
Abstract
Sexual-related post-traumatic stress symptoms (sexual-related PTSS) refers to the traumatic reactions that are replicated during sexual activity among survivors of child sexual abuse (CSA). However, the construct of sexual-related PTSS have been adapted from clinical work with survivors, and research with limited examination of the scales themselves. Given this gap, the current study offers the development of a new measure (PT-SEX) that examines sexual-related PTSS. The study was conducted online, among two convenience samples of women survivors of CSA (study 1 included 451 women and study 2 included 330 women). Six reliable PT-SEX factors emerged from Study 1: Dissociation during sex, intrusiveness during sex, shame and guilt in regard to sexual aspects, pleasing the other during sex, interpersonal distress, and hypervigilance during sex. Study 2 revealed survivors of CSA had significantly higher sexual-related PTSS levels as compared to participants without such a history. Also, post-traumatic stress disorder and sexual-related PTSS made unique and unshared contributions to the observed data, including sexual self-esteem, sexual motives, relationship satisfaction, compulsive sexual behavior, and mental health. CSA significantly moderated the associations between sexual-related PTSS and sexual self-esteem, sexual motivations of self-affirmation and coping, and depression and anxiety. Findings from the current study show that over time, the trauma of CSA seems to be implicated in survivors’ sexual experience. As sexual difficulties are accompanied by sexual-related PTSS, these symptoms are unlikely to resolve by trauma-focused therapy and must be actively targeted in therapy.
Introduction
Previous literature shows that child sexual abuse (CSA) is associated with a variety of sexual difficulties, ranging from hyposexual to hypersexual behaviors (Bigras et al., 2021; Gewirtz-Meydan & Opuda, 2022; Pulverman et al., 2018) and various other negative mental and emotional aspects in relation to their sexuality, such as greater sexual anxiety and distress (Rellini & Meston, 2007), and sexual dissatisfaction (Lemieux & Byers, 2008). Hyposexuality implies that the sexual response is consistently inhibited, typically accompanied by low initiatory behavior and poor sexual functioning, such as problems with sexual desire (Swaby & Morgan, 2009), arousal (Pulverman et al., 2018), orgasm (Swaby & Morgan, 2009), and experiencing sexual pain (Harlow & Stewart, 2005; Leclerc et al., 2010). Hypersexuality refers to intrusive fantasies and thoughts regarding sex, excessive and risky sexual behaviors, and the inability to control one’s sexuality (Abajobir et al., 2017; Slavin et al., 2020). In the current study, variables were chosen based on recent reviews in this field (Bigras et al., 2021; Gewirtz-Meydan & Opuda, 2022; Pulverman et al., 2018; Slavin et al., 2020) to represent the range of sexual difficulties following trauma, from hypersexual (compulsive sexual behaviors) to hyposexual behaviors (sexual dysfunction), and emotional and mental aspects of sexuality (motivations for sex, sexual-esteem). Notwithstanding this wealth of research on sexual difficulties in the aftermath of CSA, our understanding of the mechanism explaining the association between CSA and sexual difficulties in adulthood is limited. One of the main theoretical conceptualizations of this association relies on trauma theories that posit a direct link between different aspects of sexual abuse and different traumatic reactions (e.g., Bird et al., 2014; Bornefeld-Ettmann et al., 2018; Gewirtz-Meydan & Lahav, 2020; Kratzer et al., 2022; Lorenz et al., 2015).
The various sexual difficulties of CSA survivors can be viewed through a trauma prism. For example, a growing body of knowledge reveals that trauma is reflected in the body and that the memory of the trauma lies in the somatosensory system (Ensink et al., 2016; van der Kolk, 2014) and can account for CSA survivors’ various physical conditions, such as chronic pain, or fibromyalgia (Daphna-Tekoah, 2019; Tsur, 2020). As for sexual function, traumatic experiences that included touch are thought to be stored in the body as implicit memories and unpleasant sensations, and the survivor’s ability to experience sexual pleasure is thus seriously impacted (Gewirtz-Meydan & Ofir-Lavee, 2020; Zoldbrod, 2015). Another main theory that has been extensively used in explaining the many negative psychological outcomes following CSA, and sexual outcomes in specific (Bigras et al., 2021; Buehler, 2008; Easton et al., 2011; Lemieux & Byers, 2008; Theunissen, 2018), is the traumagenic model of Finkelhor and Browne (1985) which describes four traumagenic dynamics of CSA: betrayal, powerlessness, stigmatization, and sexualization. The traumagenic dynamics model is particularly useful for understanding how CSA may contribute to later sexual difficulties. These traumagenic dynamics can harm the ability and willingness of the survivor to engage in intimate and sexual relationships in many ways. The feeling of betrayal can lead survivors to avoid emotional and sexual relationships in the future (Theunissen, 2018), stigmatization and powerlessness can have serious effects on survivors’ sexual self-concept and sexual-esteem (Meston et al., 2006; Rellini & Meston, 2011), and sexualization can affect survivors’ social functioning on two levels: emotional (e.g., avoidance or fear of sexual intimacy and/or feelings of guilt during sex) and behavioral (e.g., problems experienced with touch and sexual arousal; Easton et al., 2011; Matorin & Lynn, 1998; Najman et al., 2005).
Based on these trauma theories, CSA survivors’ sexual difficulties evolve from the traumatic experience of the abuse (O’Driscoll & Flanagan, 2016; Rellini & Meston, 2007) and are mediated by trauma-related biological, cognitive, and affective processes (Yehuda et al., 2015). In other words, although sexual dysfunction may appear similar in behavioral manifestations to those of people with no history of CSA (e.g., their physical symptoms may align with those described in the DSM-5 for sexual dysfunction, and they may have high levels of compulsive sexual behavior, above the clinical cutoff), their history of CSA suggests that these sexual dysfunctions developed differently: They may have evolved from the traumatic experience of the abuse and as such have a different, and unique, mechanism that maintains them (Gewirtz-Meydan & Ofir-Lavee, 2020; Pulverman et al., 2018).
Most of the studies investigating the association between CSA and sexual difficulties in adulthood in relation to trauma, have examined the association between sexual-related variables and various trauma-related symptoms, such as post-traumatic stress disorder (PTSD) symptoms (Bornefeld-Ettmann et al., 2018; Gewirtz-Meydan & Lahav, 2020; Kratzer et al., 2020), sympathetic nervous system activation (Lorenz et al., 2015), and dissociation (Bird et al., 2014). However, we expect that the PTSD symptoms that include intrusion (e.g., flashbacks, nightmares), avoidance (e.g., avoidance of trauma-related thoughts or feelings and reminders), alterations in cognition and mood (e.g., overly negative thoughts and assumptions about oneself or the world, negative affect), and hyperarousal symptoms (e.g., irritability and aggression, difficulty sleeping) will be manifested within the sexuality of survivors, thereby affecting their sexual self-concept (Meston et al., 2006), their cognitions related to sex (Rellini et al., 2011), their dissociative experiences during sex (Bird et al., 2014; Hansen et al., 2012), and their feelings toward sex, such as guilt, and shame (Kilimnik & Meston, 2021).
To the best of our knowledge, however, there is to date no single comprehensive scale that examines how traumatic reactions are replicated during sexual activity. Based on the trauma perspective, and given this gap in the literature, the current study offers the development of a new scale that examines sexual-related post-traumatic stress symptoms (sexual-related PTSS), based on the established clusters of PTSD symptoms (intrusion, avoidance, alterations in cognition and mood, and hyperarousal symptoms). Integrating knowledge obtained from professionals from the fields of trauma, child sexual trauma, and human sexuality, the current study sought to develop a new scale that examines sexual-related PTSS—which is a unique set of sexual patterns that refer to the distortions of the survivor’s physical, cognitive, and emotional approach toward sex, due to the sexual trauma. In other words, these symptoms exemplify the traumatic experiences that are embedded within the sexual patterns of the survivor.
