
Abstract
Residential mobility remains an underexplored yet critical construct that may influence the risk of violence among women who exchange sex. This study examined the longitudinal relationship between residential mobility and experience of client-perpetrated physical or sexual violence among women who exchange sex in Baltimore, Maryland. Participants were at least at 18 years of age, were cisgender women, reported having engaged in transactional sex three or more times within the last 3 months, and were willing to be contacted for 6-, 12-, and 18-month follow-up visits. Analyses of responses from 370 women who exchange sex participating in at least one study visit were conducted. Unadjusted and adjusted Poisson regression models of the association over time between residential mobility and recent experience of physical or sexual violence were fit. Generalized estimating equations with an exchangeable correlation structure and robust variance estimation were used to account for clustering of participants’ responses over time. Findings demonstrated that those who had lived in at least four places in the past 6 months had a 39% increased risk of client-perpetrated physical violence (aRR: 1.39; 95% CI: 1.07–1.80; p < .05) and a 63% increased risk of sexual violence (aRR: 1.63; 95% CI: 1.14–2.32; p < .01) compared to their less-mobile counterparts. These findings provide necessary evidence of correlations over time between residential mobility and experience of client-perpetrated violence among women who exchange sex. Strengthening our understanding of how residential mobility intersects with violence is critical for the development of public health interventions that are relevant to women’s lives and needs. Future interventions should explore including residential mobility, a critical pillar of housing instability, with efforts to address client-perpetrated violence.
Keywords
Introduction
Women who exchange sex are at increased risk of experiencing physical and sexual violence globally (Deering et al., 2014). Across studies included in their systematic review, Deering et al. (2014) found that from 19% to 44% of women who exchange sex experienced occupational physical violence in the past year; similarly, 15% to 31% experienced occupational sexual violence. In Baltimore, a city located in Maryland, USA, the prevalence of physical and sexual violence among women who exchange sex is high, perpetrated by clients as well as non-paying partners and police (Decker et al., 2013; Footer et al., 2019; Lim et al., 2019). Such violence is often associated with barriers to negotiating condom use, reproductive coercion, as well as increased risk of anxiety, depression, HIV, and sexually transmitted infections, among other health outcomes (Baral et al., 2012; Beattie et al., 2020; Decker et al., 2016, 2020; Li et al., 2014; Park et al., 2019; Shannon et al., 2009; Wirtz et al., 2015).
Client-perpetrated violence is deeply influenced by the social, physical, and structural environments in which women live and work (Decker et al., 2016; Deering et al., 2014; Lazarus et al., 2011; Leddy et al., 2018; Nestadt et al., 2020; Shannon & Montaner, 2012; Shannon et al., 2008). Factors such as the criminalization and policing of sex work; food, economic, and material constraints and insecurity; gender inequity; substance use; and aspects of women’s identities, including sexual minority identity, have been shown to be significantly associated with experiences of both physical and sexual violence among women who exchange sex (Beattie et al., 2020; Deering et al., 2014; Glick et al., 2020, 2022; Platt et al., 2018; Scorgie et al., 2012). Mobility plays a critical role in shaping the environments in which women exchange sex, with the potential to disrupt and shift the spaces people move through and their social interactions. Mobility among women who exchange sex can be a response to economic vulnerability, housing instability, sex work-related stigma and discrimination, restrictive laws and policies that criminalize sex work, or simply an act to search for clients (Amram et al., 2019; Saggurti et al., 2012; Scorgie et al., 2012). As a result, mobility can shift the social and structural contexts and environments in which women exchange sex, leading to both new economic opportunities (Goldenberg, Chettiar, et al., 2014) as well as exposure to settings where they are less familiar, settings where they have fewer support systems or networks, or risky environments that can increase their exposure to violence (Deering et al., 2014; Lazarus et al., 2011; Platt et al., 2018) as well sex trafficking (Burckley et al., 2023; Chohaney, 2016; Goldenberg, Silverman, et al., 2014).
Mobility has been conceptualized in numerous ways across spatial, temporal, and social domains, encompassing micro-level movements, residential mobility, as well as geographic mobility. Micro-level mobility includes people’s daily movements or spatial patterns (Felker-Kantor et al., 2021) within and across “activity spaces,” or the physical or social spaces (e.g., places where they exchange sex as well as other sites) where people’s daily activities occur (Kwan, 2013; Matthews & Yang, 2013). Residential mobility, the focus of this study, includes the movement of people from one residence to another—typically over shorter distances (Coulter et al., 2016). Finally, geographic mobility often occurs over larger spatial areas or for longer durations (Davey et al., 2019). Mobility, whether at the micro-, residential, or geographic level, influences and is influenced by the same risk environments in which women live and work, which simultaneously influence their exposure to violence.
There is substantial variation in the language used to describe residential mobility, such as transience (Jongbloed et al., 2015) or instability (Reed et al., 2011), and how it is defined and measured. In the United States, residential mobility is often understood as a key dimension of one’s housing stability, linked with neighborhood stability, and changeable over time (Coulton et al., 2012; Frederick et al., 2014). As Swope and Hernández (2019) outline in their conceptual model of housing as a determinant of health equity, housing instability is influenced by four pillars: the cost, conditions, consistency, and context of the places where a person spends their time (Swope & Hernández, 2019). Disruptions in place—for different periods of time, across different locations—that occur with residential mobility have the potential to influence the consistency or stability of a person’s housing over time. As a result, measures of residential mobility such as eviction or number of places lived or slept in over a certain period of time are often described as components of housing instability.
