
Abstract
Intimate partner violence (IPV) is a significant global public health problem that results in high social and economic costs to individuals and communities. Compared to women in the general population, women engaged in sex work (WESW) are more likely to experience physical, emotional, and sexual IPV. This study examines the correlates of IPV among young WESW with their intimate partners in Southern Uganda. We used baseline data from the Kyaterekera project, a 5 year NIH-funded longitudinal study aimed at reducing HIV risks among 542 WESW in Southern Uganda. To examine the factors associated with IPV, we fitted three separate multi-level Poisson regression models for physical, emotional, and sexual IPV, respectively. Average age was 31.4 years, and 54% of the women reported being victims of at least one form of IPV from their intimate partners. Model one assessed correlates of sexual IPV. Being married women (β = .71, 95% CI [0.24, 1.17]), divorced/separated/widowed (β = .52, [0.02, 1.02]), depressed (β = .04, [0.02, 0.05]), and having any sexually transmitted infections (STIs) (β = .58, [0.14, 1.01]) were associated with sexual IPV. Model two assessed correlates of physical IPV. Experience of childhood sexual abuse (β = .12, [0.04, 0.19]) was associated with an increase in physical IPV, and increasing age reduced its occurrence (β = −.02, [−0.04, −0.001]). Finally, model three assessed emotional IPV. Women with higher education (β = .49, [0.14, 0.85]) and symptoms of depression (β = .02, [0.001, 0.04]) had higher risks for emotional IPV. For WESW, IPV presents an additional potential pathway for HIV and STIs acquisition and transmission through a lack of negotiating power for safe sex. Efforts to reduce violence against WESW should be prioritized as a strategy for enhancing the well-being of WESW.
Introduction
Intimate partner violence (IPV) is the most common form of gender-based violence against women. IPV has been recognized as a significant global public health problem that results in high social and economic costs to communities (Ellsberg et al., 2008). The World Health Organization (WHO) defines IPV as any behavior within an intimate relationship that causes physical, psychological, or sexual harm to those in the relationship (WHO, 2012). Globally, about 27% of ever-partnered women aged 15 to 49 years are estimated to have experienced physical, sexual, or emotional IPV in their lifetime (Sardinha et al., 2022). There are regional variations in the prevalence of IPV, with low-income countries reporting higher violence rates than high-income countries (Sardinha et al., 2022). According to the recent WHO global and regional violence estimates, Africa has the highest burden, with 45.6% of the women reporting to have experienced an act of physical or sexual IPV in their lifetime; followed by South-East Asia (40.2%). These figures are above the global prevalence rates of 27% (WHO, 2013).
In Uganda, the focus of this study, the most recent Demographic and Health Survey found that 58.4% of married women reported a past event of emotional, physical, or sexual violence attributed to their spouses (UBOS, 2018). Although many women have experienced some form of IPV from their intimate partners, evidence shows that, women engaged in sex work (WESW) are more likely to experience physical and sexual IPV compared to other women (Carlson et al., 2012; Pack et al., 2014). For example, a study conducted by Muldoon among female sex workers in conflict-affected northern Uganda revealed that over 50% of the women had experienced extreme physical or sexual violence in the previous 6 months (Muldoon et al., 2017). In addition, IPV has been identified as a risk factor for HIV acquisition since the women who are sexually, physically, or emotionally abused are less likely to negotiate for safer sex with their partners. To illustrate, a study conducted by Sileo et al. (2018) among women engaged in transactional sex in Ugandan fishing villages revealed that women with a history of sexual IPV had a fourfold increased likelihood of being HIV positive compared to those with no history of sexual IPV. Similar findings were reported by Schwitters et al. (2015) in their study on gender-based violence among WESW in Uganda. Results highlighted that client demand for unprotected sex during paid sexual acts increases WESW’s susceptibility to HIV and other sexually transmitted infections (STIs) (Schwitters et al., 2015).
Furthermore, criminalization of sex work in some countries, including Uganda, makes WESW more vulnerable to all forms of IPV because of fear of being imprisoned or judged morally (Schwitters et al., 2015). Given the higher risk of HIV among WESW (Baral et al., 2012), efforts to minimize IPV among this vulnerable population need to be prioritized to protect their health and well-being. Yet, in Uganda—the location of the current study—previous studies on IPV have focused more on the prevalence and the factors associated with IPV among women in the general population (Kyegombe et al., 2022; Miller et al., 2021; Okumu et al., 2022; Wandera et al., 2021), with less attention given to WESW. Generally, there is a dearth of literature on the determinants of IPV among WESW. To illustrate, only three articles were identified that focused on IPV among this key population (Schulkind et al., 2016; Schwitters et al., 2015; Sileo et al., 2018). Moreover, these studies were concentrated in urban areas of the country, thus highlighting a need for studies in other places like HIV hot spots across the country. This study examines the factors associated with IPV among WESW across 19 HIV hot spot communities in Southern Uganda.