We suggest that the PTSD symptom clusters should serve as the basis for understanding how the ramifications of the trauma and the PTSD symptoms are manifested in the survivor’s sexual patterns. For example, for CSA survivors who suffer from intrusive symptoms, various aspects of sexual contact, such as touch, nudity, flirting, oral or genital stimulation, and/or any kind of penetration, might be triggering (Maltz, 1988; O’Driscoll & Flanagan, 2016; Staples et al., 2012). Thus, during sexual interactions, survivors might suffer from flashbacks and other re-experiences of the trauma (Buehler, 2008; Kristensen & Lau, 2011) which can also include dissociation (e.g., Bird et al., 2014; Classen et al., 2001; Hansen et al., 2012), which interfere with the sexual response cycle and intensify distress and dysfunction. It is also highly likely that avoidance symptoms would be manifested in the sexual domain, namely, as avoidance of sexual interaction or sexual-related stimuli in CSA survivors. In addition to avoiding sex itself, survivors might also avoid different sexual acts or feelings, and such avoidance could be specific to sexual interactions with others, or it could be more generalized. Alterations in cognition and mood would likely consist of survivors’ negative beliefs about sex (e.g., “sex is harmful and disgusting”), about themselves (e.g., “I am unworthy of sexual pleasure”), and about others (e.g., “he/she uses me as a sexual object”), as well as various negative emotional reactions toward sex, such as guilt and shame (Kilimnik & Meston, 2021), anxiety, fear, and disgust (Meston et al., 2006), all of which have been documented among CSA survivors. Finally, hypervigilance, which refers to physiological processes related to hyperarousal might be implicated in sexual difficulties among CSA survivors. Hypervigilance, as part of hyperarousal, might limit an individual’s ability to focus on pleasant sensations and could exacerbate unpleasant sensations, such as sexual pain (Payne et al., 2005). In addition, activation of the sympathetic nervous system subsequent to sexual stimulation might lead to a fear response in traumatized survivors, due to the excessive sympathetic stimulation that is characteristic of PTSD (Yehuda et al., 2015). This over-stimulation, in turn, could reduce sexual desire and arousal (Lorenz et al., 2012; Rellini & Meston, 2006).
The Current Study
The overall goal of the proposed study was to better understand the sexuality of CSA survivors. Guided by the trauma perspective, and the well-established association between CSA and various hypersexual/hyposexual behaviors (Abajobir et al., 2017; Gewirtz-Meydan & Opuda, 2022; Leonard & Follette, 2002; Pulverman et al., 2018; Slavin et al., 2020), in the current study we hypothesized that there would be a unique and unshared contribution (beyond the PTSD symptoms that have been officially established in the literature and recognized in the DSM-5) of sexual-related PTSS to survivors’ sexuality. Due to the lack of measures assessing sexual difficulties experienced by individuals with histories of sexual trauma, in the current study we aimed to develop a scale to measure traumatic reactions during sexual activity, and we did so via conducting two independent studies: Study 1 was designed to create the final format of the PT-SEX questionnaire and assess its construct. In Study 2 we examined whether sexual-related PTSS (as measured by the PT-SEX scale) made a unique and unshared contribution (beyond PTSD symptoms) to survivors’ sexual esteem, compulsive sexual behaviors, sexual motives, and mental health (anxiety and depression).
Study 1
In this study we examined the psychometric properties of the proposed instrument.
Method
Participants and procedure
We conducted an online survey of a convenience sample of men and women. Participants were recruited via social media (using Facebook and Instagram). We aimed to oversample women in romantic relationships, and women that were CSA survivors, by posting advertisements in specific interest groups. The survey was accessible through Qualtrics, a secure web-based survey data collection system. The survey took 10 minutes to complete, on average, and was open from July 1 to August 25, 2020. The survey was anonymous, and no data were collected that linked participants to recruitment sources. The (University of Haifa) University institutional review board (IRB) approved all procedures and instruments.Clicking on the link to the survey guided potential respondents to a page that provided information about the purpose of the study, the nature of the questions, and a consent form (i.e., the survey was voluntary; respondents could skip any questions or quit at any time; responses would be anonymous). The first page also offered researcher contact information and details of mental health crisis centers, should participants feel distress and the need for mental health assistance. Each participant was given the opportunity to take part in a lottery that included 10 gift vouchers of 50 USD each. A total of 451 women and three men participated in the study. Three men who answered the survey were removed from the exploratory factor analysis (EFA). The average age of the participants was 29.04 years (SD = 8.78), with an age range of 18 to 69. The vast majority of women were Jewish (93.1%, n = 420) and non-religious (73.2%, n = 330). More than half of the sample (54.6%) held a university degree, and the rest had completed high school (34.8%), had received various recognized educational/vocational certificates (10.2%), or had not finished high school (0.9%). The vast majority of women (83.3%, n = 378) reported being in a relationship. Of them, 312 (69.2%) reported being in their relationship for over a year, and 65 (14.4%) reported being in their relationship for less than a year. The majority of the sample, 73.4% (n = 331), identified as heterosexual, and the rest identified as bisexual (19.1%, n = 86), lesbian (3.8%, n = 17), or other (3.8%, n = 17). Finally, of the current sample, 51.2% (n = 231) reported being sexually abused during childhood (when they were under the age of 18).
Measures
Background variables included a brief demographic questionnaire that assessed gender, age, education, religion, religiosity, relational status, and sexual orientation.
Sexual-related PTSS were assessed using the Post-Traumatic Sexuality (PT-SEX) scale which was developed to measure traumatic reactions experienced during sex. Items from the current study were developed based on consultations with clinical experts, and based on gaps in the literature. Toward developing the scale, the systematic reviews were conducted to identify gaps in the literature (Gewirtz-Meydan, 2020; Gewirtz-Meydan & Opuda, 2021, 2022). Based on the literature, the reviews, and their own clinical experience in trauma and sex therapy, the authors have generated a pool of 43 items. Four clinical experts who specialize in trauma and childhood abuse, PTSD, and sexuality, assisted with developing the initial pool of items and suggested another 17 items. The initial pool consisted of 60 items. These experts were also encouraged to offer modifications in the wording of the items developed by the authors, and to make note of any items they felt were missing, or of any redundancies. To assess the clarity of the questionnaire for laypeople, the scale was also presented to three individuals (university students with whom the principal investigators were acquainted via their social networks) who were not familiar with trauma research in general or with this research study in particular. These individuals were asked to read the items and to indicate any item whose meaning was unclear. As a result of these procedures, minor modifications were made in the wording of the items, and 14 items were omitted due to redundancy. The final version of the questionnaire included a total of 46 items. Participants were presented with the list of manifestations and items and were asked to indicate to what extent they experienced a specific reaction during sexual activity in the past 6 months on a scale from 1 (not at all) to 5 (very much).
CSA was measured using the sexual abuse subscale of the Childhood Trauma Questionnaire (CTQ-SA; Bernstein et al., 2003). The CTQ is a 28-item scale developed to assess childhood physical, sexual, and emotional abuse, as well as physical and emotional neglect. Responses to questions beginning “When you were growing up. . .” were reported on a 5-point Likert type scale, with higher numbers indicating greater perceived CSA severity. In the current study, participants were classified as having a history of CSA, if their score on the CTQ-SA (Bernstein et al., 2003) was higher than the cutoff of 6 suggested by Tietjen et al. (2010). Cronbach’s alpha for the CTQ-SA subscale in the current study was good (α = .87).