Research in the United States and Canada has explored housing instability among women who exchange sex, highlighting experiences of eviction, homelessness, or poor housing conditions (Footer et al., 2020; Glick et al., 2020; Lazarus et al., 2011; Lim et al., 2019; Lyons et al., 2021; Sherman et al., 2019; White et al., 2020). Homelessness has been shown to be associated with experiences of violence among women who exchange sex (El-Bassel et al., 2001; Shannon et al., 2009) as well as other aspects of women’s lived realities, including sexual minority identity, food insecurity, and characteristics of sex work such as earlier age of entry into sex work or frequency of sex work (Footer et al., 2020; Glick et al., 2020; Lim et al., 2019).
Within the existing literature on housing instability, residential mobility remains an underexplored yet critical construct that may influence risks of violence among women who exchange sex. While residential mobility among women who exchange sex is significantly associated with client-perpetrated violence (Goldenberg, Chettiar, et al., 2014; Hendrickson et al., 2018, 2021; Rocha-Jiménez et al., 2016), depression (Patel et al., 2016), and HIV risk (Jongbloed et al., 2015; Ramesh et al., 2012; Saggurti et al., 2012), there remains a paucity of research that has examined these associations longitudinally (Morris et al., 2018). Furthermore, few studies have considered residential mobility in conjunction with other measures of housing instability such as recent experiences of eviction, homelessness, or housing conditions to examine how such co-occurring events may influence the association between residential mobility and violence. To fill these gaps, this study examines characteristics associated with residential mobility as well as the longitudinal relationship between residential mobility and experiences of client-perpetrated physical or sexual violence among women who exchange sex in Baltimore, Maryland, a city with high rates of housing instability and violence experienced by women who exchange sex (Sherman et al., 2019).
Methods
This analysis draws on baseline, 6-month, and 12-month follow-up data collected from participants in the Enabling Mobilization, Empowerment, Risk Reduction, and Lasting Dignity (EMERALD) study. EMERALD, described previously (Sherman et al., 2019; Silberzahn et al., 2021), is a prospective two-group comparative nonrandomized trial designed to evaluate the SPARC (Sex Workers Promoting Action, Risk Reduction, and Community Mobilization) intervention. SPARC is a community-level structural intervention that includes community outreach and a drop-in center and is designed to reduce STI and HIV transmission among women who exchange sex living in Baltimore (Silberzahn et al., 2021).
Study Participants and Data Collection
EMERALD participants were recruited using time–location sampling between September 2017 and January 2019 in Baltimore from 10 recruitment areas where sex work is common. Eligibility criteria included if people were at least at 18 years of age, were cisgender women, reported having engaged in transactional sex (sold or traded oral, vaginal, or anal sex for money, food, or drugs) three or more times within the last 3 months, and were willing to be contacted for 6-, 12-, and 18-month follow-up visits (Sherman et al., 2021; Silberzahn et al., 2021). As SPARC, the intervention that EMERALD evaluated, was focused initially on addressing the needs of cisgender women, the EMERALD cohort recruitment focused on cisgender women.
Surveys were administered using audio computer-assisted self-interviewing (ACASI) software. Questions focused on sociodemographic characteristics, housing situations, substance use, mental health, factors related to sex work, experiences of gender-based violence, and other health outcomes. Participants were tested for HIV, gonorrhea, and chlamydia at each study visit. Participants responded to surveys on individual tablets, which enabled them to answer questions privately and protected the confidentiality of their responses. This meant that participants did not have to discuss sensitive issues, such as experiences of gender-based violence, with interviewers. Study staff had experience working with women who exchange sex and were trained to recognize when a participant needed support or assistance during data collection.
The study team had extensive experience working with women who exchange sex in Baltimore. The team developed a list of local resources that were closest to recruitment sites, including violence-specific resources, general case management, and healthcare. In addition, as data were collected as part of an evaluation of the SPARC intervention, the aforementioned resource lists were adapted for intervention and control areas of the project. In intervention areas, participants were also encouraged to visit SPARC, which offers case management, mobile outreach, and trauma-informed services. Referrals to area-specific resources were provided to participants upon request.
Written informed consent was required from all recruited individuals prior to their participation in the EMERALD study. Participants were compensated with a $70 gift card for participation in the baseline and $40 for each follow-up visit (Silberzahn et al., 2021). The study was approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board.
The study team collected and updated participants’ contact information through in-depth locator forms to facilitate cohort retention through participant outreach. Other approaches to maintain retention, such as branded intervention materials and real-time monitoring of publicly available demographic data (e.g., mobility, incarceration, or mortality) to track changes in study participants’ living situations, were also used (Silberzahn et al., 2021).
The present analysis included women who exchange sex who participated in at least one round of the EMERALD study (n = 376). After select observations were excluded from analysis as described below, the final analysis was based on observations from 370 women who exchange sex.