Theoretical Framework
The study is guided by the theory of gender and power that specifically explains sexual inequality, gender, and power imbalance between men and women (Connell, 1987). The theory of gender and power emphasizes the division of labor and power which favors males at the expense of women; inequities and abuse of authority and control in relationships, and the social norms that hinder women from exercising their rights by approving masculinities (Connell, 1987). The theory has been tested in previous studies to examine HIV-related exposures and patterns of IPV among women in both high- and low-income countries (Okumu et al., 2022; Wingood & DiClemente, 1998).
In the context of WESW, the theory of gender can provide insights into the relationship between IPV and WESW. To illustrate, poverty is a commonly cited reason for WESW’s engagement in sex work, leading to economic dependence on their partners, which can make it difficult to leave abusive relationships, particularly if the partner is the primary source of income. Moreover, just like women in the general population, WESW are as well likely to experience subordination in patriarchal societies where men hold a dominant position, giving them the power to question and control women’s social lives and limiting their mobility. Sex work, however, requires women to move frequently, which can spark arguments and result in violence when women need to leave their homes for work. Overall, the theory of gender’s various structures can be used to provide a comprehensive understanding of the complex relationships between sex work and IPV. We therefore postulate that, the gender-based inequities highlighted by the theory generate different exposures and risk factors that influence WESW’s risk of IPV.
The theory uncovers several factors that shape relationships between women and men that could result in the occurrence of IPV. In the context of Uganda, women’s abilities are constrained by traditional gender norms that give men supremacy (Schulkind et al., 2016). It becomes even worse for WESW, who may not disclose their work to their husbands, and once revealed, it increases their risk of IPV. It is thus critical to understand how contextual factors such as age, education, being unemployed, substance use, asset ownership, condom use, experience of childhood sexual abuse, depression, and having any STIs may shape WESW’s experiences of IPV. This study employs the theory of gender and power to examine the correlates of IPV among WESW in Southern Uganda.
Methods
Study Design and Participants
This study used the baseline data from the Kyaterekera project, a 5-year NIH-funded longitudinal study aimed at reducing HIV risk among WESW in Southern Uganda. The study sought to test the efficacy of adding savings and financial literacy to traditional HIV risk reduction in reducing the new incidence of STI and HIV among a vulnerable key population. Specifically, the Kyaterekera intervention aimed at providing alternative means of safe and sustainable income for WESW to replace sex work, a highly stigmatized and risky form of earning. Using a cluster-randomized experimental design, the study recruited 542 women recruited from 19 HIV hot spots across four districts in Southern Uganda between June 2019 and March 2020.
Each of the 19 hot spots was randomly assigned to the treatment or control condition such that all women selected from a particular hot spot received the same intervention to avoid contamination issues. Women were eligible to participate in the study if they (a) were at least 18 years; (b) reported having engaged in vaginal or anal sexual intercourse in exchange for money, alcohol, or other goods in the preceding 30 days; and (c) reported at least one episode of unprotected sexual intercourse in the past 30 days with a paying, casual, or regular sexual partner. Full details of the study are published in the study protocol (Ssewamala et al., 2019). Blood and vaginal swab samples for Gonorrhea, Chlamydia, Trichomonas, and HIV were collected from all participants who were also connected with antiretroviral therapy, STI treatment, or Pre-exposure Prophylaxis (PrEP), based on need and willingness. Our local health collaborators did the testing, counseling, and referral to treatment for patients (Nabunya et al., 2022)—working with community stakeholders.
Ethics and Informed Consent
All study procedures were approved by the Washington University in St. Louis Institutional Review Board (IRB #201811106), Columbia University IRB (IRB #AAAR9804), and the in-country local IRBs in Uganda, including the Uganda Virus Research Institute (UVRI #GC/127/18/10/690) and the Uganda National Council of Science and Technology (UNCST #SS4828). The research team obtained voluntary written consent from the WESW before participating in the study. The consent forms were translated by a certified translator from the Department of Languages at Makerere University into the local language (Luganda), the most widely used language in the region. Each participant received a copy of the consent form.