Data analysis
Study 1 was designed to create the final format of the PT-SEX questionnaire and assess its construct. First, we performed the Velicer’s minimum average partial (MAP; using the MAP R package and function, with a squared and fourth power smallest average), parallel analysis (using the psych R package and fa.parallel function), and comparison data (using the RGenData R package and EFACompData function) tests to estimate the optimal number of factors in the initial format of the questionnaire, which comprised 46 items. Following these tests, we conducted an exploratory factor analysis (EFA) with minimum residual estimation and Promax rotation (by the fa function in the psych package) and number of factors based on the previous tests. Items with low loadings (<0.3) and/or high loadings on multiple factors (>0.3) were removed to obtain the final format of the questionnaire, after which the EFA was repeated on the final format. Lastly, we calculated McDonald’s ω estimates to explore whether in addition to the factors of the questionnaire, a general second-order factor was hidden (by the omega function in the psych package), which theoretically is the general concept of PT-SEX scale.
Results
There was unanimous agreement among the MAP (squared and fourth), parallel analysis, and comparison data tests that six factors ought to be retained (see Supplemental Figure 1 for the parallel analysis scree plot and the comparison data results). The initial EFA corroborated the suggested construct validity of the questionnaire and produced adequate-to-poor fit measures—degrees of freedom corrected root mean square of the residuals (RMSR) of 0.04, root mean square error of approximation (RMSEA) of 0.065 (90% confidence interval [CI] [0.061, 0.07]), and Tucker-Lewis index (TLI) of factoring reliability of .85 (Bayesian Information Criterion (BIC) = 2,675.96).Next, we omitted items with low loading on all six factors (n = 7) and items with high loading on multiple factors (n = 14) and reached a 25-item PT-SEX questionnaire. The EFA was repeated on the 25 items, which revealed better and adequate fit indices: RMSR = 0.03, RMSEA = 0.061 (90% CI [0.051, 0.072]), TLI = .93, BIC = 0.590.29. Item loadings are presented in Table 1. In addition, McDonald’s ω indicated that a general factor (i.e., second order) resided above the six PT-SEX factors (Hierarchical ω = .75; see Supplemental Figure 2). Exploring the content of the items in each factor indicated that the 25-item PT-SEX questionnaire comprised the following factors: dissociation (seven items; e.g., “I feel like my body is having sex, but I’m not really there”); intrusiveness (five items; e.g., “The touch of my partner reminds me of the perpetrator or the traumatic experience”); shame and guilt (five items; e.g., “I feel guilty when I am sexually aroused”); pleasing the other (four items; e.g., “I feel obligated to have sex with my partner”); interpersonal distress (two items; e.g., “I feel like I am scared of my partner during sex”); and hypervigilance (two items; e.g., “During sex, I need my partner to always tell me what is going to happen next”).
EFA Item Loadings Followed by Cronbach’s αs (Study 1) of the 25-item PT-SEX Scale.
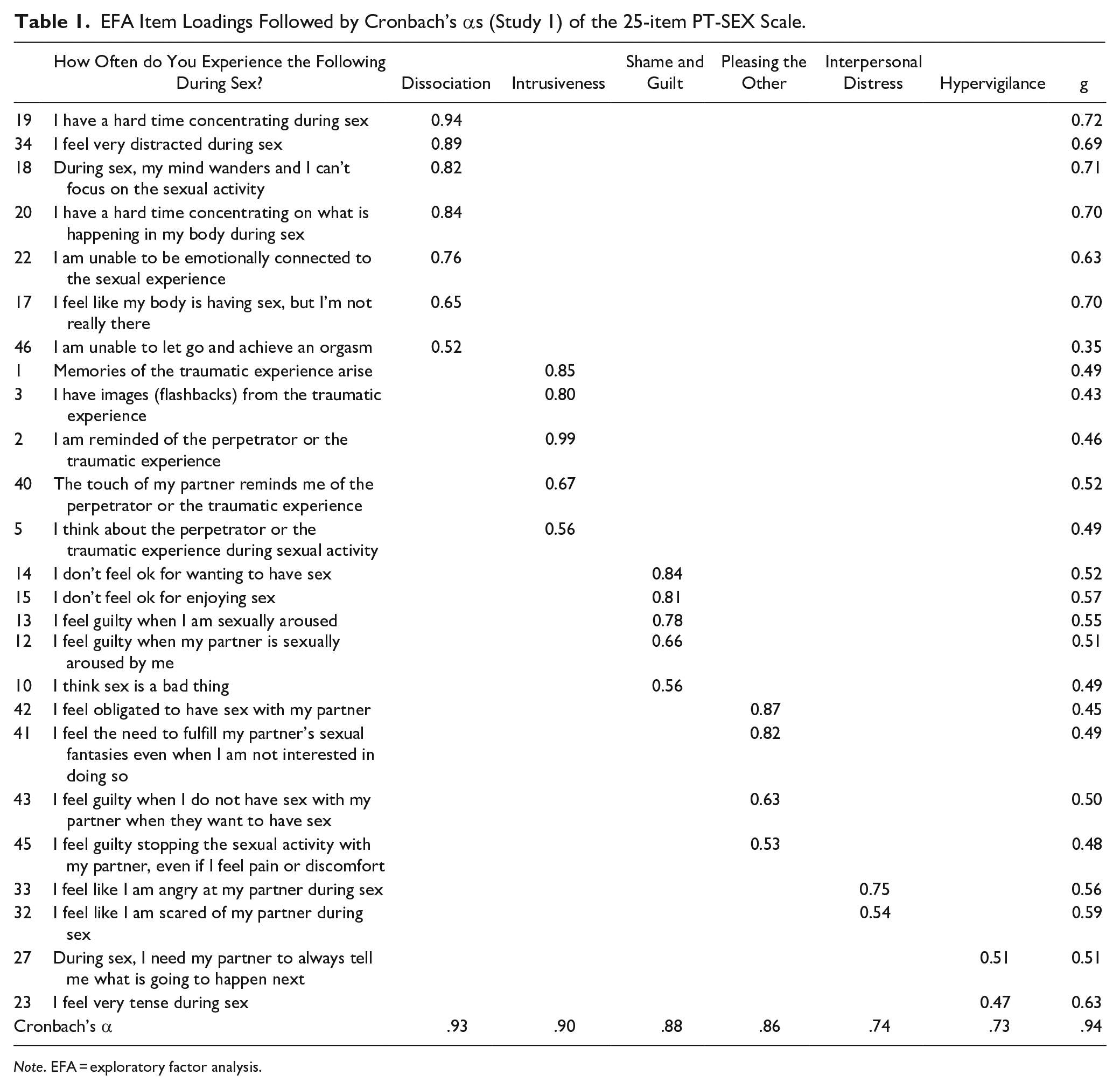
Note. EFA = exploratory factor analysis.
Study 2
In Study 2 we examined whether sexual-related PTSS (as measured by the PT-SEX scale) made a unique and unshared contribution (beyond PTSD symptoms) to survivors’ sexual esteem, compulsive sexual behaviors, sexual motives, and mental health (anxiety and depression).
Method
Participants and procedure
We conducted an online survey of a convenience sample of women. Participants were recruited via social media (using Facebook and Instagram). The survey was accessible through Qualtrics, a secure web-based survey data collection system. The survey took 25 minutes to complete, on average, and was open from November 2020 to August 1, 2021. The survey was anonymous, and no data were collected that linked participants to recruitment sources. The University of (masked for review) IRB approved all procedures and instruments. Clicking on the link to the survey guided potential respondents to a page that provided information about the purpose of the study, the nature of the questions, and a consent form (i.e., the survey was voluntary; respondents could skip any questions or quit at any time; responses would be anonymous). The first page also offered researcher contact information. In this study, no incentives were offered.
