
Abstract
This study examines the overlap between indirect exposure to forms of interpersonal violence and suicidal behavior, and the impact of the co-occurrence of these exposures on indicators of depressed mood and substance use among adolescents. Participants were a national sample of 3,917 youth aged 14–15 years, recruited online between June 2018 and March 2020, including an oversample of sexual and gender minority youth. Eight in ten (81.3%) youth reported exposure to indirect interpersonal violence and/or suicidal behavior in their lifetimes: 39.5% reported only interpersonal violence exposure, 5.9% only suicidal behavior exposure, and 35.9% reported both. Youth who reported exposure to interpersonal violence were almost three times more likely (adjusted odds ratio [OR] = 2.78, p < .001) to also report suicidal behavior exposure. Compared with youth having no indirect violence exposure, those with only interpersonal violence exposure were 2.25 times more likely (p < .001), those with only exposure to suicidal behavior 2.93 times more likely (p < .001), and those with both were 5.63 times more likely to report recent depressed mood. The unadjusted odds of any substance use was significantly elevated for each type of indirect violence exposure, with the highest odds seen among youth with dual interpersonal violence and suicide exposure (OR = 4.87, p < .001). For both outcomes, significant findings remained but were attenuated after adjusting for demographic characteristics, non-victimization adversity exposure, and cumulative direct victimization. Findings suggest that the combination of exposure to interpersonal violence and suicidal behavior appears to be particularly impactful. Results highlight that assessment of trauma exposure among adolescents needs to be more comprehensive and include not only direct and indirect interpersonal violence, but also knowledge of other people’s suicidal thoughts and behaviors.
A growing body of research on polyvictimization highlights the co-occurrence of forms of violence and the importance of cumulative impact—that is, experiencing a number of different types of violence is associated with greater mental and physical health impacts (Felitti et al., 1998; Finkelhor et al., 2007a). Indeed, in samples of youth, those who experience the highest levels of types of victimization often account for the strong association between violence and negative mental health outcomes across studies (Finkelhor et al., 2007b; Turner et al., 2006). Furthermore, the risk and protective factors for different forms of interpersonal violence, such as bullying, dating abuse, and sexual violence, are similar, leading to calls to remove silos between areas of study and instead focus on measuring co-occurrence (Hamby & Grych, 2013). Some gains have been made at connecting the study of forms of interpersonal violence victimization through a “connecting the dots” approach (Wilkins et al., 2014, 2018), but this work still often remains separate from studies of indirect violence exposure (i.e., witnessing) and particularly the study of self-directed violence, including exposure to suicide attempts and ideation. With the aim of contributing knowledge to further the integration of prevention approaches (Decker et al., 2018; Hamby & Grych, 2013), this study examines the overlap between indirect exposure to forms of interpersonal violence and suicidal behavior, and the impact of the co-occurrence of these exposures on depressed mood and substance use among adolescents.
The study uses Hamby and Grych’s Web of Violence framework (Hamby & Grych, 2013) which explains interconnections between forms of violence in terms of shared risk and protective factors including availability of community resources, positive social norms. It also centers polyvictimization theory that highlights the common negative mental health effects of exposure to traumatic events and the increasing negative impact presented by cumulative adversities across types of traumas over time (Davis et al., 2019).
A substantial proportion of U.S. adolescents witness or have other forms of indirect interpersonal violence exposure, making it a significant public health concern. Indeed, 68% of teens, aged 14–17 years have witnessed violence in their lifetime (Finkelhor et al., 2013). Furthering the public health impact is the well-documented connections between indirect violence exposure with depressive symptoms (Kilpatrick et al., 2003; Zinzow et al., 2009) and substance use (Kilpatrick et al., 2003; Thompson et al., 2020). Theories of trauma impact explain these connections by pointing out ways that the extreme physiological stress response activated by the fear of harm that victimization creates can have long-lasting impacts on physical health, cognitive functioning like memory, and emotional well-being including emotion regulation skills and symptoms of psychological distress (Marks et al., 2022; Pengpid & Peltzer, 2020). These pathways are also relevant to the stress created when witnessing someone else (such as a family member or peer) experience violence (Gollub et al., 2019). Polyvictimization theory highlights how the burden of greater dose of victimization, including exposure to community violence or violence between caregivers, creates the greatest risk for problems in well-being over time (Davis et al., 2018, 2019). Polyvictimization is a risk factor for psychological distress and for self-directed violence including suicide (Castellví et al., 2017; Johns et al., 2021). Less studied is how self-directed violence exposure (meaning, knowing someone who is at risk for self-directed violence or who has made a suicide attempt) as an adverse experience and potential trauma, may be part of the adversity burden youth carry and that should be included in polyvictimization tallies.
Indeed, there is a parallel and growing body of literature on exposure to suicide and other forms of self-directed violence (Banyard et al., 2021; Mitchell et al., 2019). This literature documents the large numbers of youth and young adults who have ever known someone close to them that made a suicide attempt or died by suicide (54%), someone who was thinking about suicide but did not made an attempt (62%), and someone who engaged in non-suicidal self-injury (43%); taken together, this amounts to 83% of youth in the United States (Banyard et al., 2021). Research also suggests that exposure to others’ suicidal behavior may negatively impact youth, including an increased risk for substance use (Cerel & Roberts, 2005; Cerel et al., 2005), personal suicidal ideation and attempts (Burke et al., 2010; Cerel & Roberts, 2005; Cerel et al., 2005; Chan et al., 2018; Hill et al., 2020; Insel & Gould, 2008; Maple et al., 2017; Mitchell et al., 2019; Randall et al., 2015), self-harm (Chan et al., 2018; McMahon et al., 2013), and emotional distress (Bottomley et al., 2018; Cerel & Roberts, 2005; Mitchell et al., 2019; Nanayakkara et al., 2013).