Data Collection
Similar to consent forms (see above), all study instruments used in data collection were translated to and administered in Luganda. To ensure that measures were culturally and linguistically appropriate, the study team worked with stakeholders in reviewing the documents to help infuse experiences relevant to WESW. Before engaging with study participants, research assistants completed the research ethics training, including the Collaborative Institutional Training Initiative (CITI) Human Subjects training and Good Clinical Practice training.
Measures
Outcome
The primary outcome was IPV, assessed using a nine-item scale adapted from the Revised Conflict Tactics Scale (Straus et al., 1996). According to the WHO, the most reliable method of measuring the prevalence of any violence is by asking respondents direct questions about their experience of specific acts of violence over a specified period (WHO, 2013). In our study, respondents were asked about their experiences with physical, emotional, or sexual abuse by their intimate partners, spouses, or lovers in the past 90 days.
Using the WHO definition of IPV (WHO, 2012), the outcome was categorized into three types of IPV, including physical, sexual, and emotional/psychological IPV. Physical IPV was measured using items that showed acts such as slapping, hitting, kicking, and beating. Specifically, physical IPV subscale had the following questions. Has your intimate partner, spouse, or lover, (a) twisted your arm or thrown something at you that could hurt, pushed, grabbed, or slapped you? (b) kicked you, slammed you against a wall, beat you up, punched or kicked you, hit you with something that could hurt or burn or scalded you on purpose? (c) broken your bones, caused bruises or other injuries that required medical care because of a fight?
Sexual IPV was measured using items that included acts of forced sexual intercourse and other forms of sexual coercion. Three questions in the sexual IPV subscale were as follows: Has your intimate partner, spouse, or lover, (a) insisted you have sex even though you did not want to? (b) forced you to have sex without a condom? (c) used or threatened to use force to make you have sex with other men in exchange for money or drugs?
Emotional IPV was measured with items that indicated acts such as insults, belittling, constant humiliation, intimidation, threats of harm, and threats to take away children. Three questions were used, including, has your intimate partner, spouse, or lover, (a) called you insulting names such as fat, ugly, slut, or whore, destroyed something that belonged to you or accused you of being a lousy love, (b) prevented you from seeing family or friends, held you captive, stalked you or verbally threatened you, hurt you or your family, (c) deprived you of food, water or sleep? Responses to each question were coded as “1 = Yes” if the participant experienced the act that the item assessed, and 0 = No if the respondent had not experienced the actions described in the item. For each sub-scale, the responses were added together to create a total score, with a theoretical range of 0 to 3 (alpha = .55, .50, and .30 for physical, sexual, and emotional IPV, respectively), while the overall alpha for the IPV scale was .69.
Independent Variables
We ascertained the demographic characteristics of the participants, including their age (continuous), marital status, education level, household size (total number of people in the household, including children and adults), and employment. Other variables included participants’ arrest information in the past 30 days, alcohol use in the past 30 days, asset ownership, depression, condom use communication about intimate partner experiences with childhood sexual abuse, and participants’ biomarker test results. Asset ownership was defined in terms of ownership of financial and physical resources. It was measured using the Asset Index, a scale comprising 21 items that assessed whether the women-owned various items such as land, gardens, house, rental property, small businesses, cars, cell phones, and cattle, to mention a few. We coded each item with a “1” if the participant owned the item and a “0” if the participant did not. We used principal components analysis to generate a latent factor variable for asset ownership.
Depression was measured using a six-item scale from the Brief Symptoms Inventory Survey (Derogatis & Melisaratos, 1983). The instrument assessed whether respondents had experienced any of the depressive symptoms, including (a) thoughts of ending life, (b) feeling lonely, (c) feeling sad, (d) feeling no interest in things, (e) feeling hopelessness about the future, and (f) feelings of worthlessness. Responses were coded from 1 = “Not at all,” 2 = “A little bit,” 3 = “Moderately,” 4 = “Quite a bit,” and 5 = “Extremely.” The theoretical range was 0 to 24 (alpha = .82). Participants were also asked questions about condom use communication to understand how well and confident they would communicate condom use with their intimate partners. Questions on this scale were adopted from the couples’ communication scale (Geeta, 2011). The questions were assessed using a five-item Likert scale ranging from 1 = definitely no to 5 = definitely yes. A higher score indicated ease of communication/discussion about condom use with their customers with a theoretical range of 7 to 35.
