
Abstract
Intimate partner violence (IPV) during pregnancy needs to be prevented because it leads to negative health outcomes for both the mother and offspring. However, it is not easy to detect women who suffer from IPV by health practitioners or public health staff due to stigma attached to it or hesitation of the women to disclose it. The aim of this study is to develop a scale using pregnancy registration records to detect IPV during pregnancy. We used administrative data of pregnancy registration records of Adachi City, Tokyo, in the 2016 fiscal year (N = 5,990). IPV was assessed at the first interview or another opportunity for further assessment by a public health nurse. The data include registration information, demographics, health and perinatal status, and social environment. Multiple logistic regression model was used to predict IPV. IPV cases were found for 24 (0.4%) cases. Subsequent child (odds ratio [OR]: 3.45, 95% confidence interval [CI] [1.02–11.6]), single marital status (OR: 7.96, 95% CI [2.88–22.2]), thinness (OR: 3.17, 95% CI [1.13–8.90]), past pregnancy of four or more times (OR: 5.25, 95% CI [1.35–20.4]), having trouble with family member (OR: 5.45, 95% CI [1.95, 15.2]), and poverty (OR: 6.27, 95% CI [2.25–17.5]) showed significant association with IPV. These variables detected IPV with good predictive power (area under receiver operating characteristic curve = 0.89, 95% CI [0.81–0.98]). We showed strong detectability of IPV during pregnancy using a scale based on pregnancy registration records in which IPV was not asked directly. The current study is useful to detect IPV during pregnancy and prevent further adverse health outcomes due to IPV during pregnancy.
Introduction
Intimate partner violence (IPV) is a major problem worldwide. It was estimated that the lifetime prevalence of physical or sexual IPV among partnered women was 29.8% in the United States, 25.4% in Europe, and 23.2% in high-income regions (World Health Organization, 2012). Further, the total cost of IPV, including women’s physical and mental health, was estimated to be more than USD 5.8 billion (World Health Organization, 2013). Specifically, a focus on IPV during pregnancy should be placed because it leads to negative health outcomes such as maternal suicide, maternal alcohol abuse and smoking (Bailey & Daugherty, 2007; Taggart & Mattson, 1996), postpartum depression (Johri et al., 2011), and also low birth weight (Campbell, 2002) and miscarriage (Silverman et al., 2006).
In Japan, the prevalence of IPV during pregnancy is increasing (World Health Organization, 2011), although it is estimated that prevalence of physical IPV during pregnancy in the country is low (approximately 1%) (Miura & Fujiwara, 2017). As the prevalence of physical IPV among women was estimated as 19.8% in 2017 based on the survey conducted by the Japan Cabinet Office (Gender Equality Bureau Cabinet Office, 2020), the prevalence of IPV during pregnancy might be lower than the other life stages. However, we postulated that this prevalence must be underestimated because Japanese women are less likely to report IPV due to feelings of shame (Gender Equality Bureau Cabinet Office, 2016b). Thus, we believe there is a need to develop a scale using existing data to detect IPV during pregnancy.
In Japan, all pregnant women have to submit a pregnancy notification form to their local government office during early pregnancy based on the Mother–Child Law, and public health nurses collect data on IPV during pregnancy (Fujiwara et al., 2021). Thus, it is feasible to detect IPV during pregnancy based on municipal pregnancy registration data.
Previously, the 10-item Intimate Partner Violence during Pregnancy Instrument (IPVPI) was developed using an anonymous questionnaire on IPV during pregnancy combined with demographic and psychosocial characteristics at 3 to 4 month health checkup, and it found moderate discriminating power (area under the curve [AUC] = 0.719, 95% CI [0.698–0.740]) (Doi et al., 2019). However, the IPVPI is developed using recalled IPV status during pregnancy as an outcome, which was retrospectively assessed at the time of 3 to 4 months health checkup, that is, after delivery; thus, outcome may be inaccurate due to both stigma and recall bias. Further, in Japan, it is difficult to prepare the system at municipality to capture IPV among pregnant women because of shortage of trained public health nurses who can assess IPV status adequately, and to prepare a safe environment where pregnant women can disclose their IPV without being hindered by a lack of space. Thus, public health nurses working in municipalities assessed IPV status among pregnant women through multidisciplinary networks, including obstetric hospitals or public women’s counseling centers. Therefore, it is necessary to develop an updated scale using administrative data on demographic and psychosocial information at the time of pregnancy, as well as data on IPV during pregnancy collected by municipalities in a longitudinal design. By using the developed scale, public health nurses may be able to detect IPV during pregnancy without directly asking about violence and provide adequate support for new mothers who suffer from IPV from their pregnancy period, such as psychological care, introduction of lawyer, or IPV shelter.