Research that is inclusive of both interpersonal violence and self-directed violence tends to focus on personal thoughts of suicide and its relationship to direct forms of interpersonal violence rather than how indirect exposure impacts mental health and how it may contribute to polyvictimization (Dworkin et al., 2020; Koyanagi et al., 2019). Researchers describe common epidemiology, risk and protective factors for suicide, community violence, and interpersonal violence including systemic oppression of groups within communities, concentrated under-resourcing and disadvantage, and connections to family and organizations like schools (Decker et al., 2018, Wilkins et al., 2014). A large gap, therefore, is the overlap and associated relative unique and combined impact of exposure to indirect forms of interpersonal violence and exposure to self-directed violence and how these may be distinct but also synergistic in their impact on mental health outcomes such as depression and substance use. This is an important question, given that these indirect exposures are often the focus of bystander trainings for violence prevention (aiming to mobilize third parties who witness or know about different forms of violence but are not direct victims themselves). To date, we know little about the impact of being in this potential bystander position. Finally, although interpersonal violence and suicidal behavior can co-occur and share several risk factors, there are some key distinguishing factors as well, including depression being a particularly strong correlate of suicidal behavior (Zimmerman & Posick, 2014). Indeed, the interpersonal psychological theory of suicide describes a set of risk factors that distinguish between individuals with suicide ideation and those who go further and make an attempt (Cero & Sifers, 2013). It is important to better understand how exposure to these two types of violence co-occur and overlap, and also are distinct.
This paper aims to study the individual and combined impact of exposure to suicidal behavior by others and interpersonal violence by others witnessed but not directly experienced as a victim in relation to depressed mood and substance use. The goal was to more clearly assess Hamby and Grych’s web of violence within one sample of high-risk individuals—adolescents. Given the strong association between cumulative direct victimization (i.e., polyvictimization) and non-victimization adversity, we adjust for these experiences in our analyses. Specifically, this study will (1) explore the demographic and psychosocial characteristics of youth who experienced (a) indirect interpersonal violence only, (b) exposure to suicidal behavior only, and (c) both indirect interpersonal violence and suicidal behavior in their lifetimes; (2) examine the overlap between exposure to suicidal behavior with different forms of indirect interpersonal violence as well as cumulative direct victimization and non-victimization adversity; and (3) examine the associations between different combinations of indirect violence exposure (i.e., interpersonal only, suicidal behavior only, both) with (1) past month depressed mood and (2) past year substance use in the context of direct victimization and non-victimization adversity.
Methods
Growing up with media is a national, longitudinal survey of youth designed to study sexual violence in adolescence (Ybarra & Petras, 2020; Ybarra & Thompson, 2018). In addition to the original cohort recruited in 2006, a cohort of 3,917 new youth aged 14–15 years was recruited between June 2018 and March 2020, including an oversample of sexual and gender minority (SGM) youth to support subgroup analyses. Data from this new cohort comprise the analytic sample for this article. Table 1 provides details of the demographic characteristics.
Youth Demographic Characteristics by Types of Indirect Violence Exposure Use.
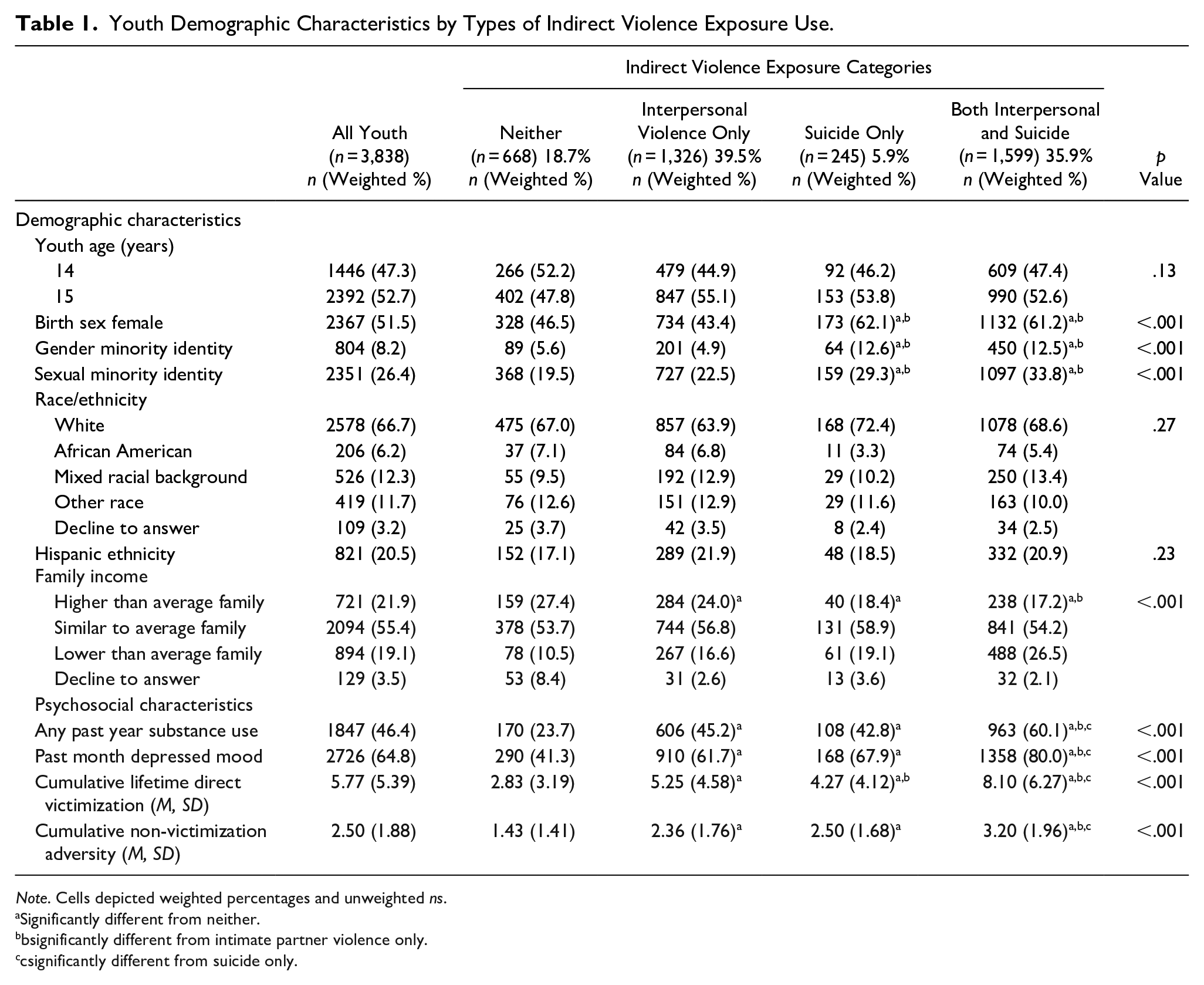
Note. Cells depicted weighted percentages and unweighted ns.