A total of 330 individuals participated in the study. Of them, 98 reported having experienced CSA, and 232 did not report such abuse. In the group of survivors of CSA, the vast majority were women (94%, n = 92), with a mean age of 26 (SD = 6.19). A little more than half (55%, n = 54) reported being married, and the rest were either single (33.1%, n = 32), divorced (11%, n = 11), or widowed (1%, n = 1). About half (55%, n = 53) completed a high school degree, and another 46% (n = 45) had a higher education degree. In terms of religion, respondents identified as Jewish (65%, n = 64), Muslim (27%, n = 26), or other (8.2%, n = 8). The majority reported being non-religious (63%, n = 62). For most of the survivors (62%, n = 60), the abuse occurred only once, whereas 38% (n = 36) reported that the abuse happened more than one time. The average age at onset of abuse was 12 (SD = 8). As for the group with no history of CSA, the majority were women (69%, n = 160), with a mean age of 35 (SD = 10.30). More than half (64%, n = 148) reported being married, and the rest were either single (25.3%, n = 58), divorced (11%, n = 25), or widowed (0.4%, n = 1). Among this group, the vast majority (70%, n = 160) held a higher education degree. In terms of religion, respondents identified as Jewish (52%, n = 119), Muslim (40%, n = 91), or other (7.9%, n = 18). The majority reported being non-religious (54%, n = 125). Sample size was determined by a power analysis to detect significant interaction in regression-based analyses—the main analysis in Study 2—using interactionPoweR R package. Effect size of all paths was set to β = .17 to allow the detection of small-to-moderate effects. The current sample allows a power of 88.2%.
Measures
Background variables included a brief demographic questionnaire that assessed gender, age, education, and relational status.
Sexual-related PTSS were assessed using the PT-SEX scale, previously described in Study 1.
CSA was measured using the sexual abuse CTQ-SA (Bernstein et al., 2003), previously described in Study 1. Cronbach’s alpha for the CTQ-SA subscale in the current study was good (α = .87).
PTSD symptoms were measured via the PTSD Checklist (PCL-5) for the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) (Weathers et al., 2013). The PCL-5 is a 20-item self-report measure that evaluates the degree to which individuals have been bothered in the past month by DSM-5 PTSD symptoms related to their most distressing event from the past. Items are rated from 0 (not at all) to 4 (extremely) and are summed for a total severity score (ranging from 0 to 80). Cronbach’s alpha for the PCL-5 total score in the current study was excellent (α = .96).
Sexual esteem was measured using the sexual esteem subscales of the Multi-dimensional Sexuality Questionnaire (MSQ; Snell et al., 1993) to assess participants’ sexual self-esteem (e.g., “I am confident about myself as a sexual partner”). The subscale is composed of five items, each rated on a 5-point scale ranging from 0 (not at all characteristic of me) to 4 (very characteristic of me). The items within the subscale are summed, with higher scores indicating greater sexual self-esteem. Snell et al. (1993) demonstrated the factorial validity of the MSQ subscales and found them not to be contaminated by social desirability biases. In the current study, internal consistency for the subscale was high (0.93).
Sexual dysfunction was measured by the Female Sexual Function Index (FSFI) (Katz & Marshall, 2003) and the International Index of Erectile Function (IIEF) (Rosen et al., 1997). The FSFI questionnaire includes 19 items to evaluate female sexual function, comprising six domains: sexual arousal, sexual desire, satisfaction, lubrication, orgasm, and pain during sexual activity in women. The answers to four of the questions are assigned 1 to 5 points, and the answers to the remaining 14 questions, 0 to 5 points. Additionally, each domain has its own impact on the calculation of the final score. The total FSFI score ranges between 2 and 36, with higher scores indicating better female sexual function. In the current study, internal consistency for the scale was excellent (0.94). The IIEF includes 15 items to evaluate men’s sexual functioning over the previous 4 weeks in five domains: erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction. Summed total scores range from 5 to 75, with higher scores indicating better sexual function. Cronbach’s alpha for the current sample was good (.80).
Compulsive sexual behavior disorder (CSBD) was assessed using the CSBD-19 (Bőthe et al., 2020). The CSBD-19 is a self-report measure that evaluates and assesses participants’ sexual compulsivity (e.g., “Even though my sexual behavior was irresponsible or reckless, I found it difficult to stop”). The scale is composed of 19 items, each rated on a 4-point scale ranging from 0 (totally disagree) to 4 (totally agree). The items within the scale are summed, with higher scores indicating higher levels of compulsive sexual behavior. Bőthe et al. (2020) demonstrated high reliability and validity of the CSBD-19 total score and subscales. In the current study we used the total score of the CSBD-19 to assess participants’ compulsive sexual behavior and found the internal consistency for the scale to be high (0.92).
Sexual motives were assessed with the 29-item Sex Motives Scale (Cooper et al., 1998). Participants rate a series of reasons for having sex by indicating how often they have sex for each reason (1 = almost never/never to 5 = almost always/always). The measure consists of six subscales: (1) enhancement (e.g., having sex because it feels good), (2) intimacy (e.g., having sex to feel closer to partner), (3) self-affirmation (e.g., having sex to feel better about self), (4) coping (e.g., having sex to feel better when feeling low), (5) partner approval (e.g., having sex because partner will be angry if I don’t), and (6) peer pressure (e.g., having sex because friends are having sex). For the current sample, internal consistencies for the subscales were as follows: enhancement (α = .90), intimacy (α = .93), self-affirmation (α = .89), coping (α = .88), peer pressure (α = .88), and partner approval (α = .91). In the current sample, and given the nature of the sample (i.e., adults), the peer pressure measure had very small variance and extreme positive skewness given that 76.49% of the sample reported the lowest score (i.e., 1). Accordingly, we decided to refrain from using this facet of sexual motivations.
Relationship satisfaction was assessed using the Relationship Assessment Scale (RAS; Hendrick, 1988). The RAS is a seven-item measure of global relationship satisfaction. Responses are given on a 5-point Likert scale. Items are calculated by average scores ranging from 1 to 5 with higher scores indicating greater relationship satisfaction. Cronbach’s alpha in our study was .85.
Depression and anxiety were assessed using the short version of the Brief Symptom Inventory (BSI-18; Derogatis & Melisaratos, 2004), an 18-item scale used to assess a wide range of self-reported psychopathological symptoms. Individuals are asked to indicate on a 5-point Likert scale how often (0 = not at all to 4 = frequently) they had experienced a symptom within the past month. These items yield three subscales of psychological distress, including depression, anxiety, and somatization, as well as a global BSI score computed by averaging all 18 items. The BSI-18 has shown very good reliability and validity for the assessment of psychological distress (Franke et al., 2017). In this sample, Cronbach’s alpha for the depression scale was .88, and it was .90 for anxiety.