Childhood sexual abuse was assessed using a modified version of the Childhood Sexual Abuse (CSA) Interview formulated by Finkelhor (1979) and Sgroi et al. (1982). This version of CSA was based on a previous study examining WESW and use drugs in Central Asian country (Witte et al., 2015). The eight-item scale assessed the sexual experiences that participants might have experienced with someone at least 5 years older than the respondent, including a relative, family friend, or stranger. Some of the questions were as follows: “When you were 18 years old or younger, did an adult or someone at least 5 years older than you touch or fondle you in a sexual way?” and “When you were 18 years old or younger, did a relative attempt oral, anal, or vaginal intercourse with you?” Responses to the Items were coded as “1” if participants responded yes to any of the questions asked and “0” if they responded no. Responses were then summed up and became a continuous variable ranging from 0 to 8, with a higher score indicating higher child sexual abuse. The Cronbach’s alpha was .79 for the eight items. We also included participants’ biological test results when confirmed positive from a laboratory test, including three STIs, namely, Gonorrhea, Trichomonas, or Chlamydia, and HIV.
Statistical Analysis
We used Stata version 17 for all the analyses. Continuous variables were summarized using means and standard deviations, while categorical variables were summarized using percentages and proportions. To examine the correlates of IPV, we fitted separate multi-level Poisson regression models corresponding to the three forms of IPV (physical, emotional, and sexual). In each model, we fitted the socio-demographic variables, including (age, marital status, household size), childhood experiences of sexual abuse, employment status, arrest history, alcohol use in the past 30 days, asset ownership, condom use, communication with an intimate partner, symptoms of depression, HIV test results, and whether participants had any STIs. In fitting the multilevel models, level one included IPV scores and participant-level predictor variables, while level two included clusters at the level of the hot spots. We initially ran null model without any predictor variables to determine the level of clustering from the hot spots, after which we included the independent variables in the full models. In all the analyses, Huber–White cluster-adjusted confidence intervals were reported, and all p values below .05 were considered significant.
Results
Sample Characteristics
A total of 542 WESW were recruited in the study, of whom 54% reported having been victims of at least one form of IPV from their intimate partners including spouses, or lovers. In particular, 25% reported having experienced sexual IPV, while 29% and 28% of the women experienced physical and emotional IPV, respectively. The average age was 31.4 years (SD = 7.18). Most participants (61%, n = 331) were divorced/widowed/separated from their partners, and 63.5% (n = 344) had achieved up to primary education. The average household size was 3.4 (SD = 2.19), and more than half (53.7%) of the women lived in small towns. Details are included in Table 1.
Characteristics of 542 WESW.

Note. BSI = Brief Symptoms Inventory; STI = sexually transmitted infection; WESW = women engaged in sex work.
Table 2 presents the results for the prevalence of the different forms of IPV. Overall, 136 (25.1%) participants reported having experienced sexual IPV, while 156 (28.8%) and 155 (28.6%) reported experiencing physical and emotional IPV, respectively.
IPV among 542 WESW in Uganda.
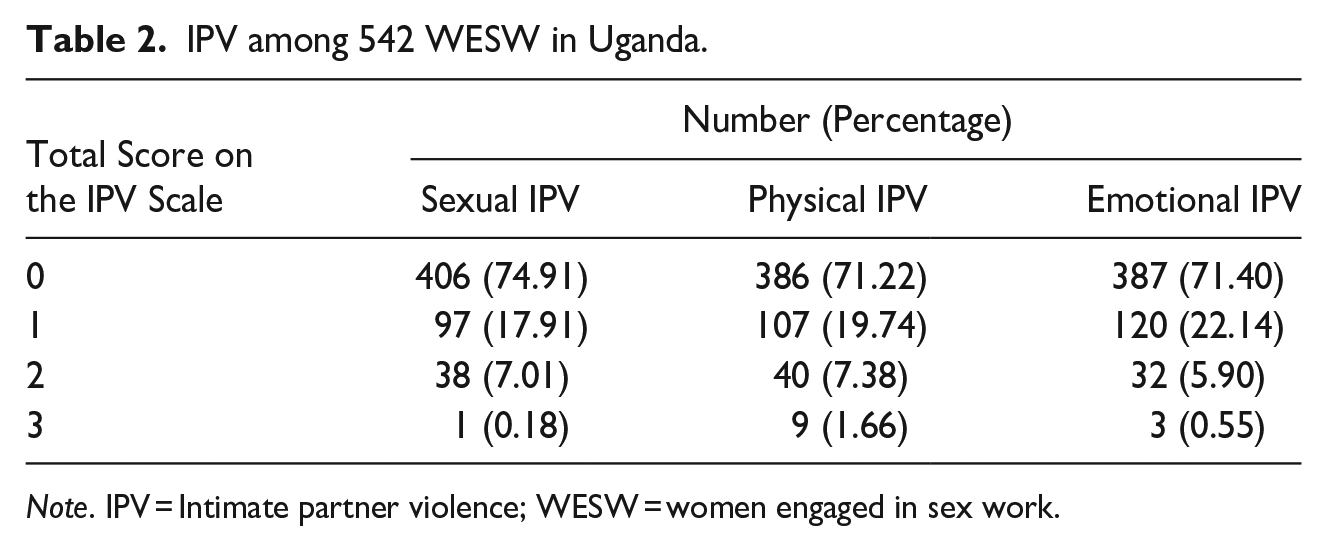
Note. IPV = Intimate partner violence; WESW = women engaged in sex work.