Measures
Recent experience of client violence
The primary outcome of interest for the current analysis was any recent (past 6 months) experience of physical violence perpetrated by a client, defined as any recent experience versus none. The analysis is limited to client-perpetrated violence, rather than violence perpetrated by others, to examine how residential mobility influences the work and risk environments where women exchange sex. Physical violence was defined as having been hit, punched, slapped, otherwise physically hurt, or threatened with a weapon. The secondary outcome of interest was any recent (past 6 months) experience of client-perpetrated sexual violence (any vs. none). Sexual violence was defined as a client using physical force (e.g., hitting, holding down, or use of a weapon) to force sex against the participant’s will. Violence measures were adapted from the Revised Conflict Tactics Scale (Straus et al., 1996) and asked at each time point.
Residential mobility
The primary explanatory variable of interest was recent residential mobility, defined as the number of places an individual reported staying or living in the past 6 months. Recent residential mobility was asked at each time point and was categorized to compare those with high mobility (four or more places) to those with less mobility (fewer than four places lived). The cutoff for this dichotomous variable was set using the median-split of participants’ responses to avoid sparse categories in subsequent bivariate and multivariate analyses. This cutoff is also consistent with previous literature examining the effects of residential mobility on health outcomes among women who do not exchange sex (Jelleyman & Spencer, 2008; Morris et al., 2018). “Don’t know” and “refused to respond” responses were coded as missing for the purposes of analysis (n = 24 observations). A subset of 30 observations across 26 participants reported living in zero places in the last 6 months. Further investigation showed that 5 of these 30 observations coincided with reports of recent homelessness, but this was not true for all. Participants who reported living in zero places also reported, at other time points, living in 1–44 places in the past 6 months. As there was no clear or distinct pattern comparing these responses to other housing instability-related measures or to residential mobility at other time points, these observations were excluded from the analyses presented here.
Other covariates of interest
Other covariates of interest included time-varied factors (measured at each time point) and fixed factors (measured at baseline only). These covariates included (1) additional housing instability measures, (2) sociodemographic characteristics, (3) additional structural vulnerabilities, (4) factors related to sex work, and (5) substance use and mental health. These covariates were considered in light of previous research suggesting their important role in the mobility of women who exchange sex or experiences of violence.
Additional housing instability measures were both time-varied and fixed. Fixed housing instability measures included length of time living in Baltimore at baseline (more than 5 years, 1–5 years, or less than 1 year/not living in Baltimore) and experience of eviction within the last 6 months at baseline (any vs. none). Time-variant housing instability measures included recent homelessness (any within the last 6 months vs. none) and place where the participant reported staying most of the time in the last 6 months. Responses included their own/rented place, a family member’s place, a non-family member’s place, or unstable locations (e.g., shelter, transitional housing, street, park, car, abandoned/vacant building, or other location).
Sociodemographic characteristics of interest were fixed factors, measured at baseline, and included age (18–29, 30–39, 40–49, or 50+), race/ethnicity (Black, White, or other), education (less than high school, high school graduate/GED, or some college or more), and sexual orientation identity (sexual minority—gay, lesbian, bisexual, queer, or same gender loving vs. heterosexual). Additional structural vulnerabilities included both fixed and time-varied factors. Two measures of financial insecurity were fixed factors: any savings (vs. none) at baseline and any debt (vs. none) at baseline. Food insecurity was a time-varied factor, defined as self-reported hunger at least weekly versus less than weekly. Factors related to sex work were both time-variant and fixed. The fixed factors related to sex work were (1) frequency of sex work in the past 3 months (1–3 times a month, 1–6 times a week, or daily) at baseline and (2) whether new clients were found on the street or in public places like parks in the past 6 months (yes vs. no) at baseline. Time-variant factors included (1) whether participants reported exchanging sex as a source of income (yes vs. no) and (2) the number of clients in the past week (4 or more clients vs. 0–3 clients). Recent substance use measures were time-variant and based on self-reported use of heroin, crack/cocaine, or opioids, or having injected any drugs within the past 6 months (any vs. none). Mental health measures included depression and post-traumatic stress disorder (PTSD). Fixed factors were self-reported diagnosis with a major depressive disorder at baseline (any vs. none) and PTSD symptom severity at baseline (severe symptoms vs. less severe), defined using a cutoff score of 33 or higher on the PTSD Checklist for DSM-5 (PCL-5) (Weathers et al., 2013). Self-reported depressive symptom severity (severe vs. less severe) was time-variant and based on responses to the Patient Health Questionnaire (PHQ)-9 comparing scores of 12 or higher versus <12 (Kroenke et al., 2001).
Statistical Analysis
Descriptive statistics were used to describe recent experiences of violence, residential mobility, as well as other covariates of interest outlined above. Trends in participants’ residential mobility and experiences of violence across the three survey rounds were examined graphically. Graphs were then used to depict average predicted values and 95% confidence intervals from unadjusted Poisson regression models of (1) residential mobility over time, (2) recent experience of physical violence over time, and (3) recent experience of physical violence over time, fit using generalized estimating equations (GEE) with an exchangeable correlation structure and robust variance estimation to account for clustering of participants’ responses over time (Zou & Donner, 2013). This Poisson GEE model with strong variance estimation is robust for deviation from distribution assumption including overdispersion in the data.