Significantly different from neither.
bsignificantly different from intimate partner violence only.
csignificantly different from suicide only.
Participants were recruited through study advertisements on social media, particularly Facebook and Instagram. Online ads encouraged youth to “have their voice heard” and “make a difference.” Survey aims were not mentioned to reduce self-selection bias based upon interest in a particular topic and the incentive was not mentioned at this point to help reduce fraudulent activity. Multiple steps were taken to ensure the authenticity of the sample, including comparing the age entered in the screener with their date of birth. Duplicates were identified by comparing phone numbers and email addresses across participants. Those interested clicked on the online advertisement, which linked them to a secure survey website. The first page provided a study description and contact information for study staff. The subsequent pages asked screening questions to determine eligibility. Those who were eligible (i.e., 14–15 years of age and living in the United States, English, or Spanish speaking) were then asked to read an assent form and to indicate their willingness to participate in the survey before continuing with the main survey.
To promote a diverse sample, demographic quotas were identified and determined at the screener phase of the study. Once the targeted number of youth in a particular group had been achieved (e.g., White, non-Hispanic, cisgender girls), subsequent youth in this group who were otherwise eligible were deemed ineligible. Because of this complex quota sampling structure, it is not possible to come up with a truly accurate number of people who were ineligible using this methodology. To enhance the diversity and representativeness of our sample to all SGM youth in particular, we requested and were granted a waiver of parental permission for participants under 18 years of age. Indeed, a waiver is necessary to avoid fatal sampling bias in the SGM sample that would occur by only including those who are out to their parents (Cwinn et al., 2021). Moreover, requiring parental consent could potentially place youth in situations where their sexual experiences and/or sexual attraction could be unintentionally disclosed to their caregivers. In some families, this could pose physical or emotional danger for the youth. Appropriate mechanisms were in place to protect the youth, such as localized referrals to mental health supports. The protocol was reviewed and approved by Pearl Institutional Review Board.
Participants were given a $15 incentive as an Amazon gift code for completing the survey. Ineligible youth were directed to a web page that included links to general resources for youth (e.g., https://youngwomenshealth.org).
Measures
Exposure to suicidal behavior (Turner & Butler, 2003; Turner et al., 2006) was measured by asking “has someone close to you ever tried to kill him or herself on purpose (like by shooting or cutting him or herself, or taking too many pills or drugs)?” Response options were yes, no, or decline to answer.
Indirect Interpersonal Violence Exposure
Nine questions asked about lifetime witnessing of violence; seeing or hearing about a range of types of violent experiences across multiple domains (yes/no), including assault (2 items) (Hamby et al., 2004): “Have you in real life seen someone get attacked or hit on purpose?”; interpersonal violence (3 items) (Hamby et al., 2004)”; “Have you in real life seen or heard one of your parents get hit, slapped, punched, or beat up by your other parent, or by their boyfriend, girlfriend, or partner?”; and sexual violence (4 items): “Have you ever seen or heard about someone you know in-person who said something sexual to someone when that person did not want to hear it.” Items are examined individually as well as part of a total count of number of types of indirect violence exposures experienced (mean = 1.79, SD = 1.63, range: 0–7).
Substance Use
Questions were based on those asked in the Youth Risk Behavioral Surveillance Survey (Centers for Disease Control and Prevention, 2020). In the past 12 months have you. . . (1) had a drink of alcohol, like beer, wine, or vodka, other than a few sips without your parents’ permission; (2) smoked a tobacco (regular) cigarette, even just a puff; (3) smoked an e-cigarette, even just a puff; (4) smoked marijuana or pot; (5) used an inhalant like whippets, glue, and paints; (6) taken a prescription drug (such as OxyContin, Percocet, Vicodin, codeine, Adderall, Ritalin, or Xanax) without a doctor’s prescription; (7) used steroids or shots without a doctor’s prescription; (8) used a “club drug” like ecstasy (MDMA), GHB, Rohypnol, or Special K (ketamine); and (9) used meth (also called speed, crystal, crank, or ice), heroin (also called smack, junk, or China White), or cocaine, including powder, crack, or freebase (yes/no/decline to answer for each). A positive response to any of these types of substance use was indicative of any substance use in the past year.
Depressed Mood
Youth were asked one item developed for the study: In the last month, was there ever a time of 2 weeks or longer when you were feeling unhappy, bummed out, depressed, or down most of the day or nearly every day? Response options were no, yes, and not sure. Not sure responses were conservatively coded as “no” under the assumption that if the participant was unclear, it was less likely to be salient. Indicators of depressed mood have been found to be a strong indicator of clinical depression in children and adolescents (Cole et al., 2011).