Correlates of IPV
Table 3 presents results from the Poisson regression models for the correlates of IPV among WESW. The first model assessed the correlates of sexual IPV. Results showed that, being married (β = .71, 95% CI [0.24, 1.17], p = .003), divorced/separated/widowed (β = .52, [0.02, 1.02], p = .040), depressed (β = .04, [0.02, 0.05], p < .001), and having STIs (β = .58, [0.14, 1.01], p = .010) were associated with an increase in sexual IPV. Model 2 examined the correlates of physical IPV. Marital status was also significant in the model. Specifically, being divorced/separated/widowed (β = .53, [0.11, 0.95] p = .013) was associated with increased likelihood of physical IPV. Similarly, women who reported a record of arrest (β = .34, [0.07, 0.61], p = .012) and had experience of childhood sexual abuse (β = .12, [0.04, 0.19], p = .002) were more likely to experience physical IPV. In contrast, increasing age was associated with a reduction in physical IPV (β = −.02, [−0.04, −0.001], p = .038).
A Multi-Level Mixed Effects Poisson Regression Models Showing the Determinants of IPV Among 542 WESW.
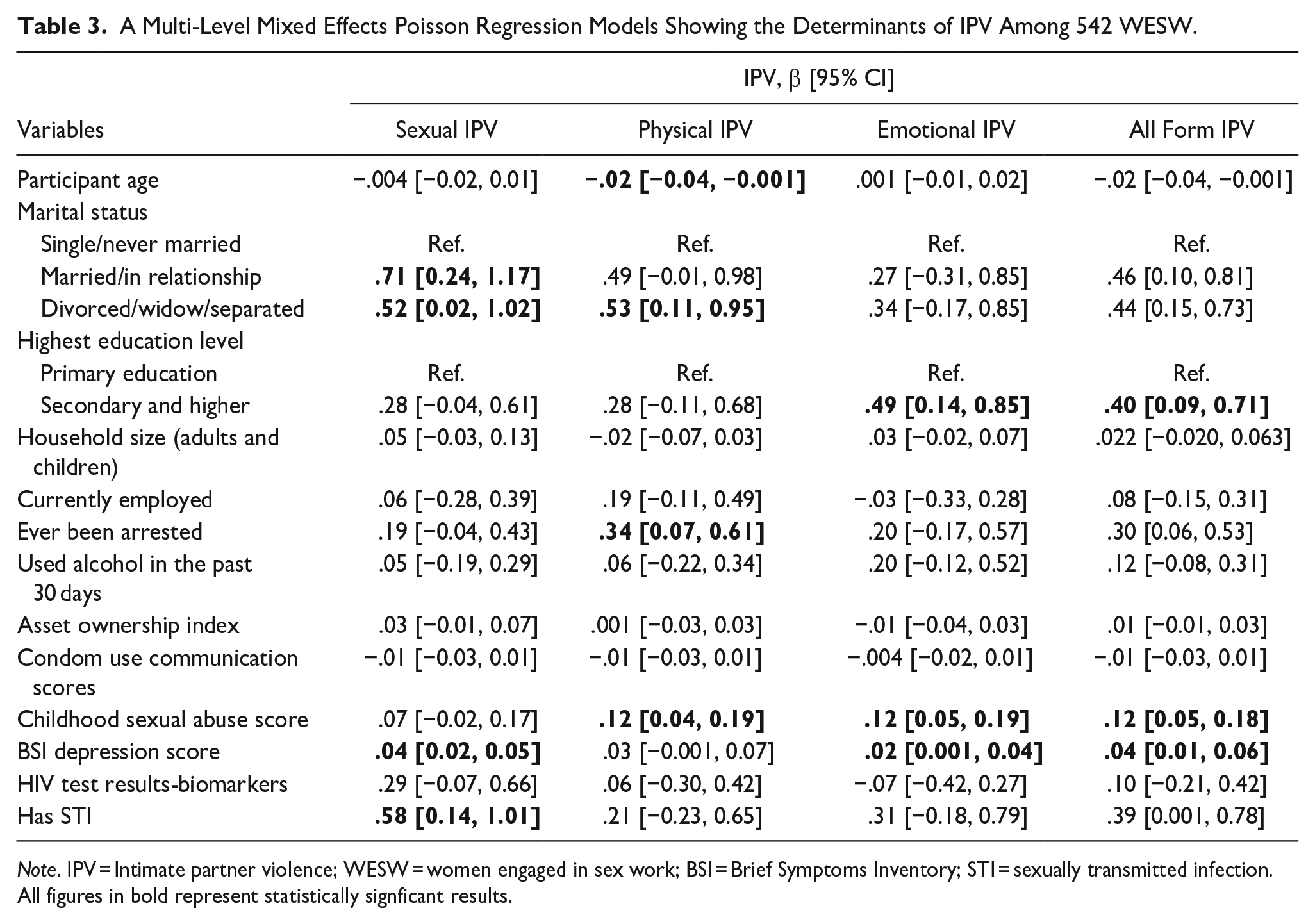
Note. IPV = Intimate partner violence; WESW = women engaged in sex work; BSI = Brief Symptoms Inventory; STI = sexually transmitted infection.
All figures in bold represent statistically signficant results.
Model 3 assessed factors associated with emotional IPV. Results showed that participants’ education was significantly associated with emotional IPV. In particular, women with secondary or higher education were more likely to experience emotional IPV than those with low education levels (β = .49, 95% CI [0.14, 0.85], p = .007). In addition, women with past experiences of childhood sex abuse (β = .12 [0.05, 0.19], p = .001) and symptoms of depression (β = .02 [0.001, 0.04], p = .039) had higher chances of experiencing emotional IPV.
Discussion
Guided by the theory of gender and power (Connell, 1987), this study examined the correlates of IPV among WESW in Southern Uganda. Findings indicated that 54% of the women experienced some form of IPV. Specifically, sexual IPV (25%) was the least prevalent, while 29% and 28% of the women experienced physical and emotional IPV, respectively. Other studies conducted among WESW have reported a range of IPV prevalence rates. For