The analysis included two steps. First, to better understand the primary explanatory variable of interest, identify potential confounders, and inform interpretation of results, factors associated with residential mobility were examined separately by survey round using χ2 tests. Second, factors associated with recent experiences of client violence were examined separately by survey round using χ2 tests considering physical and sexual violence separately. Unadjusted and adjusted Poisson regression models of the association over time between residential mobility and recent experience of physical or sexual violence were then fit using GEE with an exchangeable correlation structure and robust variance estimation to account for clustering of participants’ responses over time. Selection of covariates for the initial full multivariate models was conducted separately for each outcome. Covariates were retained for the initial full models for each outcome if they were significantly associated with their respective outcome of interest in unadjusted bivariate Poisson regression models based on a cutoff of p = .2. A manual backward model building approach was utilized to fit the final model, with Wald tests used to determine those variables that contributed to the final reduced model based on a cutoff of p = .2. The final model created using this approach was compared to that using a cutoff of p = .1 and to those proposed by automatic forward and backward stepwise selection. Collinearity of covariates used in the final adjusted models was compared based on variance inflation factors (VIFs) as well as polychoric correlation matrices. In final models, recent experience of homelessness and recent use of heroin were dropped due to high collinearity with other covariates. All VIFs in final models presented here were below two, and polychoric correlation matrices showed correlation coefficients lower than 0.57 overall, suggesting lack of significant collinearity (Vatcheva et al., 2016). Cui’s quasi-likelihood under the independence model criterion (QIC) was used to compare models fit using GEE to determine the set of covariates included in final models. QIC values were similar across models compared, with the final models developed using the manual backward model building approach with a cutoff of p = .2 having the lowest QIC values for both outcomes of interest.
The final models presented here examined the associations between residential mobility and violence and adjusted for survey round, study group (intervention vs. control), as well as the following covariates: aspects of housing instability (length of time living in Baltimore at baseline, place where stayed most of the time, and recent eviction at baseline), sociodemographic characteristics (sexual orientation identity), additional structural vulnerability (recent experience of hunger, any savings at baseline, and any debt at baseline), factors related to sex work (exchanging sex as a source of income and number of clients), and substance use and mental health (use of crack/cocaine or opioids, and PTSD symptomology).
To account for loss to follow-up, a sensitivity analysis was conducted where adjusted models examining factors associated with recent experience of physical or sexual violence from clients were fit using the full sample and compared to results fit using a restricted sample limited to those who participated in all three survey rounds (n = 193). To examine the potential impact of overdispersion of the data, a sensitivity analysis was conducted where results from final adjusted Poisson GEE models were compared with results from final adjusted population-averaged negative binomial models.
Results
Participants’ Characteristics at Baseline
Participants’ housing instability, sociodemographics, structural vulnerability, substance use, and mental health at baseline are shown in Table 1, overall and stratified by residential mobility. Fifty-two percent of participants reported high recent residential mobility at baseline. Most reported living in Baltimore for more than 5 years (71%). While only 7% had a recent eviction, two-thirds (68%) said that they had recently experienced homelessness. Those reporting high residential mobility more commonly reported recent homelessness (92% vs. 43%, respectively; p < .001) and staying in unstable locations than did their less-mobile counterparts (63% vs. 21%, respectively).
Sociodemographic Characteristics, Housing Instability, Additional Structural Vulnerabilities, Factors Related to Sex Work, Substance Use, and Mental Health by Participants’ Residential Mobility at Baseline (N = 370).

Reported p-value based on Pearson’s χ2 tests.
n = 2 missing at baseline.
n = 3 missing at baseline.
n = 2 missing at baseline.
n = 1 missing at baseline.
n = 8 missing at baseline.
p < .001. **p < .01. *p < .05. ^p < .1.
Participants reporting high residential mobility at baseline tended to be younger, with a larger proportion of mobile participants 18 to 29 years of age (28% vs. 18%, respectively). Most participants were White (57%) and had less than a high school graduation (46%), and nearly one-third reported a sexual minority identity (32%). There were no statistically significant differences in residential mobility by race/ethnicity, education, or sexual orientation identity.
More than 62% of participants at baseline described experiencing hunger at least weekly, which was more common among those with high residential mobility (Table 1). Participants with high residential mobility also more often reported exchanging sex as a source of income (80% vs. 64%, respectively; p = .001), exchanging sex daily (61% vs. 44%, respectively), having four or more clients in the past week (78% vs. 59%, respectively; p < .001), and finding new clients on the street or in public places like parks (88% vs. 77%, respectively; p = .004). A larger percentage of mobile women reported recent substance use, including heroin, crack/cocaine, opioids, and injecting any drugs, than did less-mobile women (Table 1).
At baseline, nearly one-third of participants self-reported receiving a major depressive disorder diagnosis (32%), and 53% had high PTSD symptoms based on the PCL-5. A larger percentage of women with high residential mobility had more severe depressive symptoms than did their less-mobile counterparts (51% vs. 40%, respectively; p = .037).