Direct victimization consists of a count of the number of positive endorsements to the following types of victimization that were directed at the participant and experienced in the past year: sexual harassment, sexual assault, robbery, physical assault, and peer victimization. More specifically, eight different types of past year sexual harassment were queried (Koss & Gidycz, 1985; Lipson, 2001). Lifetime sexual victimization included four items: sexual assault, coercive sex, attempted rape, and rape (Ybarra et al., 2016). Past year theft was queried with one item asking if “Someone stole something from me” (Hamby et al., 2004). Past year physical assault was queried with two items: “Another person or group attacked me” and “Someone pulled a knife or gun on me” (Hamby et al., 2004). Past year generalized peer victimization was measured using six items (Ybarra et al., 2012). As an example, “How often have others around your age bullied you by: Hitting, kicking, pushing, or shoving you.”
Lifetime non-victimization adversity (Turner & Butler, 2003; Turner et al., 2006) was measured using nine items (yes/no), including lifetime exposure to non-violent traumatic events (serious illnesses, accidents, and parental imprisonment) and chronic stressors (substance abuse by family members and homelessness).
Demographic Characteristics
For multivariate analyses, age was included as a categorical variable given the small age range: 14 and 15 years. Self-reported household income comprised three answer choices: lower than average, about average, and higher than average. For multivariate analyses, those who indicated their family income was “lower than average” were compared to all other youth. Youth reported their race (coded as White vs. other for multivariate analyses) and ethnicity (coded as Hispanic vs. other). Sex was coded as female at birth versus other and sexual identity as sexual minority (i.e., gay, lesbian, bisexual, questioning, queer, pansexual, asexual, other) versus heterosexual/straight. Gender minority included youth who identified as transgender, gender queer, non-binary, pangender, questioning, unsure, and some other identity versus cisgender (i.e., gender same as sex assigned at birth). In the absence of following youth to observe their behavior—which is both infeasible and likely unethical—it is difficult to determine whether self-report is accurate. To adjust for this, self-reported honesty is included in the regression model, on a scale of 1 (not at all honest) to 5 (extremely honest) (Ybarra et al., 2008). Validity is suggested: Consistent with prior research (US Surgeon General, 2001), those who report a high degree of dishonesty are also more likely to report externalizing behaviors.
Data Analysis
Missing data were generally low and never greater than 5%, and in all cases, replaced with the item mean for sum scores and coded as zero (“symptom absent”) for dichotomous measures at the item level. To address research question 1, we explored both demographic (e.g., age, birth sex, sexual minority identity, gender minority identity, race, ethnicity) and psychosocial (e.g., cumulative direct victimization, cumulative non-victimization adversity) characteristics across four categories of exposure: (1) none, (2) interpersonal violence only, (3) suicidal behavior only, and (4) both interpersonal violence and suicidal behavior using design-based F statistics, which account for complex sampling design. Next, we report the rates of types of indirect interpersonal violence exposure, count of indirect interpersonal violence exposures, count of direct victimization types, and count of types of non-victimization adversities between youth who did and did not report suicidal behavior exposure; adjusted odds for each were calculated using logistic regression analyses (with suicidal behavior exposure as the outcome variable) controlling for youth demographic characteristics and self-reported honesty in answering survey questions. Three separate logistic regression analyses were conducted with past month depressed mood as the outcome and the following as independent variables: (1) indirect violence exposure (interpersonal violence only, suicidal behavior only, both interpersonal violence and suicidal behavior) with neither as the reference category; (2) plus demographic characteristics; and (3) plus cumulative direct victimization and cumulative non-victimization adversity. Finally, the above regression analyses were conducted with any substance use as the outcome and analyzed using logistic regression.
Data were weighted to represent the population of U.S. adolescents aged 14–15 years, using results from the 2019 National Youth Behavior Risk Surveillance System. Weighting was accomplished using iterative proportional fitting to balance the distributions of all variables (Deming & Stephan, 1940). Cell weights were computed based on combinations of the following variables: age, gender, sexual intercourse (ever had yes/no), and sexual identity.
Results
Prevalence Rates of Youth Exposure to Indirect Interpersonal Violence and Suicidal Behavior
Eight in ten (81.3%) youth reported exposure to indirect interpersonal violence and/or suicidal behavior in their lifetimes: 39.5% reported only interpersonal violence exposure, 5.9% only suicidal behavior exposure, and 35.9% reported both. Types of exposure varied by birth sex with more females reporting any exposure (either alone or combined) that involved suicidal behavior (Table 1). Sexual minority and gender minority youth were also more likely to report exposure to suicidal behavior only or in combination with interpersonal violence compared to their non-sexual or gender minority peers. Compared with youth with no exposure, those living in households with self-appraised lower-than-average incomes were more likely to report any indirect violence exposure, and particularly both interpersonal violence and suicidal behavior exposure. No differences were noted across exposure groups based on youth age, race, or ethnicity. Psychosocial characteristics varied significantly based on type of exposure with the dual interpersonal violence and suicidal behavior exposure group reporting the highest levels of psychological challenge: any past year substance use, past month depressed mood, cumulative lifetime direct victimization, and cumulative lifetime non-victimization adversity types.
Intersection of Exposure to Suicidal Behavior and Interpersonal Violence
Any exposure to interpersonal violence, as well as each specific type measured, was significantly related to elevated odds of suicidal behavior exposure, even while taking into account youth demographic characteristics (Table 2). Specifically, youth who reported exposure to interpersonal violence were almost three times more likely (adjusted odds ratio [aOR] = 2.80, p < .001) to also report suicidal behavior exposure. Furthermore, for each additional type of interpersonal violence exposure, there was a 1.39 increased odds of suicidal behavior exposure. Similar patterns were noted for each additional type of direct victimization experienced (aOR = 1.11, p < .001) and each type of non-victimization adversity experienced (aOR = 1.31, p < .001).
