, coaches, or neighbors.
Our findings did not support the hypothesis that children living in neighborhoods with higher scores of child opportunity benefitted from treatment more than children living in areas with lower opportunity scores. This is promising because it indicates that treatment effectiveness is not dependent upon the level of child opportunity in a given neighborhood. Therefore, if providers can successfully engage children in neighborhoods with lower child opportunity in treatment after exposure to violence, they can expect the treatment to have a similar effectiveness with these children. While the neighborhood child opportunity level may not impact treatment outcomes, it did impact treatment engagement. In fact, several of the variables that could represent social determinants of health both at the exosystem and microsystem level were found to differ across treatment engagement groups. Children in the Completer group were more likely to live in neighborhoods with higher scores of overall child opportunity, have fewer people living in their home, and have higher total annual household incomes. In considering neighborhood-level factors it is important to note that we did not find differences between the treatment groups on exposure to community violence. This suggests that studies that limit the impact of the neighborhood to this single variable could underestimate the impact of exosystem level factors on a child’s treatment engagement after exposure to violence.
Consistent with previous studies, children in the Completer group were also more likely to be White, and children in the Nonengager and Attriter groups were more likely to be Black. Our findings add to the literature examining factors that facilitate and inhibit treatment engagement in families of color at the community-level (Atdjian & Vega, 2005; Burns et al., 2004; Costello, et al., 2014; Fraynt et al., 2014; Pumariega et al., 2013; Risser & Schewe, 2013). As mentioned previously, differences in treatment engagement by race could be due to disparities in the macrosystem and the impact of systemic oppression and structural racism on policy, culture, and the built environment (Collins et al. 2010; Halfon et al. 2020; Kim & Drake, 2018; Slopen & Heard-Garris, 2022). These disparities compound the effects of social determinants of health at all levels of the social ecology through an unequal distribution of opportunity. While beyond the scope of this study, it is important to consider the historic role of inequity and exploitation within child-serving systems that could contribute to an ongoing lack of trust in traditional methods of mental health treatment and social service providers. Unfortunately, until some of these more macrolevel influences are addressed, we are likely to continue to see racial disparities in treatment engagement. To that end we underscore the calls of other researchers (Halfon et al., 2020; Slopen & Heard-Garris, 2022) for advancing work that addresses racial health disparities by investing in equitable systems and policies aimed at assisting families.
Our study supports the theory that a child’s ability to receive treatment after exposure to violence is impacted by the systems in which they live and grow. Children from families that have more resources and that live in areas with greater access to opportunity are more likely to complete treatment. Furthermore, our findings indicated that children that completed treatment had improved behavioral and emotional functioning. While a child’s neighborhood opportunity index did not impact the benefit they saw from treatment once they engaged, it did impact their level of engagement; such that children in lower opportunity areas were less likely to engage in treatment that would improve their behavioral and emotional functioning. This is a classic example of health disparity. Families that experience more risk factors for violence exposure also experience the compound effects of disparities in access to and effectiveness of treatment. Low-income families have reported barriers to receiving treatment including lack of reliable transportation and lack of reliable child-care for siblings (Lyon et al., 2013). Although our study did not ask directly about barriers to treatment, our results demonstrated consistent group differences in risk factors (number of people living in the home, annual income, and parent stress) across the engagement groups. In order to improve treatment engagement, providers can consider including assessing barriers to treatment during the intake process and addressing any identified barriers within the treatment plan. In addition, to improve equity in access to mental health resources, models or interventions including family support or peer support specialists could be implemented. Furthermore, training providers to assess barriers through a cultural competency model can help to protect against approaching families through a lens of white privilege. This is important because such a lens could lead providers to underestimate the parent’s level of stress or lack of control a parent might feel in their ability to engage in their child’s care.
Overall, our study suggests that efforts toward building community capacity and cohesion and social support in neighborhoods with high incidences of violence might not only help to decrease violence but could also increase mental health treatment engagement. Mental health providers can help by finding ways to increase engagement in mental health treatment for all children whose social determinants of health put them at increased risk for violence exposure and adverse outcomes. Furthermore, this study highlights the importance of better understanding how to support families to reach successful completion of treatment for their children after they have been exposed to violence. These findings also build on the recommendations of previous research of how critical it is that each child’s unique set of presenting risk and protective factors are assessed and integrated into the treatment plan (Berkowitz, 2003; Risser & Schewe, 2013). To provide comprehensive treatment, it is recommended that providers consider the unique family and community systems surrounding each child.