The aim of this study is to develop a scale to identify risk of IPV during pregnancy using administrative data, for both pregnancy registration record and captured IPV, at municipality in Japan.
Methods
Data
We used all data from pregnancy registration records of Adachi City, Tokyo, in the 2016 fiscal year, from April 1, 2016 to March 31, 2017 (N = 5,990). Most mothers registered their pregnancy at municipalities during the first trimester. Among them, 35 mothers were registered twice due to abortion the first time, and then getting pregnant again within the same fiscal year. In addition, two mothers delivered twice within the same fiscal year. We included these cases because they can be a consequence of IPV. We took care of diversity by using all data in Adachi City, Tokyo.
Intimate Partner Violence
In Japan, women who are exposed to IPV are recommended to seek consultation at a public women’s center, via telephone or visit. Then, the information can be shared with public health nurses. Further, IPV status can be shared from obstetric hospitals to public health nurses to support the victimized women, until the expectant mother delivered. In other words, IPV status has not been screened using existing scales. IPV was defined as physical abuse, psychological abuse, and sexual abuse from spouses and partners in the Act on the Prevention of Spousal Violence and the Protection of Victims in Japan (Gender Equality Bureau Cabinet Office, 2016a), and IPV was captured only if victimized women consulted to a specific institution, such as public women’s counseling centers or obstetric hospitals. Therefore, the IPV status data collected by public health nurses can be considered as salient IPV cases that need support.
Variables in Pregnancy Registration Form
The pregnancy registration form in Adachi City included the following: registration information including date of registration (weekday or weekend); geographical location of health centers among the five centers in Adachi City; type of center where pregnancy record is submitted (included the city hall, public health center, or community center); and demographics including maternal age (calculated based on date of birth and date of registration) and parity. “Teenage pregnancy for first baby” was assessed based on the age of first children and maternal current age. As for marital status, if husband’s name was filled out, the case was considered as married, and if it was blank, the case was considered as unmarried. Further, for health and perinatal status, information including height and weight (for calculation of body mass index [BMI]), gestational week, drinking status during pregnancy (yes/no), having a smoker within family (yes/no), past medical history including mental disorder, and the woman’s feelings when her pregnancy was confirmed (“happy,” “unexpected but happy,” “unexpected and confused,” “did not know what to do,” or “no feelings”) was included. This variable was further collapsed as “distressed” (“did not know what to do” and “no feelings”), and “not distressed” (“happy” and “unexpected but happy”). Past pregnancy of four or more times was assessed based on frequency of parity and abortion. Multiple pregnancy status was coded if municipality issued a maternal and child health book multiple times. Social environment was also asked including health insurance (including public aid), social support (yes/no), trouble within family (yes/no), and subjective economic status (“stable,” “able to manage,” “difficult to manage,” or “unstable”).
Analysis
All pregnancy registrations submitted between April 1, 2016 and March 31, 2017 were analyzed (N = 5,990). Multiple logistic regression analysis was conducted to investigate the risk factors for IPV during pregnancy. First, crude association of each risk factor on IPV was examined by logistic regression analysis. Second, multiple logistic regression analysis including all variables was applied, which showed a significant association with IPV during pregnancy in the crude model. To create a formula that can predict IPV using the selected risk factors, odds ratios (ORs) from multiple logistic regression analysis were used for weighting the risk factors, following a previous study (Quan et al., 2011). The weighting system was carried out as follows: the score was not weighted when ORs ranged from 1.00 to 1.49; the score was doubled when ORs ranged from 1.50 to 2.49; and the score was tripled when ORs ranged from 2.50 to 3.49. Data were analyzed using STATA version 14.1 (StataCorp, 2015. College Station, TX, USA: StataCorp LP).
Results
Table 1 shows the characteristics of the sample. IPV cases were found in 24 (0.4%) cases. Most of the women registered their pregnancy on weekdays (98.2%) and none with IPV registered on weekends. Teenage pregnancy was minor (92 cases; 1.5%), and it was not found among women with IPV. As for parity, first and subsequent pregnancy were almost equally distributed. Single mother status was found in 12.8% of women, and was higher among women with IPV than women without (62.5% vs. 12.6%). As for health status, most women (69.4%) showed an appropriate BMI range (between 18.5 and less than 25). Women with mental illness accounted for 3.0%, which was higher among women with IPV (8.3%). The majority had a gestational age at registration of before 20 weeks (97.2%), and 6.9% reported feeling distressed, which was higher among women with IPV (25.0%). As for social factors, women without social support and having trouble with a family member accounted for 8.8% and 6.6%, respectively, and both factors were more prevalent among women with IPV (29.2% and 37.5%, respectively). Less than 10% of the women reported that their subjective socioeconomic status caused difficulties in daily survival; however, majority of the women with IPV (66.7%) reported experiencing difficulties in daily survival and stress.