Intersection of Exposure to Suicide and Indirect Interpersonal Violence.
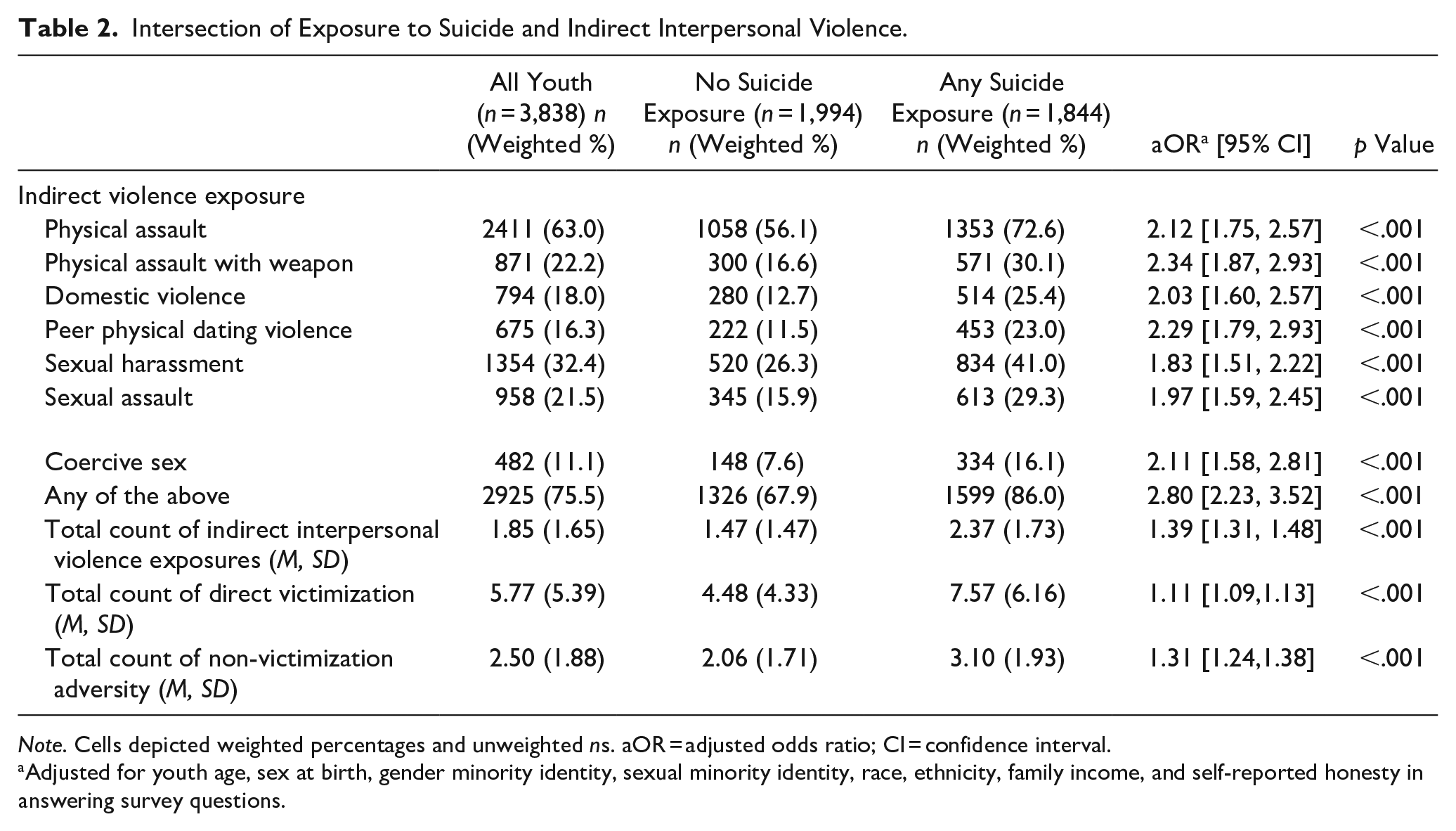
Note. Cells depicted weighted percentages and unweighted ns. aOR = adjusted odds ratio; CI = confidence interval.
Adjusted for youth age, sex at birth, gender minority identity, sexual minority identity, race, ethnicity, family income, and self-reported honesty in answering survey questions.
Association Between Types of Violence Exposure and Past Month Depressed Mood
64.8% of youth reported past month depressed mood. Compared with youth having no indirect violence exposure, those with only interpersonal violence exposure were 2.25 times more likely (p < .001), those with only exposure to suicidal behavior 2.93 times more likely (p < .001), and those with both were 5.63 times more likely to report depressed mood, without taking into account demographic characteristics or direct victimization and adversity exposure (Table 3). After further adjusting for demographic characteristics (Model 2), these relationships remained, although became slightly attenuated. In Model 3, after adjusting for direct victimization and adversity experience, each type of indirect violence exposure still contributed to past month depressed mood, with the largest attenuation seen among youth with dual interpersonal violence violence (IPV) and suicide exposure where the adjusted odds reduced to 2.79 (p < .001).
Logistic Regression Analysis of the Association Between Types of Indirect Violence Exposure and Past Month Depressed Mood.