Limitations
There were several limitations to this study. First, due to the large proportion of young children, self-report measures were not utilized; thus, all the child variables were based on parent or therapist report. Second, because there was no standard number of sessions required, the determination of whether a child completed treatment was made by the therapist. While this practice mirrors real-world therapy settings, it is possible that therapists rated children as not completed with treatment when their parents may have felt they had met their goals and/or completed therapy. Third, these data were collected as part of care at several community-based sites where treatment, not research, is the main priority; this led to quite a bit of missing data. Fourth, because this study does not have a control group, we cannot determine with certainty whether improvements seen across the study were in fact due to the treatment provided. Fifth, we could not speak to the impact of the mesosystem on the child other than inferring some level of influence from the parent social support and stress measures; future studies should aim to better target this level of the model. Sixth, while our sample was racially/ethnically diverse, White children still made up 40%, and the sample lacked socioeconomic and geographic diversity. It is possible that a sample at the national level with greater racial/ethnic and socioeconomic diversity could have different results. However, given historic patterns of disparities in communities of color (Collins et al., 2010; Kim & Drake, 2018) it is likely a more diverse sample would strengthen many of the findings. Finally, some of our findings were not replicated in the one child per family sample. This may indicate that the weighting of additional siblings is influencing the effects of the number of people in the home and therapist-rated parental stress in the full sample.
In addition, there are some limitations to the GIS methods used and the COI 2.0 measure (Acevedo-Garcia et al., 2020). Most notably, the COI 2.0 measure is not currently constructed to account for longitudinal, temporal effects. Zip codes boundaries can change slightly over time, and the dataset used for COI 2.0 in this study was based on the boundaries set in quarter 4 of 2015. It is possible that cases seen in different years, particularly those closer to 2001, may have had slightly different neighborhood conditions. In addition, previous research (Grubesic & Matisziw, 2006) indicates that there are limitations to using zip codes for geographic analysis as there are some differences in spatial patterns of zip codes and the ZCTA used in GIS software. Finally, we do not have information on how long families were living at the zip code they provided at intake, and previous research indicates that the amount of time spent in a given neighborhood is critical in determining the impact of that neighborhood on the child’s development (Chetty et al., 2018). Therefore, if a family did not live in the zip code indicated for very long the neighborhood may not have influenced the child. Based on these limitations, it is not surprising that our findings had rather small effect sizes. It is recommended that future studies aim to replicate these findings using participant address and ask about duration of time at each address to identify an address that represents each individual’s childhood home to better account for the temporal neighborhood effects.
Implications
Our study emphasizes the importance of recognizing the various systems in which a child is embedded when considering treatment engagement and effectiveness. A child’s development is impacted significantly not only by individual-level factors but also the characteristics of their family and the community in which they were raised. If we can better understand the impact of various social determinants of health on treatment engagement and effectiveness, we can better address health disparities. Furthermore, our results highlight the importance of assessing and addressing presenting issues of parents to increase pediatric engagement in care, particularly parents who report high levels of stress as they may be less likely to engage and more likely to discontinue their child’s treatment. It is critical that providers recognize that this discontinuation is likely not due to a lack of effort or buy-in from the parent, but often simply because they have other stressors in their lives and their perception of their child’s need for therapy might differ from that of the provider. These competing demands may make it difficult for some parents to continue bringing their child to treatment on a regular basis. Providing parents with resources to address their own stress and consistently working with them to identify and navigate barriers to treatment through efforts such as family navigation programs, parent support, or parent skills training may help to increase treatment engagement and completion in pediatric populations exposed to violence.
Footnotes
Acknowledgements
We would like to acknowledge Dr. Zoran Martinovich for providing statistical consultation on our analyses. Dr. Martinovich is an Assistant Professor at Northwestern University Feinberg School of Medicine and reports no conflicts of interest.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.