Data analysis
The study comprised 330 participants, with 98 of them reporting having experienced CSA and 232 of them not reporting CSA. Prior to the main analyses, we examined the normal distribution of all main study measures using a series of Shapiro-Wilk normality tests, the presence of univariate outliers using the robust median absolute deviation (Routliers R package), and of multivariate outliers using the Minimum Covariance Determinant approach (Routliers R package). Given that skewed distributions were detected (as commonly happens in clinical data) as well as multiple outliers, all analyses were robust analyses. Specifically, we examined whether participants with a history of CSA as compared with those without such a history had different levels of PTSD and sexual-related PTSS, and therefore we conducted Yuen’s trimmed mean t-tests for independent samples. To examine whether the groups differed in sexual-related PTSS clusters, we conducted semi-parametric multivariable analyses of variance (MANOVA) with the wild bootstrap approach (1,000 resampling cycles) and Rademacher weights followed by Yuen’s trimmed mean t-tests for independent samples. Next, we examined whether sexual-related PTSS predicted participants’ sexual self-esteem, sexual functioning, sexual motives (self-affirmation, intimacy, enhancement, coping, and partner approval), relationship satisfaction, CSBD, depression and anxiety, above and beyond the contribution of PTSD. We also examined whether the associations between sexual-related PTSS, PTSD, and sexual-related measures were moderated by participants’ history of CSA. To do so, we conducted a series of hierarchical robust regressions (using the rlm function of the MASS R package) with the MM-estimator. In the first step of the models, we introduced participants’ PTSD, sexual-related PTSS, and CSA (yes, no) as predictors. In the second step of the models, we added the interactions between PTSD and sexual-related PTSS on the one hand, and CSA on the other hand. To avoid multicollinearity, all measures were centered around the sample mean (apart from CSA, which was dummy coded, 1 = yes and 0 = no). Significant interactions were probed by simple slopes tests using the interactions R package.
Results
Differences in PTSD and sexual-related PTSS
Means, standard deviations, and Yuen’s trimmed t-statistics are presented in Table 2 and Figures 1 and 2. The analyses of the overall PTSD and sexual-related PTSS levels indicated that participants with a history of CSA had significantly higher PTSD and sexual-related PTSS as compared with participants without such a history. Based on the confidence intervals of the effect sizes, the analyses also revealed that the magnitude of differences in PTSD was stronger than the magnitude of differences in sexual-related PTSS. Exploring in more depth the differences in sexual-related PTSS, the semi-parametric MANOVA revealed a difference in the multivariate factor of the sexual-related PTSS clusters, modified ANOVA-Type Statistic (MATS) = 62.55, pwildBS < .001. Univariate Yuen’s trimmed t-tests indicated that whereas participants with a history of CSA had significantly higher dissociation, intrusiveness, pleasing the other, and hypervigilance than did participants without such a history, the sensations of shame and guilt as well as interpersonal distress were not significantly different.
Means, Standard Deviations, Yuen’s Robust t-Statistics and Effect Sizes for Differences Between Participants With a History of Child Sexual Abuse and Those Without Such a History, in PTSD, Sexual-Related PTSS, and Sexual-Related PTSS Clusters.
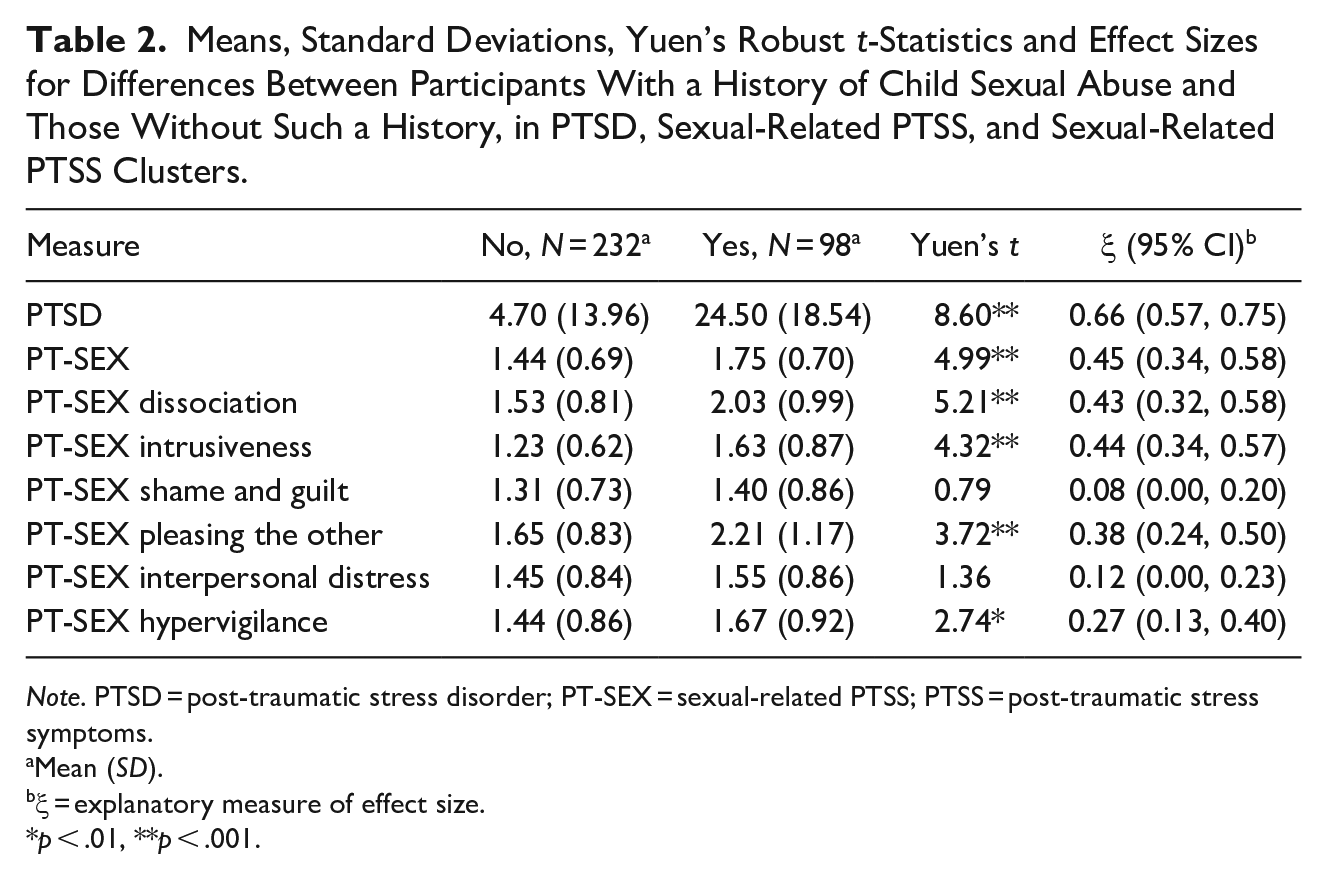
Note. PTSD = post-traumatic stress disorder; PT-SEX = sexual-related PTSS; PTSS = post-traumatic stress symptoms.
Mean (SD).
ξ = explanatory measure of effect size.
p < .01, **p < .001.