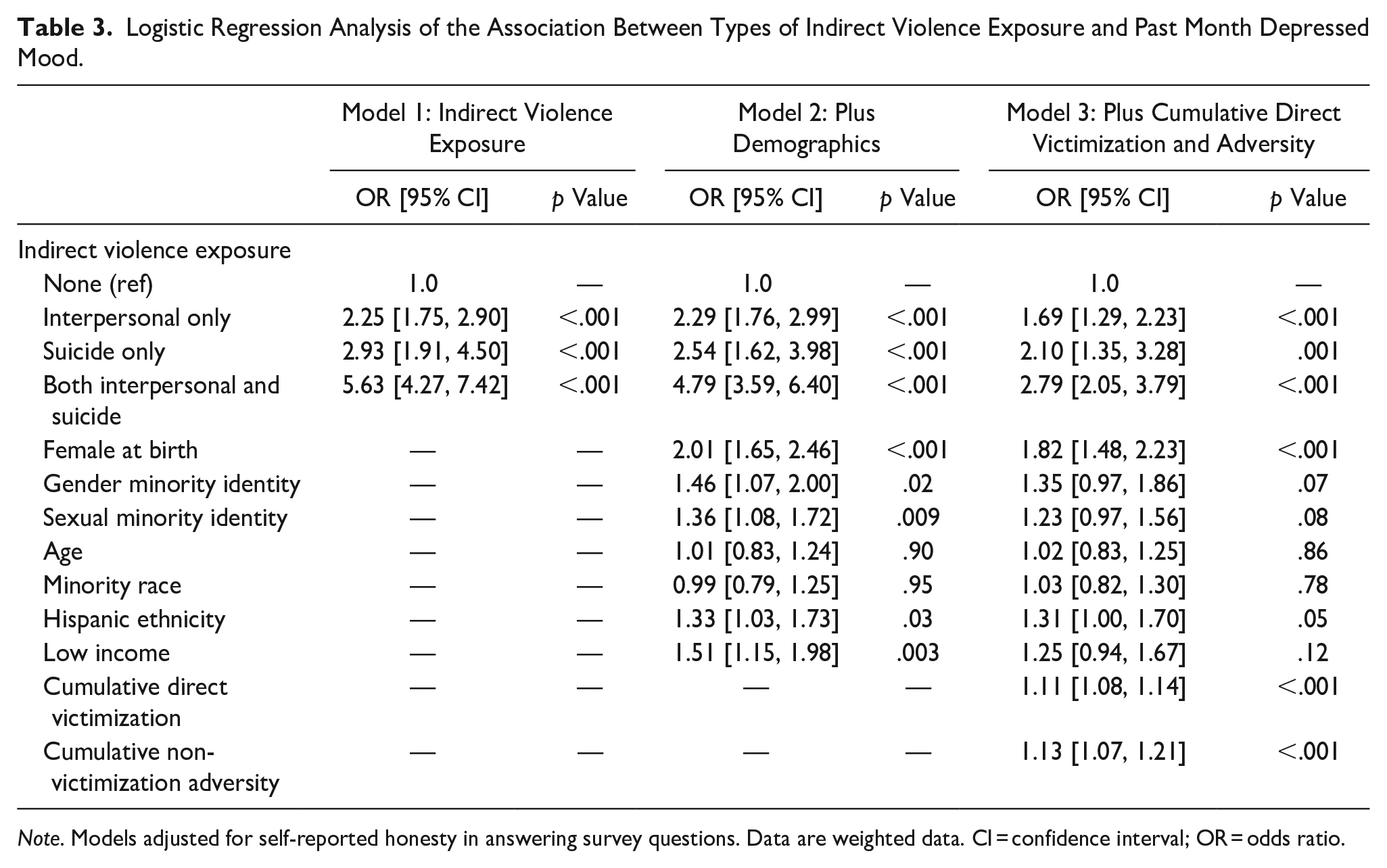
Note. Models adjusted for self-reported honesty in answering survey questions. Data are weighted data. CI = confidence interval; OR = odds ratio.
Association Between Types of Indirect Violence Exposure and Past Year Substance Use
46.4% of participants reported any substance use in the past year. As seen in Table 4, the unadjusted odds of any substance use were significantly elevated for each type of indirect violence exposure, with the highest odds seen among youth with dual interpersonal violence and suicide exposure (OR = 4.87, p < .001). Similar odds were seen when taking into account demographic characteristics. Even after taking into account cumulative direct victimization and non-victimization adversity experience, the relationships between the different groups of exposures remained significant, but attenuated, with the highest odds of substance use among those with dual IPV and suicide exposure (aOR = 2.50, p < .001).
Logistic Regression Analysis of the Association Between Types of Indirect Violence Exposure and any Past Year Substance Use.