example, results from Wilson et al., among women engaged in transactional sex in Kenya indicated that 10.6% experienced physical, 10.1% emotional, and 3.6% sexual IPV (Wilson et al., 2016). On the other hand, Sileo et al. showed that 62% and 51% of the women in their sample had experienced sexual and physical IPV, respectively (Sileo et al., 2018). Hence, findings suggest the need for addressing IPV as a public health issue, which can potentially have a long-term impact on the society if not given urgent attention.
In our first model that examined correlates of sexual IPV, results indicated that married, divorced/separated/widowed women were more likely to experience sexual and physical IPV than women who are single or never married. Since married women have a higher likelihood of being in contact with their intimate partners, it is possible that their chances of experiencing abuse is high. On the other hand, the conservative gender norms give power to men in families while marginalizing women. For instance, in most patriarchal societies, including Uganda, where the study was conducted, men are regarded as superiors and heads of households with more power in their hands (Okumu et al., 2022). Such power imbalances, as highlighted by the theory of gender and power, prohibit men from admitting to being victims of IPV to maintain their masculinity as defined by traditional cultural norms (Yan & Karatzias, 2020).
A mixed methods study by Uribbali and colleagues among WESW in Mexico revealed that power dynamics was a great source of conflict among couples. Specifically, men were not comfortable taking orders from women even when the highest percentage of household income was provided by women (Ulibarri et al., 2019). Similarly, a study conducted by Okumu and colleagues on the patterns of IPV among married women in Uganda indicated that, ever-married women face multiple risks, such as limited decision-making power and low levels of education, that expose them to severe forms of sexual and physical IPV (Okumu et al., 2022). Thus, women’s participation in decision-making in the family may protect them from experiencing sexual and physical violence (Logie et al., 2019). Hence, intervention strategies must challenge existing cultural norms and promote gender equitable norms, which could help address IPV against WESW.