Sample Distribution.
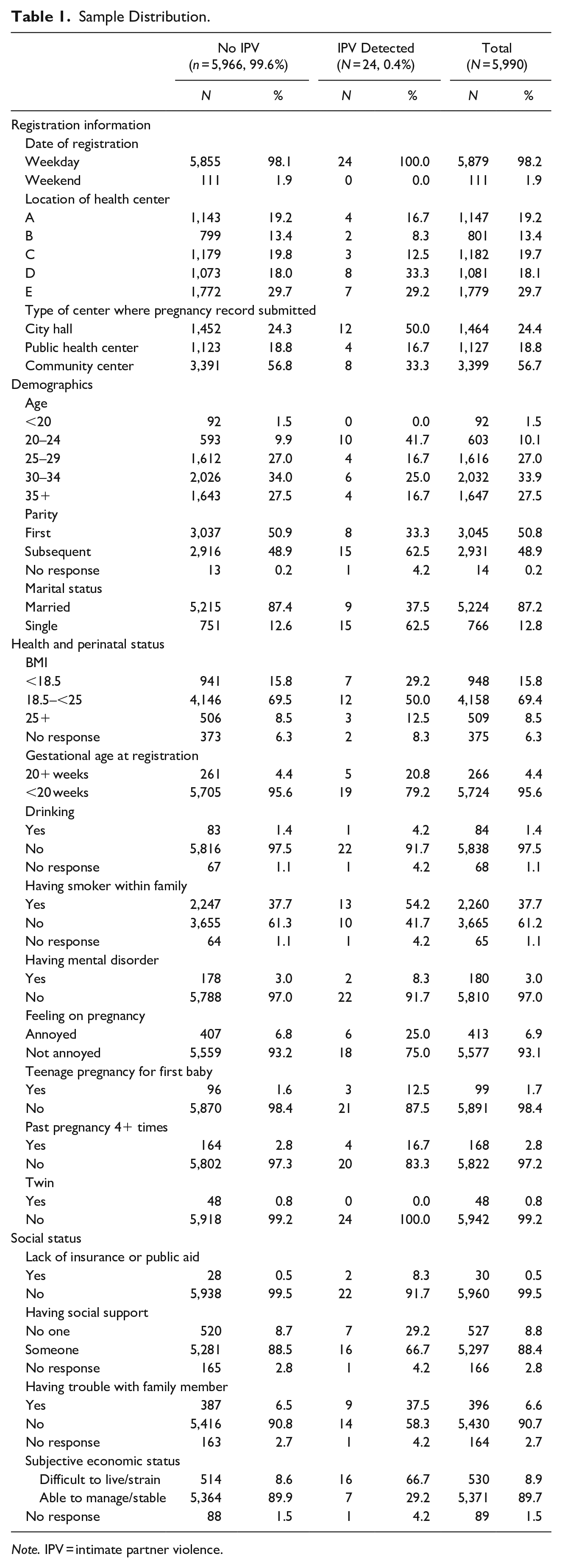
Note. IPV = intimate partner violence.
Table 2 shows the OR of each variable for IPV during pregnancy. For the variables related to registration and demographics, women who registered at the city hall, no response on parity, and single mother status showed a significant positive association with IPV during pregnancy. Further, for health status, thinness, teenage pregnancy for first baby, past pregnancy of four or more times, registration at late gestational week (later than 20 weeks), and feeling distressed when they found out they were pregnant showed significant higher risk for IPV. Meanwhile, mental disorders, drinking, and smoker within family showed a positive but not significant association. As for social environment, lack of insurance or receiving public aid, not having social support, having trouble with family member, and subjective poverty showed a significant positive association with IPV during pregnancy.
Crude Odds Ratio of Each Variable for Intimate Partner Violence During Pregnancy.