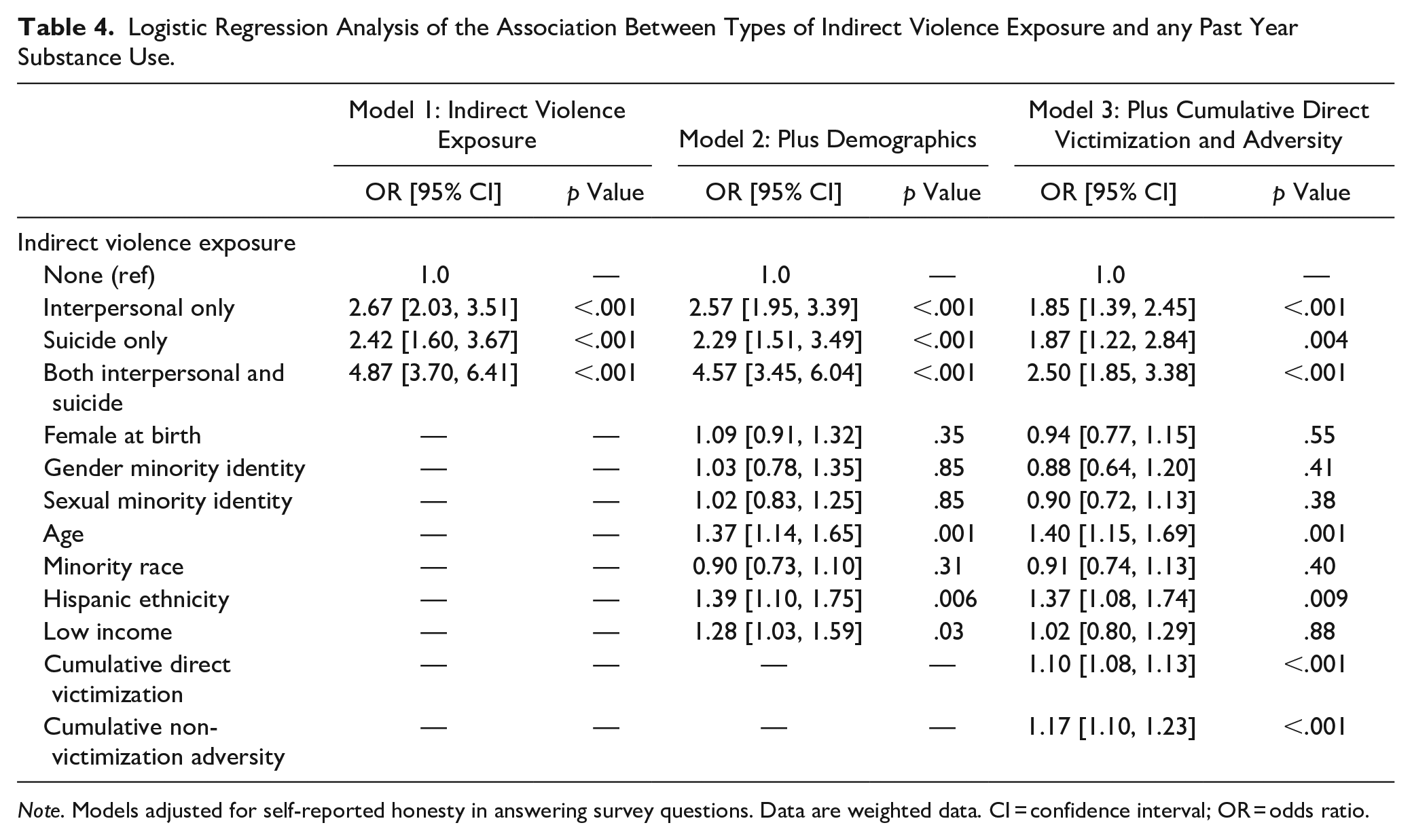
Note. Models adjusted for self-reported honesty in answering survey questions. Data are weighted data. CI = confidence interval; OR = odds ratio.
Discussion
In this study, more than four in five youth nationally were exposed to violence indirectly—both interpersonal and self-directed in nature—by the time they reached their early-to-mid teens. Both interpersonal and self-directed violence exposures were related to psychosocial challenge for teens and these effects showed up even when a person’s own direct victimization and adversity experiences were accounted for. Indeed, the combination of exposure to interpersonal violence and suicidal behavior appeared to be particularly impactful. These findings highlight that assessment of trauma exposure among adolescents needs to be more comprehensive and include not only experiencing and witnessing violence, but also other people’s awareness of the suicidal thoughts and behaviors of others. Knowing individuals in one’s network who have been affected by self-directed and interpersonal violence can influence well-being and may be appropriate topics for clinical interventions.
At the same time, it is possible that youth who are experiencing depressive symptoms and/or are struggling with substance use may be more likely to have friends who are depressed, suicidal, or experiencing interpersonal violence. Indeed, research on social networks provides some evidence of contagion of mood within networks (Block & Burnett Heyes, 2020; Prinstein, 2007) and self-directed violence contagion within networks of youth is well documented (Abrutyn et al., 2020; Copeland et al., 2019). It may be beneficial to ask youth presenting with depressive symptoms or substance use about their friends and the experiences they are dealing with as well. Research is all too often siloed by type of violence exposure. This study highlights the importance of continuing to “connect the dots” as the Centers for Disease Control and Prevention assert (Wilkins et al., 2014). A complete understanding of the impact of adversity burden across the lifespan needs to connect a range of adverse childhood experiences to a wide array of direct, indirect, and self-directed violence exposures in adolescence. Prevention strategies could then take more inclusive approaches rather than diffusing resources by trying to address specific risk behaviors and forms of violence individually (Decker et al., 2018). Furthermore, the findings about these interconnections and the burden of distress they create argues for making trauma-informed interventions more widely available to young people (Neelakantan et al., 2019; Smith et al., 2019).
Findings also suggest that when youth are exposed to suicidal behavior, it is much more likely to occur alongside interpersonal violence exposure, rather than alone. Suicidal behavior exposure does not exist in isolation. These findings support theories including the web of violence and polyvictimization but expand our empirical understanding of these frameworks to include traumas that are experienced indirectly. While programs such as Mental Health First Aid and physician screening for suicide are important, more should be done to make sure screenings are inclusive and comprehensively assess the adversity burden of today’s youth. The CDC’s report Connecting the Dots makes the argument that the overlapping risk factors between different forms of interpersonal violence and also self-directed violence make it likely that a person experiencing one type is likely to also be carrying the burden of others. This study reminds us that it is not only important to talk with youth about their own experiences of victimization, but also to engage them in assessing more indirect forms of violence. These findings expand our understanding of self-directed violence as not just a consequence of interpersonal violence victimization, but also a co-occurring form of trauma exposure. As we describe in more detail below, youth indirectly exposed to violence are bystanders or actionists that prevention programs work to engage in risk reduction and violence and suicide prevention efforts. To date, bystander or gatekeeper trainings are very siloed by topic. A set of programs focus on sexual or dating violence (Coker et al., 2019; Edwards et al., 2019) while a separate set focus on peers getting help for peers who may be experiencing suicidal ideation of mental health problems (Maslowski et al., 2019). The prevention field needs to do more to build connections between these prevention efforts.