Trends in Residential Mobility and Client-Perpetrated Physical or Sexual Violence Over Time
The percentage of participants reporting high residential mobility decreased over time, from 52% at baseline to 32% and 30% at subsequent rounds. An unadjusted Poisson regression model adjusting for clustering of responses within participants showed that there was a 34% reduction in the risk of high residential mobility from baseline to round 2 (IRR: 0.66, 95% CI: 0.55–0.79, p < .001) and a 41% reduction in risk of high residential mobility from baseline to round 3, respectively (IRR: 0.59, 95% CI: 0.49–0.72; p < .001). Average predicted values and 95% confidence intervals based on this unadjusted Poisson regression model are shown in Figure 1.

Percentage of participants with high residential mobility, recent experience of client-perpetrated physical violence, and recent experience of client-perpetrated sexual violence over time. Graph depicts average predicted values and 95% confidence intervals from unadjusted Poisson regression models of (1) residential mobility over time, (2) recent experience of physical violence over time, and (3) recent experience of physical violence over time, fit using GEE with an exchangeable correlation structure and robust variance estimation to account for clustering of participants’ responses over time.
Recent experience of client-perpetrated physical violence also decreased over time from 33% at baseline to 20% and 17% at subsequent rounds. A similar reduction was evident when comparing recent experiences of sexual violence from baseline (26%) to rounds 2 and 3 (13% and 11%, respectively; Figure 1). An unadjusted Poisson regression model showed a 37% reduction in risk of physical violence from baseline to round 2 (IRR: 0.63; 95% CI: 0.48–0.81, p < .001) and a 47% reduction in risk of physical violence from baseline to round 3 (IRR: 0.53; 95% CI: 0.40–0.70, p < .001). Results of an unadjusted Poisson regression model of recent experience sexual violence were similar, with a 49% and 54% reduction in risk of sexual violence from baseline to round 2 (95% CI: 0.37–0.71, p < .001) and baseline to round 3, respectively (95% CI: 0.32–0.65, p < .001). Average predicted values and 95% confidence intervals based on these unadjusted Poisson regression models are shown in Figure 1.
Correlates Over Time With Client-Perpetrated Physical or Sexual Violence
Bivariate and multivariate Poisson regression models of factors associated with physical or sexual violence over time are shown in Table 2. After adjusting for survey round, study group, and other covariates, participants with high residential mobility had a 39% increased risk of physical violence (aRR: 1.39; 95% CI: 1.07–1.80; p < .05), and a 63% increased risk of sexual violence (aRR: 1.63; 95% CI: 1.14–2.32; p < .01) compared to less-mobile participants (Table 2).
Bivariate and Multivariate Poisson Regression Models of Factors Associated Over Time With Recent Experience of Physical or Sexual Violence Perpetrated by a Client.
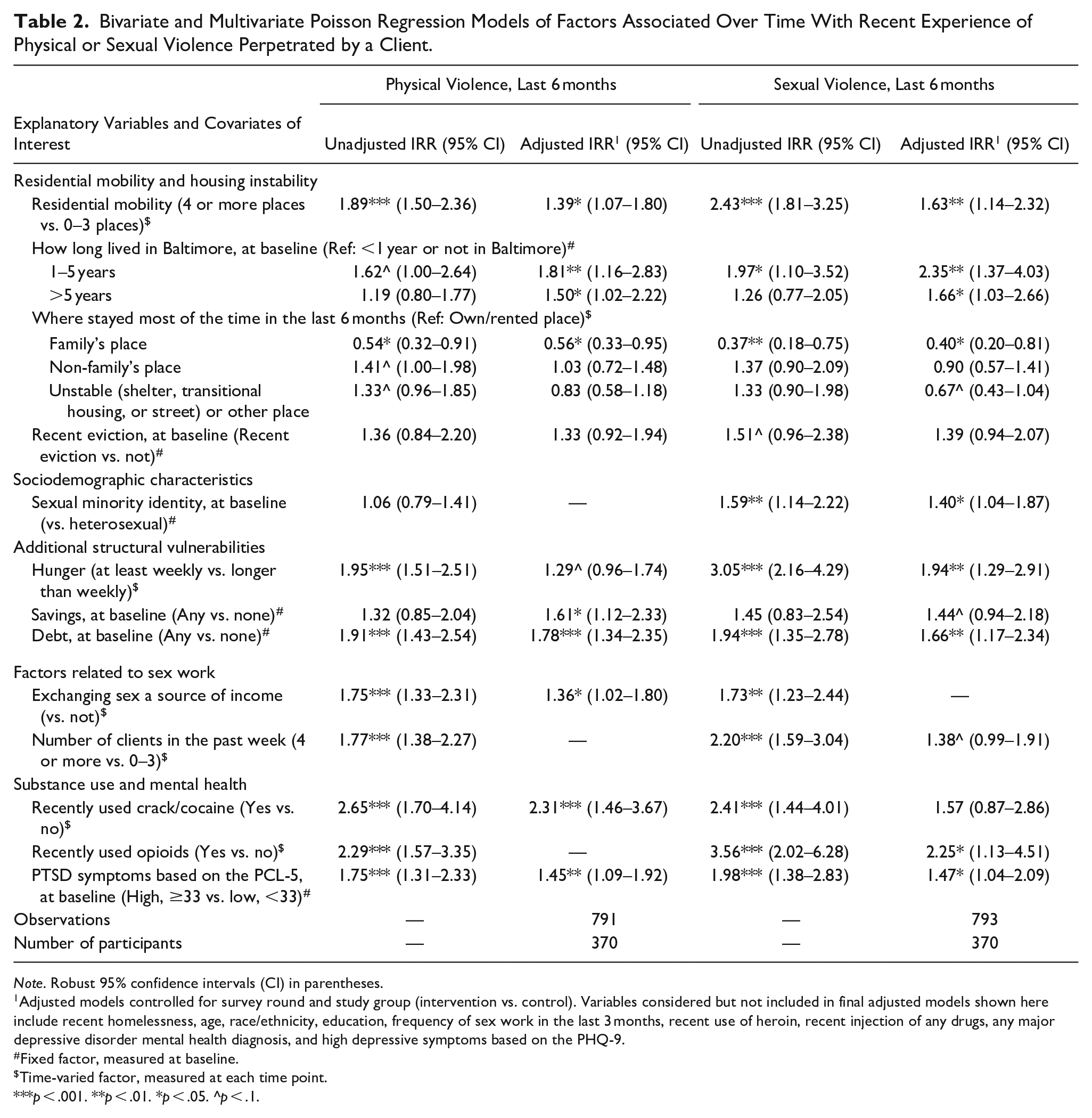
Note. Robust 95% confidence intervals (CI) in parentheses.