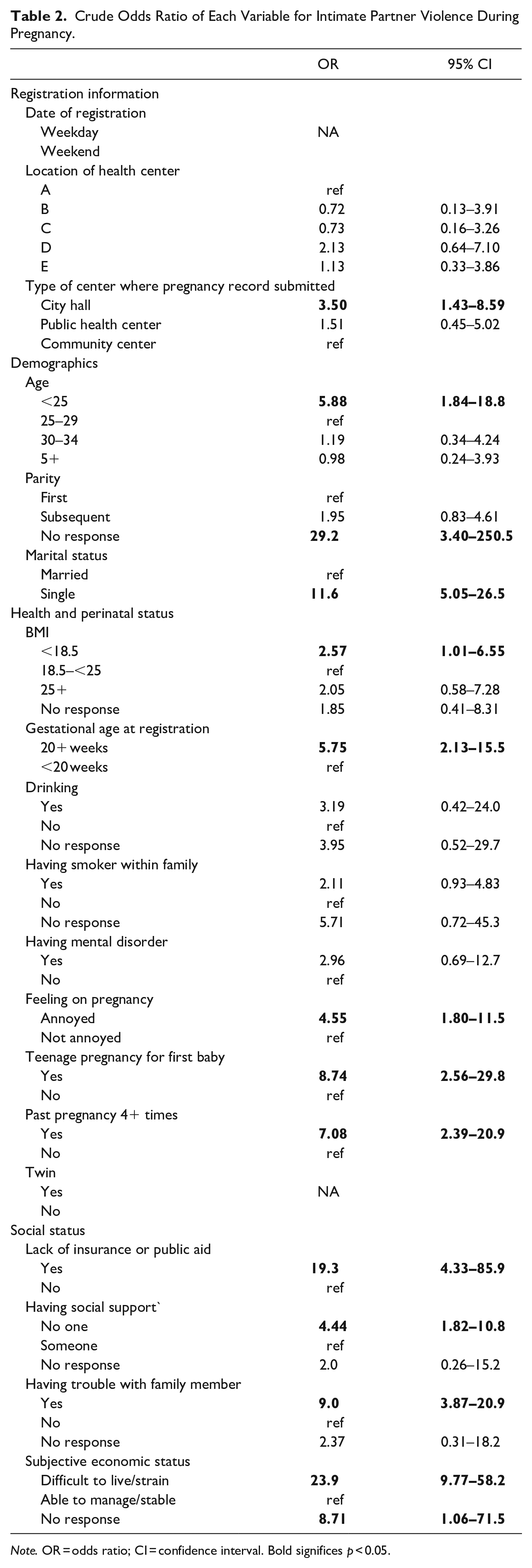
Note. OR = odds ratio; CI = confidence interval. Bold significes p < 0.05.
ORs of multiple logistic regression analyses are shown in Table 3. After adjustment for variables which were significant in the crude model, we found that subsequent child (OR: 3.45, 95% confidence interval [CI] [1.02–11.6]), single marital status (OR: 7.96, 95% CI [2.88–22.2]), thinness (OR: 3.17, 95% CI [1.13–8.90]), past pregnancy of four or more times (OR: 5.25, 95% CI [1.35–20.4]), having trouble with family member (OR: 5.45, 95% CI [1.95–15.2]), and poverty (OR: 6.27, 95% CI [2.25–17.5]) showed a significant association with IPV. R-square of this model reached 0.33.