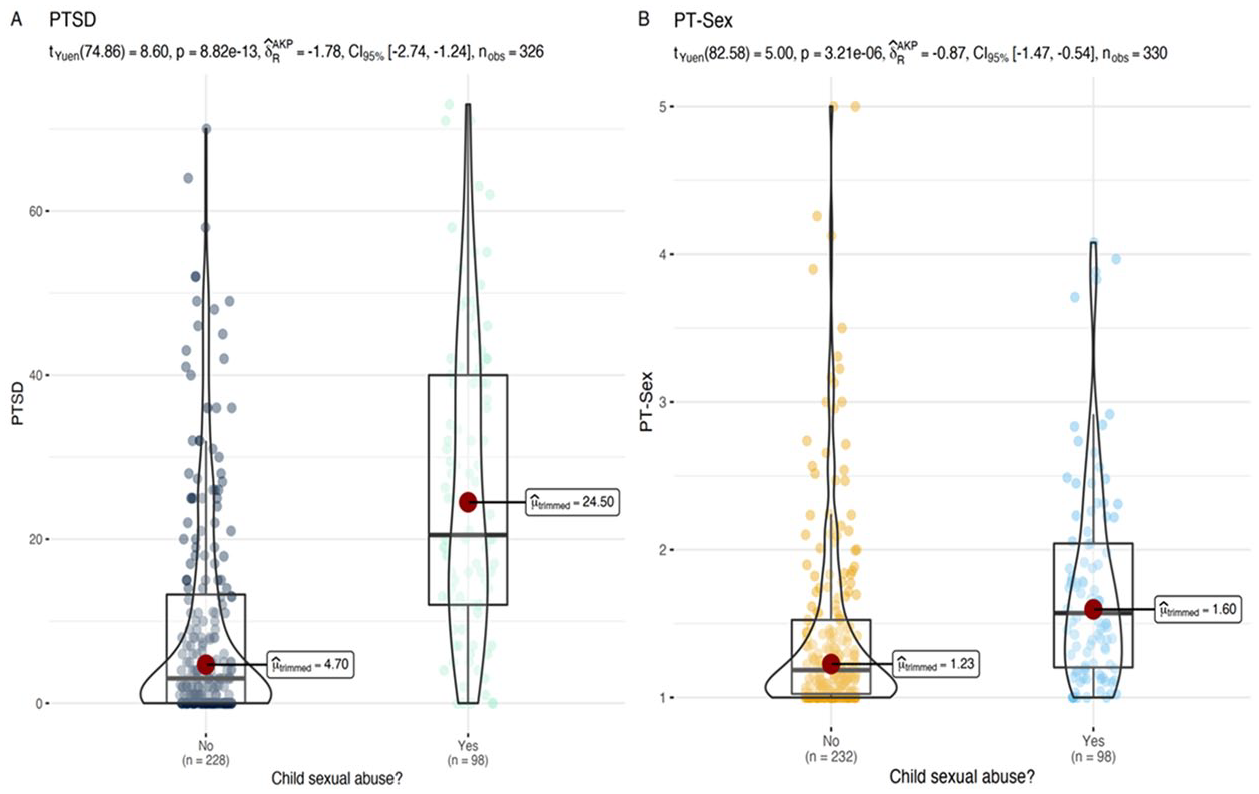
Differences in PTSD: (a) and sexual-related PTSS and (b) between participants with and without a history of child sexual abuse.
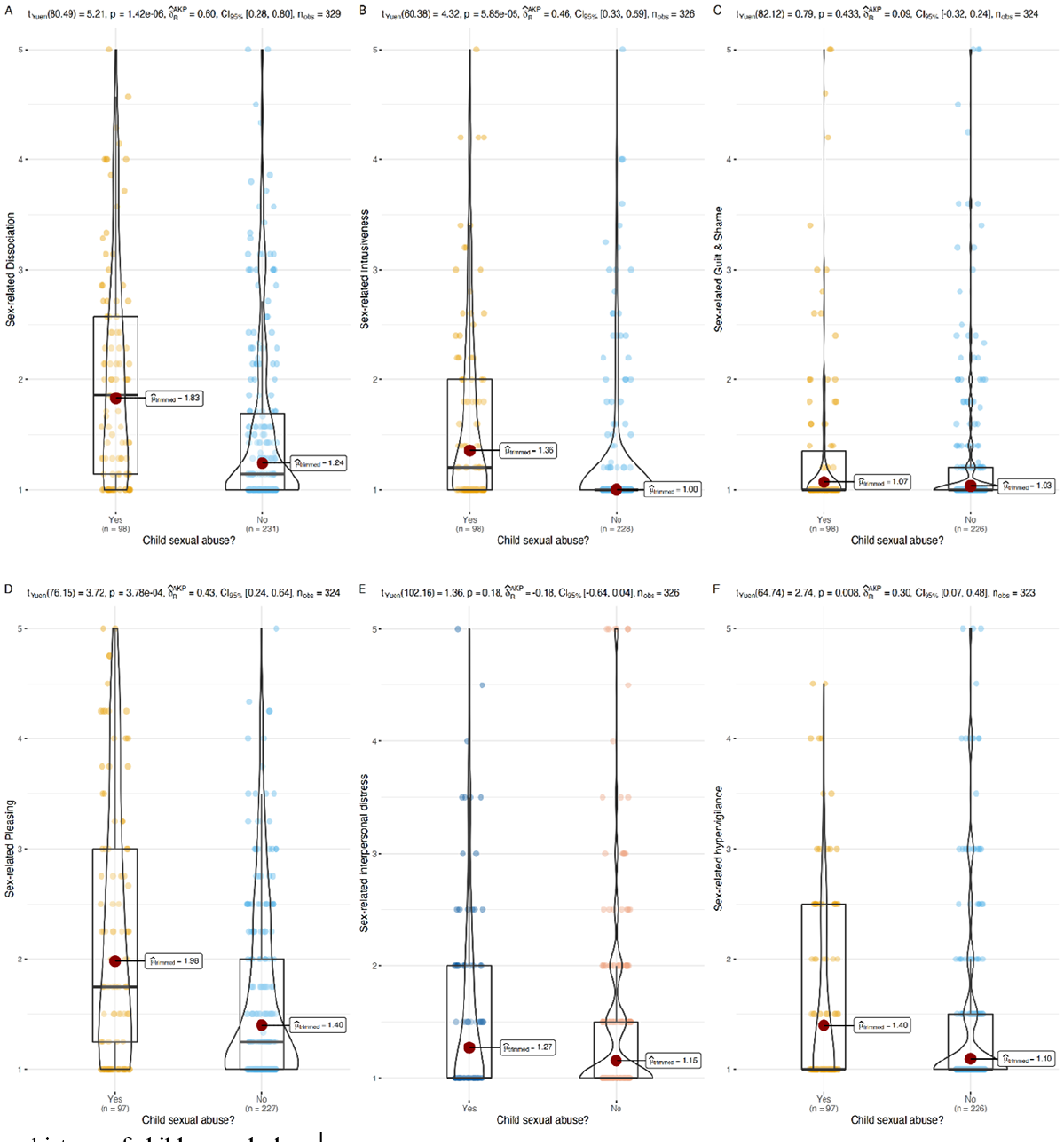
Differences in sexual-related PTSS clusters between participants with and without a history of child sexual abuse.
Effects of PTSD and sexual-related PTSS
Reported effects of PTSD and sexual-related PTSS were taken from the first step of the models (i.e., before the interactions were introduced into the models). Regarding most of the outcomes, PTSD and sexual-related PTSS made unique and unshared contributions to the observed data. Specifically, higher PTSD and/or sexual-related PTSS were associated with having sex for the purpose of self-affirmation and coping; with lower relationship satisfaction; and with higher CSBD and depression. Sexual-related PTSS, but not PTSD, was also linked with lower sexual self-esteem and having sex for reasons of partner approval. PTSD, but not sexual-related PTSS, was associated with having sex for reasons of intimacy and enhancement, and with higher anxiety.
The moderating role of CSA
As presented in Figure 3, CSA significantly moderated the associations between sexual-related PTSS on the one hand, and sexual self-esteem (A), sexual motivations of self-affirmation (B) and coping (C), depression (D), and anxiety (E), on the other. We did not find that CSA moderated the association between sexual-related PTSS and sexual functioning, however, differences in sexual functioning were indeed found. Simple slopes tests indicated that among participants with a history of CSA, sexual-related PTSS was associated in a significantly stronger fashion with lower sexual self-esteem (b = −0.71, SE = 0.18, t = −3.88, p = .00013), and greater motivations (i.e., for having sex) of coping (b = 0.67, SE = 0.13, t = 5.19, p < .00001), as compared with participants without a history of CSA (b = −0.31, SE = 0.12, t = −2.64, p = .0086 for sexual self-esteem, and b = 0.27, SE = 0.08, t = 3.31, p = .001 for the sexual motivation of coping). In addition, the tests revealed that whereas sexual-related PTSS was associated with a greater sexual motivation of self-affirmation (b = 0.45, SE = 0.17, t = 2.71, p = .007), depression (b = 0.53, SE = 0.12, t = 4.56, p < .00001), and anxiety (b = 0.32, SE = 0.12, t = 2.62, p = .009) among participants with a history of CSA, sexual-related PTSS was not significantly linked with these measures among those without a history of CSA (b = 0.15, SE = 0.12, t = 1.20, p = .23 for the sexual motivation of self-affirmation, b = 0.06, SE = 0.08, t = 0.77, p = .44 for depression, and b = 0.02, SE = 0.08, t = 0.21, p = .84 for anxiety).