Implications
Conducting interpersonal violence research with a diversity lens is critical given the extensive health disparities faced by marginalized groups, such as SGM youth, racial and ethnic minorities, and youth living in low-income households (Bent-Goodley, 2021; Tajima, 2021). For example, given the complex cluster of social and economic problems that are often linked with interpersonal violence and suicide, such as poverty and marginalized social identity status, a diverse range of individual-, family-, and community-based interventions may be needed which can be informed by research. Consistent with previous studies (Banyard et al., 2021; Mitchell et al., 2021), the current research found adolescents from low-income families (a marker of low resourced communities) and those who identified as SGM were more likely to report both interpersonal violence and suicidal behavior exposure. Findings provide more evidence for our existing knowledge base about the health disparities faced by these marginalized communities. Strengths-based prevention strategies encourage practitioners to go beyond individual interventions and those that are siloed by type of violence to create more comprehensive policies and supportive social and cultural contexts and resources that can diminish these risk factors (Banyard & Hamby, 2022).
The current sample is diverse from a racial and ethnic perspective with one in five youth who identified as Hispanic and three in 10 as a racial minority group. With this large sample size, we were able to analyze and identify how those of Hispanic descent reported elevated rates of depressed mood and substance use, even in the context of other demographic characteristics, indirect and direct violence exposure, and non-victimization adversity. Discrimination may play a role; in one study among Hispanic adolescents in Los Angeles, perceived discrimination in 9th grade significantly predicted depressive symptoms and drug use in 11th grade (Basáñez et al., 2013). Findings highlight the need for the incorporation of culture to better understand how the lived experiences of marginalized youth contextualizes our understanding of the mental and behavioral health needs of this and other under-represented groups in interpersonal violence research.
The current findings have particularly important implications for prevention. The findings remind us that we may think we are doing primary prevention with adolescents when in fact many of them already have been exposed to trauma (Brush & Miller, 2019) in the form of these indirect exposures and thus may be in need of intervention services. Our violence prevention efforts need to work across many levels, to not only prevent future instances of violence, but also to heal those that have been exposed to others’ trauma. A robust body of research has established the evidence base for a range of effective trauma-informed treatments for adolescents. The issue is making such resources widely available and accessible, especially for youth in under-resourced communities that are also shouldering the burden of historic and systemic oppressions. There is also a need for research to better establish the evidence base for trauma treatment practices in accessible spaces like schools (Maynard et al., 2019).
Beyond intervention, the current findings are important for both suicide and violence prevention programs that use a bystander/gatekeeper model. Innovations in prevention of interpersonal and self-directed violence increasingly focus on third party training of those who witness these traumas to position them to respond and help. In the interpersonal violence field, this has been called bystander training (Coker et al., 2019; Mujal et al., 2021) and gatekeeper training in the suicide prevention field (Holmes et al., 2021). Themes such as bystander training fit with calls for an integrated public health approach to indirect interpersonal violence and suicide prevention and response (Decker et al., 2018).
This study suggests that being a bystander in these instances may itself have potential negative effects on bystanders. To date, many bystander programs focus mainly on teaching helping skills—promoting recognition of violence or suicidal behavior and describing strategies that might be used to respond. Current findings indicating positive relationships between violence exposure and personal negative affect, as well as past research (Mitchell et al., 2022), suggest that such programs should also include important self-care modules so that bystanders can promote and protect their own well-being while assisting others. The Mental Health First Aid program is an example of a prevention strategy that includes such a module, reminding bystanders to check in with their own emotions and to seek support and mental health promoting resources (Morgan et al., 2018). Bystander trainings need to include components that help potential bystanders expand their toolkits of healthy coping behaviors through strengths-based practices like integrating mindfulness or exercise or narrative writing (Banyard & Hamby, 2022). Furthermore, training programs often are individual focused, teaching skills to individual bystanders rather than creating a community of helping so that the stress and burden of helping is shared. Bystander training is often provided in one or two sessions with little follow-up. Bystanders may benefit from being connected to more ongoing communities of practice/helping so that they have a community to check in with about their helping efforts, what worked or not, and what they might try in the future. Indeed, a recent study by Mitchell and colleagues (Mitchell et al., 2022) found that one in five bystanders to self-directed violence did not feel good about the helping they did. More widespread attention to bystander self-care in prevention can protect bystanders which also may make people more willing to help again in the future.
Limitations
The measure for depressed mood is broad and should not be considered as a marker for clinical depression or depressive symptomatology; more research is needed that includes a more thorough assessment of mental health indicators. The cross-sectional nature of this study limits inferences about temporal associations. We do not know, for example, how recent the interpersonal violence and suicidal behavior exposures were, nor how close the participant was to the person which has implications for impact (Cerel et al., 2017). We also do not know if poorer mental health and differing levels and types of substance use are increasing the likelihood of exposure to interpersonal violence and suicidal behavior, or if such exposure are linked to negative affect.
Conclusion
Exposure to both interpersonal violence and suicidal behavior are significant public health concerns affecting our youth population. Although much research is available to inform our understanding of each type of exposure separately, there is a notable gap in our understanding of how such exposures overlap. This study provides new insight into the potential impact of exposure to both types of violence on depressed mood and substance use for youth. Findings highlight the importance of including both simultaneously when considering clinical assessments of youth as well as prevention and intervention strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by an NIH grant, R01 HD083072b. The funder did not participate in the work.