Furthermore, depression was associated with increased sexual and emotional IPV among WESW. Symptoms of depression, such as feeling sad, worthless, and hopeless (Derogatis & Melisaratos, 1983) may affect women’s ability to settle conflicts in a relationship which opens room for IPV. The findings of an earlier study indicated that severe depressive symptoms were associated with sexual difficulties and dissatisfaction among women as it affected their mood and interest (Montejo et al., 2018), leading to forced sex. Similarly, a systematic review of longitudinal studies revealed that depressive symptoms increased the odds of IPV in women (Devries et al., 2013). There is, however, a bidirectional relationship between IPV and depression. For example, women exposed to IPV are more likely to report increased depressive symptoms, and women who report severe depressive symptoms are likely to experience IPV (Alangea et al., 2018; Devries et al., 2013). Thus, the programing implication here is that addressing depression and its associated outcomes among WESW may help reduce sexual and emotional IPV. We suggest, therefore, promoting mental health programs that target WESW who are experiencing depression but also victims of IPV.
In addition, early experiences of childhood sexual abuse were associated with both physical and emotional IPV. This could be related to the memories, which may affect women’s psychological well-being, and put them at a greater risk of re-victimization. Similar findings have been documented in studies that women who experience childhood sexual abuse are at increased risk of sexual violence in adulthood from their intimate partners, as they consider it acceptable behavior (Alangea et al., 2018; Parcesepe et al., 2015). Findings of a WHO multi-county study on women’s health and domestic violence indicated that women in relationships where both she and her partner were abused in childhood are at a greater risk of IPV in adulthood (Abramsky et al., 2011). The implication of this finding is that in order to address and prevent re-occurrence of sexual IPV in adulthood, interventions aimed at addressing childhood abuse should respond with a need to the children who have witnessed sexual IPV. This could help in reducing their risk of violence in later life.
Contrary to other studies that have revealed an association between higher levels of education and reduced IPV experience (Abramsky et al., 2011; Amegbor & Pascoe 2021; Gubi et al., 2020), our study results indicate that WESW with higher levels of education were more likely to experience physical and sexual forms of IPV. On one hand, higher education empowers women and improves their social status. Hence, women gain more control over their intimate partner’s behaviors and sexual decisions, making them less vulnerable to IPV (Logie et al., 2019). On the other hand, the improved status of women may threaten some men, thereby increasing tension in couples, resulting in male-perpetrated IPV to regain their power (Peralta et al., 2010). The implication for this finding is that efforts should be made to address the gender-power differences that make men feel threatened by women’s improved social status and lead to IPV perpetration.
Furthermore, findings indicated that age was protective against physical IPV. Specifically, an increase in age was associated with a decrease in physical IPV. These findings are in line with previous studies. For example, Black et al. studied the prevalence and correlation of IPV against women in northern Uganda. The study found that age was a significant determinant of IPV. In particular, younger women were more likely to experience IPV than older women (Black et al., 2019). There are several plausible explanations for this relationship. For instance, it is possible that as people age, they may develop better coping mechanisms, communication skills, and emotional regulation, which can reduce the likelihood of physical violence in intimate relationships. In addition, as relationships mature, couples may develop more equitable power dynamics and learn to negotiate conflicts more effectively, which can further decrease the potential for physical violence. Social and cultural norms may also discourage physical violence in intimate relationships, and these norms may become more firmly established as people age. These factors suggest that aging may bring about a reduction in physical IPV. However, it is important to recognize that other forms of abuse may still occur in intimate relationships at any age. The implication for this finding is that developing appropriate interventions that target younger WESW is essential for their health and physical well-being.
Women who reported having STIs, including Gonorrhea, Trichomonas, Chlamydia, and HIV were more likely to experience sexual IPV. This could be attributed to women’s lack of negotiating power for safe sex in relationships, which puts women at higher risk of contracting STIs, including HIV. El-Bassel and her colleagues’ recent report sheds light on the intricate relationship between IPV and the risk of contracting STIs and HIV. The report identifies sexual violence as the primary biological mechanism linking IPV to these health issues, as it leads to inconsistent condom use due to a lack of negotiation power (El-Bassel et al., 2022).