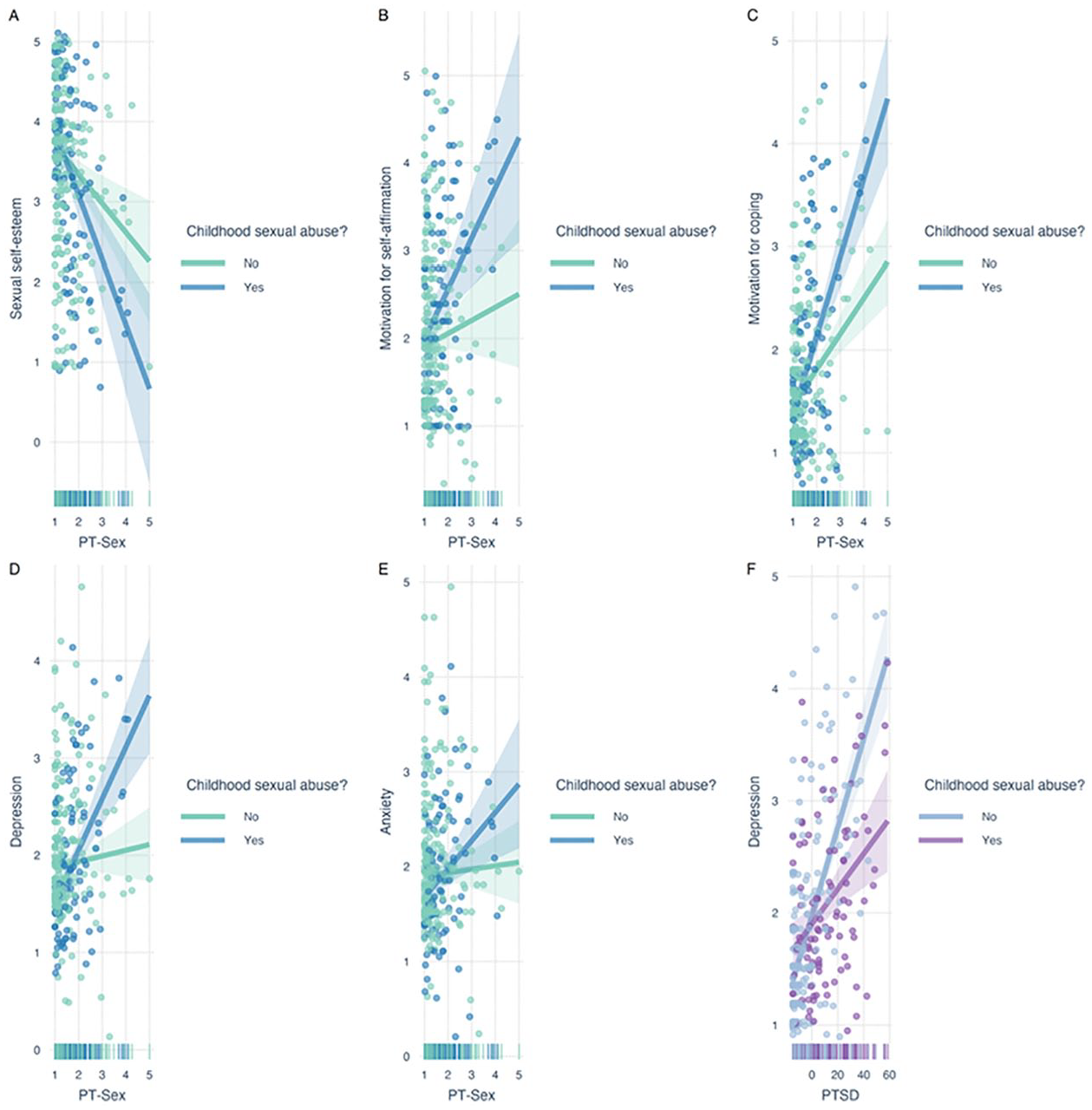
Simple slopes results presenting the moderating role of child sexual abuse regarding the links between sexual-related PTSS and sexual self-esteem (a), self-affirmation (b), coping (c) sexual motivations, depression (d), and anxiety (e). This figure also presents the moderating role of child sexual abuse regarding the links between PTSD and depression (f). Bands refer to 95% confidence intervals of the regression lines. Bottom vertical lines refer to rug plots indicating the distribution of participants’ PT-SEX or PTSD.
Finally, the models also revealed that CSA moderated the effect of PTSD on depression. Unexpectedly, PTSD was more strongly associated with depression among participants without a history of CSA, b = 0.79, SE = 0.07, t = 11.29, p < .00001, than among those with such a history, b = 0.31, SE = 0.09, t = 3.55, p = .0005.
Discussion
Despite the well-established association between CSA and sexual difficulties in adulthood (Bigras et al., 2021; Gewirtz-Meydan & Opuda, 2020; Pulverman et al., 2018; Slavin et al., 2020), there is a limited amount of research on how symptoms of PTSD interplay within this association. To date, researchers on sexuality among CSA survivors have examined the moderating or mediating role of PTSD in the relation between abuse history and adult sexuality (e.g., Bornefeld-Ettmann et al., 2018; Gewirtz-Meydan & Lahav, 2020). Currently, the sexuality of CSA survivors is measured independently of the trauma by examining the relationship between sexual dysfunction and trauma-related variables. However, there is a growing understanding that the trauma of CSA survivors is not only related to their sexual function but it is also manifested in their minds and bodily experiences during sexual interactions (Kratzer et al., 2022). The importance and need for the PT-SEX scale is, therefore, clear.
The PT-SEX scale may serve as a useful tool in exploring sexual-related PTSS among adult survivors of child abuse. The current findings yielded six PT-SEX scale factors: dissociation during sex, intrusiveness during sex, shame and guilt in regard to sexual aspects, pleasing the other during sex, interpersonal distress, and hypervigilance during sex. These subscales correspond with findings of previous studies indicating that CSA survivors often experience dissociation (Bird et al., 2014; Hansen et al., 2012), sexual-related shame and guilt (Pulverman & Meston, 2019), and hypervigilance (Lorenz et al., 2012, 2015; Meston & Lorenz, 2013; Rellini & Meston, 2006) during sexual activity. Survivors of CSA who report high levels of dissociation in particular often engage in sex to gain their partners’ approval (Gewirtz-Meydan & Lahav, 2020). As for interpersonal distress, research on this aspect is scarce. However, the literature suggests that CSA can affect the way survivors view the other and their role in the relationship. As a result of the abuse, the other is often seen by the survivor as dangerous, untrustworthy, unavailable, abusive, unresponsive, insensitive, exploitative, and not dependable (Gewirtz-Meydan & Ofir-Lavee, 2020). This is especially true when the abuse was carried out by a significant person in the child’s life (who was supposed to have protected the child), or when other significant people in the child’s life failed to identify or prevent the abuse, or were reluctant to help the child and stop the abuse. These perceptions of the other may be carried into adult sexual relationships and can be projected onto current sexual partners, and survivors might even confuse their current partners with their abusers (Hughes, 1994). Eventually, these representations of the other may prevent survivors from feeling safe and loved in their relationships, from allowing themselves to be vulnerable and emotionally intimate with their partners, and from being open about their emotional and sexual needs, all of which are essential elements in developing healthy intimacy.