Adjusted Odds Ratios of Selected Variables for Intimate Partner Violence During Pregnancy.
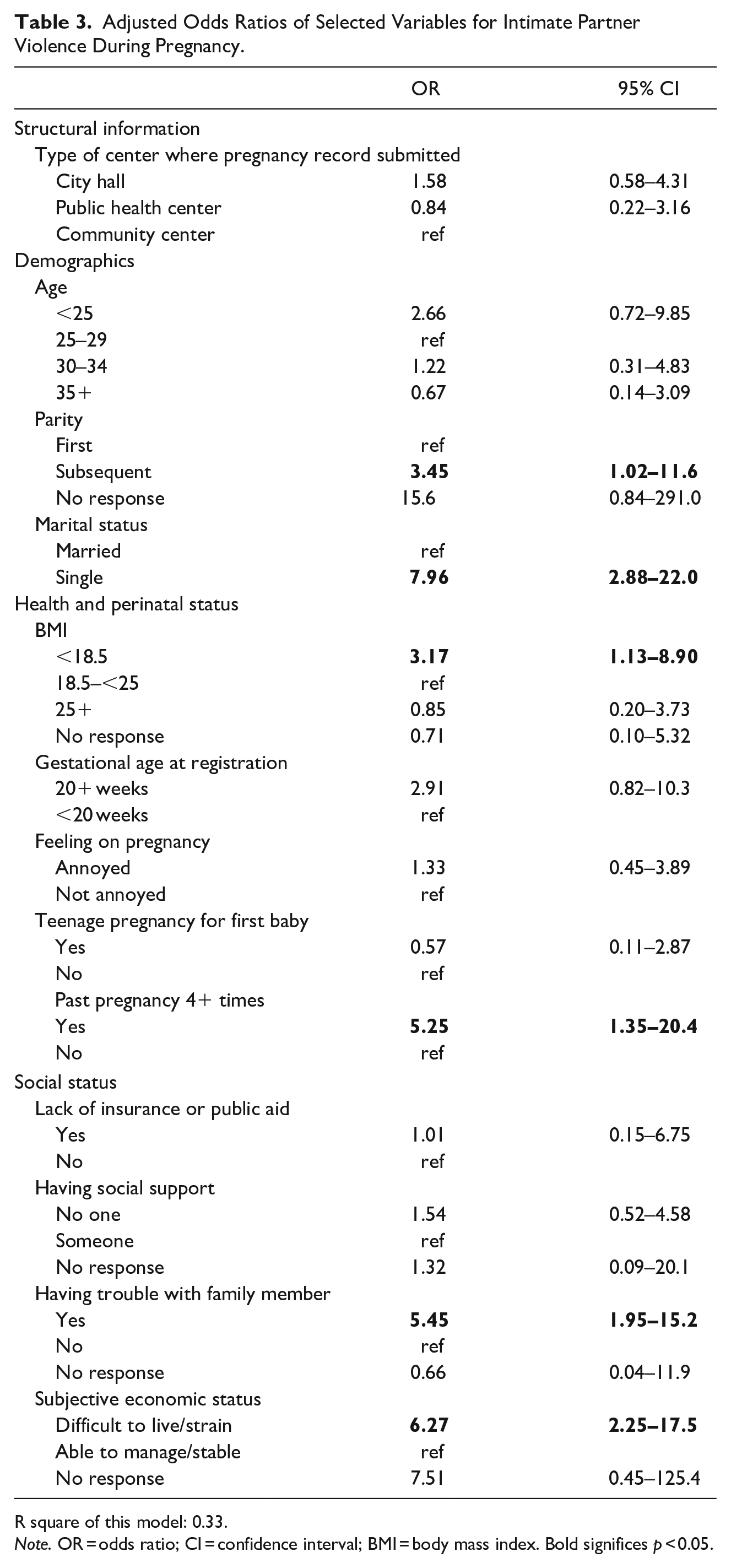
R square of this model: 0.33.
Note. OR = odds ratio; CI = confidence interval; BMI = body mass index. Bold significes p < 0.05.
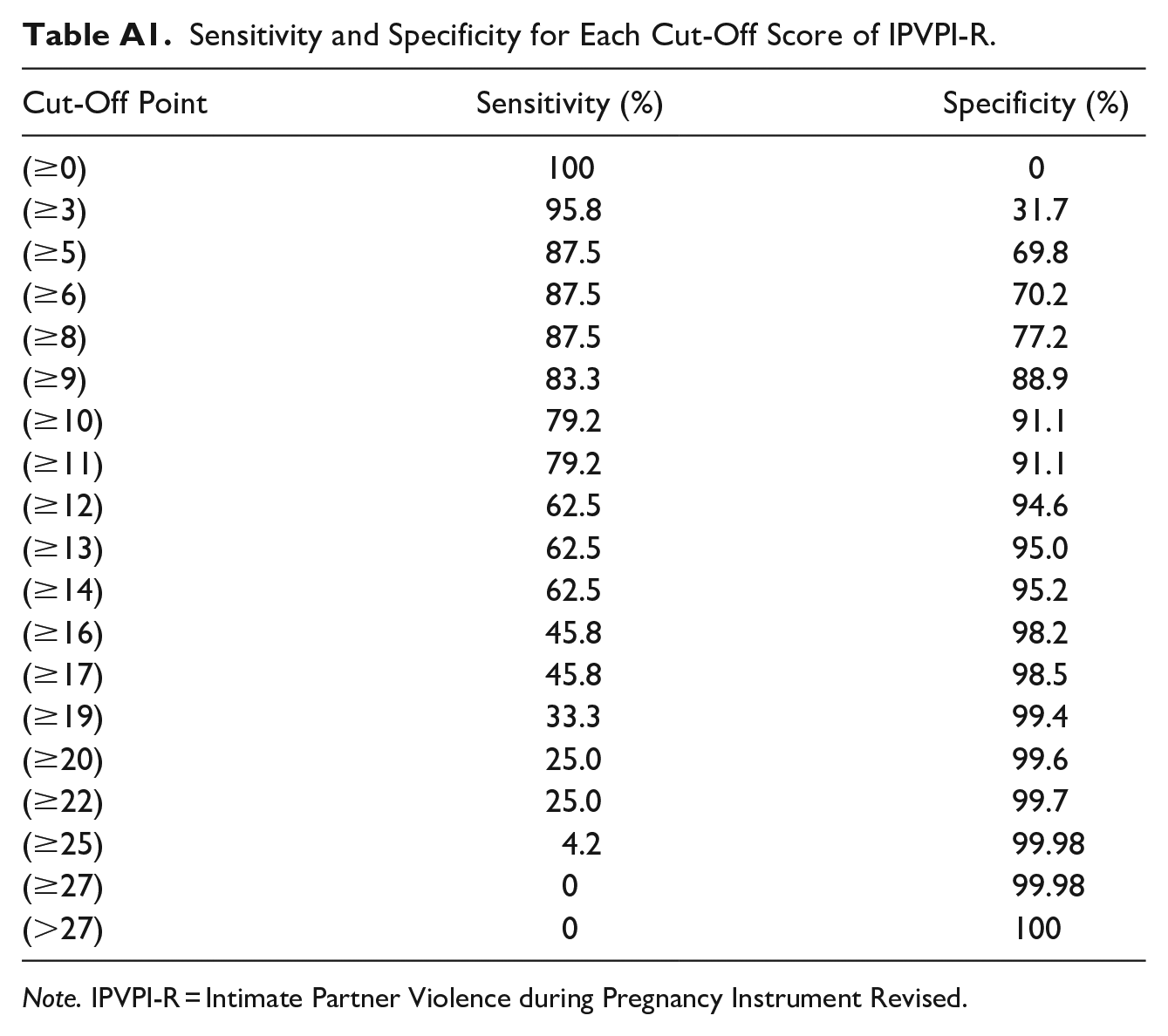
Table 4 shows the six variables and scores to detect IPV during pregnancy, hereinafter referred to as the Intimate Partner Violence during Pregnancy Instrument Revised (IPVPI-R). Using the OR found in multivariate logistic regression model, single marital status scored 8, followed by poverty (i.e., unstable socioeconomic status reported subjectively) which scored 6, and four times or more past pregnancy and having trouble with family member which scored 5, and subsequent delivery and thinness, both of which scored 3. The total score from IPVPI-R detected IPV with good discrimination (area under receiver operating characteristic curve = 0.89, 95% CI [0.81–0.97]) is shown in Figure 1. The cut-off of IPVPI-R score was considered as 8/9, with sensitivity of 0.83 and specificity of 0.89 (see Table A1).
Intimate Partner Violence During Pregnancy Instrument Revised.
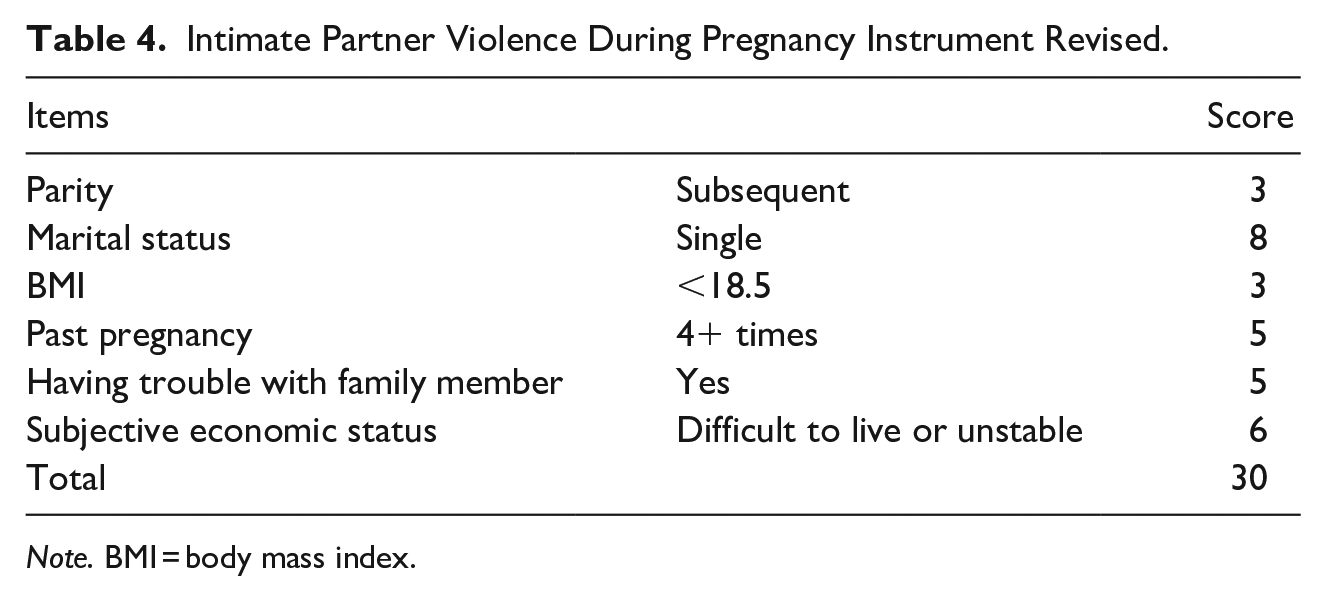
Note. BMI = body mass index.