Adjusted models controlled for survey round and study group (intervention vs. control). Variables considered but not included in final adjusted models shown here include recent homelessness, age, race/ethnicity, education, frequency of sex work in the last 3 months, recent use of heroin, recent injection of any drugs, any major depressive disorder mental health diagnosis, and high depressive symptoms based on the PHQ-9.
Fixed factor, measured at baseline.
Time-varied factor, measured at each time point.
p < .001. **p < .01. *p < .05. ^p < .1.
Those who lived in Baltimore for 1 to 5 years and longer than 5 years had significantly increased risk of physical violence compared to those who lived in Baltimore for less than 1 year or who did not live in Baltimore at baseline (1–5 years aRR: 1.81, 95% CI: 1.16–2.83, p < .01; 5 or more years aRR: 1.50, 95% CI: 1.02–2.22, p < .05). A similar trend was evident in multivariate models of sexual violence (Table 2). Participants reportedly staying most of the time at a family member’s place had a 44% (aRR: 0.56; 95% CI: 0.33–0.95; p < .05) and a 60% (aRR: 0.40; 95% CI: 0.20–0.81; p < .05) reduced risk of physical and sexual violence compared to those spending most of their time in a place they owned or rented (Table 2).
Participants reporting a sexual minority identity had a 40% greater risk of experiencing recent sexual violence compared to their heterosexual counterparts (aRR: 1.40; 95% CI: 1.04–1.87; p < .05). Those who reported experiencing hunger at least weekly had a 29% greater risk of recently experiencing physical violence perpetrated by a client (aRR: 1.29; 95% CI: 0.96–1.74; p < .1) and a 94% increased risk of recently experiencing sexual violence (aRR: 1.94; 95% CI: 1.29–2.91; p < .01). Both having any savings or having any debt at baseline were positively associated with an increased risk of recent physical and sexual violence in adjusted Poisson regression models (Table 2). Participants who reported that exchanging sex was a source of income had a 36% increased risk of physical violence (aRR: 1.36; 95% CI: 1.02–1.80; p < .05). Having at least four clients in the past week was associated with an increased risk of recent sexual violence compared to those reporting less than four clients in the same time period (aRR: 1.38; 95% CI: 0.99–1.91; p < .1). Participants recently using crack/cocaine had significantly increased risk of physical violence (aRR: 2.31; 95% CI: 1.46–3.67; p < 0.001), while those recently using opioids had an increased risk of sexual violence (aRR: 2.25; 95% CI: 1.13–4.51; p < .05) compared to those who did not report recently using these substances. Those with scores suggesting more severe PTSD symptoms had a significantly increased risk of experiencing physical and sexual violence, respectively, compared to those with lower PCL-5 scores (physical aRR: 1.45, 95% CI: 1.09–1.92, p < .05; sexual aRR: 1.47, 95% CI: 1.04–2.09, p < .05).
Results of the sensitivity analysis showed that the associations described and presented here were consistent in restricted models where the sample was limited to those who participated in all three survey rounds. In this sensitivity analysis, participants who reported more recent residential mobility had an increased risk of physical violence (aRR: 1.42; 95% CI: 1.01–2.00; p = .043; data not shown) and an increased risk of sexual violence (aRR: 1.64; 95% CI: 1.03–2.62; p = .039; data not shown) compared to their less-mobile counterparts. Results from population-averaged negative binomial models with robust variance estimation showed consistent, significant associations between residential mobility and physical violence (aRR: 1.36; 95% CI: 1.04–1.78; p = .023; data not shown) and sexual violence (aRR: 1.66; 95% CI: 1.15–2.39; p = .006; data not shown).
Discussion
This study is one of the few to explore residential mobility among women who exchange sex and its associations with violence. We documented not only the high prevalence of residential mobility among women who exchange sex in Baltimore but also significant associations between residential mobility and increased risk of client-perpetrated physical and sexual violence after adjusting for women’s sociodemographic characteristics, structural vulnerability, substance use, and mental health. These findings provide necessary evidence of correlations over time between residential mobility and experience of client-perpetrated violence among women who exchange sex.