The PT-SEX scale showed good internal consistency in its six factors. In line with the theoretical literature, levels of sexual-related PTSS, as measured by the PT-SEX scale, were higher among participants who had a history of child abuse than they were among non-abused participants. This finding is in line with findings from previous studies in the fields of CSA, trauma symptoms, and sexual difficulties (e.g., Bird et al., 2014; Gewirtz-Meydan & Lahav, 2020; Hansen et al., 2012; Kratzer et al., 2020; Lorenz et al., 2012, 2015; Meston & Lorenz, 2013; Pulverman & Meston, 2019; Rellini & Meston, 2006). As for the specific factors, participants with a history of CSA had significantly higher levels of dissociation, intrusiveness, pleasing the other, and hypervigilance than did participants without such a history.
The current findings indicated that PTSD and sexual-related PTSS made unique and unshared contributions to survivors’ sexual esteem, sexual compulsivity, relationship satisfaction, and overall depression. In addition, sexual-related PTSS also made a unique and unshared contribution to survivors’ engagement in sex for reasons of self-affirmation and coping with negative feelings. This finding challenges the view of how to treat sexual difficulties of CSA survivors. Namely, the sexual difficulties of CSA survivors are often considered to be one aspect of many psychopathologies related to the abuse (e.g., depression, PTSD, sleep disorders) that will resolve on their own once the trauma of the sexual abuse is treated. However, a meta-analysis suggest that psychological treatment for PTSD may not have a significant and comprehensive effect on sexual difficulties (O’Driscoll & Flanagan, 2016). Given that only four studies were included in this meta-analysis, there is a need for further examination of the efficacy of clinical intervention to treat sexual dysfunction and other sexual-related difficulties among survivors of CSA (Gewirtz-Meydan, 2020). In an intervention carried out by Classen et al. (2001), present-focused group therapy and trauma-focused group therapy improved survivors’ traumatic symptoms, but neither intervention reduced survivors’ engagement in risky sexual behaviors. Researchers and clinicians have suggested that actively targeting and addressing sexual difficulties is more effective (i.e., than broadly targeting trauma) for survivors (Kristensen & Lau, 2013; Maltz, 2002; Meston et al., 2013).
Limitations and Future Studies
The results of the present study should be considered in light of its limitations. First, this study was based on self-report measures which may have been subject to response biases and shared method variances. Future studies should examine the validity of the PT-SEX scale among clinical samples and possibly also among participants who experienced different types of traumas (with proper adaptation of the wording). Also, as our samples were mostly based on non-religious Jewish women, PT-SEX should also be validated among more diverse samples. Second, the present study did not encompass the entire spectrum of psychopathology that CSA survivors encounter in their adult lives. Future research should examine the explained variance of sexual-related PTSS in other mental health conditions such as somatization, eating disorders, and suicidal ideation. In addition, further investigation is needed to examine the effect of sexual-related PTSS on other sexual-related measures, such as sexual distress, sexual assertiveness, sexual fantasies, and engagement in risky sexual behaviors. Third, while we examined PTSD levels, we did not account for other adversities and traumas which can also account for high levels of PTSD. We did not have information concerning sexual activity in past 6 months, and future research should account for different sexual activities as well (including both sole and partnered sexual activities). Fourth, the possible implications of using convenience sampling should be taken into account. Furthermore, there was an overrepresentation of women (vs. men) in the present sample. These factors limit the generalizability of the study and point to the need to explore the phenomenon of sexual-related PTSS among more diverse samples, and specifically among clinical samples of male and LGBTQI (lesbian, gay, bisexual, transgender, queer, intersex) survivors of CSA. Future research should examine the validity of the PT-SEX scale among men.
Theoretical and Clinical Contribution
Notwithstanding the limitations above, the present results indicate that the PT-SEX scale has good psychometric characteristics, supporting the feasibility of its use in measuring sexual-related PTSS. Prior to the development of the PT-SEX scale, there were no reliable or valid means of quantifying sexual-related PTSS. Sexual variables were mostly examined in relation to trauma variables (e.g., PTSD and dissociation) or other sexual variables (e.g., sexual shame, or sexual self-concepts).
The main clinical implication of the current study findings is that PTSD symptomatology are implicated within survivors’ sexual experiences. In other words, although sexual difficulties among survivors of CSA appear to be similar to those of individuals who did not experience CSA, the source of these difficulties among CSA survivors may very well stem from the trauma, and may manifest as sexual-related PTSS (Gewirtz-Meydan & Ofir-Lavee, 2020).
Another main clinical implication of this study is that sexual-related PTSS (i.e., beyond symptoms of PTSD) makes a unique and distinct contribution to sexuality. Our study findings align with the findings of a meta-analysis suggesting that psychological treatment for PTSD may not have a significant and comprehensive effect on sexual difficulties (O’Driscoll & Flanagan, 2016). Some clinicians hold the assumption that sexual difficulties will resolve on their own if the trauma (of the SA) is treated. However, this study suggests that if sexual difficulties are accompanied by sexual-related PTSS, therapists may consider addressing these symptoms directly. Finally, assuming there is “post-traumatic sexuality” with unique sexual patterns in the aftermath of CSA, this may require the examination of innervations for treating sexual difficulties among survivors, as many of the original sex-therapy protocols did not include CSA survivors (Hall, 2017). Developing interventions that address the unique challenges of post-traumatic sexuality, such as mindfulness based therapy (Brotto et al., 2012) or expressive writing (Meston et al., 2013), instead, may be more effective in addressing the sexual difficulties that emerge as a result of CSA (Gewirtz-Meydan, 2020). Clinicians and sex therapists treating sexual difficulties following trauma should study the relationship between sexual difficulties and the different mechanisms in which the trauma can affect one’s sexual function, satisfaction, and wellbeing. It is also important that clinicians treating trauma survivors acquire appropriate knowledge on the various sexual difficulties. In the case of applying trauma therapy, sexual difficulties should be addressed, while in the case of applying sex therapy, sex therapy interventions should be modified to be more trauma-informed (Gewirtz-Meydan, 2020).
Supplemental Material
sj-docx-1-jiv-10.1177_08862605221118969 – Supplemental material for Sex in the Shadow of Child Sexual Abuse: The Development and Psychometric Evaluation of the Post-Traumatic Sexuality (PT-SEX) Scale
Supplemental material, sj-docx-1-jiv-10.1177_08862605221118969 for Sex in the Shadow of Child Sexual Abuse: The Development and Psychometric Evaluation of the Post-Traumatic Sexuality (PT-SEX) Scale by Ateret Gewirtz-Meydan and Dana Lassri in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We wish to thank the people who helped us develop the scale: Mili Lev, MSW and Certified couples and family therapist; Yael Sherer, Founder and Manager of Israel’s lobby against sexual violence.
Author’s note
Dr. Gewirtz Meydan is an affiliated researcher at The Crimes Against Children Research Center (CCRC), the Haruv Institute, and at the Interdisciplinary Research Centre on Intimate Relationship Problems and Sexual Abuse (CRIPCAS), and Dr. Lassri is affiliated researcher at the Research Department of Clinical, Educational and Health Psychology, UCL (University College London) and at Haruv Institute.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Supplemental Material
Supplemental material for this article is available online.
Authors Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.