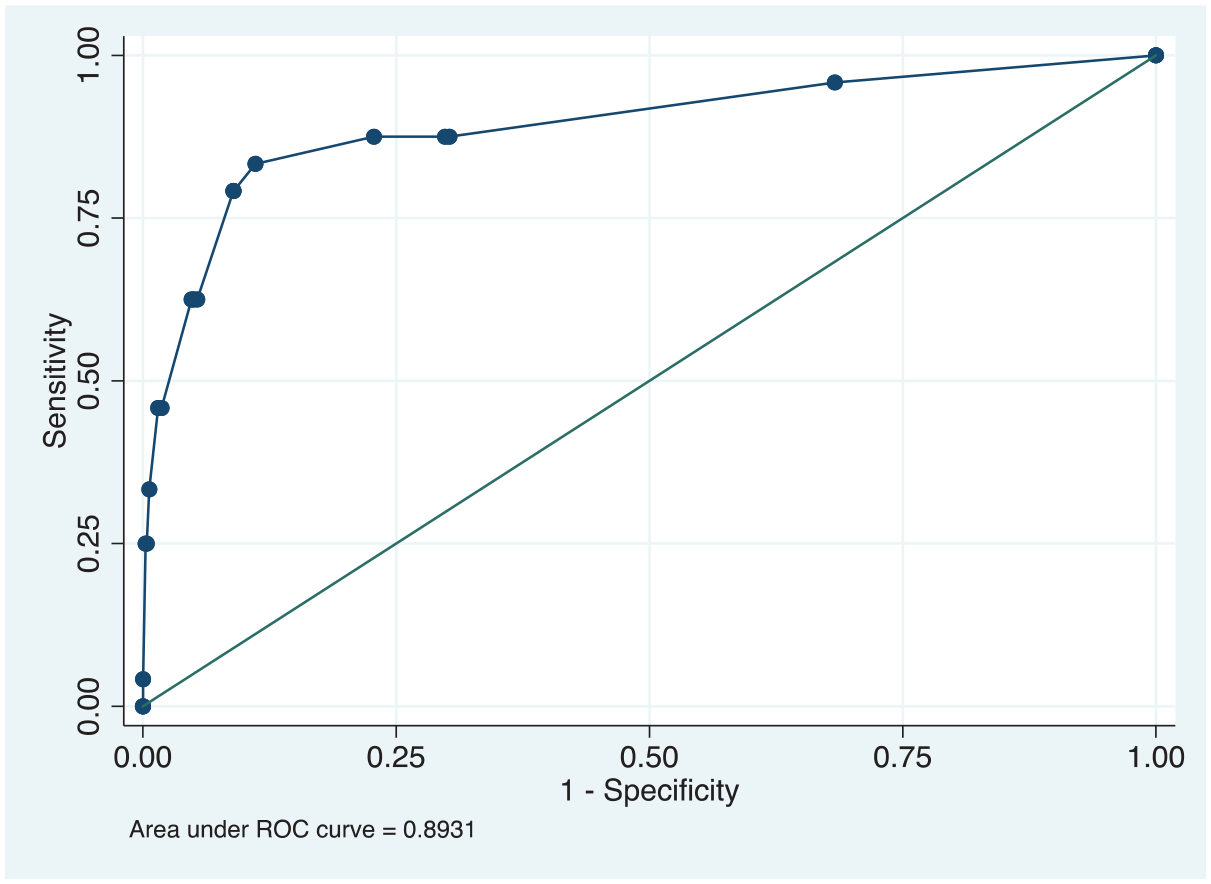
ROC curve of IPVPI-R.
Discussion
By using administrative data in a prospective design, we found that single marital status, poverty, past pregnancy of four or more times, having trouble with family member, subsequent delivery, and thinness measured at pregnancy registration, were independently strongly associated with IPV during pregnancy. Moreover, in combination of these six variables with weighted based on OR, we have developed a new scale to detect IPV during pregnancy, named IPVPI-R, which showed detectability of IPV during pregnancy with high sensitivity and specificity. As IPVPI-R used administrative data on IPV status, this scale would be better to capture IPV during pregnancy which need consultation than previous IPVPI, because the IPVPI used IPV status based on a self-administered questionnaire, which might be biased due to stigma or recall bias.