Strengthening our understanding of how residential mobility intersects with violence is critical for the development of public health interventions that are relevant to women’s lives and needs. Previous research has shown that residential mobility can be the result of existing economic vulnerability and social and structural discrimination, which have been shown to predict violence among women who exchange sex (Beattie et al., 2020; Decker et al., 2016; Deering et al., 2014; Lazarus et al., 2011; Leddy et al., 2018; Nestadt et al., 2020; Platt et al., 2018; Scorgie et al., 2012; Shannon et al., 2008; Shannon & Montaner, 2012). At the same time, residential mobility can be a determinant of violence in its own right, disrupting connections with places and people and leading to the exchange of sex in new settings, with new clients, without support systems or networks, all of which can increase the potential for violence. Future research should build on the findings of this study to examine the causal relationship and pathway linking residential mobility and client-perpetrated violence. To do this, it will be critical to further investigate the factors that lead women who exchange sex to be mobile, how the context of sex work varies for those with higher residential mobility, and the potential for such mobility or transience to be related to sex trafficking (Burckley et al., 2023; Chohaney, 2016; Goldenberg, Silverman, et al., 2014).
Residential mobility has been conceptualized as a critical aspect of housing instability (Coulton et al., 2012; Frederick et al., 2014; Swope & Hernández, 2019). Here, we present evidence in support for Swope & Hernández (2019)’s conceptual model of housing as a determinant of health equity by demonstrating robust associations between distinct measures of housing consistency (i.e., residential mobility, where women stayed most of the time, and recent eviction), one of the four pillars of their model, and client-perpetrated violence among women who exchange sex. Future research should draw on additional measures across the remaining pillars, including cost, conditions, and context, to examine whether and how these other pillars intersect with consistency to influence experiences of violence among women who exchange sex in Baltimore. The associations between residential mobility and place where participants stayed most of the time in the last 6 months, as well as with recent homelessness, at baseline provide preliminary evidence of these intersections. Building on these findings, future investigations could inform the design of more effective housing policies that address these women’s unique needs and promote health equity.
Additional aspects of women’s social locations, structural vulnerabilities, substance use, and mental health were also associated with participants’ experiences of physical and sexual violence in this study. The relationship between sexual orientation identity and recent experience of sexual violence among women who exchange sex reinforces the need for public health interventions to recognize women’s intersectional identities and the intersectional stigma they experience, influenced by both their engagement in sex work as well as other aspects of their social locations such as gender, race/ethnicity, or sexual orientation identity (Glick et al., 2020; Lyons et al., 2021; Rouhani et al., 2021). Financial and food insecurity were also significantly associated with increased risk of violence—both physical and sexual—suggesting that residential mobility intersected with other forms of material insecurity influences the environments in which women live and work putting them at increased risk for violence (Lim et al., 2019; Whittle et al., 2020). At baseline, those with high residential mobility also more commonly experienced hunger, illuminating how such material insecurity may be exacerbated in the lives of mobile women who exchange sex. Associations between substance use, including crack/cocaine and opioids, and experience of physical or sexual violence from clients reinforce previous findings in Baltimore (Decker et al., 2021; Fehrenbacher et al., 2020) and the ways in which sex work and drug use often overlap to affect the interactions women have with their clients (Lavalley et al., 2020). With evidence that mobile women who exchange sex more commonly reported using certain substances at baseline, residential mobility must be understood as an important factor influencing women’s daily lives and the environments in which they live and work. Together, these findings suggest that public health interventions should acknowledge the intersectional identities and experiences of women who exchange sex when designing violence-prevention programs. Furthermore, sex trafficking is an additional layer of vulnerability that may intersect with other aspects of people’s intersectional identities that, while not the focus of this study, have been shown in previous research to be correlated with structural vulnerabilities, substance use, mental health, and exposure to violence (Graham et al., 2019; Ottisova et al., 2016). Structural interventions can be used to take a comprehensive approach to address the social determinants of health, including residential mobility and housing instability, that influence client-perpetrated violence and other health outcomes among women who exchange sex.
Mobility has been conceptualized as having a disruptive influence on women’s lives, influencing people’s access to material resources as well as social relationships and social support that may lead them to exchange sex in different environments—perhaps without existing support networks—that may put them at increased risk of violence and affect care-seeking (Camlin & Charlebois, 2019; Davey et al., 2018; Goldenberg et al., 2012). This analysis demonstrated that staying most of the time in certain places, such as a family member’s place, was protective against both physical and sexual violence. The protective effect of living with family, found in this study to be associated with reduced risk of violence compared to those staying in their own or rented place, demands further exploration. Those staying with family may have greater access to critical social resources than those in other housing contexts. However, the type of familial relationship, and the characteristics of the family member’s place, should be investigated further. Research is needed to unpack these mechanisms in greater depth, including qualitative research to understand the nature of women’s mobility and how it influences their social relationships. This may include not only family members but also relationships with clients. While these findings did not distinguish between new and regular clients, future research should examine whether residential mobility and other aspects of housing instability affect the types of clients that participants have, how often they interact with those clients, and where interactions with those clients take place. These associations could inform more advanced quantitative analytical methods such as structural equation modeling to help identify pathways through which mobility influences violence.