Furthermore, Kyriakakis and colleagues’ research on the experiences of women engaged in transactional sex work in Barbados supports previous studies highlighting the detrimental effects of IPV on women’s sexual health. The study found that IPV significantly impaired women’s ability to negotiate condom use with their intimate partners, making them more susceptible to contracting HIV and other sexually transmitted diseases (Kyriakakis et al., 2023). These findings underscore the critical role that gender, and power dynamics play in sexual health, as male dominance in relationships can impede women’s ability to negotiate for safe sex practices, leaving them at a higher risk of contracting STIs and HIV/AIDS. This is a key component of the theory of gender and power. Given the nature of their work, WESW are at a higher risk of experiencing sexual IPV. Health interventions that encourage screening and treatment for STIs and HIV among WESW should be promoted.
Limitations
This analysis is cross-sectional, and as a result, we cannot infer a causal relationship between the factors discussed in this paper and IPV. Future studies should integrate longitudinal measures to ascertain the determinants of IPV. In addition, the measures related to IPV were self-report. Moreover, the participants were asked about these incidents since turning age 18. Some reported incidences could have been experienced with previous intimate partners, which may lead to a misclassification of the partnerships. Nevertheless, given the sensitivity and stigma around IPV, women might have underreported their experiences with IPV. For example, the WHO multi-county study revealed that interviewer factors, as well as privacy and context of the interview, could have affected women’s reporting of their experiences with IPV (Abramsky et al., 2011).
Conclusions and Implications
IPV is both a driver and a consequence of engaging in sex work among women (Wilson et al., 2016). Hence, exposure to IPV has significant effects on women’s health and well-being. The WHO report indicates that women who have been physically or sexually abused by their intimate partners are more likely to be exposed to STIs, including HIV, than those who have never experienced IPV in their lifetime (WHO, 2013). For WESW, IPV presents an additional source of violence and a potential pathway for HIV and STI acquisition and transmission through a lack of negotiation power for safe sex. Our study examined the correlates of IPV among WESW in Southern Uganda. Findings revealed that marital status, educational level, age, experience of childhood sexual abuse, depression, and arrest history were associated with IPV. Our findings add to the dearth of literature in the country investigating the factors associated with IPV among WESW. This population is neglected in the prevention efforts for IPV but is disproportionately vulnerable to IPV-associated health outcomes. Hence, the double burden of IPV and HIV risk among WESW necessitates interventions aimed at preventing the occurrence of IPV and enhancing the well-being of WESW. That is to say, programs aimed at promoting women empowerment should be promoted to challenge gender norms and attitudes that belittle women and make them vulnerable to IPV.
Footnotes
Acknowledgements
We would like to acknowledge and thank the women employed by sex work who participated in this study and whose experiences contributed to the findings of this paper. We also thank our research team at the International Center for Child Health and Development-Masaka field offices for their support in collecting the data. Our thanks are also due to our research collaborators and partners, including Rakai Health Sciences Program, TASO Masaka, Villa Maria, Reach the Youth Uganda, the Community Collaborative Board, and the study’s Data Safety and Monitoring Board for their respective support to the Kyaterekera project. Correlates of Intimate Partner Violence among Young Women Engaged in Sex Work in Southern Uganda.
Authors’ Contributions
FMS and SSW wrote the grant and obtained funding for the study. JN prepared the first draft of the manuscript with input from SK. SK and JN conducted the analysis. JK, RM, EN, and FN coordinated the field activities, including data collection, cleaning, and management. All authors reviewed the manuscript and made significant contributions to the manuscript. They also approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by the National Institute of Mental Health (NIMH) under award number R01MH116768 (MPIs: Fred M. Ssewamala, PhD & Susan S. Witte, PhD). NIMH had no role in the study design, data collection, analysis, interpretation of findings, and preparing this manuscript. The content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the NIMH or National Institute of Health (NIH).
Ethical Approval
All study procedures were approved by the Washington University in St. Louis Institutional Review Board (IRB #201811106), Columbia University IRB (IRB #AAAR9804), and in-country local IRBs in Uganda, including the Uganda Virus Research Institute (UVRI #GC/127/18/10/690) and the Uganda National Council of Science and Technology (UNCST #SS4828).
Availability of Data and Materials
The datasets analyzed during the current study are available through the corresponding author on reasonable request.