The risk factors found as IPVPI-R items were consistent with those of previous studies, including IPVPI (Doi et al., 2019). That is, multiple parity, having trouble with family member, and poverty as subjective socioeconomic status were also risk factors for IPVPI. However, while young maternal age, feeling distressed about the pregnancy, and lack of social support were associated with IPV during pregnancy in IPVPI, our data did not show that these variables were associated with IPV during pregnancy. This discrepancy may be due to the inclusion of marital status in IPVPI-R, that is, single marital status was more likely found in young maternal age, feeling distressed about the pregnancy, and lack of social support. Further, we found that an objective risk factor, thinness, was a risk factor of IPV during pregnancy. This is consistent with previous study, although in Bangladesh, a developing country, underweight women aged 15 to 24 years old were more likely to report physical and/or sexual IPV (Ferdos & Rahman, 2018). Although the directionality is unknown, that is, whether IPV induced thinness or thinness induced IPV, we found that thinness, which was often assessed at obstetric clinics and public health center, is one of the markers to detect IPV during pregnancy.
We add to the literature that IPVPI-R can be detectable without asking about IPV per se at the time of pregnancy registration. There exist several other screening tools to assess IPV, such as Abuse Assessment Screen (Kataoka et al., 2004), Partner Violence Screen (McFarlane et al., 1992), and Violence Against Women Screen (Feldhaus et al., 1997). However, IPVPI-R is useful in that it does not ask about IPV per se, which is important, especially in Japan, where people tend to hesitate to report IPV status to public health centers or obstetric clinics (Gender Equality Bureau Cabinet Office, 2016b). Although the IPVPI could also detect IPV during pregnancy without asking about IPV, IPVPI-R is more accurate as it is a report of IPV during pregnancy, while IPVPI was developed based on a self-report questionnaire. Although we showed that IPVPI-R is useful to detect IPV without asking IPV during pregnancy, having a safe space is warranted to inquire about the details of IPV situations (e.g., severity, frequency, or duration) from the detected mother.
We need to address several limitations before concluding. First, although we used administrative data on IPV status, some IPV cases were not captured by public health nurses or obstetric clinics, that is, IPV cases were only those who seek help during pregnancy, which may induce self-selection bias. Thus, this predictive model, IPVPI-R may underestimate the IPV cases during pregnancy, which were not captured by municipalities. Second, the number of IPV cases was small, so several risk factors were dropped due to underpower. For example, young maternal age of less than 25 years old and late gestational week at registration showed high OR (2.66 and 2.91, respectively), suggesting that these variables might be significantly associated with IPV during pregnancy if we had a larger number of IPV cases. A further replication study in municipalities with higher prevalence of IPV during pregnancy is warranted to examine whether other variables might be critical to predict IPV during pregnancy. Third, pregnant women may not report actual status on the items in the registration form which listed items as risk factors of IPV, such as subjective economic status or having trouble with family member, due to social-desirability bias. Nonetheless, we found several objective risk factors, such as marital status, thinness, parity, and past pregnancy.
The strength of this study is the use of administrative data, a prospective design, and population-based data. Further, IPVPI-R has strong predictability of IPV during pregnancy with AUC of 0.89, despite using only six items. This suggests that it is a feasible scale to be used in public health settings, without asking IPV status directly. Nonetheless, further research is needed to confirm the usefulness of IPVPI-R in other regions in Japan or in other countries.
In conclusion, we developed the IPVPI-R, which showed strong detectability of IPV during pregnancy using six items, and without the need to ask about IPV directly. The current study is useful to detect IPV during pregnancy and prevent further adverse health outcomes due to IPV during pregnancy, such as postpartum depression, low birth weight, and child maltreatment.
Footnotes
Appendix
Sensitivity and Specificity for Each Cut-Off Score of IPVPI-R.
| Cut-Off Point | Sensitivity (%) | Specificity (%) |
|---|---|---|
| (≥0) | 100 | 0 |
| (≥3) | 95.8 | 31.7 |
| (≥5) | 87.5 | 69.8 |
| (≥6) | 87.5 | 70.2 |
| (≥8) | 87.5 | 77.2 |
| (≥9) | 83.3 | 88.9 |
| (≥10) | 79.2 | 91.1 |
| (≥11) | 79.2 | 91.1 |
| (≥12) | 62.5 | 94.6 |
| (≥13) | 62.5 | 95.0 |
| (≥14) | 62.5 | 95.2 |
| (≥16) | 45.8 | 98.2 |
| (≥17) | 45.8 | 98.5 |
| (≥19) | 33.3 | 99.4 |
| (≥20) | 25.0 | 99.6 |
| (≥22) | 25.0 | 99.7 |
| (≥25) | 4.2 | 99.98 |
| (≥27) | 0 | 99.98 |
| (>27) | 0 | 100 |
Note. IPVPI-R = Intimate Partner Violence during Pregnancy Instrument Revised.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by JST RISTEX Grant Number JPMJRX16G5, Japan. We thank Dr Kazutaka Masuda, Ms Kawamura, Ms Sekine, and other public health nurses at Section of Health Prevention at Adachi City Hall.