These findings reinforce the importance of housing interventions, such as supportive housing models (Lazarus et al., 2011), in addressing violence and its sequelae. Residential mobility must be considered when designing public health interventions with women who exchange sex. Community-based interventions must ensure that intervention approaches are accessible to mobile populations and address the unique needs of those on the move. This includes spatial flexibility in the design of public health programs and integration of more robust follow-up approaches—using digital technologies or more novel data collection approaches (Felker-Kantor et al., 2021)—to improve data collection and retention over time. These efforts should be complemented by policies that address housing and determinants of residential mobility explicitly.
This study is not without its limitations. First, residential mobility was measured by number of places lived rather than other spatial, temporal, and social dimensions (Davey et al., 2019) such as destination, frequency, duration, agency (e.g., forced or voluntary), or reason for mobility (e.g., for the purposes of work). Further research should build on this study to understand how such domains intersect and influence housing instability, women’s risk environments, and exposure to violence. Further research to examine women’s agency in their own residential mobility will be critical to understanding how mobile women’s daily lives and work differ from non-mobile women who exchange sex. Forced mobility, be it through sex trafficking or another form of coercion, reduces control over the environments in which people live and work, leading to a greater potential for exploitation and dangerous conditions that can lead to violence (Bank et al., 2017; Goldenberg, Silverman, et al., 2014; Ristock et al., 2019; Ritterbusch, 2016). Given the potential link between engaging in sex work and human trafficking (Burckley et al., 2023), it is possible that residential mobility, in some instances, could reflect sex trafficking patterns among women who exchange sex. However, mobile sex work should not be equated with sex trafficking (Steen et al., 2015), and it is critical that the nuances across mobility, sex work, and sex trafficking be disentangled to inform more effective programs and policy (George et al., 2011; Mai, 2013; Yingwana et al., 2019). In addition, future models should examine neighborhood effects on experiences of violence, given the ways in which mobility disrupts the spaces in which women who exchange sex live and work. This could include, for instance, examining the effect of residential mobility within neighborhoods on client-perpetrated violence as has been done with other studies on intimate partner violence (Fedina et al., 2019). Frequency is just one piece of that mobility, and other measures used recently with women who exchange sex, such as daily activity diaries to explore individuals’ activity spaces (Felker-Kantor et al., 2021), could also be applied to improve data collection on residential mobility and housing status. Second, the results of this study are focused on structurally vulnerable women who exchange sex, most of whom have a history of substance use. These findings are not intended to be representative of all women who exchange sex. Future studies should explore the relevance of the dynamics identified here to women who exchange sex in other settings and with diverse lived realities.
In addition, loss to follow-up in this longitudinal study may imply that those who participated in all rounds of the study were different from those who did not. To address this limitation, a sensitivity analysis was conducted to compare results of a complete case analysis to results including participants with responses at least in one time period. Trends were consistent across models, suggesting that those who participated in all three rounds were not significantly different from those who were lost to follow-up in terms of the associations of interest. Furthermore, the use of a manual backward model selection approach may have increased the risk of selection bias. This model selection approach was chosen given the number of covariates that were theoretically relevant to the model and the relatively small sample size under consideration for analysis. We used a manual backward selection approach to finalize the models presented here to prioritize the most parsimonious model that was a good fit of the data. Finally, while this study examined the correlations over time between residential mobility and experiences of client-perpetrated violence, it did not examine whether mobility over a given time period predicted experiences of violence at subsequent time periods. Thus, the associated identified here do not necessarily imply causality. Further research should explore to what extent mobility predicts experiences of violence. The mechanisms through which mobility might influence women’s risk environments must be considered in the timing of data collection and recall periods used in data collection.
Conclusion
Together, this study begins to fill a significant gap in the literature understanding residential mobility and violence among women who exchange sex. Drawing on three rounds of data gathered from cisgender women in Baltimore, findings from this longitudinal study demonstrated that those who had greater residential mobility had an increased risk of client-perpetrated physical and sexual violence compared to their less-mobile counterparts, even after adjusting for other aspects of housing instability, social locations, structural vulnerabilities, factors related to sex work, substance use, and mental health. Structural interventions designed to address the social determinants of health among women who exchange sex should consider the role of housing instability, in particular residential mobility. Furthermore, public health interventions should acknowledge the extent of mobility among women who exchange sex in their design and implementation to ensure intervention effectiveness.
Footnotes
Acknowledgements
We acknowledge and thank the participants in the EMERALD study, SPARC clients, research study, and SPARC staff, the EMERALD study community advisory board, the Baltimore City Health Department, the Behavioral Health Leadership Initiative, Legal Aid of Maryland, and the Maryland Volunteer Lawyers Network for their invaluable contributions to this work. This project would not have been possible without their involvement and contributions.
Declaration of Conflicting Interests
The author(s) declared a potential conflict of interest (e.g., a financial relationship with the commercial organizations or products discussed in this article) as follows: Coauthor Susan G. Sherman, PhD, is an expert witness for the plaintiffs in opioid litigation. The other authors declare no conflicts of interest.
Funding
The EMERALD study was supported by the National Institute on Drug Abuse (R01DA041243); the National Institute of Mental Health (F31MH118817); and Johns Hopkins University Center for AIDS Research, a National Institutes of Health–funded program (P30AI094189).